Steroids
Corticosteroids
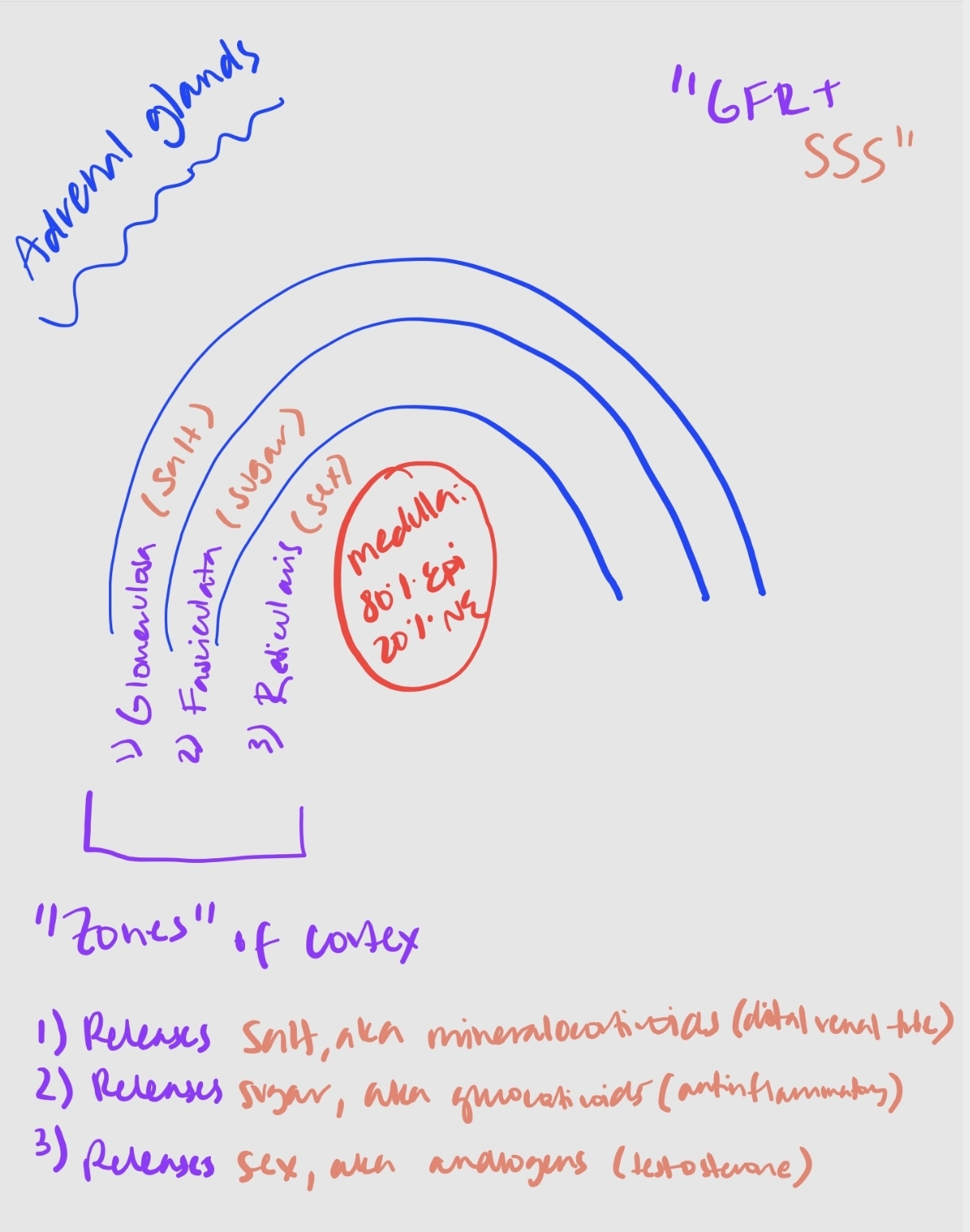
The actions of corticosteroids are classified according to the potencies of their compounds to:
Mineralocorticoid Effect: Evokes distal renal tubular reabsorption of sodium in exchange for potassium ions.
