Health and Medicine
🫀 Circulatory system
Circulatory System 🫀
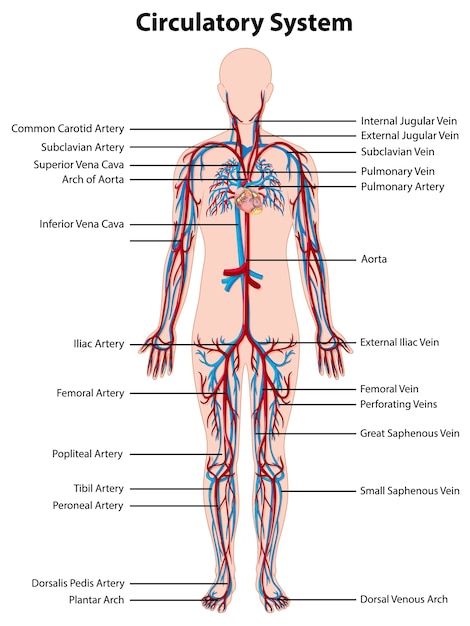
The Circulatory system, also known as the Cardiovascular system, is a vital network of organs and vessels that circulate blood through the body. Its responsibilities include delivering oxygen and nutrients to cells while removing waste materials. This system is made up of the heart, blood, blood vessels and the lymphatic system. The blood vessels also consist of 3 different parts: the veins, arteries, and capillaries.
Functions:
Transporting oxygen, nutrients, and hormones while removing waste materials.
Thermoregulation:- maintaining optimum body temperature.
Protects the body against diseases and infection.
Heart
The heart is a muscular organ about the size of your fist that pumps blood throughout the body. It is located in the thorax, which includes the heart, lungs (which are on either sides of the heart), and the diaphragm which is located under the lungs and heart. By pumping blood the heart ensures that there is blood flow which is essential in order for a cell to survive, because if there is no blood flow then the waste (CO2) produced by the cell would start to accumulate in a nearby blood vessel and likely clog the entire area. The cell would not be receiving any nutrients or oxygen either causing the cell to die.
Path of blood through the heart:
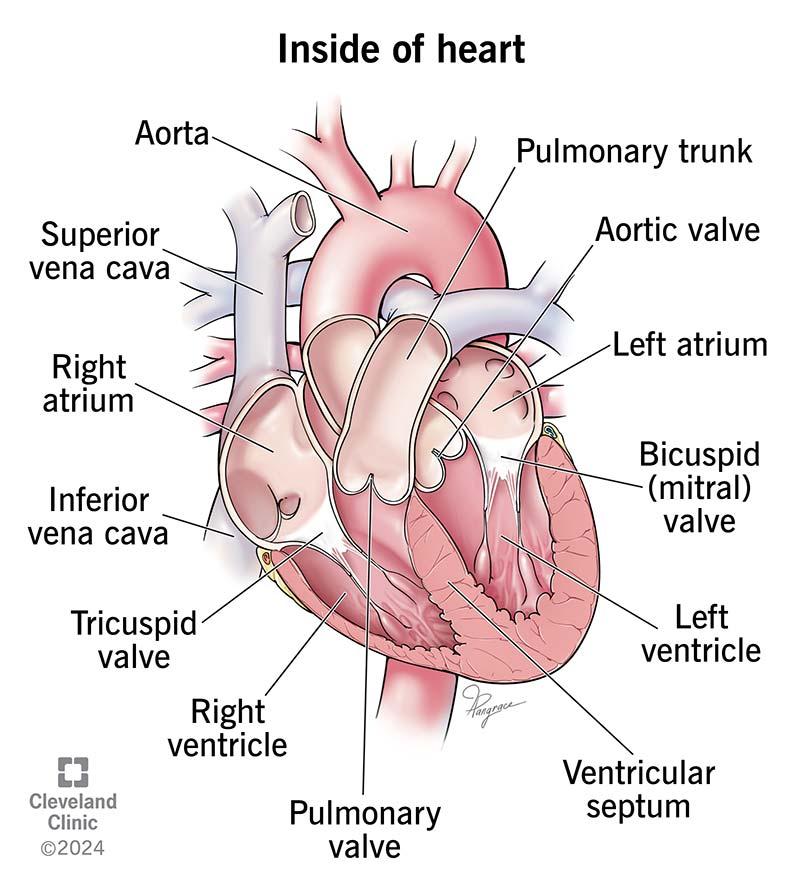
Blood travels to the heart through veins and away from the heart using arteries. Blood from all around the body comes to the heart from the superior and inferior vena cavae or veins and they end up in the right atrium. At this stage the blood is deoxygenated. From the right atrium the blood passes through the tricuspid valve to get to the right ventricle. Then the blood has to pass through another valve known as the pulmonary valve in order for blood to enter the lungs through the left and right pulmonary arteries. In the lung the blood gets rid of CO2 and collects Oxygen. From the lungs the blood goes back to the heart though the pulmonary veins and dumps into the left atrium. There it passes through the mitral valve and enters the left ventricle.
The final valve that the blood passes through is the aortic valve, and from there it goes through the aorta and then disperses to the rest of the body.
The 2 circulations in the body
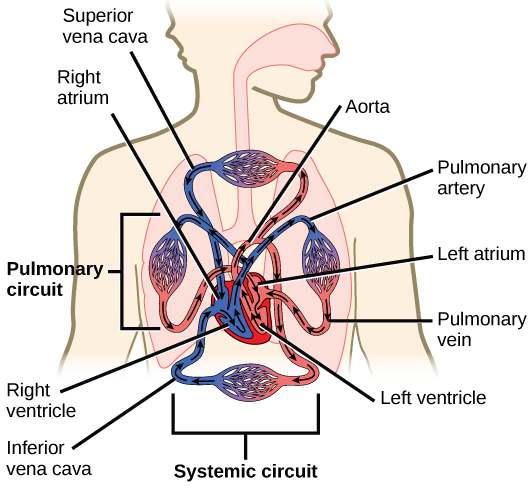
There are 2 different types of blood circulations in the body : Pulmonary circulation and Systematic circulation.
Pulmonary circulation:
This is the first part of the journey and in this the blood starts in the right side of the heart at the right ventricle and goes through the pulmonary trunk where it splits into 2 pulmonary arteries, one to the right lung and one to the left lung. As the blood comes out of the other side of the lung it goes through the left and right pulmonary veins. From the pulmonary veins the blood drains into the left atrium. This circulation relies on the right ventricle as the pump.
Systematic circulation:
This is the second part of the journey and in this circulation, the blood starts in the left ventricle and goes around to the body which includes all of the organs, and parts. Essentially the blood goes through the aorta from the left ventricle. The aorta branches and splits into several segments. These segments lead to the various tissues, organs and parts of the body, and then come out of the other side. In the end the blood ends up in the right atrium, and the Superior & Inferior Vena Cava are the ones responsible for bringing the blood back to the heart from the rest of the body. This system relies on the left ventricle as the pump.
The sounds of the heart (Lub-Dub):
At the same time as when there is blood moving from the right atrium to the right ventricle there is also blood moving from the left atrium to the left ventricle. This is because the heart is constantly pumping blood meaning that the blood from one cycle enters the left atrium after going through the lungs, and then from the left atrium it goes to the left ventricle. Meanwhile blood from another cycle just enters the heart through the right atrium after dropping off the oxygen at various parts of the body, which then goes to the right ventricle.
As soon as the blood enters the ventricles from the atriums through the tricuspid and mitral valve, those two valves snap shut in order to prevent backflows into the atriums. This produces a sound known as “Lub” or 1st heart sound/ S1. As these two valves close the pulmonary and aortic valves open. Then as soon as the blood goes into the pulmonary and aortic arteries through their respective valves, those valves also close to prevent backflow. The sound produced this time is known as “Dub” or 2nd heart sound/ S2. When these 2 valves close the other two valves (tricuspid and mitral) open. The opening and closing of these valves are what result in the heartbeat sounds. These two combined form the “Lub Dub” sound that you hear. The gap between when S1 occurs and S2 occurs is known as systole and this is the contraction phase of the heart when the ventricles pump blood to the rest of the body. The gap between S2 and the next S1 is called the diastole and this is when blood is refilling from the atriums into the ventricles.
Parts of the heart:
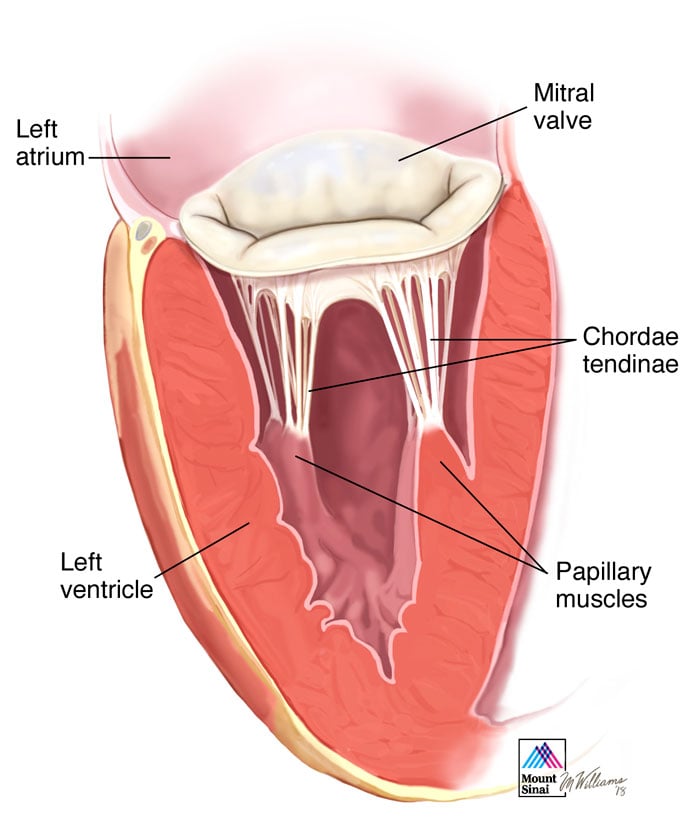
The atrioventricular valves are the tricuspid and mitral valve. To prevent these valves from opening and closing at wrong times in the wrong directions, they are tethered to the walls of the ventricles by chordae tendineae, and papillary muscles. If the chords break then the flow of blood would go the wrong way, causing the heart to be the last one to receive blood potentially causing heart failure.
Interventricular Septum (IVS):
It is a thin muscular wall that separates the left and right ventricle. It is made up of two parts; the membranous and the muscular. The IVS helps coordinate the contraction of the ventricles. Many babies are born with VSD (Ventricular Septal Defect) which is a hole in the membrane of the IVS. This allows blood to flow incorrectly between the left and right ventricles.
3 Layers of the Heart Muscle:
The innermost layer is known as the endocardium, and it covers the atrium, ventricles and valves on both the left and right side. The endocardium is very similar to the inner lining of the blood vessels. It is a very thin layer, and it acts as a barrier, controlling the exchange of substances between the blood and the heart muscle.
