Electronic Fetal Monitoring (EFM) Essentials
Electronic Fetal Monitoring (EFM) Essentials
EFM Overview
EFM is an ongoing, indirect screening tool for fetal oxygenation not diagnostic tool.
Fetal heart rate (FHR) changes detect interruptions in fetal oxygenation.
Factors Affecting Uterine Blood Flow
Excessive uterine activity(mom having contractions to low or too frequent)
Maternal hypotension or hypertension(can cause seizures in mom) .
Placental changes: calcifications, degenerative changes, infarction(abruption where it can tears from the wall/ if it does the baby has no oxygen!!) , decreased surface area.
Infection (Chorioamnionitis) and edema.
EFM Components
External: Ultrasound (measures FHR), Tocodynamometer (measures contraction frequency).
Internal: Intrauterine Pressure Catheter (IUPC) (measures uterine activity internally), Fetal Scalp Electrode (FSE) (measures FHR internally).
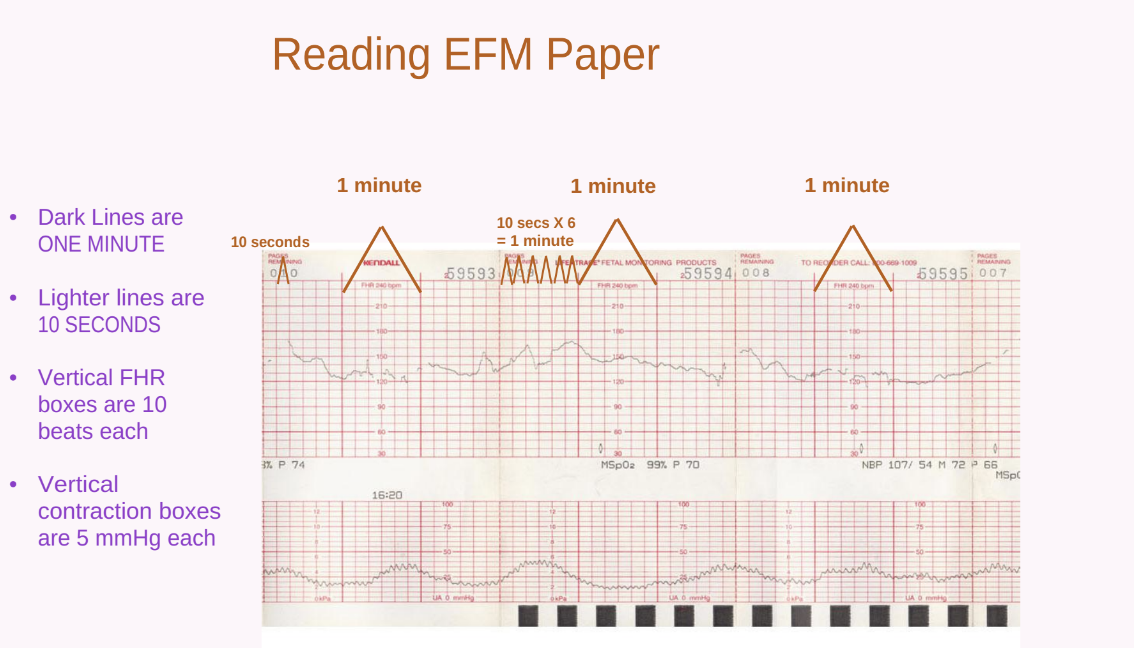
Reading EFM Paper
Dark lines: minute intervals.
Lighter lines: second intervals.
Vertical FHR boxes: beats each.
Vertical contraction boxes: mmHg each.
FHR Characteristics
FHR Baseline
Normal range: bpm.
Approximate mean FHR rounded to increments of bpm over a -minute window.
