Ch. 14 Later life: Physical challenges of old age Cognitive dev
Tracing Physical Aging
normal aging- Universal, often progressive signs of physical deterioration intrinsic to the aging process.
normal aging shades into disease, then disability, and, finally death
Three basic principles program this inevitable process of body decay.
Principle #1: Chronic Disease Is Often Normal Aging “At The Extreme”
bone loss and atherosclerosis are perfect examples
these changes produce familiar later-life illnesses, osteoporosis and heart disease.
chronic disease: Health disorders that do not ease but persist and often get worse over time.
arthritis is one of the top-ranking chronic illnesses in later life
many y age-related diseases are not fatal
They interfere with the ability to function in the world.
activities of daily living (ADL) problems: Difficulty in performing everyday tasks that are required for living independently. ADLs are classified as either basic or instrumental.
Principle #2: ADL Impairments Are a Serious Risk During the Old-Old Years
Years ADL limitations come in two categories
Instrumental ADL problems refer to trouble performing tasks important for living independently, such as cooking and cleaning.
Basic ADL limitations refer to problems with fundamental self-care activities, such as standing or getting to the bathroom or feeding oneself.
When people have these severe disabilities, they typically need full-time caregiving help.
old-old years are when these problems really strike
Half of all U.S. adults over 85 living in their homes have instrumental ADL difficulties.
Basic ADL limitations affect 1 in 10 people over 75
Principle #3: The Human Lifespan Has a Defined Limit
aging has a fixed end
In September 2019 worldwide, there were roughly 35 documented “supercentenarians” — people who had lived until 112 or beyond
More people than ever are surviving past a century
Can We Live to 200?
The key is what one biologist calls “undernutrition without malnutrition.”
Research study: The animals are restricted to less food but given a nutritionally rich diet.
Calorie restriction is an all-purpose anti-ager, enhancing everything from glucose metabolism to cardiac function
obesity, especially via its side effect of diabetes (impaired sugar metabolism), causes every organ from our eyes, to heart, to kidneys to prematurely break down.
Although intermittent fasting can slow many risk factors for chronic disease, it’s unclear if this regimen can push back the biological limit of human life.
Why extending the maximum lifespan in the near future is an unrealistic dream?:
Aging results from multiple genetic timers and metabolic processes that accumulate over time.
No single intervention can halt aging entirely due to its complex nature.
Stem-Cell Research:
Advances in technology, like stem-cell research, promise cellular regeneration for diseases like Parkinson's.
However, these technologies can only temporarily delay the onset of other age-related conditions, such as cancer.
Analogy to Old Cars:
Human bodies are comparable to old cars, where replacing defective parts only delays the inevitable systemic failure
Our body’s evolutionary expiration date is naturally set well below a century, because natural selection promotes living through grandparenthood.
even in the most affluent nations, the probability of a twentyfirst-century newborn living to 100 remains low.
extending the maximum lifespan is far harder than the breakthroughs that allowed us to reach later life.
As socioemotional selectivity theory beautifully points out, knowing our life is near its end motivates us to savor every moment.
Religious young people, researchers find, reject life extension on spiritual grounds: “Only God can give and take away life”
Socioeconomic Status, Ethnicity, Aging, and Disease
socioeconomic status predicts how long we live comes from scanning the huge life expectancy gaps around the world: Babies born in the Central African Republic can expect, on average, to survive to age 53
Infants lucky to emerge from the womb in Monaco have a 50/50 chance of living almost 40 years longer — to age 89.5
→ mirrored by a socioeconomic health gap: The worldwide disparity between the health of rich people and poor people.
in 2014, this gap between the most impoverished (lowest 5 percent) and richest (top 5 percent) of adults was a decade for women and 15 yrs for men.
this split widen as twenty-first-century income inequalities increased
Between 2001 and 2014, life expectancy rose by close to three years for the richest 5 percent of Americans
. From 2015 to 2018, for the first time in U.S. history, life expectancy at birth declined
life expectancy did rise slightly in 2019, but then dipped again in the first half of 2020 when the coronavirus hit
→ both male and female lost an entire year of expected life
men bear the brunt of this life-destroying barrier to constructing a competent middle-class life.