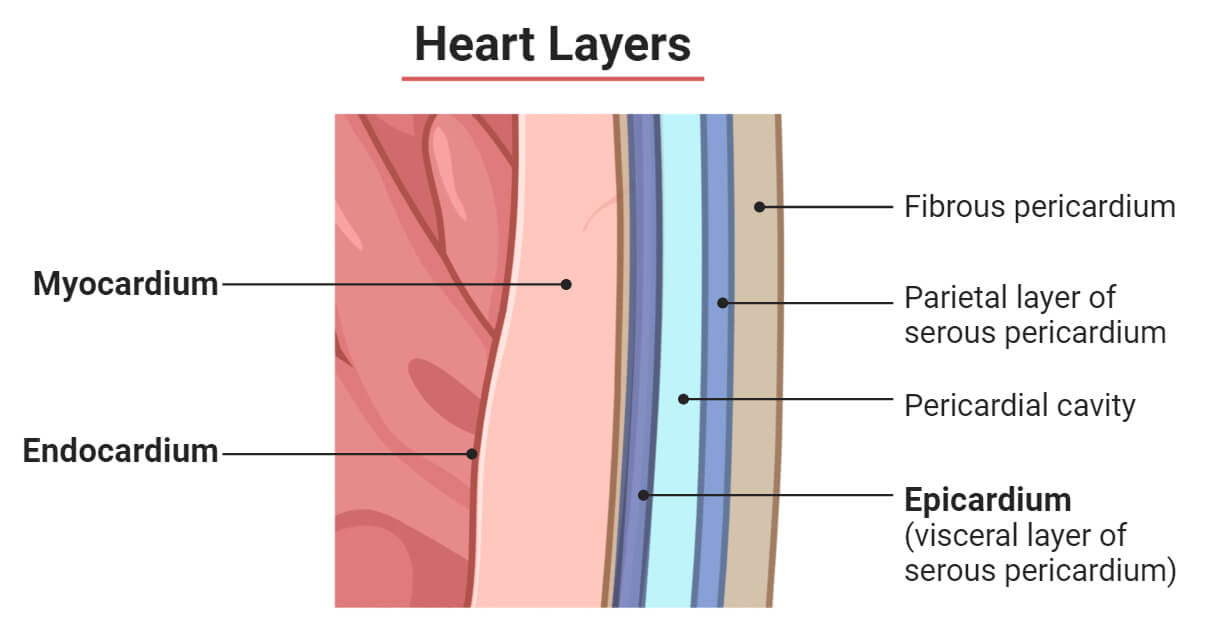
The next layer into the heart in the myostole which makes up the biggest part of the heart wall. It consists of cardiac muscle and is responsible for generating force to pump blood throughout the body. This is where all of the contractile muscle is, therefore most of the work is being done in these parts of the walls.
On the other side of the myocardium is the pericardium, which is a thin layer. The myocardium has two layers with a little bit of gap between them. The gap is not made of cells but contains a little bit of fluids. The way this works is that, as your heart grows, it grows into a sac or balloon kind of thing located under the sac. As the heart grows into the sac, it causes the balloon to spread around it making it a continuous sac with one layer against the myocardium and another layer with a little gap. The pericardium itself has two names. The layer hugging the organs is known as the visceral pericardium or Epicardium.
The layer on the other side of the gap is called the parietal pericardium. Outside the pericardium is the protective fibrous pericardium. This is a tough outer layer that provides structural support, and prevents overfilling.
Blood Vessels
Arteries vs. Veins:
Arteries- carry blood away from the heart, HIGH blood pressure, low blood volume()
Veins- carry blood towards the heart, LOW blood pressure, high blood volume()
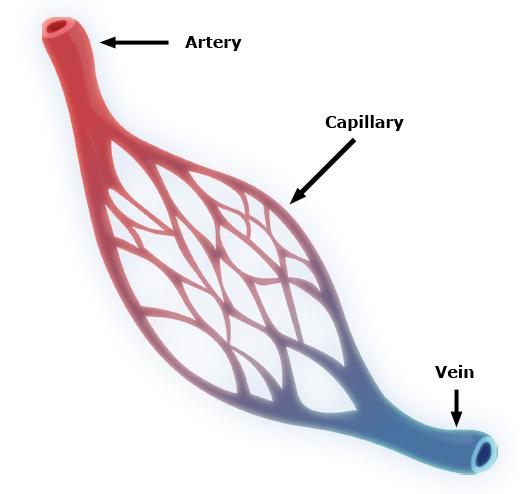
As blood goes away from the heart through the arteries, the arteries branch multiple times getting smaller and smaller as they go making vessels. Until then the blood will be oxygenated but as the artery branches smaller and smaller it will start to lose a lot of its oxygen to the fluids and cells around them. Here the blood becomes less oxygenated and these vessels start building into the veins. The small vessels that bridge between your arteries and your veins are known as capillaries and this is where a lot of the gas and nutrient exchange occurs. After going through the heart the blood will come back to the heart through the veins. Then it goes to the right atrium, then the right ventricle where it gets pumped towards the lungs through the pulmonary artery. Then the blood gets oxygenated and comes back in through the pulmonary veins and into the left atrium and left ventricle into the aorta where it goes to the rest of the body and the process restarts.
Arteries, arterioles, venules, and veins:
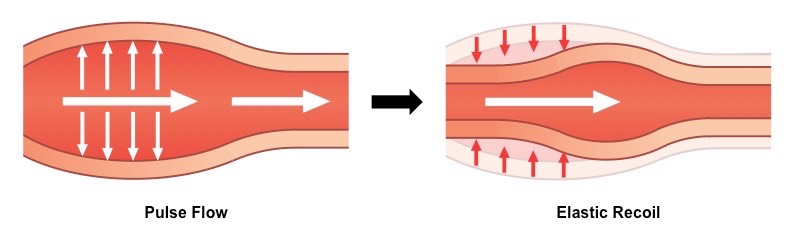
In order for blood to get to anywhere in your body it basically leaves through your heart which is a large artery. Then it branches down smaller, becoming a medium artery. The two things together; large and medium arteries, are sometimes known as “Elastic arteries”. One reason as to why they are called this is because they have a lot of a protein named elastin in the walls of the blood vessel. The elastic arteries can basically stretch to accommodate the pressure of the blood. Due to the high pressure of the blood that goes through here some of the pressure energy converts into elastic energy balancing out high pressures.
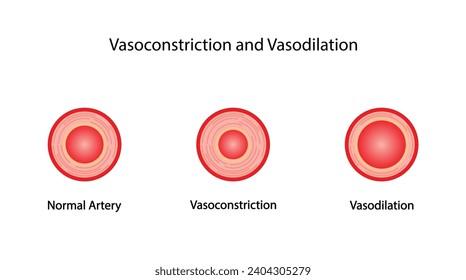
From the elastic arteries and the medium arteries, the arteries break down further forming the small artery and then the arteriole where the gas and nutrient exchange occurs. The smaller artery and the arteriole are sometimes together called the “muscular arteries”. The walls of these arteries are made up of smooth muscle. These arteries can perform vasoconstriction which is the tightening down of the blood vessels. This process increases resistance in the arteries. Most of this process takes place in the arteriole.
From the muscular arteries the blood goes through the capillaries, and gets collected in the venules. From the venules the blood travels through the veins which have valves, ensuring that the blood flows in the right direction. The veins deal with high amounts of blood while the arteries deal with high pressure. Then all the blood from the veins goes through the inferior and superior vena cavae.
Cardiac output
Cardiac output is the total volume of the blood pumped by the heart into the circulatory system per minute. It is the primary metric used to assess the heart’s ability to deliver oxygen and nutrients to tissues and meet the body’s metabolic needs.
Formula: CO = HR x SV
Cardiac output (CO): Typically expressed in L/min. A normal resting value for a healthy adult is around 5L/min.
Heart Rate (HR): The number of heartbeats per minute (typically between 60 - 100 at rest).
Stroke Volume (SV): The volume of blood ejected from the left ventricle with each single beat (Typically around 70ml at rest).
Stroke Volume
It is the volume of blood ejected from the left ventricle of the heart in a single contraction. The stroke volume of a normal healthy adult is around 70 ml at rest.
the formula to calculating it is SV = EDV - ESV
End-diastolic volume (EDV): The maximum volume of blood in the ventricle at the end of the filling stage (diastole), typically around 120 ml.
End-systolic volume (ESV): The remaining volume of blood in the ventricle after it finishes pumping (systole), typically around 50 ml.
Component of Stroke Volume
1. Preload (The Filling Pressure): Preload is the stretching of the cardiac muscle fibers just before the heart contracts. It is directly determined by the volume of blood entering the ventricle during diastole.
The Mechanism: According to the Frank-Starling Law of the Heart, greater stretching of the muscle fibers results in a more forceful contraction.
The Impact: An increase in venous return (blood flowing back to the heart) increases preload, which directly increases stroke volume.
2. Contractility (The Pumping Strength): Contractility is the intrinsic strength of the cardiac muscle contraction at any given preload. It operates independently of muscle stretch.
The Mechanism: It is regulated by the autonomic nervous system and chemical messengers. Sympathetic stimulation (like adrenaline) increases the amount of calcium available to the heart cells.
The Impact: Higher calcium levels allow the heart muscles to contract harder, which decreases the remaining ESV and increases stroke volume.
3. Afterload (The Resistance): Afterload is the pressure or resistance that the ventricles must overcome to open the semilunar valves and eject blood into the arteries.
The Mechanism: It is primarily determined by systemic arterial blood pressure and vascular resistance.
The Impact: If arterial pressure is high (as seen in clinical hypertension), the heart must work harder to push blood out. This leaves more blood behind in the heart (higher ESV), which decreases stroke volume.
4. Ejection Fraction Correlation: Stroke volume is also used to calculate the Ejection Fraction (EF), which is a key clinical index of heart health. Ejection fraction represents the percentage of blood pumped out of the total volume available.
EF = (SV / EDV) x 100
A normal resting ejection fraction typically ranges between 55% and 70%, meaning the heart never fully empties itself with a single beat.
Blood Pressure
Blood pressure is the lateral force exerted by circulating blood against the walls of the arterial blood vessels. Blood pressure is usually taken from your brachial artery which is in your upper arm. It is basically the force exerted/ surface area. It is represented or measured as two numbers: systole/diastole. The blood pressure measures the changes in pressure over heartbeats. The formula to calculate it is BP = CO x TPR. CO is the Cardiac Output which is the volume of blood pumped per minute. TPR or Total Peripheral Resistance is the systematic resistance to blood which is primarily dictated by the diameter of arterioles.
A standard clinical blood pressure reading (120/80 mmHg) {anything higher would indicate high BP}is measured in millimeters of mercury and consists of two phases:
Systolic Blood Pressure (SBP): The top number. It reflects the maximum pressure exerted against arterial walls when the left ventricle contracts and ejects blood during systole.
Diastolic Blood Pressure (DBP): The bottom number. It reflects the minimum pressure remaining in the arteries when the ventricles relax and fill during diastole.
Regulation of Blood Pressure
Short term Neural Mechanisms (Seconds-Minutes)
Baroreceptor reflex (Most Important):
When BP rises: Artery walls stretch -> signals travel via Cranial nerves IX & X to the medulla -> Sympathetic activity drops while Parasympathetic rises -> results in lower cardiac output, lower heart rate and vasodilation -> BP returns to normal
When BP drops: Artery stretch decreases -> signals drop -> medulla surges sympathetic activity and cuts parasympathetic activity -> increases CO, HR and causes vasoconstriction -> BP returns to normal.
Chemoreceptor Reflex: Triggered by chemical shifts (decreased oxygen & pH, rise in CO2), Sensory bodies route signals via CN IX & X to the medulla -> drives Sympathetic activity -> causes vasoconstriction to increase BP (with a mild increase in HR).
CNS Ischemic Response (Cushing effect): An emergency survival mechanism. Severe BP drops cause brain hypoxia and high CO2 -> forcefully stimulates the vasomotor center -> triggers a massive sympathetic discharge -> causes extreme vasoconstriction to drastically increase BP.
Marey’s Law: States that BP and Heart Rate are inversely related. High pressure stimulates the baroreceptors to reflexively slow the heart down while low pressure triggers a faster heart beat.
Intermediate mechanisms (minutes-hours)
Capillary Fluid Shift:
If BP drops: Fluid physically shifts from bodily tissues into the bloodstream (=300 ml) -> expands blood volume -> raises BP.