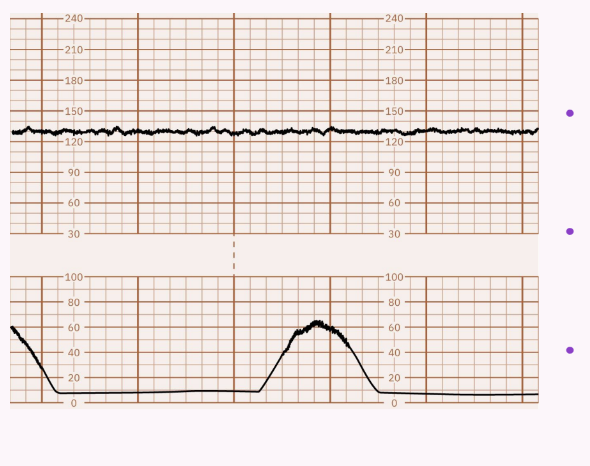
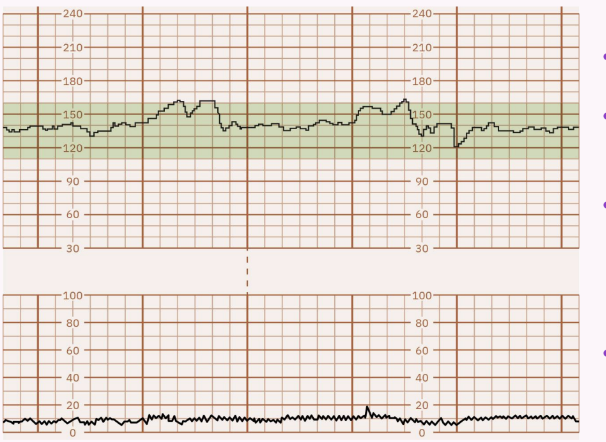
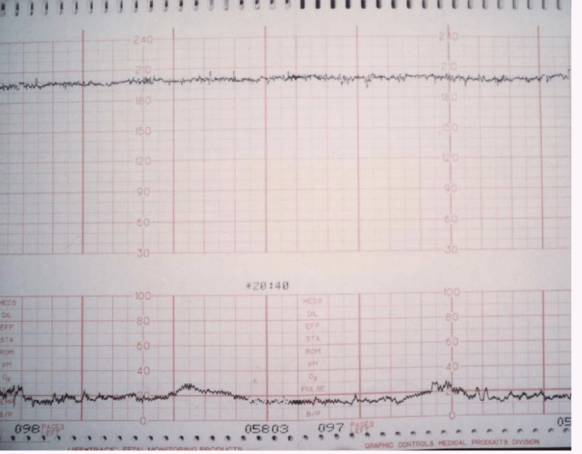
FHR Variability
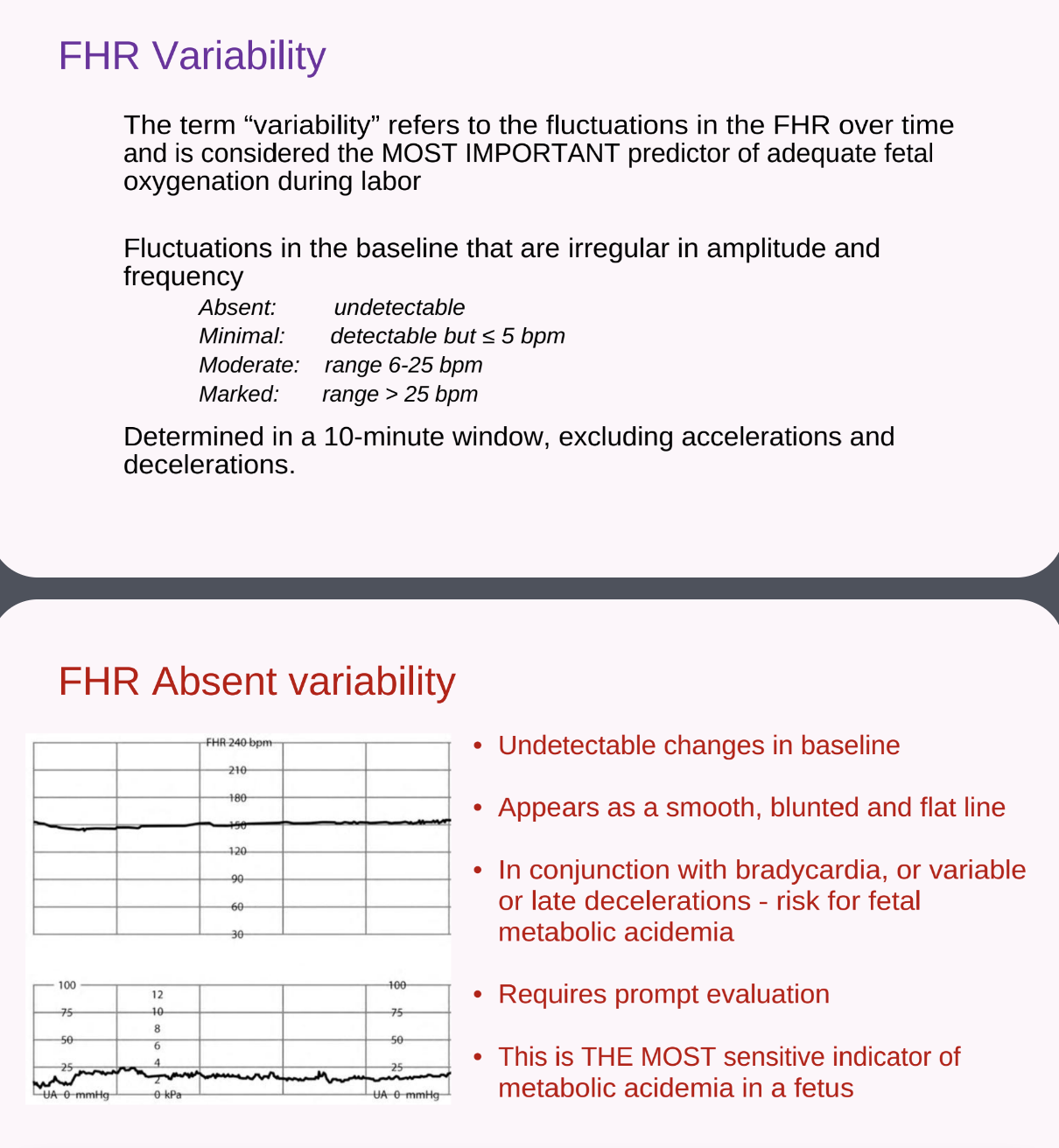
Most important predictor of adequate fetal oxygenation.
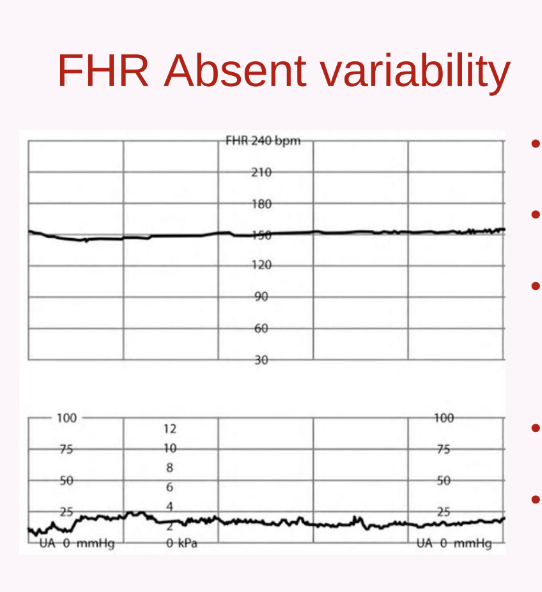
Absent: Undetectable; associated with risk for fetal metabolic acidemia, requires prompt evaluation.
Minimal: Detectable but bpm; may indicate fetal hypoxemia if prolonged.
Moderate: Range bpm; indicative of fetal well-being and adequate oxygenation.
this is what we want!! very happy baby!
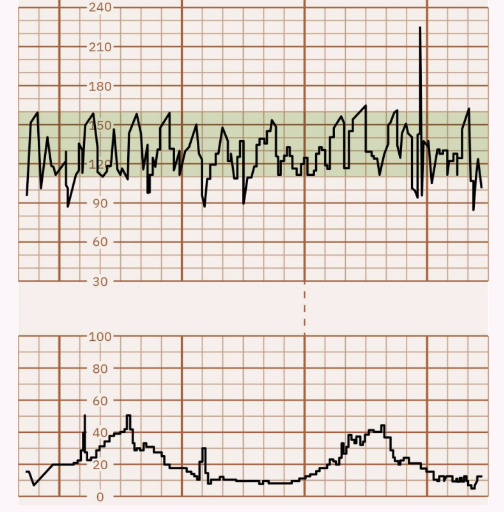
Marked: Range > 25 bpm; rare, often considered benign.
