muscarinic acetylcholine receptors and AChE
There are five subtypes of muscarinic receptors which differ by their polypeptide chains, binding pocket and coupled intracellular receptor
The M1 “neural” receptor is found in autonomic ganglia and are responsible for the modulation of ganglionic transmission
The M2 “cardiac” receptor is found in cardiac atria and conducting tissue and is responsible for cardiac slowing and decreased force if contraction
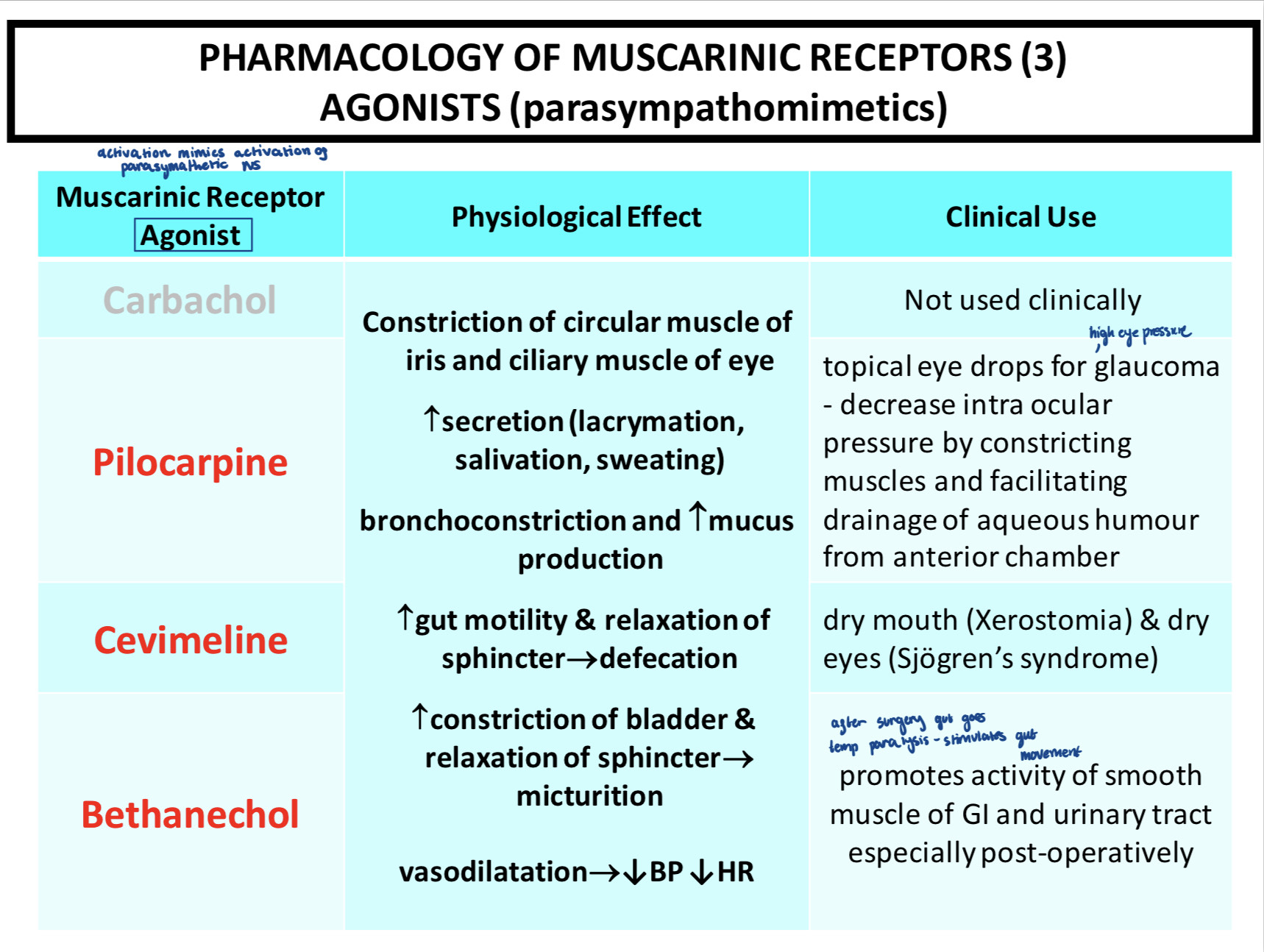
The M3 “glandular” receptor is found in salivary glands and smooth muscle of the gut. It is responsible for secretion of saliva and increased gut motility
The M4 receptor is found in the CNS and is responsible for modulation of synaptic transmission
The M5 receptor is found in substantia nigra in the CNS and is responsible of modulation of synaptic transmission
All muscarinic receptors are G protein coupled
The 1,3 and 5 receptors and linked to the G protein subtype G-alpha-q and has protein kinase c and Ca2+ as their second messenger. Physiologically, they are responsible for excitation, secretion and contraction
2 and 4 subtypes are coupled to G-alpha-I receptors and have reduced cAMP and PKA activity as well as G-beta-y opening K+ channels as their secondary messengers. Physiologically, they are responsible for inhibition and reduced force or rate contraction