Glucocorticoid Effect: Produces an anti-inflammatory effect.
Critical for maintaining homeostasis during severe stress.
Mechanism of Action:
Glucocorticoids:
Produced in the zona fasciculata of the adrenal cortex.
Attach to cytoplasmic receptors to enhance or suppress transcription of DNA.
Leads to changes in protein synthesis.
Inhibit cytokine secretion via posttranslational effects.
Mineralocorticoids:
Produced in the zona glomerulosa of the adrenal gland.
Regulate water and electrolyte balance.
**main one is Aldosterone
Receptors present in distal renal tubules, colon, salivary glands, and hippocampus.
Cortisol
Cortisol is a stress hormone produced in the zona fasciculata of the adrenal cortex. It is the most potent endogenous glucocorticoid produced.
Controls body homeostasis, stress, and immune responses.
Aids in the metabolism of fats, proteins, carbohydrates.
Increases blood glucose levels, providing additional energy for muscles.
Released by the adrenal gland but regulated by the pituitary gland.
Cortisol Levels:
Maximal levels occur just before awakening (6-9 am).
Lowest levels between 11 pm to 1 am.
Stress activates the hypothalamic-pituitary-adrenal (HPA) axis, increasing serum ACTH and cortisol levels.
High Cortisol Level Symptoms:
High blood pressure.
Fatigue.
Erectile dysfunction.
reduced sex drive
weakened immune response
weight gain
hyperglycemia
Hyperglycemia is the most common s/e of giving steroids in the OR
insomnia
poor concentration/memory
Low Cortisol Level Symptoms:
Sugar and salt cravings.
Decreased sex drive.
Anxiety.
Weight gain.
Insomnia
Irritability.
Bone and muscle loss.
Depressed mood.
fatigue
Exogenous Glucocorticoids
Purpose of Administration: Have anti-inflammatory and immunosuppressive properties.
Anti-inflammatory Properties:
Glucocorticoids reduce both early and late stages of inflammation.
Suppress initial vasodilation and infiltration of leukocytes, leading to decreased pain.
Immunosuppressive Properties:
Used to treat diseases associated with an overactive immune system, such as:
Allergic reactions (e.g., angioneurotic edema, asthma).
Collagen-vascular disorders (e.g., lupus erythematosus).
Eye diseases (e.g., acute uveitis).
Gastrointestinal diseases (e.g., inflammatory bowel disease).
Hematologic disorders (e.g., acquired hemolytic anemia).
Systemic inflammation and infections.
Inflammatory conditions of bones and joints (e.g., arthritis).
Neurologic disorders (e.g., cerebral edema).
Organ transplants (to prevent rejection).
Pulmonary diseases (e.g., aspiration pneumonia).
Renal disorders (e.g., nephrotic syndrome).
Skin diseases (e.g., atopic dermatitis).
Thyroid diseases (e.g., malignant exophthalmos).
Immunosuppression occurs via three mechanisms:
Direct the development of undifferentiated T helper cells
Inhibit synthesis of interleukins 1 and 2
Induce T cell apoptosis
Exogenous Corticosteroids
Administration Routes: Topical, oral, intravenous, intramuscular, inhaled, intranasal, rectal, and ophthalmic.
Metabolism:
Metabolized by the liver.
Excreted by the kidneys.
Side Effects:
Redistribution of fat from extremities to face and trunk.
Acne.
Insomnia.
Increased appetite.
Increased gluconeogenesis.
Opportunistic infections.
Psychosis.
Long-term high doses may cause iatrogenic Cushing's syndrome.
Examples of synthetic corticosteroids:
Short Acting (<12 hours):
Hydrocortisone.
Cortisone.