Sinusoidal Pattern: A smooth, sine wave-like undulating pattern ( cycles/minute for minutes) without accelerations; very concerning.

Absent Variability: No detectable changes in fetal heart rate; typically associated with fetal distress and requires immediate evaluation. NEVER WANT TO SEE STRAIGHT LINES!!!!!
its normal for it to happen for a little bit because mom just got some medication but if it is greater than or equal to bpm, it could indicate potential complications that need to be addressed promptly.
FHR Accelerations
Abrupt increase in FHR ( < 30 seconds to peak, lasting < 2 minutes).
weeks gestational age: bpm increase for seconds ( rule).
< 32 weeks gestational age: bpm increase for seconds ( rule).
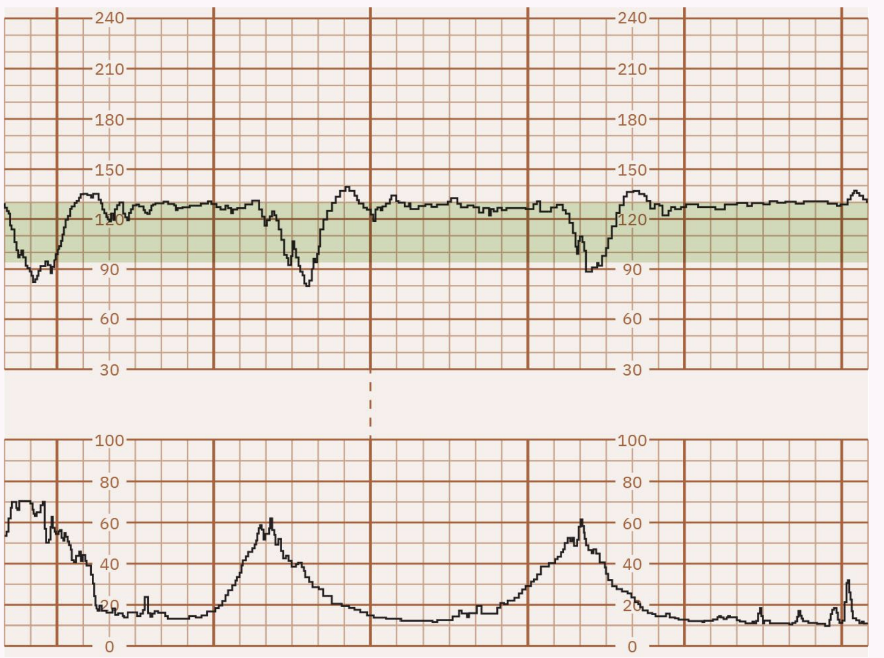
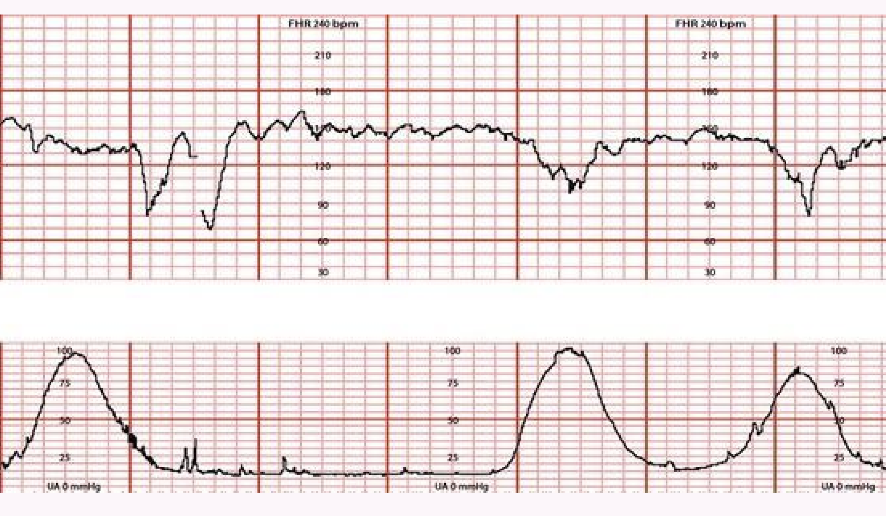
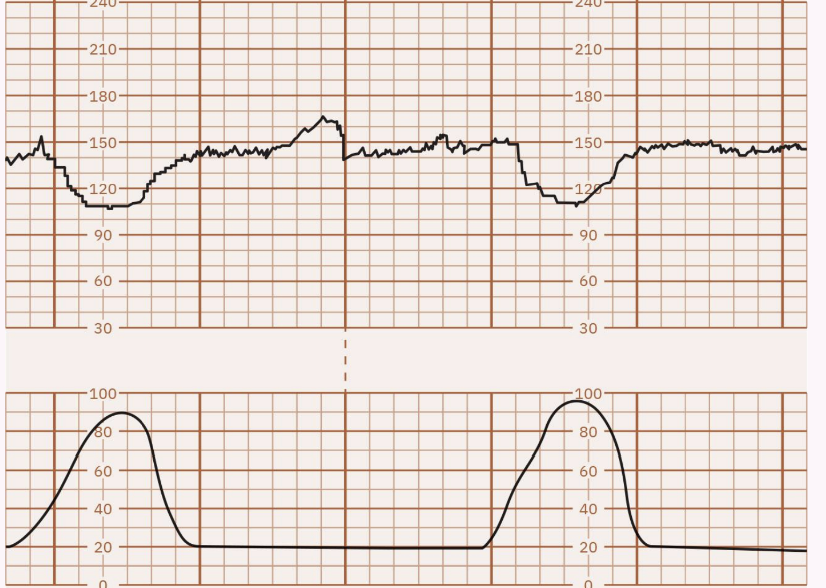
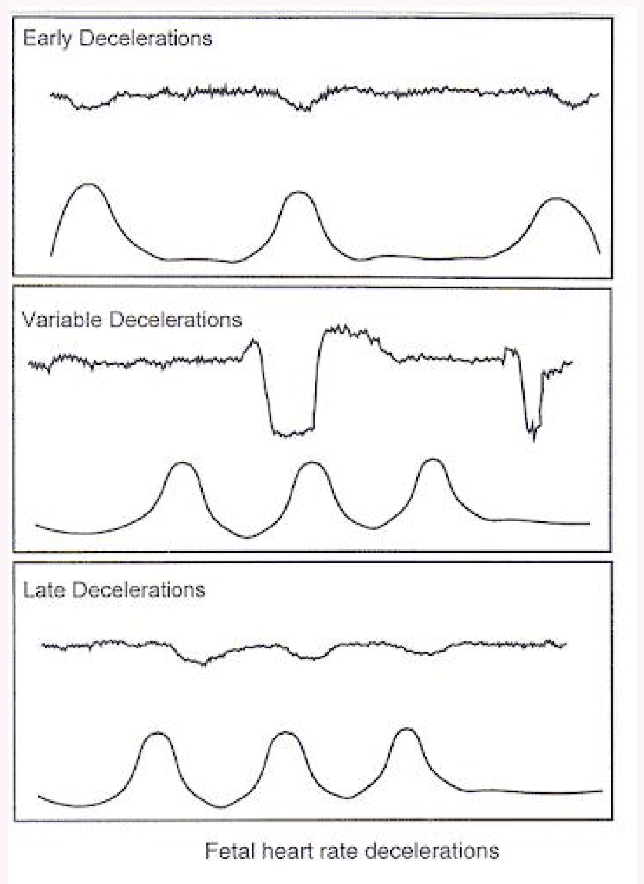