Gaq works by stimulating PLC-beta which breaks down PIP2 to DAG and IP3. IP3 promotes the release of Ca2+ from internal stores while DAG activates PKC.
Gai inhibits adenylate cyclase which reduces cAMP due to the reduced activation of PKA and Ca2+ channel activity. Gby activates K+ chnnels which lead to its influx, leading to hyperpolarization and reduced excitation
 Pirenzepine was believed to be an an antagonist if the M1 receptor in gastric acid secretion. However, experiments proved this wrong. There was no less gastric acid secretion in response to CCh in mice lacking the M1 receptor compared with WT mice but there was a very strong reduction in gastric acid secretion in mice lacking M3 receptors.
Pirenzepine was believed to be an an antagonist if the M1 receptor in gastric acid secretion. However, experiments proved this wrong. There was no less gastric acid secretion in response to CCh in mice lacking the M1 receptor compared with WT mice but there was a very strong reduction in gastric acid secretion in mice lacking M3 receptors.
Cholinesterases breakdown ACh so is the target of many drugs. There are two types of cholinesterases:
“True” cholinesterases
present at cholinergic synapses which release ACh of a neurotransmitter
bound to the postsynaptic membrane in the synaptic cleft by an anchor
pseudocholinesterases
widely distributed and found in plasma and circulating in the bloodstream
important in inactivating the depolarising neuromuscular blocker '#
both are inhibited by most clinically relevant anticholinesterases
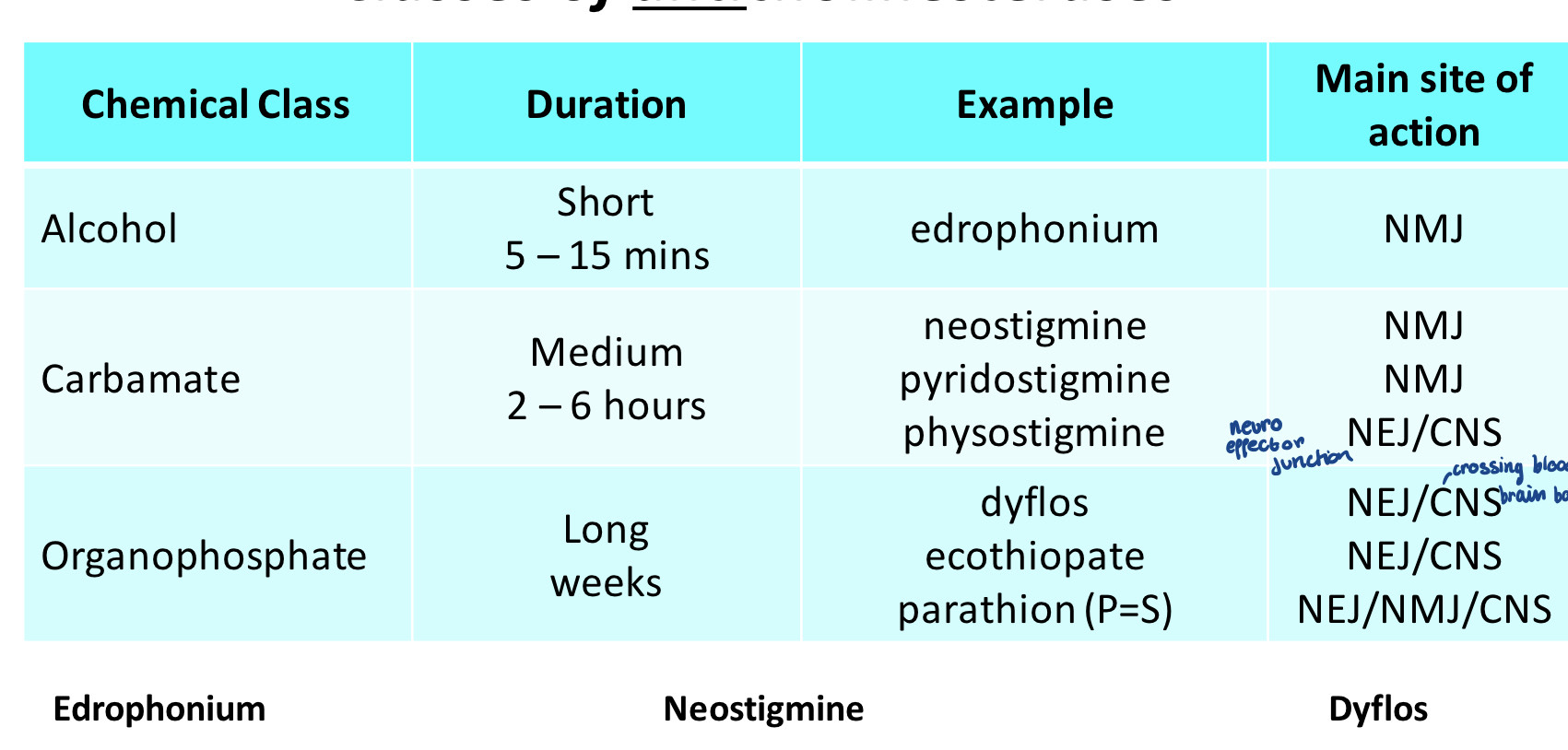
There are different classes of anticholinesterases as they will need to have different specificities and duration times.
 Cholinesterases work by attracting the choline group of ACh to the anionic site and the acetate group to the esteric site and then cleaving it. anticholinesterases work by blocking this second step either as reversible or irreversible blockers
Cholinesterases work by attracting the choline group of ACh to the anionic site and the acetate group to the esteric site and then cleaving it. anticholinesterases work by blocking this second step either as reversible or irreversible blockers
Reversible anticholinesterases
These are not as long lasting so are used as temporary drugs. An example of a drug that is an anticholinesterase is neostigmine which works by not allowing the choline group to escape from the enzyme binding pocket and ACh builds up in the synapse. This is slowly hydrolysed until the enzyme bind pocket is unblocked.