Intermediate Acting (12-36 hours):
Prednisone.
Prednisolone.
Methylprednisolone.
B-prednisone
Triamcinolone.
Paramethasone.
Long Acting:
Betamethasone.
Dexamethasone (Decadron).
Dexamethasone (Decadron)
Glucocorticoid steroid that is a fluorinated derivative of prednisolone. NO mineralocorticoid activity.
Common Dosages:
4 mg for PONV (given at beginning of surgery since takes a little bit)
4-12 mg for airway edema (typically 10 mg).
10 mg for head and back surgeries.
**0.75 mg is equivalent to 20 mg of cortisol.
Uses in Anesthesia:
Postoperative nausea and vomiting (PONV).
Airway edema.
Cerebral edema.
Pain management.
Anaphylaxis.
Epidural steroid injection/Regional nerve blocks (prolongs duration of block)
Hydrocortisone (Solu-Cortef)
Commonly used for “Stress Dose” in patients with recent chronic steroid history (>2 weeks).
Large amount of mineralocortoid activity.
Dosage: 100 mg.
Methylprednisolone (Solu-Medrol)
Glucocorticoid with minimal (but still some) mineralocorticoid activity.
5 times more potent than hydrocortisone.
Uses:
Anti-inflammatory.
Respiratory support (short-term to inhibit bronchoconstriction).
Treat or prevent allergic reactions.
Spinal shock.
Dosage:
Standard: 40-60 mg IV q6 hours.
Common anesthesia dose: 125 mg (not frequently used due to hyperglycemic and immunosuppressive effects).
4 mg has an anti-inflammatory effect equivalent to 20 mg of cortisol.
Prednisolone
Often used as the sole treatment for adrenocorticoid insufficiency.
Predominant glucocorticoid activity; minimal mineralocorticoid activity.
Triamcinolone (Kenalog)
Corticosteroid with reduced mineralocorticoid effect compared to prednisolone.
Commonly used for epidural steroid injections off-label.
Side Effects:
May cause mild diuresis initially with sodium loss.
Might induce edema in patients with decreased GFR
Can lead to unusual side effects: skeletal muscle weakness, anorexia, and sedation.
Steroid Main Points
25 mg Cortisone Equivalents:
20 mg Hydrocortisone
4 mg Methylprednisone
5 mg Prednisolone/prednisone
0.75 mg Dexamethsone
Most to least anti-inflammatory effects:
Aldosterone (0)
Cortisone (0.8)
Cortisol (1)
Prednisolone/prednisone (4)
Methylprednisone (5)
Dexamethasone (25)
Perioperative Management
Patients receiving glucocorticoids for a limited time should continue their medication as prescribed, as the likelihood of short-term use affecting the HPA (hypothalamus-pituitary-adrenal) axis is minimal.
For patients on glucocorticoids for an extended period, the perioperative management with a “stress dose” of steroids remains controversial.
Dosing Recommendations:
For Minor Surgery (e.g., inguinal hernia repair): Hydrocortisone 100 mg intravenously at induction + maintenance dose (approx. 20 mg/d).
For Major Surgery (e.g., chest or abdominal surgery): Hydrocortisone 100 mg at induction + 100 mg every 8 hours for 24 hours.
Nagelhout has the following recs:
Minor stress is 25 mg hydrocortisone
Moderate stress is 50-75 mg hydrocortisone
Major stress (e.g., CABG) is 100-150 mg hydrocortisone
HPA Response Assessment:
Patients currently taking steroids < 10 mg/d: Assume normal HPA response.
Patients currently on steroids > 10 mg/d may have a compromised HPA response and need coverage.
Nagelhout says patients taking >20 mg/day of prednisone for >3 weeks have a suppressed HPA axis and require stress-dose steroids
Patients who stopped taking steroids < 3 months ago may have a compromised HPA response, while those who stopped > 3 months ago can assume normal HPA response.