social-class differences in health appear well before old age
for disadvantaged adults, so called old-age limitations oen appear in midlife
ex. low birth weight, linked to poverty and race, is epigenetically associated with premature heart disease and earlier death
COVID stats: in 2020, Native Americans, Hispanic Americans, and African Americans were nearly twice as likely to contract this disease
→ their COVID hospitalization rates were four times higher than White Americans due to living in low-efficacy neighborhoods, not having enough money, lack of access to healthful foods
despite having lower median incomes, Hispanic Americans outlive White Americans by almost three years
Hispanic Paradox: The fact that, although generally less affluent, Hispanic Americans statistically outlive White Americans.
→ hispanics often live embedded in nurturing multigenerational families
Chetty’s research: if low-income people live in economically diverse neighborhoods, particularly communities boasting a higher fraction of college graduates, they live longer than we might expect
our level of education in itself predicts how quickly we age
Telomere shortening is an overall benchmark of body aging, as it shows that a cell has reached senescence and can no longer divide
researchers found that high school graduates had shorter telomeres than people who attended college, a difference that was particularly striking among Black men
→ going to college predicts having a longer life!
Gender, Aging, and Disease
the main reason for this gap can be summed up in one phrase: fewer early heart attacks
Illnesses of the cardiovascular system (the arteries and their pump, the heart) are the top-ranking killers for both women and men
heart disease and stroke account for roughly 1 in 3 deaths
men are roughly twice as likely as women to die of heart attacks in midlife
premature heart attacks means that men tend to “die quicker and sooner.” For women, the pattern is “surviving longer but living frailer
During their twenties, thirties, and forties, only women experience the physical ailments related to pregnancy and menstruation.
→ have higher rates of arthritis, vision impairments, and obesity ( illnesses that produce ADL problems) but don’t lead to death.
health span: The number of years people can expect to live without ADL problems.
Lifespan Strategies to Extend LaterLife Health:
Focus on children: prevent premature births and to make inroads in child poverty, as the seeds of poor health emerge during our earliest years.
Focus on constructing caring communities: Chetty’s research underlines the health benefits efficacious communities produce. close attachments are the glue that has allowed our species to survive (and thrive).
Sensorimotor Changes (Vision)
By the late forties and fifties, people have trouble seeing close objects.
Presbyopia, the term for age-related difficulties with seeing close objects, is a classic tip-off, like gray hair, that people are no longer young.
Older people have particular trouble seeing in dim light
They cannot distinguish certain colors as clearly or see visual stimuli as distinctly as before
Presbyopia is caused by changes in a structure toward the front of the eye called the lens
→ A transparent, disk-shaped structure in the eye that bends to allow us to see close objects.
As people reach midlife, the transparent lens thickens, develops impurities, and can no longer bend.
limits vision in dimly lit places where people need as much light as possible to see.
older people view the world through a cloudier lens, they see far less well when a beam of light shines in their eye
this could lead to a cataract, a familiar late-life chronic condition (curable)
Our Bridge to Others: Hearing
Hearing loss is associated with physical and cognitive decline
→ can provoke depression
Poor hearing robs us of understanding language, our bridge to other minds.
→ hearing difficulties are common in later life
males are several times more likely than females to develop hearing problems in midlife
The main reason is that age-related hearing loss has an environmental cause: exposure to noise
Men are more likely to be construction workers, ride motorcycles, and play in metal bands
male or female — who spends decades working in noisy milieus is virtually destined to have hearing impairments after age 65
Presbycusis: the characteristic age-related hearing loss — is caused by the atrophy or loss of the hearing receptors, located in the inner ear
→ affect people’s ability to quickly process speech
older people have special difficulty hearing consonants — for instance, mistaking the word time for dime
. The receptors coding high-pitched tones are most vulnerable
Elderspeak: Communication style used when an older person looks frail and impaired, involving talking loudly and slowly, as if to a baby.
→ We use simpler phrases and grammar and employ infantile “loving” words, such as darling, that we would never adopt when addressing a “real” adult.
for the future: avoid high noise environments and cover your ears when passing by noisy places
Motor Performances
Being slow naturally puts older people out of sync with the physical world
age-related slowing alone may help explain why our time oriented society has such negative prejudices against older adults
The slowness is mainly caused by the loss in information-processing speed that starts decades earlier, in young adulthood
→ slowed reaction time: The speed at which a person can respond to a stimulus.