Irreversible anticholinesterases
Dyflos essentially covalently binds to the binding pocket of the enzyme with no spontaneous hydrolysis. Introduction of an organophosphate where the phosphate joins to the binding pocket. This can then be reactivated if -NOH is added as the phosphate will transfer onto this and reactivate the enzyme. However, the phosphate group bond will get stronger over time and so will become harder to break
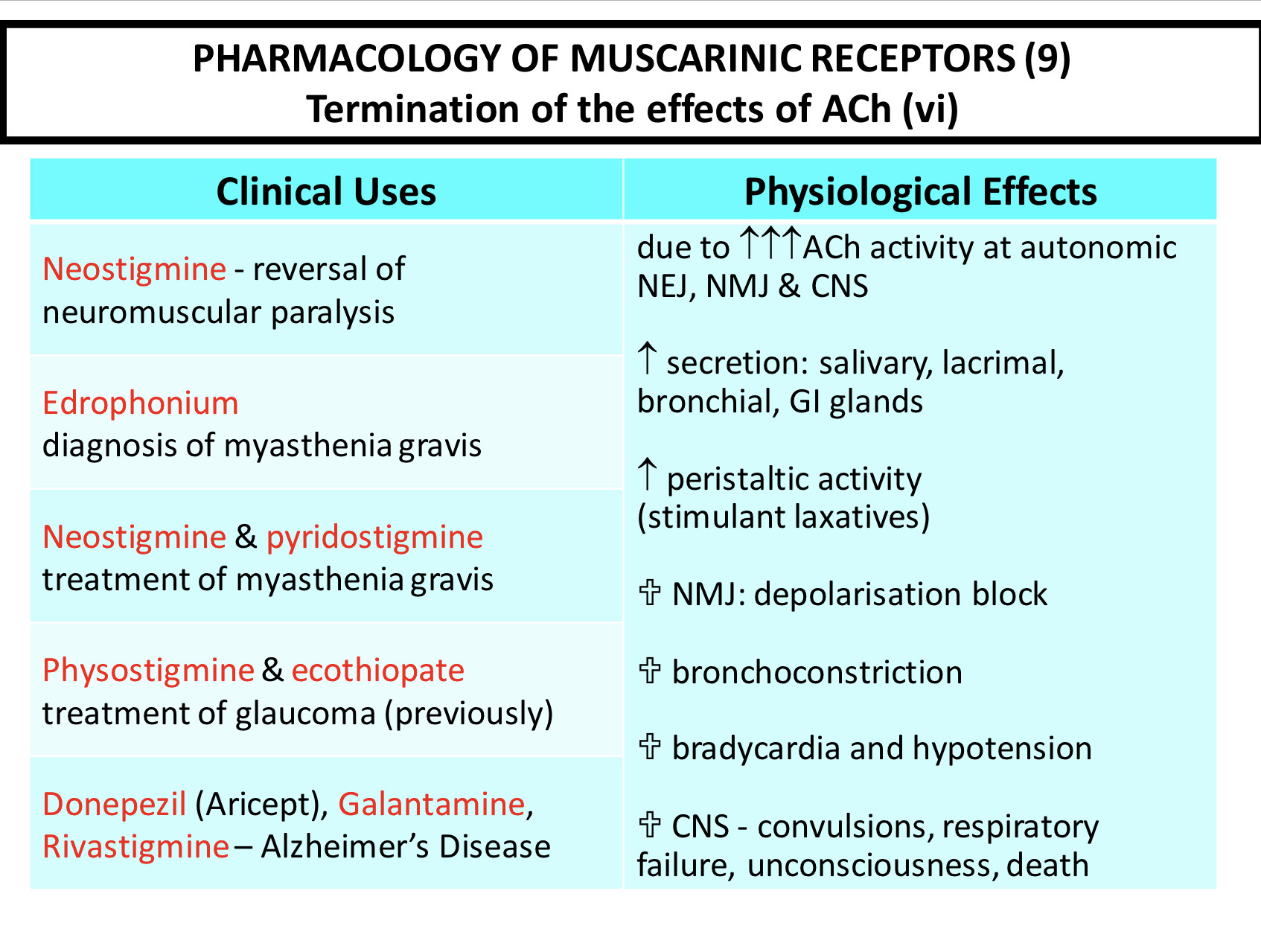 Myasthenia gravis is an auto immune disease where antibodies are made against the NMJ nAChR. This means that the receptors can be crossed linked and internalised or deactivated and leads to decreased strength of muscle contraction. It can be reversed by anticholinesterases
Myasthenia gravis is an auto immune disease where antibodies are made against the NMJ nAChR. This means that the receptors can be crossed linked and internalised or deactivated and leads to decreased strength of muscle contraction. It can be reversed by anticholinesterases