If BP rises: Excessive pressure pushes fluid out of the blood into tissues -> shrinks blood volume -> lowers BP.
Stress Relaxation: When BP rises sharply, blood vessels adapt by stretching -> vascular smooth muscle relaxes -> prevents sudden, dangerous spikes in pressure.
Reverse Stress Relaxation: When BP drops, vessel stretch decreases -> smooth muscle automatically contracts -> elevates BP.
Long Term Fluid mechanisms (hours-days)
Catecholamines (Adrenaline, Noradrenaline): Increase Heart Rate, strengthens heart muscle contractions, and boosts CO -> BP rises.
RAAS axis: A drop in BP or kidney perfusion releases Renin -> converts protein to Angiotensin I -> converts to Angiotensin II -> causes direct vasoconstriction and triggers Aldosterone -> kidneys retain sodium and water -> increases blood volume -> raises BP.
Vasopressin (ADH): Increases water reabsorption in the kidneys and triggers vasoconstriction -> raises BP.
ANP (Atrial Natriuretic Peptide): The built in relief valve.
Triggers water/sodium vasodilation -> lowers BP.
Local Chemicals:Bradykinin & Histamine: Cause vasodilation -> lower BP.
Endothelin: A highly potent vasoconstrictor -> raises BP.
Emotional Fainting (Vasovagal Syncope)
This pathway explains how a mental or sensory trigger creates a physical collapse:
Intense emotion/fear/sight of blood -> Cerebral Cortex -> Hypothalamus -> Vagal Center Stimulation
This dual-action response triggers:
Dropped Sympathetic Outflow -> Widespread Vasodilation
Surged Parasympathetic Outflow -> Severe drop in Heart Rate (HR)
Final Result: Sudden crash in BP and cerebral blood flow -> Fainting (Syncope).
RAAS
The Renin-Angiotensin-Aldosterone System (RAAS) is the body's primary long-term hormonal axis for regulating blood volume, sodium balance, and systemic blood pressure
1. The Triggers (Sensors)
Low Blood Pressure: Drops renal perfusion pressure.
Low Sodium (): Sensed by macula densa cells in distal tubules.
Sympathetic Surge: -adrenergic stimulation from stress/trauma
2. The Kidney Catalyst
Renin Secretion: Juxtaglomerular (JG) cells release the enzyme renin into blood.
3. The Conversions
Step A: Renin cleaves angiotensinogen (inactive protein from liver) into Angiotensin I (inactive precursor).
Step B: Angiotensin-Converting Enzyme (ACE) (from blood vessel linings, mostly lungs) cleaves Angiotensin I into Angiotensin II (fully active hormone).
4. Angiotensin II Actions
Arterioles: Causes direct, powerful vasoconstriction -> ↑ Total Peripheral Resistance (TPR).
Adrenal Cortex: Stimulates release of the steroid hormone aldosterone.
Brain: Triggers hypothalamus thirst center and releases ADH (Vasopressin) to retain pure water.
5. Aldosterone Execution
Target: Nephron's late distal tubules and collecting ducts.
Mechanism: Reabsorbs Sodium () into blood; water follows via osmosis.
Trade-off: Dumps Potassium () and Hydrogen () into urine.
Result: ↑ Blood volume, ↑ venous return, ↑ stroke volume.
6. Negative Feedback StopShutoff: Rising blood pressure and normalized sodium levels stop JG cells from releasing renin, halting the cascade.

Renin- It is an enzyme produced and released by the kidneys that plays a crucial role in regulating your blood pressure, blood volume and sodium balance.
Angiotensin- It is a peptide hormone that plays a crucial role in regulating blood pressure and fluid balance. It works by constricting (narrowing) blood vessels and triggering the body to retain water and sodium which naturally raises blood pressure.
Aldosterene- It is a steroid hormone produced by your adrenal glands. Its primary function is to regulate blood pressure by managing sodium and water reabsorption in the kidneys while prompting the excretion of potassium. It plays a crucial role in maintaining your body's fluid balance and electrolyte levels.
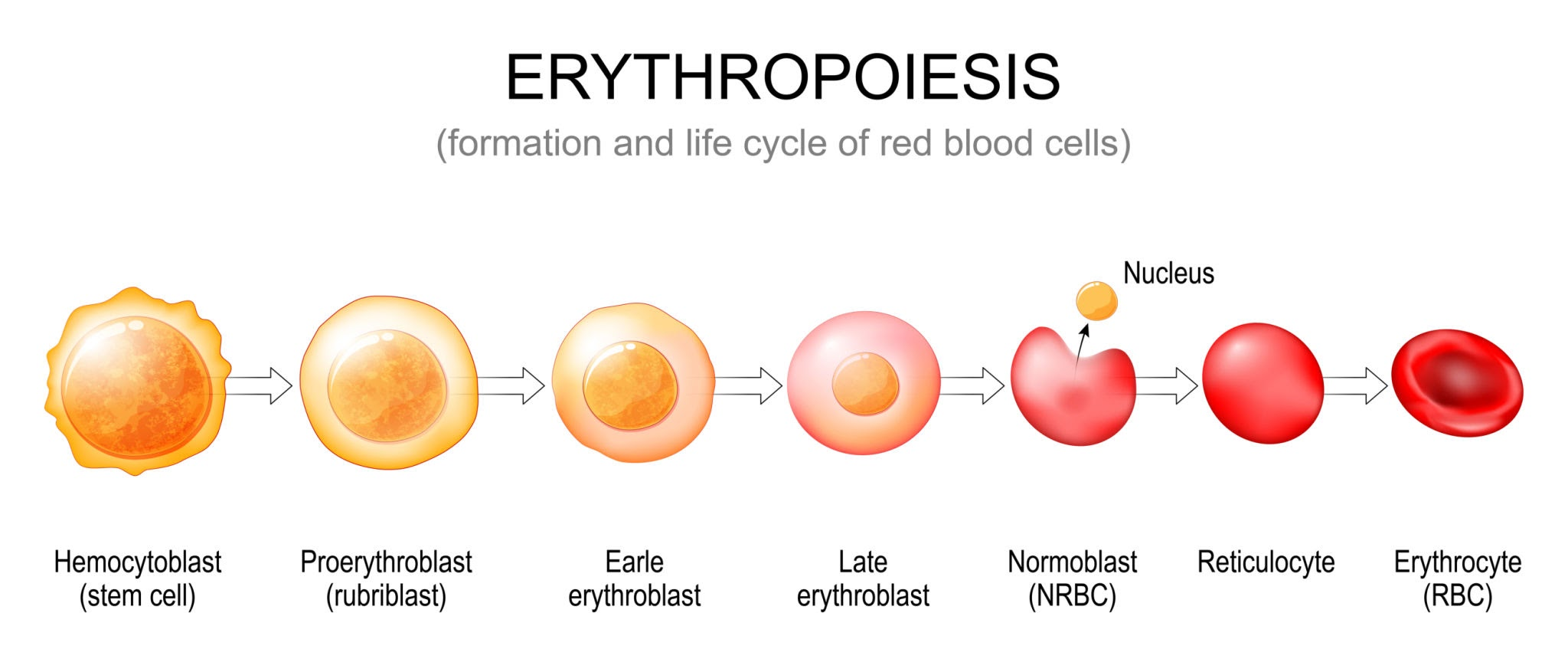
Erythropoetin
It is a vital glycoprotein hormone produced primarily by the kidneys that regulates the production of red blood cells. It acts as a chemical messenger, traveling through the bloodstream to instruct the bone marrow to generate new RBCs which contain hemoglobin which is essential for the transport of oxygen. Other names for it include EPO, hemopoietin, and hematopoietin.
How it works: The body controls EPO levels using a sensitive negative feedback loop based on oxygen tracking.
Oxygen Sensing: Specialized fibroblast cells in the kidney continuously monitor blood oxygen concentrations.
Hormone release: When tissue oxygen drops (hypoxia) - due to anemia, lung disease or moving to a high altitude - the kidneys quickly ramp up EPO production.
Bone marrow activation : EPO travels to the bone marrow and binds to specific receptors on immature blood stem cells. It prevents those cells from dying (apoptosis) and forces them to grow into healthy functional RBCs.
Feedback Shutdown: Once the new RBCs restore normal oxygen delivery the kidneys slow down EPO production.
Cardiovascular Diseases
Hypertension
Also known as high blood pressure it is a chronic medical condition where the force of blood pushing against your artery walls is consistently too high. It is usually when you have a blood pressure reading of 130/80 mmHg or higher. It is often called the silent killer as it has no visible symptoms while gradually damaging your heart, blood vessels and vital organs.
Blood Pressure Category | Systolic mmHg (top) | Diastolic mmHg (bottom) |
|---|---|---|
Normal | Less than 120 AND | Less than 80 |
Elevated | 120-129 AND | Less than 80 |
Stage 1 Hypertension | 130-139 OR | 80-89 |
Stage 2 Hypertension | 140 or higher OR | 90 or higher |
Hypertensive Crisis | Higher than 180 AND/OR | Higher than 120 |
Types and Causes
Hypertension is generally classified into two main categories based on its cause:
Primary (Essential) Hypertension: This is the most common form, developing gradually over many years with no single identifiable cause. It is heavily influenced by genetics, older age, and lifestyle factors like high sodium diets, physical inactivity, and stress.
Secondary Hypertension: This type appears suddenly and is caused by an underlying medical condition. Common triggers include kidney disease, sleep apnea, thyroid problems, adrenal gland tumors, or certain prescription medications.
Health Complications (Consequences of leaving it untreated)
Heart Attack and Stroke: High pressure stiffens and damages arteries, blocking or bursting blood vessels supplying the brain and heart.
Kidney Damage: Hypertension can narrow and weaken the blood vessels in your kidneys leading to chronic kidney disease.
Vision loss: Strained or torn blood vessels in the eyes can cause permanent vision impairment.
Dementia: Narrowed arteries can limit blood flow to the brain, leading to vascular dementia.
Management and Treatment
Hypertension is highly manageable through a combination of daily habits and medical support:
Lifestyle Modifications: Adopting the DASH eating plan (low sodium, high potassium), getting at least 150 minutes of moderate exercise weekly, limiting alcohol, and quitting tobacco.
Medications: If lifestyle changes are not enough, healthcare providers frequently prescribe antihypertensive drugs such as ACE inhibitors, ARBs, diuretics, or calcium channel blockers to help relax blood vessels.
Atherosclerosis
Atherosclerosis is a chronic inflammatory disease characterized by the buildup of sticky plaque inside your arteries, which restricts the flow of oxygen-rich blood to your organs and tissues. This plaque is a mixture of cholesterol, fat, calcium, blood cells, and cellular waste. Over time, the plaque hardens, narrowing the arteries and making them stiff and less flexible.
The Four Stages of Plaque Formation
Atherosclerosis is a slow, progressive condition that often begins as early as childhood and develops over several decades.
:Stage 1: Initial damage. The inner lining of the artery (the endothelium) suffers microscopic injuries due to high blood pressure, smoking, or elevated toxins.
Stage 2: Fatty streak. Low-density lipoprotein (LDL or "bad") cholesterol enters the damaged vessel wall and becomes oxidized, signaling white blood cells to travel to the site.
Stage 3: Plaque growth. White blood cells absorb the cholesterol, forming "foam cells" that clump together with calcium and other waste to create a growing, fibrous plaque mass.
Stage 4: Plaque rupture. The hardened plaque becomes unstable and cracks open. This triggers a rapid blood clot (thrombus) that can completely block blood flow instantly.