Age changes in the skeletal structures propelling action compound the slowness:
osteoarthritis- the joint cartilage wears away, making everything from opening a jar to running for the bus an endurance test
osteoporosis- the bones become porous, brittle, and fragile and are prone to break. ( women are more susceptible to this disease of euro and asian descent)
→ slender women have frailer, smaller bones which can break at the slightest pressure and cannot knit themselves back together ex. hip fractures are a special danger
falling is a fear that older adults share worldwide
older drivers are the age group most vulnerable to dying in crashes
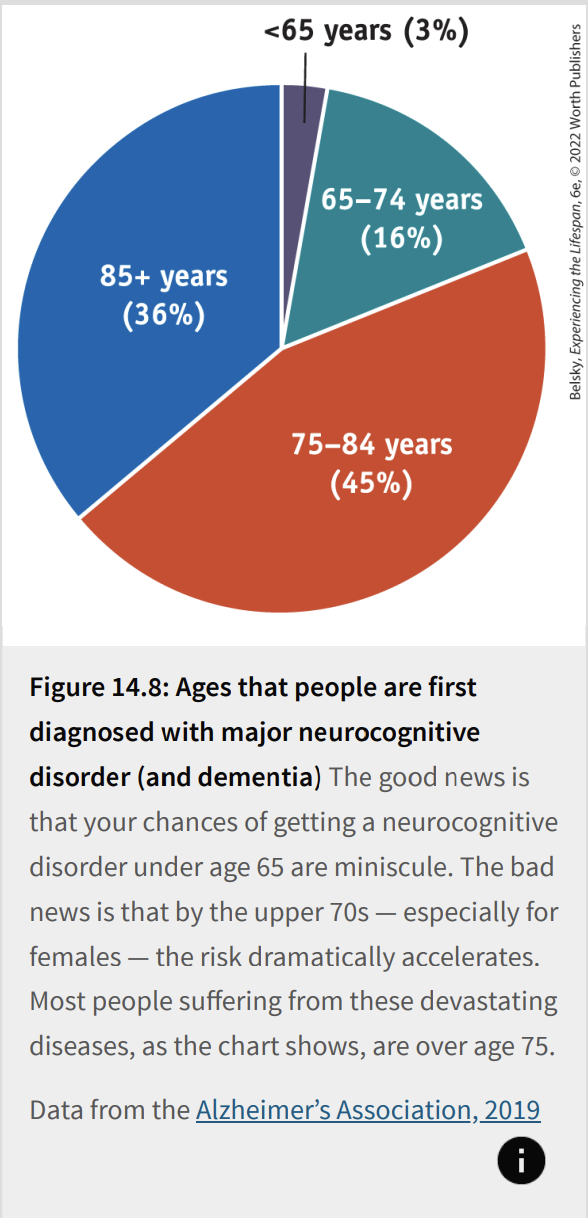
Neurocognitive Disorders (and Dementia)
Major neurocognitive disorder (and dementia) is the umbrella term for a host of illnesses that produce serious, progressive cognitive losses.
→ major neurocognitive disorder (and dementia) General terms for any illness involving serious, progressive cognitive decline that interferes with a person’s ability to live independently. (A minor neurocognitive disorder is the label for a less severe impairment in memory, reasoning, and thinking that does not compromise independent living.)
these diseases involve the total erosion of our personhood
Abstract reasoning becomes difficult.
People cannot think through options when making decisions
People are unable to name common objects, such as a shoe or a bed.
people may be unable to speak or move
infectious diseases such as pneumonia or coronavirus often lead to death.
The Dimensions
The brain changes often set in years before the person shows palpable signs of mental loss
can be hard to define when the illness begins
The deterioration progresses at different rates from person to person and varies depending on the specific disease.