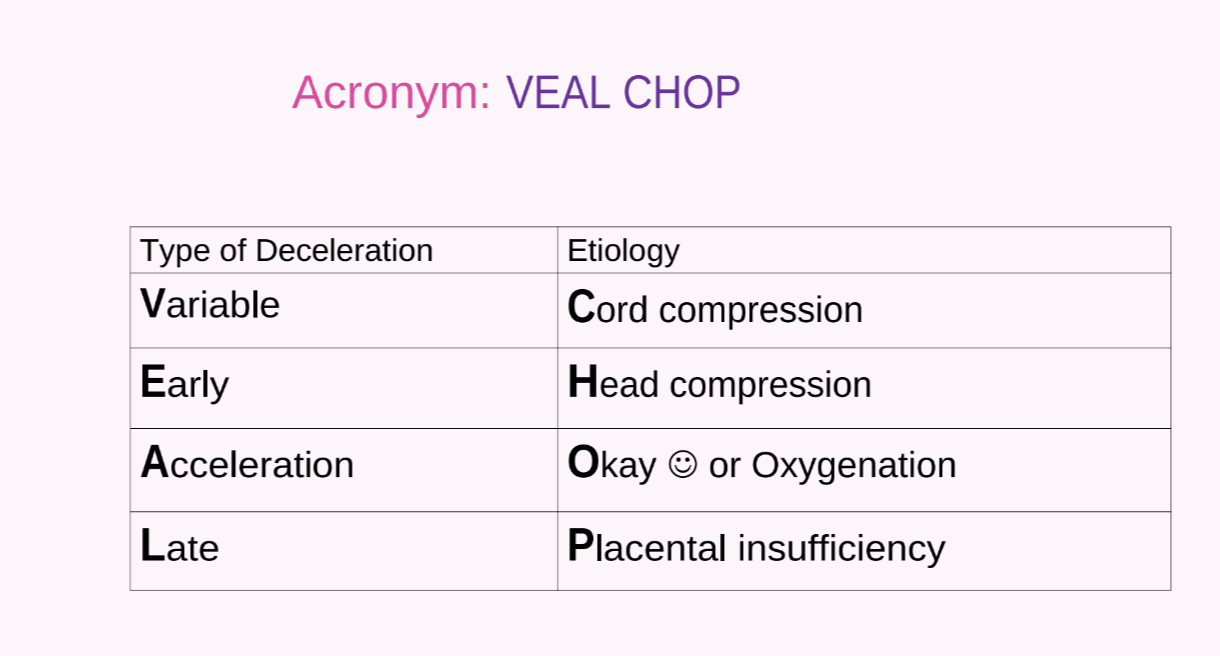
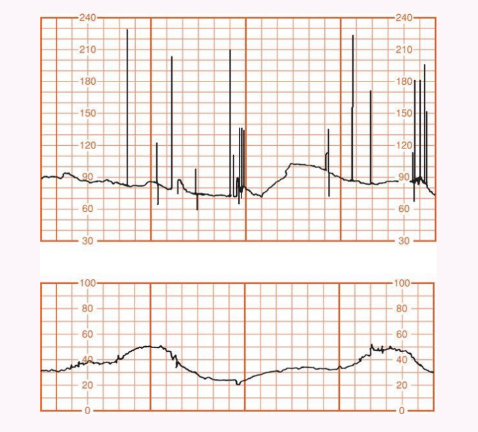
FHR Decelerations (VEAL CHOP)
Variable: Cord compression; abrupt decrease.
If you notice this CHANGE THE POSITION!
Early: Head compression; gradual decrease/return, symmetrical, peaks with contraction.
Acceleration: Okay/Oxygenation.
Late: Placental insufficiency; gradual decrease/return, occurs after peak of contraction.
FHR Tracing Categories
Category I (Normal): Baseline bpm, moderate variability, no late or variable decelerations, accelerations present/absent, early decelerations present/absent
Category II (Indeterminate): Characteristics not Category I or III ; may include baseline heart rate between bpm with decreased variability, variable decelerations that are intermittent, and/or transient late decelerations.
Category III (Abnormal): Absent variability with recurrent late or variable decelerations or bradycardia; or sinusoidal pattern.
end up in the OR (immediate delivery)
Non-Stress Testing (NST)
Assesses fetal well-being in response to activity.Reactive NST:At least accelerations in minutes for fetuses weeks gestation, with normal baseline, moderate variability, and no late decelerations.
FHR Bradycardia and Tachycardia
Bradycardia: Baseline < 110 bpm for > 10 minutes
profound bradycardia (< 60 bpm) is an emergency (CPR).
external recessitation: should be initiated immediately to maintain fetal oxygenation and prevent long-term complications.
moving mom around
prolapse
uterine rupture
cord compression may occur during labor, which can lead to fetal distress and requires careful management to ensure the safety of both mother and baby.
significant abdonimal pain
hard abdomen other than a contraction?