Major Risk Factors
The primary drivers that damage the arterial walls include high LDL cholesterol, high blood pressure (hypertension), cigarette smoking, diabetes or insulin resistance, and lifestyle factors.
Cardiovascular Complications
Atherosclerosis typically shows zero symptoms until an artery is blocked by at least 50% or a plaque completely ruptures. Depending on which arteries are affected, it causes distinct, serious medical conditions
:Coronary Artery Disease (CAD): Plaque in the heart's arteries restricts blood flow, causing chest pain (angina) or a full heart attack if completely blocked.
Carotid Artery Disease: Plaque builds up in the main arteries of the neck supplying the brain, which can lead to a transient ischemic attack (TIA) or a debilitating stroke.
Peripheral Artery Disease (PAD): Hardened plaques restrict blood flow to the limbs—especially the legs—resulting in cramping pain during exercise (claudication), cold extremities, or poor wound healing.
Chronic Kidney Disease: Blockages in the renal arteries starve the kidneys of blood, severely impairing their ability to filter waste.
Treatment procedures include lifestyle changes, medication and surgical intervention.
Myocardial Infarction
Myocardial infarction (MI), commonly known as a heart attack, is a life-threatening medical emergency that occurs when blood flow to a portion of the heart muscle is severely reduced or completely blocked, causing tissue damage or death from lack of oxygen.
Key symptoms include chest discomfort, radiating pain, breathing difficulties and systemic signs like unexplained fatigue, heavy sweating, dizziness, nausea or vomiting.
Common causes are plaque rupture, blood clot formation, and arterial spasm.
Classification Types
STEMI: ST-segment elevation myocardial infarction, indicating a total artery blockage that requires immediate surgical reopening.
NSTEMI: Non-ST-segment elevation myocardial infarction, meaning a partial or temporary blockage that still requires urgent medical care.
Diagnostic Methods
Emergency teams use a combination of tests to confirm an MI diagnosis.
Electrocardiogram (ECG): Measures the heart's electrical activity to identify rhythm issues and structural blockages.
Cardiac biomarker blood tests: Detects elevated levels of cardiac troponins, which are proteins released into the bloodstream when heart muscle cells die.
Coronary angiography: Uses imaging dye to visualize exactly where blockages are located in the blood vessels.
Immediate Treatments
Medications: Administered immediately, including chewable aspirin to prevent clotting, nitroglycerin for chest pain, and thinners or clot-busting drugs.
Percutaneous Coronary Intervention (PCI): A catheter procedure using a balloon and a stent to physically open up the blocked artery.
Coronary Artery Bypass Grafting (CABG): Open-heart surgery used in complex cases to reroute blood flow around severe blockages
Prevention strategies include dietary adjustment, regular physical activity, chronic disease control, and tobacco cessation.
Heart Failure
Heart failure occurs when the heart muscle is too weak or too stiff to pump enough oxygen-rich blood to meet the body's needs. It is a serious, chronic, and typically progressive condition, but contrary to its name, it does not mean the heart has completely stopped beating. Instead, the heart struggles to keep up with its workload, leading to fluid backup and oxygen deprivation throughout the body.
Symptoms are shortness of breath, persistent fatigue, swelling (edema), sudden weight gain, and chronic coughing.
Types
Left-Sided Heart Failure: The most common form. The left ventricle cannot effectively pump blood to the body, causing fluid to back up into the lungs.
Systolic Failure (Reduced Ejection Fraction): The heart muscle becomes too weak to squeeze and pump blood out properly.
Diastolic Failure (Preserved Ejection Fraction): The heart muscle becomes stiff and thick, meaning it cannot relax and fill with enough blood between beats.
Right-Sided Heart Failure: Usually triggered by left-sided failure. The right ventricle is too weak to pump blood to the lungs, causing fluid to back up into the abdomen, legs, and veins.
Common Causes and Risk Factors
Heart failure is usually the result of another underlying medical condition that has damaged or overworked the heart over time:
Coronary Artery Disease (CAD): Plaque buildup narrows the arteries supplying the heart, which can lead to a heart attack and permanent muscle damage.
High Blood Pressure (Hypertension): Forces the heart to work much harder to circulate blood, eventually causing the muscle to stiffen or weaken.
Cardiomyopathy: Diseases of the heart muscle itself, which can be caused by infections, heavy alcohol use, or inherited genetic traits.
Diabetes and Obesity: Metabolic conditions that place extra stress on cardiovascular function.
Heart Valve Defects: Malfunctioning valves prevent proper blood flow, causing the chambers to pump harder to compensate.
Treatment
Medications: These include beta-blockers to lower heart strain, ACE inhibitors to relax blood vessels, diuretics ("water pills") to flush out excess fluid, and newer therapies like SGLT2 inhibitors.
Lifestyle Adjustments: Sticking to a strict low-sodium diet, tracking daily weight, limiting fluid intake, and participating in structured cardiac rehabilitation.
Implantable Devices: Devices such as pacemakers or Implantable Cardioverter-Defibrillators (ICDs) help keep the heart beating in a regular rhythm.
Advanced Procedures: In end-stage scenarios, surgical interventions like ventricular assist devices (VADs) or a heart transplant may be required.
🩸 Blood
Blood
Blood is mostly fluid but it also contains cells and nutrients that make it thicker than water. An average adult male has about 5 liters (10.5 pints) of blood while an average adult female has about 4 liters (8.5) pints. Blood makes up 8% of your total weight. It is made up of four parts: The blood is filtered by the spleen
Plasma (55%)
Red blood cells (44%)
White blood cells (+ Platelets account for 1%)
Platelets
Function
Blood carries oxygen and nutrients to cells and tissues as it takes waste away from the cells. It protects our bodies from infections and marks clots that can stop bleeding after an injury. Lastly it also regulates body temperature and blood pressure.
Where is it made
Blood starts in the bone marrow which contains stem cells. Stem cells are the earliest versions of blood cells and once they completely develop they enter the blood vessels as whole blood.
Parts of blood
Plasma
Plasma is a yellowish fluid that is more than 90% water, and its main job is to transport. The other 10% are made up of 8% protein (eg. Albulin, Antibody, fibrinogen (+clotting factors)) and 2% hormones, electrolytes and nutrients. It carries blood cells, essential proteins and salts throughout the body while also carrying waste products away from cells to the kidneys and livers. It also maintains body temperature and keeps blood cells moving through the body.
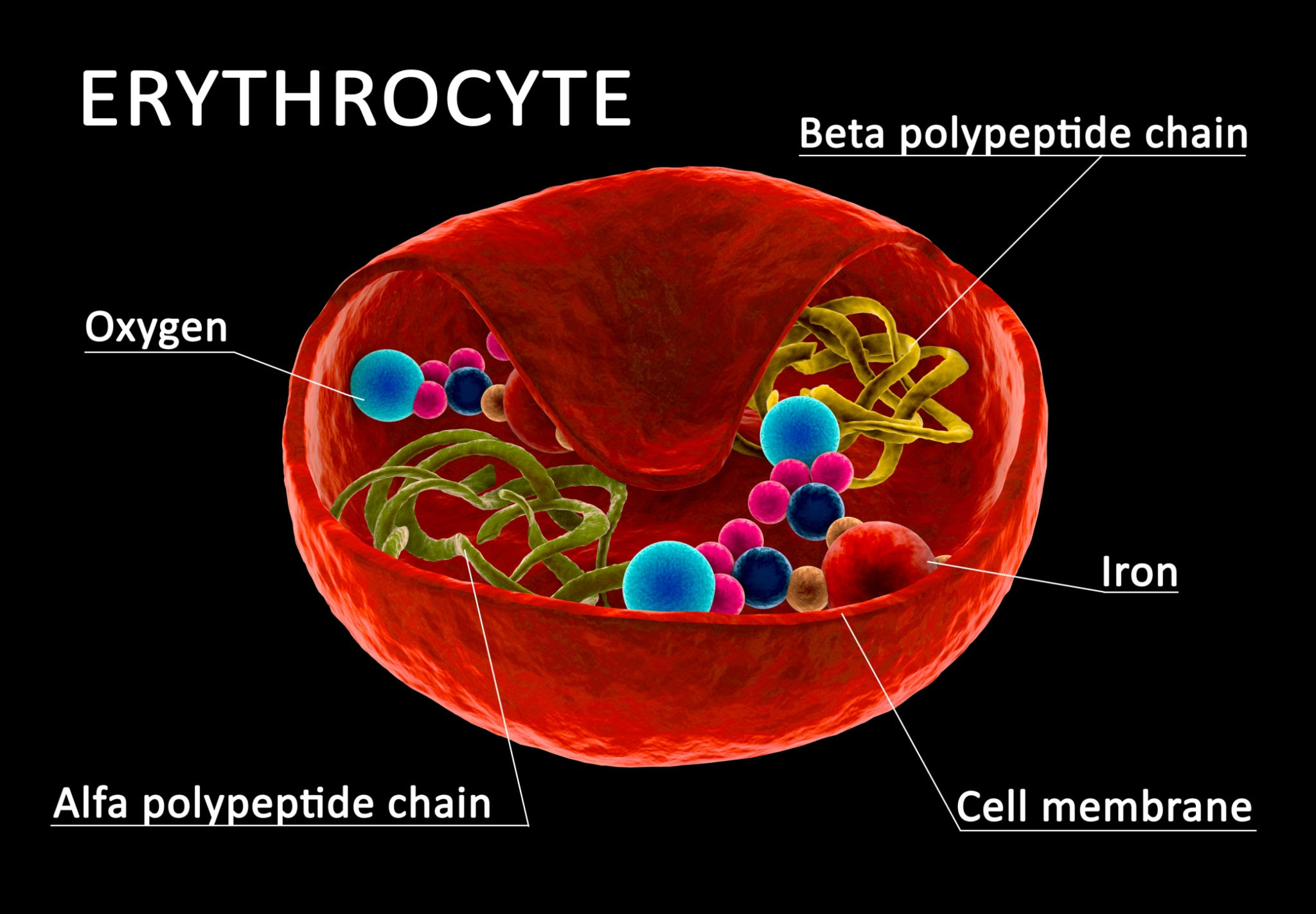
Red blood cells (Erythrocytes)
They are specialized enucleated cells packed with hemoglobin designed primarily for oxygen transport from lungs to peripheral tissues and carbon dioxide transport back to the lungs.
They get their color from the protein hemoglobin and they live about 120 days before your body makes new cells to replace them.
Their shape is a biconcave disc profile and their surface area is between 136 to 140 μ m². It can squeeze through micro-cappilaries with a diameter of 7.5μm, and a thickness between 1.0 to 2.0 μm.
Males have between 5.0 to 5.5 x μL. Females and children have between 4.5 to 5.0 x μL.
The nitric oxide in the red blood cells helps regulate vascular tone and blood pressure.
They develop in the bone marrow and are released into the bloodstream once they fully mature which takes around 7 days.
Composition & Membrane biophysics
Hemoglobin (Hb): Accounts for 34% of cell mass (〜30 picograms/cell). Normal range; 14-16 g/dL (men) and 12-14 g/dL (women).
Cytoskeleton: The membrane has a highly flexible protein network containing spectrin, actin, and ankyrin. This grid allows RBCs to reversibly deform when squeezing through 3 μm capillaries.
Antigenic Determinants: Glycoproteins and glycolipids on the external leaflet dictate the ABO and Rh blood group.
Physiological metabolism
They rely on anaerobic glucose metabolism as they don't have a mitochondria, generating net 2 ATP to maintain membrane ion pumps ().