People survive an average of 4 to 8 years after being diagnosed with these conditions; but the time from diagnosis to death can be as long as 20 years
→ these impairments are typically illnesses of advanced old age
Over age 85, 1 in 3 people is destined to develop memory problems this severe.
since 1988, a person’s risk of getting this diagnosis at any given age declined a remarkable 13 percent per decade
→ however, because more of us are living longer, and the huge baby boom cohort has flooded into later life, the number of people with these severe problems is destined to sharply increase
it cost the United States $290 billion. By 2050, the projected cost is apt to be $1 trillion or more
The Main Causes
Vascular neurocognitive disorder (also called vascular dementia) involves impairments in the vascular (blood) system, or network of arteries feeding the brain.
caused by multiple small strokes
Alzheimer’s disease directly attacks the core structure of human consciousness, our neurons.
With this illness, the neurons wither away and are replaced by strange wavy structures called neurofibrillary tangles and senile plaques (bullet-built structures that replace normal neurons, characteristic of Alzheimer’s disease)
Targeting the Beginnings: The Quest to Nip Alzheimer’s in the Bud
The main front in the war to prevent Alzheimer’s centers on a protein called amyloid, a fatty substance that is the basic constituent of the senile plaques
Most scientists believe the accumulation of a toxic form of amyloid produces a compound called tau (p-tau) that internally sets off the tangles and neural decay (
Having other ADL problems plus moderate memory loss strongly raises the chance of soon progressing to full-fledged disease.
Adults diagnosed with subjective cognitive decline and mild cognitive impairment are centrally important in this effort.
→ These people either believe they have suffered dramatic memory changes or, in mild cognitive impairment, show significant learning problems on neuropsychological tests
more than half of all people diagnosed with mild cognitive impairment develop Alzheimer’s within the next five years
most researchers believe that the number one candidate for an anti-Alzheimer’s strategy is exercise
at a minimum, going to the gym or walking will help with the vascular component of this illness
Options and Services for Frail, Elderly People
In Japan, nursing homes are common.
In China, the need for women to work full time makes it difficult to provide hands-on care when the oldest generation needs help with daily life
The Scandinavian countries offer our best examples of elder care that advanced Western societies can provide
In Sweden, Norway, and Denmark, government-funded home health services swing into operation to help impaired older people “age in place” (for them to stay in their own home)
Scandinavian older adults don’t need to face that anxiety-ridden question: “Can I afford to get help?”
Alternatives to Institutions in the United States
Medicare pays only for services defined as cure-oriented
→ does not cover help with activities of daily living — the very services such as cooking or cleaning or bathing that keep people out of a nursing home when they are having trouble functioning in life
A continuing-care retirement community is a residential complex that provides different levels of services, from independent apartments to nursing home care. Residents arrive in relatively good health and get the appropriate type of care as their physical needs change
An assisted-living facility is designed for people who have ADL limitations, but not impairments that require full-time, 24-hour care. offers care in a less medicalized, more homey setting. Residents have private rooms; they can keep the cherished mementos that allow them to live a dignified life.
Day-care programs are for older people who live with families. provides activities and a place for an older person to go when family members work. invaluable for people with early Alzheimer’s disease
Home health services help people age in place (at home). Paid caregivers come to the person’s house to cook, clean, and help with personal care activities such as bathing
Nursing Home Care
Nursing homes, or long-term-care facilities, provide shelter and services to people with basic ADL limitations, individuals who require 24 hr caregiving help.
main risk for entering these institutions is being very old, average age is late 80s
females live sicker into advanced old age, women make up the vast majority of residents in long-term care.
Evaluating Nursing Homes
Nursing homes may offer perks from beauty parlors to private rooms.
Nursing home residents are barred from leaving the facility unless relatives check them out; they are subject to random checks from caregivers
They do not have input regarding when to eat (or what to eat)
They can’t just decide to lie in bed or refuse to take a medicine
Their every action is dependent on the workers providing care
In one poll from a Swiss nursing home, 2 in 3 staff members reported being the target of a resident’s verbal aggression within the previous two weeks
Sexual harassment is also an uncomfortable risk when nursing home workers need to bathe cognitively impaired residents and wash their private parts.
Nursing home aides, like their counterparts in day-care centers, earn poverty-level wages.
→ The main hands-on care provider in a nursing home who helps elderly residents with basic ADL limitations