will complain with severe abdominal pain
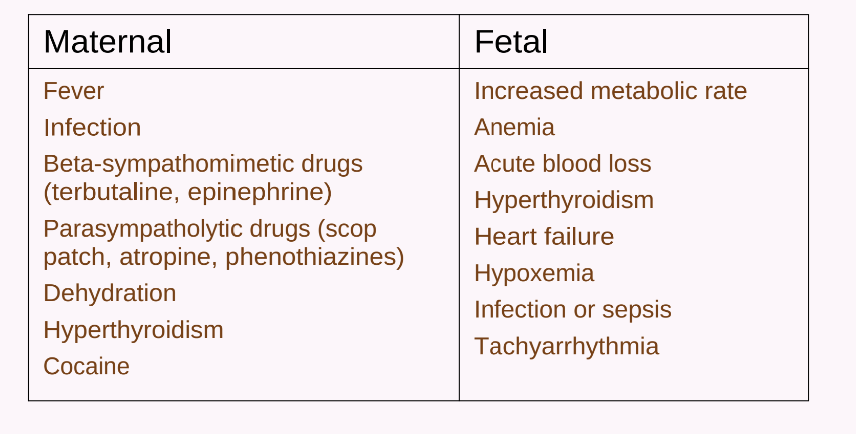
Tachycardia: Baseline > 160 bpm for > 10 minutes; common causes include maternal fever, medications.
Intrauterine Resuscitation (Golden Rules)
change position, iv bolus and call provider
you can hit stop on the pitocin while waiting for the provider
Maternal Repositioning (lateral- left to right)
IV Fluid Bolus.
Oxygen Administration (no longer routinely recommended; discontinue based on fetal response).
Uterine Activity Assessment
Frequency: Beginning of one contraction to the beginning of the next; Average number of contractions in minutes over -minute period (> 5 contractions in minutes = tachysystole: not enough resting time).
Duration: Length of contraction in seconds.
Intensity: Assessed by palpation (mild, moderate, strong) or in mmHg (IUPC: the most accurate).
Resting Tone: Between contractions; assessed by palpation (soft, hard) or in mmHg (IUPC).
very important since we need to oxygenate the baby
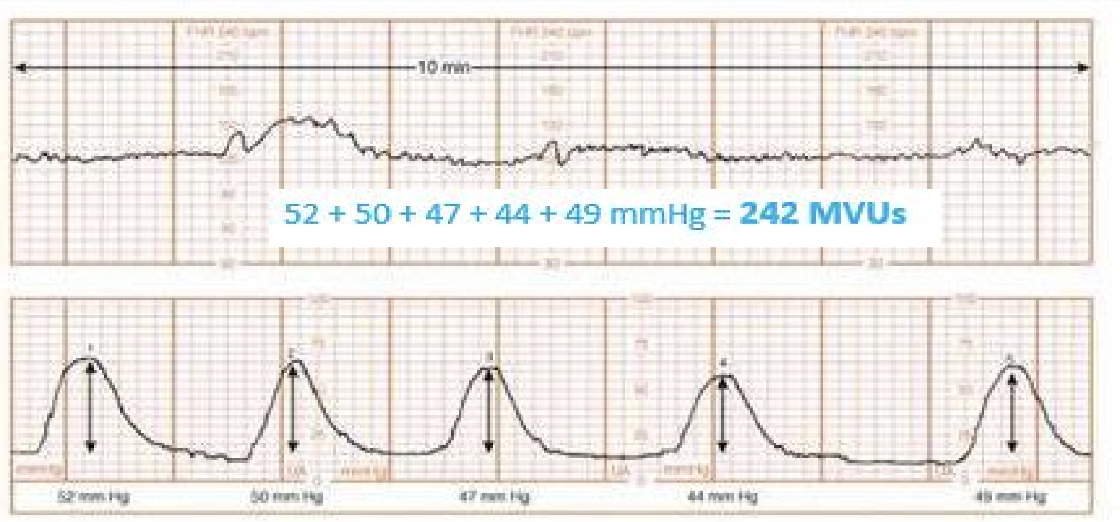
Montevideo Units (MVUs): Quantifies uterine activity with an IUPC; sum of (peak intensity - resting tone) for contractions over minutes. Adequate labor: MVUs.
peak minus the resting tone= to give you the MVU
Tachysystole: > 5 contractions in minutes; reduces maternal-fetal gas exchange and requires intervention (repositioning, fluid bolus, adjust Pitocin, tocolytics).