White blood cells (leukocytes)
They are a part of your immune system and when germs or cancer cells attack, the white blood cells find and destroy them. They have a nucleus, do not contain hemoglobin, and can move out of blood vessels into tissues to fight infections. Adults normally have between 4,000 to 11,000 cells per microliter (μL) of blood. Their lifespan varies widely from a few hours to several days though some memory cells can live for years. They are created in the red blood marrow from hematopoietic stem cells through a process called leukopoiesis They use diapedesis (squeezing through capillary walls) and chemotaxis (following chemical scent trails) to hunt down pathogens. WBCs are divided into two main categories based on whether they contain granule-like packets under a microscope.
Granulocytes (The first responders) : chemical filled granules in cytoplasm & multi-lobed nuclei (polymorphonuclear cells)
Neutrophils (50-70% Frontline Soldiers): They have 3-5 lobes in their nucleus and are the first ones to arrive at an infection site. They swallow bacteria (phagocytosis) and release chemical traps. When they die in battle the form pus.
Eosinophils (1-4% The Parasite Hunters): They have a two lobed nucleus and specialize in attacking parasite worm infections. They also help control allergic reactions by dampening inflammation.
Basophils (0.5-1% The Alarm System): They are jam-packed with purple granules that often hide the nucleus and they trigger inflammation during allergic reactions. They release histamine (which dilates blood vessels to cause swelling/redness) and heparin (an anticoagulant that prevents blood from clotting too quickly so other WBCs can travel easily).
Agranulocytes (The specialists) : smooth cytoplasm without prominent granules and have a simpler larger nucleus.
Monocytes (2-8% The giant clean up crew): They are large cells with kidney-bean or horseshoe shaped nucleus. They wander in the blood for a few days and enter tissues where they form into giant cells called macrophages. They act as garbage disposals, swallowing large amounts of bacteria, dead cells and cellular debris.
Lymphocytes (20-40% The elite special forces): They are slightly larger than a RBC with a massive, round nucleus that fills most of the cell. They are responsible for specific immunity (targeting specific germs and creating long-term memory). The 3 main types are :
B-lymphocytes (B-cells): Produce antibodies that act like targeted missiles to neutralize specific germs.
T-lymphocytes (T-cells): Direct the immune response and directly kill infected body cells or cancer cells.
Natural Killer (NK) Cells: Destroy virus infected cells and tumor cells without needing prior activation.
Platelets (thrombocytes)
Platelets are plate-shaped membrane bound fragments of much larger cells. They are usually the first ones there if a blood vessel is damaged or bleeding. Platelets seal damaged blood vessels by forming clots and that way, blood stays in while germs stay out. They are oval shaped when inactive and sprout tiny spider-like arms when activated. They are only 2-4 μm in diameter, don’t have a nucleus and cannot reproduce. They only live for about 7-10 days before they are destroyed by the spleen and liver. The normal range of count in humans is 150,000-450,000 platelets per microliter (μL) of blood. They are the ones that perform hemostasis.
They are formed in red bone marrow from giant cells called megakaryocytes. A single megakaryocyte develops long extensions that break off into thousands of tiny pieces directly in the bloodstream, which are your platelets. The process is strictly regulated by thrombopoietin (TPO), a hormone produced primarily by the liver and kidneys
Structure and Components of Platelets- Even without a nucleus, they are packed with structural proteins and chemical packets (granules) essential for clotting:
Actin and Myosin: Contractile proteins that allow the platelet to shrink and pull the edges of a wound together.
Alpha (ɑ) granules: Contain von WIllebrand factors (vWF), clotting facts, and Planet-Derived Growth Factors (PDGF) to stimulate tissue repair.
Dense (δ) Granules: Contain ADP (to recruit more platelets), serotonin (to constrict blood vessels) and calcium (essential for the clotting cascade).
Hemoglobin (Hb)
It is an iron-rich conjugated protein found in red blood cells. Its primary mission is to transport oxygen from the lungs to the body tissues and assist in bringing carbon dioxide back. It is a globular, tetrameric protein- meaning it is made of 4 subunit chains working together.

The Globin part: Protein chains synthesized by ribosomes. In a normal adult (HbA) it consists of 2 alpha (ɑ) and 2 beta (β) chains.
The Heme part: A non-protein ring structure (porphyrin) synthesized partly in the mitochondria. Nestled in the center of each heme ring is an iron atom in its ferrous state ().
Binding Capacity: Because there are 4 heme groups per hemoglobin molecule, one single molecule of hemoglobin can transport up to 4 molecules of oxygen.
The Allosteric Shift: Hemoglobin changes its shape based on whether it is holding oxygen:
T-state (Tense State): This is the deoxygenated form when subunits are tightly bound by ionic bonds making it hard for oxygen to bond.
R-state (Relaxed State): The "oxygenated" form. When the very first molecule forces its way onto a heme group, it ruptures those ionic bonds. The molecule relaxes, making it significantly easier for the next three molecules to snap into place. This is called cooperative binding.
Hemoglobin bound to oxygen is oxyhemoglobin, while it becomes deoxyhemoglobin when released. Hemoglobin with carbon monoxide is carboxyhemoglobin.
Hemostasis
It is a regulated physiological process that stops bleeding as blood clots, allowing the body to begin repairing the injury. It has 4 stages to the process.
Step 1: Autonomic pain nerve reflexes and chemicals released by traumatized endothelial cells and platelets (such as endothelin-on and thromboxane A2 enforce vasoconstriction where the walls of the smooth muscle contract to make the lumen smaller and minimize blood loss.
Step 2 (primary hemostasis): Platelets in the blood stick to the damaged tissue creating a temporary barrier (plug).
Step 3 (secondary hemostasis): The body initiates the coagulation cascade which is a step-by-step enzymatic activation of plasma proteins (clotting factors, mostly synthesized by the liver and denoted by Roman numerals). This turns the fragile platelet plug into a permanent clot.
Step 4: The platelet plug and a substance called fibrin form a solid, stable clot like bricks and mortar. During healing, normal tissue replaces this fibrin clot
Once the wound has healed underneath its stable seal and the clot is no longer needed, the clot is broken down by a process called fibrinolysis. This process elevates a protein in the blood called D-dimer.
Blood Clotting
Blood clotting is also known as coagulation and it is the 3rd step of hemostasis. It occurs immediately after the platelet plug forms and relies on the rapid chain reaction known as the coagulation cascade. When the injury exposes blood to protein outside vessel walls it triggers a domino effect among 12 specialized liver proteins (clotting factors). Each of the activated factors turns on the next one in the sequence. This chain reaction leads to the activation of an enzyme called prothrombin activator which converts inactive blood protein (prothrombin) into its active form (thrombin). The thrombin acts as the master enzyme needed to build the final structural seal. The thrombin changes a soluble, floating fluid protein called fibrogin into insoluble, sticky strands called fibrin. These long fibrin strands weave tightly across the temporary plug. The mesh traps passing red and white blood cells, securing the entire structure into a solid clot.
Conditions and Disorders that affect blood
Blood cancer
Starts when there is a mutation in the genes that tell your body how to make blood cells.This causes your body to make abnormal blood cells that multiply faster. Some blood cancers include leukemia, Lymphoma, and Myeloma.
Blood disorders
Noncancerous conditions where blood cells can’t do their job correctly. They range from harmless conditions to potentially life threatening ones. They include Anemias, Blood clotting disorders and bleeding disorders.
Anemia
It is when your blood has lower than normal amount of healthy blood cells or hemoglobin, reducing the body's ability to carry oxygen to tissues. Symptoms include fatigue, weakness, pale or yellowish skin, shortness of breath, dizziness or lightheadedness, cold hands and feet, irregular or rapid heartbeats. Causes of it are blood loss, lack of red blood cell production due to malnutrition, and high rates of cell destruction.
Types of anemia:
Iron Deficiency Anemia: The most common form caused by a shortage of iron which the bone marrow needs to make hemoglobin.
Vitamin Deficiency Anemia: Results from low levels of Vitamin B12 or folate, leading to abnormally shaped, low functioning red blood cells.
Anemia of Chronic Disease: Triggered by underlying medical conditions - such as kidney disease, cancer, or rheumatoid arthritis- that interfere with RBC production.
Aplastic Anemia: A rare, serious condition where the bone marrow stops producing enough of all types of blood cells.
Hemolytic Anemia: Occurs when red blood cells are destroying faster than the bone marrow is producing them.
It is diagnosed through the CBC or Complete blood count. Doctors look at the levels of hemoglobin and hematocrit, Mean Corpuscular Volume (MCV), and Reticulocyte count. To treat it, vitamin deficiencies must be treated through either dietary changes or oral tablets. Medical and hormonal therapies, blood transfusions, and Surgical Hemostasis are also options for more severe cases. If it is left untreated it could cause things from fatigue to hypoxia to heart failure.
Leukemia
Leukemia is a broad term for cancers of the body's blood-forming tissues, primarily originating in the bone marrow and lymphatic system. It occurs when acquired genetic mutations cause the bone marrow to produce an overabundance of abnormal, immature white blood cells (called blasts or leukemia cells). These dysfunctional cells crowd out healthy red blood cells, platelets, and normal leukocytes, undermining the body's ability to transport oxygen, clot blood, and fight off infections.
Acute vs. Chronic: Acute include immature, non-functional cells that multiply rapidly, causing severe symptoms within weeks and require immediate, aggressive therapy. Chronic involves more mature cells that accumulate slowly, often remaining sympathetic and unnoticed for years.
Lymphocytic vs. Myelogenous: : Lymphocytic types affect the lymphoid stem cells that normally mature into infection-fighting lymphocytes. Myelogenous types affect the myeloid stem cells that normally develop into red blood cells, platelets, and other types of white blood cells.
Acute Lymphoblastic Leukemia: (ALL): Most common type of pediatric cancer, when the bone marrow produces too many immature lymphocytes (lymphoblasts). Grows rapidly and requires immediate, aggressive treatment.
Acute Myeloid Leukemia (AML): Affects myeloid cells, which mature into red blood cells, platelets, and certain white blood cells. Most common in adults and causes a sudden drop in healthy blood cells, leading to quick onset of fatigue and bruising.
Chronic Lymphocytic Leukemia (CLL): A slow growing cancer affecting lymphoid cells. Common in older adults and abnormal cells build up over time despite looking mature.
Chronic Myeloid Leukemia (CML): A slow-growing cancer affecting the myeloid cells, typically driven by a specific genetic mutation called the Philadelphia chromosome. Mainly affects adults.
Symptoms include fatigue, infections, bruising & bleeding, swollen lymph nodes, and unexplained weight loss. Diagnosis is through the Complete Blood Count (CBC) test and treatment includes chemotherapy, radiation therapy, and immunotherapy, like other cancers.
Hemophelia
Hemophilia is a rare, typically inherited genetic bleeding disorder in which the blood does not clot properly due to a deficiency in specific clotting proteins. This impairment slows down secondary hemostasis, causing individuals to bleed for a significantly longer time after an injury, surgery, or dental work.
Types:
Hemophilia A: Known as classic hemophilia, this is the most common form and is caused by a deficiency in clotting factor VIII (8).
Hemophilia B: Often called Christmas disease, this rarer type occurs due to a lack or severe shortage of clotting factor IX (9).
Hemophilia C: A highly unusual form caused by a deficiency in clotting factor XI (11), which usually presents with milder symptoms.
The condition is primarily genetic and inherits through an X-linked recessive pattern, meaning the altered genes reside on the X chromosome. Because males inherit only one X chromosome (from their mother), they are disproportionately affected by the condition. Females inherit two X chromosomes; those carrying the gene on one chromosome are classified as carriers. Carriers usually do not display severe symptoms, though some experience abnormal bleeding or heavy menstruation. Around 30% of cases arise spontaneously from a new genetic mutation with no prior family history. In very rare instances, adults can develop "acquired hemophilia" if their immune system mistakenly attacks healthy clotting factors.
Treatment options include factor replacement therapy, prophylaxis, non-factor, hormone and gene therapies.
Sickle Cell Disease
Sickle cell disease (SCD) is a group of inherited genetic blood disorders characterized by abnormal hemoglobin, which causes red blood cells to become rigid, sticky, and shaped like a crescent or sickle. Unlike healthy, round red blood cells that move smoothly through blood vessels, these misshapen cells clump together and block blood flow, preventing oxygen from reaching tissues and vital organs.
Types: The specific form of SCD a person develops depends entirely on the abnormal hemoglobin genes they inherit from their parents:
HbSS (Sickle Cell Anemia): The most common and severe form where a person inherits two sickle hemoglobin "S" genes.
HbSC Disease: A usually milder version where a person inherits one hemoglobin "S" gene and one hemoglobin "C" gene.
Sickle Beta-Thalassemia: A variation where a person inherits one "S" gene alongside a gene for thalassemia, another type of inherited anemia.
Sickle Cell Trait (SCT): Occurs when a person inherits only one sickle gene and one normal gene. These individuals are carriers, rarely show symptoms, but can pass the gene to their children.
Key Symptoms and Complications - Symptoms usually manifest during early childhood, often starting around 5 to 6 months of age.
Vaso-occlusive Crises (VOC): Sudden, excruciating episodes of pain in the chest, back, joints, or limbs caused by blocked blood flow.
Chronic Anemia: Sickle cells break down prematurely and live for only 10 to 20 days instead of the normal 90 to 120 days, resulting in a constant shortage of red blood cells, severe fatigue, and weakness.
Infections and Organ Damage: Constant blockages can damage organs over time—particularly the spleen, which impairs the immune system and leaves patients vulnerable to life-threatening infections.
Acute Chest Syndrome: A life-threatening lung complication characterized by chest pain, fever, coughing, and difficulty breathing.
Management and Breakthrough Treatments
While patients historically managed the disease through hydration, pain medications, and routine blood transfusions, advanced therapeutic strategies have dramatically shifted the outlook for patients:
Disease-Managing Medications: Hydroxyurea is commonly prescribed to stimulate the production of fetal hemoglobin, which helps prevent red blood cells from sickling.
Bone Marrow Transplants: A stem cell transplant from a compatible donor offers a definitive cure, though it carries significant risks and finding a matched donor can be difficult.
Breakthrough Gene Therapies: Historically significant advancements, such as FDA-approved gene therapies, actively rewrite or modify a patient's genetic instructions to produce healthy hemoglobin, effectively offering new cure options.
Blood types
Blood types are determined by the presence or absence of certain antigens – substances that can trigger an immune response if they are foreign to the body. Blood transfusions and organ transplants depend on donors and recipients having compatible blood types. There are 4 main blood types: A, B, AB, and O. Your blood type is based on whether you have antigen A or B on your red blood cells. It is also determined based on a protein called the Rh factor. If you have this protein then your blood type is classified as positive (+), and if you don't have it then your blood type is classified as negative (-). This makes a total of 8 common blood types: A+, A-, B+, B-, AB+, AB-, O+, O-.
This is a compatibility chart, showing which blood types are compatible for blood donations/ transfusions and organ donations.
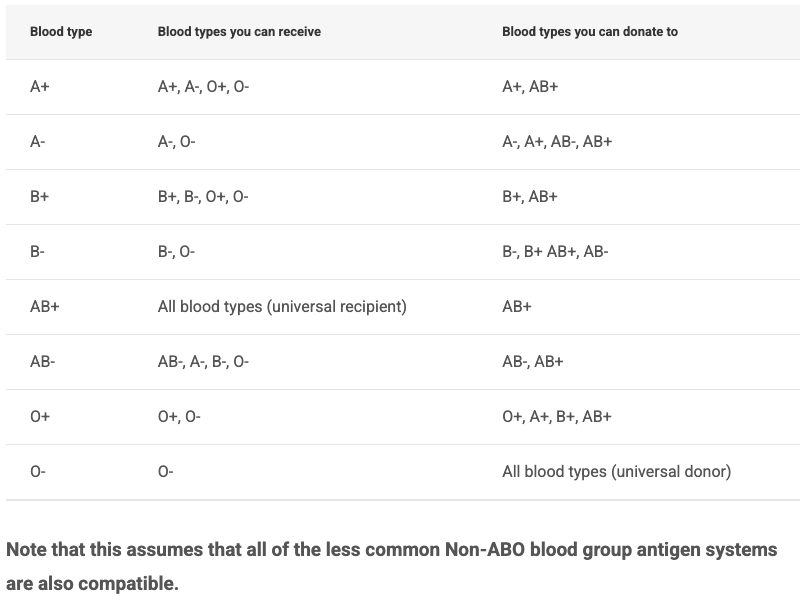
Blood types usually remain the same throughout your entire lifetime however it may change sometimes. Circumstances that can result in a change include a bone marrow transplant or leukemia. Not all changes in the blood types are permanent.
🫁 Respiratory System
Respiratory System 🫁
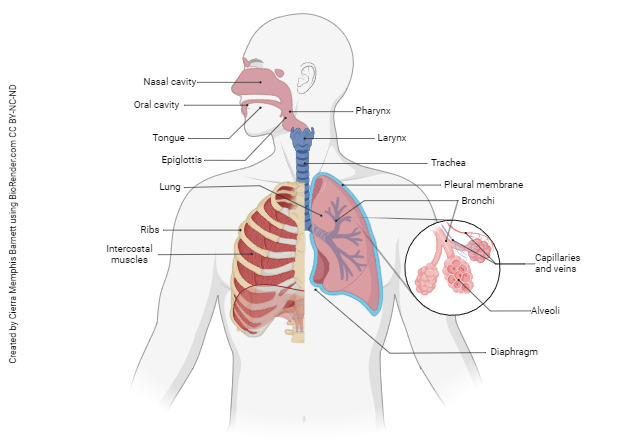
The respiratory system is a complex network of organs and tissues, primarily the lungs, airways (trachea, bronchi), and diaphragm, that enables breathing and gas exchange. Its main function is to deliver oxygen to the blood while removing carbon dioxide, supporting metabolism and maintaining pH balance.
Parts of the Respiratory System
Epoglottis- Small flap of cartilage; prevents food from entering trachea during swallowing
Bronchus- Two main branches from trachea, one to each lung.
Lung- Main organs of respiration, spongy tissue for gas exchange.
Cut end of Rib- Part of rib cage, protects lungs.
Heart- Pumps deoxygenated blood to the rest of the body.
Diaphragm- Large muscle below lungs, aids in breathing.
Bronchiole- Smaller branches of bronchi leading to alveoli.
Alveoli- Tiny air sacs at end of bronchioles, site of gas exchange.
Pleural fluid- Lubricating fluid between pleural membranes.
Pleural membranes- Double-layered membrane surrounding lungs.
Trachea- Windpipe; reinforced with cartilage rings, carries air to lungs.
Larynx- Voice box; contains vocal cords.
Path of Air through Respiratory System
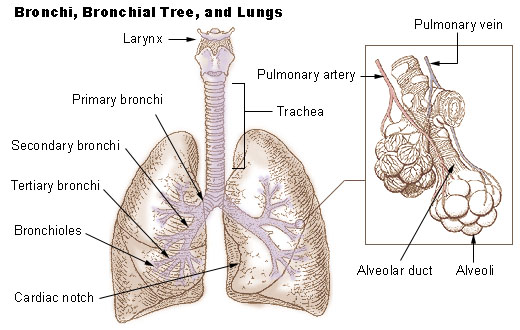
Air goes into your body through both your nose and your mouth, however the air you breath through your nose is warm and moist while the air through your mouth is cold and dry. This air makes it down the throat meeting two chambers or tubes which are the esophagus and the larynx (voicebox). The esophagus is for food and water while the larynx is for air, therefore a flap or valve known as the epiglottis covers the larynx, when you are consuming food to prevent choking. As oxygen travels down the larynx and trachea it enters the lungs and bronchial tree. The trachea splits into the left and right main bronchus, while the split in the middle is known as the Carina. The bronchi are known as the main (primary bronchi) which are broken down further into lobars (secondary bronchi), and then segments (tertiary bronchi), followed by bronchioles finally reaching Alveoli where the air drops of oxygen, takes in waste, makes a u-turn and leaves back the same way.
INHALING (INSPIRATION) & EXHALING (EXPIRATION)
The lungs cannot expand on their own; instead, they rely on changes in the surrounding thoracic cavity. This cavity is bound by the sternum (breastbone), 12 pairs of ribs (with the upper 7 pairs directly attaching to the sternum), and a muscular floor known as the diaphragm.
Inhalation (An Active Process): When you breathe in, the brain signals the respiratory muscles to contract. The diaphragm contracts and flattens downward, while the external intercostal muscles between the ribs contract to lift the rib cage upward and outward. This combined movement expands the volume of the thoracic cavity. According to Boyle's Law, this volume increase drops the internal pressure below atmospheric pressure, creating a vacuum that pulls air into the lungs and stretches open the elastic, elastin-rich alveoli. This active movement requires metabolic energy in the form of ATP.
Exhalation (A Passive Process): During quiet breathing, exhaling requires no active chemical energy. The diaphragm and intercostal muscles simply relax, causing the thoracic cavity to recoil and shrink. Driven by the elastic potential energy stored in the elastin proteins surrounding the alveoli, the lungs passively snap back to their original size. This decrease in volume increases internal air pressure, forcing air out of the lungs
Thermoregulation in Lungs
Thermoregulation in the lungs acts as a vital cooling mechanism. As the cold air is inhaled it reaches the alveoli which has blood flow next to it. The heat from the blood and blood cells transfers to the air until they reach equilibrium, making the air temperature equivalent to that of the body temperature. Therefore the air you inhale is colder than the air you exhale.
Alveole
Alveole are sacs at the ends of the bronchioles which are so small, they are only around 200-300 microns in diameter. Alveoli also have super thin membranes and have arteries or veins next to them meaning that they have blood flow next to them. The total alveoli’s internal surface area is around 75 square meters or between 70-100 square meters. On average a person has around 300-500 alveoli.
How air actually gets in and out of the lungs
As air goes through your bronchioles and alveoli the oxygen is basically allowed to cross the membrane and go to the veins where they are absorbed by the blood. Likewise the waste in the blood from the arteries or carbon dioxide leaves the blood and crosses the alveoli’s membrane joining the air on its journey back through the respiratory system out through either the nose or mouth. These arteries and veins that perform gas exchange are known as pulmonary arteries and veins as they go from the heart to the lung to the alveoli and back.
Right under the lungs is located the thoracic diaphragm. And the diaphragm kind of drives the process of respiration as mentioned in the “How does the lung change volume?”, section.
Respiratory Volumes and Capacities
This is the volume of gas in the lungs at a given time during the respiratory cycle. They are derived from the summation of different lung volumes and the average total lung capacity of an adult human male is about 6 liters. These values change based on depth of respiration, age, gender, ethnicity and body composition.
Tidal Volume (TV): Normal air inhaled/exhaled per breath = 500 ml, 10% of VC
Inspiratory Reserve Volume (IRV): Air inspired forcibly after TV = 2500-3000 ml
Expiratory Reserve Volume (ERV): Air expired forcefully after TV = 1000 to 1100 ml
Residual Volume (RV): Air remaining after forceful expiration = 1100 to 1200 ml
Inspiratory Capacity (IC): TV + IRV = 3000 to 3500 ml
Expiratory Capacity (EC): TV + ERV = 1500 to 1600 ml
Functional Residual Capacity (FRC): ERV + RV = 2100 to 2300 ml
Vital Capacity (VC): IRV + TV + ERV = 4500 to 5000 ml
Total Lung Capacity (TLC): VC + RV = 5000 to 6000 ml
Exchange of gases and Partial Pressure
The gas exchange is the exchange between oxygen and carbon dioxide in the respiratory system. Partial pressure is the pressure exerted by an individual gas in a mixture of gases. It is designated as for oxygen and for carbon dioxide. Gases always diffuse from an area of higher partial pressure to an area of lower partial pressure.
Partial Pressure values (mmHg)
Gas | Atmospheric Air | Alveoli (Lungs) | Deoxygenated blood | Oxygenated blood | Body Tissues |
|---|---|---|---|---|---|
159 | 104 | 40 | 95 | 40 | |
0.3 | 40 | 45 | 40 | 45 |
Transport of Oxygen
97% of oxygen is transported by the Red Blood Cells or is bound to the hemoglobin
Each hemoglobin (Hb) binds 4 oxygen molecules and this process is Oxhemoglobin → Hb + =
3% is dissolved in Plasma
Saturation is the state or condition when hemoglobin is unable to hold or carry any more oxygen.
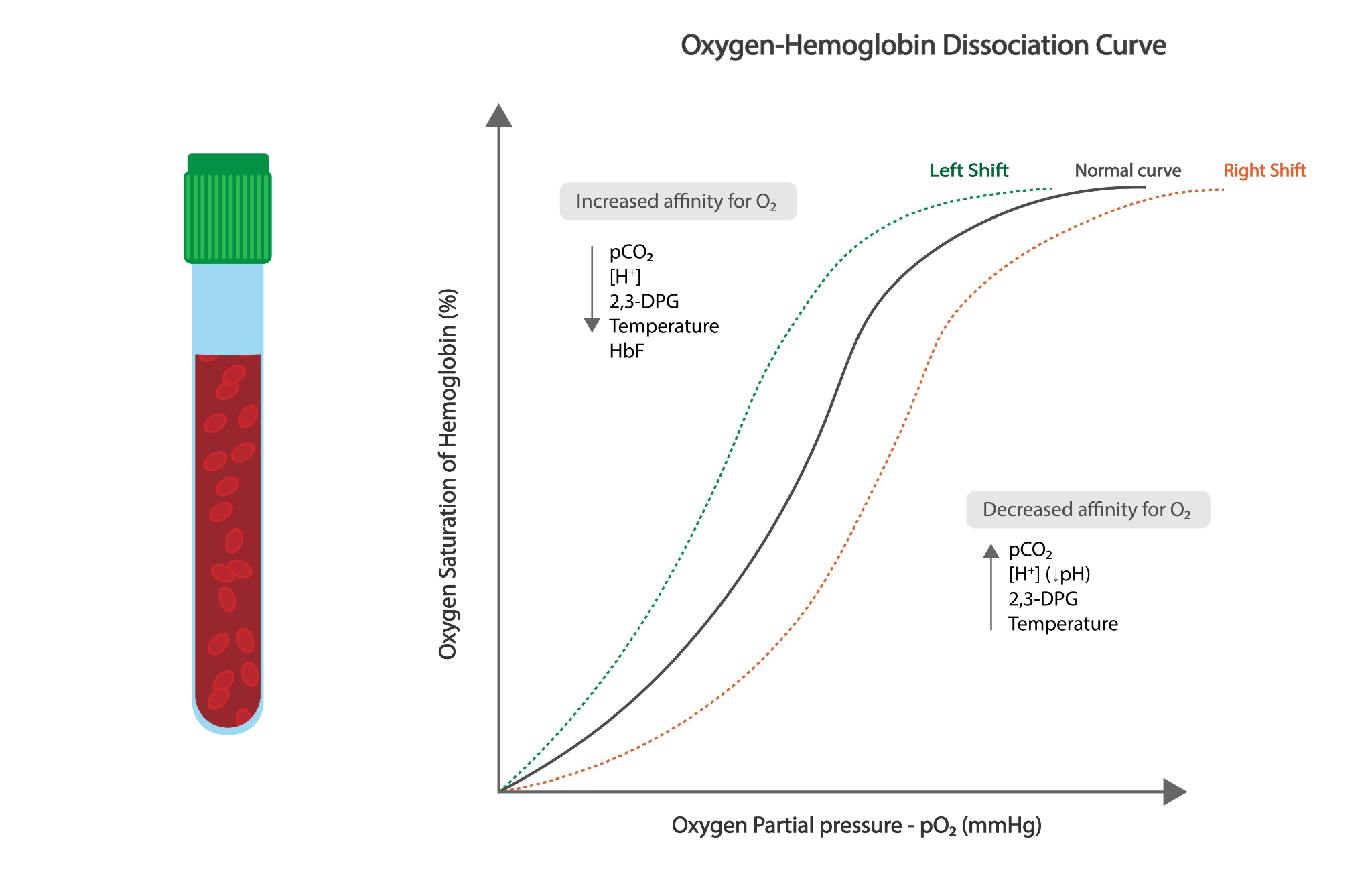
The curve is sigmoid due to cooperative binding. When the first oxygen molecule binds to a hemoglobin subunit, it alters the shape of the protein. This conformational change vastly increases the affinity(attraction) of the remaining subunits for oxygen. Conversely, the release of the first oxygen molecule makes it easier to release subsequent ones.
Right Shift: Decrease in partial pressure of oxygen, increased CO2, lower ph, increased temperature, or high 2,3-BPG. It is when oxygen is unloaded more easily to the tissues.
Left Shift: Decreased CO2, higher pH (alkaline), lower temperature, low 2,3-BPG, or fetal hemoglobin. It is when oxygen is held by the tiger by hemoglobin.
It favors oxygen release in high CO2, high , and high temperatures.
Bohr Effect: It is the rightward shift caused by an increase in CO2 and drop in blood ph. Active muscles produce lactic acid and carbon dioxide, which directly stimulates hemoglobin to drop off more oxygen exactly where it is needed most.
Transport of Carbon Dioxide
Carbon dioxide is transported by the blood from cells to the alveoli.
70 % as bicarbonate ()
20 to 25% as carbino-haemoglobin
7% is dissolved in plasma
Regulation of Respiration
It is coordinated by the neural mechanisms in the brain stem and chemical feedback loops.
Neural Control: drives automatic breathing
Medulla Oblongata- It acts as the primary peacemaker system. Generates the basic rhythmic pattern of breathing by sending nerve signals to the diaphragm and external intercostal muscles.
Pons- Modulates the activity of the medulla. It smoothens out the transition between inhaling and exhaling, preventing over-inhaling of the lungs.
Cerebral Cortex- Allows conscious, voluntary breathing overrides like speaking or breath-holding.
Chemical Controls- Chemoreceptors
Central chemoreceptors: Located in the medulla and are highly sensitive to pH and levels in cerebrospinal fluid. It reads fluctuations in the pH of cerebrospinal fluid. If rises, the fluid becomes more acidic, causing the brain to trigger deeper, faster breathing to blow off excess .
Peripheral chemoreceptors:: They are located in the aorta and carotid arteries. Detect drops in arterial blood (hypoxia), alongside spikes in and hydrogen ions . They are responsible for triggering rapid breathing when oxygen levels are dangerously low.
Disorders of respiratory system
Asthma- it is the allergy/inflammation of bronchi and bronchioles. It causes difficulty in breathing
Emphysema- It is the damage of the alveolar walls, and it results in reduced respiratory surface. The primary cause is smoking.
Cystic Fibrosis: A genetic disorder causing abnormally thick, sticky mucus to clog the airways.
Ventilation vs. Respiration
Ventilation is the physical mechanical act of moving air in and out where your body muscles contract, stretch or move.
Respiration is the biochemical process of the actual gas exchange. Oxygen moves from the alveoli into the blood stream, and carbon dioxide moves from the blood into the alveoli to be exhaled.
Bicarbonate Buffer System
It is a crucial homeostatic mechanism that maintains the pH of the blood and extracellular fluid between a strict range of 7.35 and 7.45. It uses a reversible chemical balance between carbon dioxide, carbonic acids, and bicarbonate ions to neutralize sudden changes in acidity or alkalinity.
Chemical Equation (two step reversible reaction):

How the System Responds
If blood becomes too acidic (high ): Excess hydrogen ions bind to bicarbonate () to form carbonic acid (). This breaks down into carbon dioxide and water which is exhaled by the lungs.
If blood becomes too alkaline (low ): Carbonic acid dissociates, releasing hydrogen ions () into the blood to lower the pH back to normal.
Organ System Regulation
Lungs: Control carbon dioxide levels. Rapid breathing expels more carbon dioxide, shifting the equation left to reduce blood acidity. Slow breathing retains carbon dioxide, shifting the equation to the right to increase acidity.
Kidneys: Control bicarbonate levels. They excrete or reabsorb bicarbonate into the blood and filter out excess hydrogen ions as needed.
Respiratory Diseases
Asthma
Asthma is a chronic respiratory condition characterized by the inflammation, swelling, and narrowing of the airways in the lungs, making it difficult to breathe.
Common symptoms include wheezing, coughing, shortness of breath, and chest tightness.
Common triggers include allergens, irritants, cold weather, physical exertion (exercise), and infections.
Treatment- though there are no proper cures it is manageable
Long-term control medications: Taken daily to reduce underlying airway inflammation and prevent attacks.
Quick-relief (rescue) inhalers: Short-acting bronchodilators used to rapidly open up airways during a sudden flare-up.
Asthma Action Plan: A personalized written guide created with your physician to track symptoms and adjust treatment.
COPD
Chronic Obstructive Pulmonary Disease (COPD) is a group of progressive, long-term lung conditions that block airflow and make it difficult to breathe. The disease destroys the elasticity of lung tissues and inflames airways, usually combining elements of both emphysema (damage to the tiny air sacs) and chronic bronchitis (constant airway inflammation).
Common symptoms include shortness of breath, a persistent cough, frequent coughing, chest tightness and chronic fatigue.
Primary causes include cigarette smoking (up to 75%), environmental exposure, and genetics (A rare genetic condition called alpha-1 antitrypsin (AAT) deficiency can trigger the disease even in non-smokers).
Its four stages are Mild, Moderate, Severe, Very Severe.
Treatments
Smoking Cessation: The single most effective action to stop further lung damage.
Medications: Inhalers containing bronchodilators to relax airways, and corticosteroids to lower inflammation.
Pulmonary Rehabilitation: A specialized program combining guided exercise, breathing strategies, and psychological support.
Oxygen Therapy: Portable supplemental oxygen devices used when blood oxygen levels become dangerously low.
Vaccinations: Staying current on flu, pneumonia, RSV, and COVID-19 vaccines protects fragile lungs from severe respiratory infections.
Pneumonia
Pneumonia is an acute respiratory infection that causes the tiny air sacs (alveoli) in one or both lungs to fill with fluid or pus, making breathing difficult and limiting oxygen intake. This condition ranges in severity from mild to life-threatening, particularly threatening older adults, infants, and individuals with underlying chronic illnesses.
Common symptoms include coughing, shortness of breath, fever, chest pain, fatigue, and confusion.
Causes
Pneumonia is classified by the specific germ causing the underlying lung infection:
Bacterial: The most prevalent form, frequently caused by Streptococcus pneumoniae. It can develop independently or strike after an upper respiratory infection.
Viral: Triggered by respiratory viruses like influenza, RSV, or SARS-CoV-2 (COVID-19). Viral cases are often milder but increase your risk of secondary bacterial infections.
Fungal: Less common and primarily found in individuals with weakened immune systems or chronic health issues.
Aspiration: Occurs when foreign material, such as food, liquids, or vomit, is inadvertently inhaled into the airways and triggers an infection.
Treatment
Effective treatment always depends on the definitive cause and severity of the condition:
Medications: Doctors prescribe specific antibiotics for bacterial types, while antivirals or antifungals are target-issued for other types.
Home Care: Prioritize ample rest, stay hydrated to loosen thick lung mucus, and utilize fever-reducers.
Prevention: Staying updated on targeted immunizations—such as pneumococcal, flu, and COVID-19 vaccines—greatly reduces risk. Proper handwashing and avoiding cigarette smoke are also vital safeguards.
Tuberculosis
Tuberculosis (TB) is a serious, highly contagious bacterial infection caused by Mycobacterium tuberculosis that primarily targets the lungs, but it is fully preventable and curable. The bacteria spread from person to person through microscopic droplets released into the air when an infected individual coughs, sneezes, talks, or sings. While it is a global public health concern, it requires prolonged or close contact to spread, meaning you are most likely to catch it from family members or coworkers rather than strangers.
Common symptoms of Active TB include severe prolonged cough, coughing up blood or deep mucus (sputum), persistent chest pain, unintended weight loss, chronic fatigue or muscle weakness, and unexplained fever or heavy night sweats.
Latent TB vs. Active TB Disease: An infection does not always make a person sick. The body can handle the bacteria in two distinct ways:
Latent TB Infection: The immune system walls off the bacteria, keeping them dormant. Individuals have no symptoms, do not feel sick, and cannot spread the bacteria to others. However, the infection can reactivate years later if the immune system weakens.
Active TB Disease: The bacteria multiply because the immune system fails to contain them. Individuals feel sick, experience severe symptoms, and can readily transmit the disease to others if it affects their lungs or throat.
Diagnosis and Screening:
TB Skin Test (Mantoux): A tiny amount of tuberculin fluid is injected just below the skin of the forearm. A trained provider must check the site 48 to 72 hours later for localized swelling.
TB Blood Test (IGRA): A single blood draw measures how your immune system responds to TB proteins. This method is highly specific and is not altered by prior TB vaccinations.
Treatment and Cure
Treating Latent TB: Taking a single antibiotic like isoniazid for several months destroys the dormant bacteria and prevents active disease from developing later.
Treating Active TB: Patients must take a combination of four standard antibiotics (including isoniazid and rifampicin) for 6 to 9 months. Skipping doses can cause the bacteria to mutate into dangerous drug-resistant strains.
Cell Biology
Cell Structure & Organelles
Tab 4
Mutations
A & G are purines while C, T & U are pyrimidines
Gene MUtations- change in a single nucleotide base pair.
SUbstitution
Transition: A purine is replaced by a purine (A↔G) or a pyrimidine is replaced by a pyrimidine (C↔T).
Transversions: A purine is replaced by a pristine or vice versa (ex: :A↔C)
Silent mutation: The base change still codes for the same amino acid due to the degeneracy of the genetic code. So the protein also ends up the same.
Missense mutations: The base change results in a different amino acid, so the protein structure also changes. Ex: Sickle cell anemia which is a mutation to the β-globin gene.
Nonsense mutation: The base change introduces a premature stop codon which ends the protein chain early usually making it nonfunctional.
Frameshift mutation- the number of nucleotide inserted or deleted is not a multiple of 3
Insertion: adding of one or more nucleotides
Deletion: removing one or more nucleotides
This alters every single amino acid after the site of mutation and has the biggest impact on protein. EX: Cystic Fibrosis, Duchenne Muscular Dystrophy
Chromosomal mutations- large scale structural changes in chromosome numbers; detectable via karyotyping.
Deletion: Loss of a chromosomal segment. Ex: Cri-du-chat syndrome
Duplication: Repetition of a chromosome segment, often leading to a chromosome family.
Inversion: 180 degree rotation of a chromosomal segment.
Paracentric-Does not include the centrometer
Pericentric- Includes the centrometer
Translocation: Shifting a segment to a non-homologous chromosome
Aneuploidy: Loss or gain of an individual chromosome, typically caused by nondisjunction in during meiosis
Polyploidy: Gain of entire sets of chromosomes. Common in plants, rare and lethal for humans.
Forward vs. Reverse Mutations
Forward: Changes the wild-type phenotype to mutant phenotype
Reverse (Reversion): Changes a mutant phenotype back to the wild-type phenotype
Spontaneous vs. Induced Mutations
Spontaneous: Occur naturally during DNA replication errors or tautomeric shifts.
Induced: Caused by environmental agents known as mutagens.
Physical Mutagens: UV rays (cause Thymine dimers) and X-rays (cause double-stranded breaks).
Chemical Mutagens: Base analogs (e.g., 5-Bromouracil), Alkylating agents (e.g., EMS), and Intercalating agents (e.g., Ethidium Bromide).
USMDO Master Checklist
USMDO Master Checklist
CELL BIOLOGY & BIOCHEMISTRY
Macromolecules
Monosaccharides
Disaccharides
Polysaccharides
Glycogen
Starch
Cellulose
Triglycerides
Phospholipids
Cholesterol
Steroid hormones
Amino acids
Peptide bonds
Primary protein structure
Secondary protein structure
Tertiary protein structure
Quaternary protein structure
DNA structure
RNA structure
Nucleotides
Cell Structure & Organelles
Nucleus
Nucleolus
Ribosomes
Rough ER
Smooth ER
Golgi apparatus
Mitochondria
Lysosomes
Peroxisomes
Vacuoles
Cytoskeleton overview
Cytoskeleton
Microtubules
Dynein
Kinesin
Cilia
Flagella
Actin
Myosin
Intermediate filaments
Cell Membrane & Transport
Phospholipid bilayer
Membrane proteins
Cholesterol in membranes
Membrane fluidity
Diffusion
Osmosis
Facilitated diffusion
Active transport
Sodium-potassium pump
Endocytosis
Phagocytosis
Pinocytosis
Receptor-mediated endocytosis
Exocytosis
Enzymes & Metabolism
Enzyme structure
Active site
Competitive inhibition
Noncompetitive inhibition
ATP
Catabolism
Anabolism
Cellular Respiration
Glycolysis
Pyruvate oxidation
Krebs cycle
Electron transport chain
Oxidative phosphorylation
ATP yield
NADH production
FADH2 production
Cell Signaling
Receptors
GPCRs
Receptor tyrosine kinases
Intracellular receptors
cAMP
IP3
DAG
Calcium signaling
Signal transduction pathways
Cell Cycle
Cell cycle phases
Cell cycle checkpoints
Mitosis
Cytokinesis
Meiosis
Crossing over
Independent assortment
Cell Death
Apoptosis
Necrosis
GENETICS & MOLECULAR BIOLOGY
Mendelian Genetics
Dominant inheritance
Recessive inheritance
Codominance
Incomplete dominance
Punnett squares
Dihybrid crosses
Linked genes
Sex-linked inheritance
DNA & Replication
DNA structure
Antiparallel strands
DNA replication
Helicase
Primase
DNA polymerase
Ligase
Leading strand
Lagging strand
Gene Expression
Transcription
RNA polymerase
Promoters
mRNA
tRNA
rRNA
Translation
Codons
Ribosomes
Gene Regulation
Operons
Transcription factors
Enhancers
Silencers
Epigenetics
Mutations
Point mutationsMissense mutationsNonsense mutationsSilent mutationsFrameshift mutationsInsertionsDeletions
Biotechnology
PCR
Gel electrophoresis
DNA sequencing
Recombinant DNA
CRISPR
Gene therapy
Microbiology
Bacterial structure
Gram-positive bacteria
Gram-negative bacteria
Viral structure
Lytic cycle
Lysogenic cycle
Retroviruses
Stem Cells
Totipotent stem cells
Pluripotent stem cells
Multipotent stem cells
Cancer Biology
Oncogenes
Proto-oncogenes
Tumor suppressor genes
Metastasis
Angiogenesis
p53
Ras
RB
APC
BRCA
HUMAN PHYSIOLOGY
Homeostasis
Homeostasis overviewNegative feedbackPositive feedback
Tissue Types
Epithelial tissue
Connective tissue
Muscle tissue
Nervous tissue
Digestive System
Digestive tract anatomy
Mouth
Esophagus
Stomach
Small intestine
Large intestine
Liver
Pancreas
Gallbladder
Digestion of carbohydrates
Digestion of proteins
Digestion of lipids
Absorption
Parietal cells
Chief cells
Goblet cells
Cardiovascular System
Heart anatomyBlood flow pathwayCardiac cycleCardiac outputStroke volumeBlood pressureRAAS systemReninAngiotensin IIAldosteroneErythropoietin
Blood
Red blood cellsWhite blood cellsPlateletsHemoglobinHemostasisBlood clotting
Respiratory System
Respiratory anatomyAlveoliGas exchangeOxygen transportCarbon dioxide transportBicarbonate buffer systemVentilationRespiratory regulation
Renal System
Kidney anatomy
Nephron anatomy
Glomerulus
Proximal tubule
Loop of Henle
Distal tubule
Collecting duct
Filtration
Reabsorption
Secretion
ADH
Aldosterone
Water balance
Endocrine System
Hypothalamus
Pituitary gland
Growth hormone
TSH
ACTH
ADH
Oxytocin
Thyroid gland
T3
T4
Parathyroid hormone
Pancreas
Insulin
Glucagon
Adrenal cortex
Cortisol
Aldosterone
Adrenal medulla
Epinephrine
Hormone feedback loops
Nervous System
Neuron anatomy
Resting membrane potential
Action potential
Synapses
Acetylcholine
Dopamine
Serotonin
GABA
Glutamate
Sympathetic nervous system
Parasympathetic nervous system
Immune System
Innate immunity
Adaptive immunity
Neutrophils
Macrophages
Dendritic cells
Eosinophils
Mast cells
B cells
T cells
Antibodies
MHC
Cytokines
Histamine
Inflammation
Vaccines
Reproductive System
Male reproductive anatomy
Testes
Epididymis
Vas deferens
Female reproductive anatomy
Ovarian cycle
Menstrual cycle
FSH
LH
Estrogen
Progesterone
Musculoskeletal System
Muscle contraction
Sliding filament theory
Skeletal muscle
Bone remodeling
Calcium regulation
Integumentary System
Skin layers
Skin functions
HUMAN DISEASE
Genetic Disorders
Down syndrome
Edwards syndrome
Turner syndrome
Klinefelter syndrome
Williams syndrome
Cystic fibrosis
Sickle cell disease
Endocrine Diseases
Type 1 diabetes
Type 2 diabetes
Graves disease
Hashimoto thyroiditis
Diabetes insipidus
Cardiovascular Diseases
HypertensionAtherosclerosisMyocardial infarctionHeart failure
Blood Disorders
AnemiaLeukemiaHemophiliaSickle cell disease
Respiratory Diseases
AsthmaCOPDPneumoniaTuberculosis
Gastrointestinal Diseases
GERD
Peptic ulcer disease
Crohn disease
Ulcerative colitis
Renal Diseases
Kidney failure
Nephrotic syndrome
Diabetes insipidus
Neurological Diseases
Parkinson disease
Alzheimer disease
Multiple sclerosis
Epilepsy
Autoimmune & Immune Disorders
Lupus
Rheumatoid arthritis
Allergies
Immunodeficiencies
Infectious Diseases
HIV/AIDS
Influenza
Hepatitis
Cholera
Pertussis
Tetanus
Botulism
Tuberculosis
Cancer
Hallmarks of cancer
Oncogenes
Tumor suppressors
Metastasis
Cancer therapies
HIGHEST VALUE TOPICS
Endocrine physiology
Cardiovascular physiology ✓
Immune system
Cell signaling
Cancer biology
Genetics disorders
Respiratory physiology✓
Kidney physiology
Infectious diseases
Biotechnology