joints of lower limb😭
Joints of the Lower Limb
Hip Joint
Location: Between the lower limb and the pelvic girdle.
Type: Strong and stable multiaxial ball and socket type of synovial joint.
Articulation: Head of the femur (the ball) articulates with the acetabulum (the socket).
Function: Designed for stability over a wide range of movement.
Articular Surfaces of the Hip Joint
Articulation Details:
The round head of the femur articulates with the cup-like acetabulum of the hip bone.
Articular cartilage covers all of the femoral head except for the fovea for the ligament of the femoral head.
Acetabulum Composition:
Formed by three bony parts.
The acetabular rim is a semilunar articular part covered with articular cartilage, known as the lunate surface.
Acetabular Features
Acetabular Notch: Missing inferior segment of the circle.
Acetabular Labrum:
A fibrocartilaginous rim attached to the margin of the acetabulum.
Increases the acetabular articular area by nearly 10%.
Transverse Acetabular Ligament: Bridges the acetabular notch and is a continuation of the acetabular labrum.
Non-Articular Part: Acetabular fossa, formed by the ischium.
Hip Joint Ligaments
Fibrous Layer: Forms ligaments of the hip joint from the pelvis to the femur.
Iliofemoral Ligament:
Strong, Y-shaped ligament located anteriorly and superiorly.
Attaches to the anterior inferior iliac spine (AIIS) and the acetabular rim proximally, and the intertrochanteric line distally.
Known as the body’s strongest ligament; prevents hyperextension of the hip joint during standing by screwing the femoral head into the acetabulum.
Other Ligaments
Pubofemoral Ligament:
Located anteriorly and inferiorly.
Originates from the obturator crest of the pubic bone and merges with the fibrous layer of the joint capsule.
Prevents overabduction of the hip joint.
Ischiofemoral Ligament:
Located posteriorly.
Weaker than the iliofemoral and pubofemoral ligaments.
Together with ligaments and peri-articular muscles, they maintain the structural integrity of the joint.
Blood Supply of the Hip Joint
Main Vessels:
Medial and lateral circumflex femoral arteries (branches of the profunda femoris artery and femoral artery).
Artery to the head of the femur (branch of the obturator artery).
Retinacular arteries (branches of the circumflex femoral arteries).
Nerve Supply of the Hip Joint
Hilton's Law: States that the nerves supplying the muscles extending directly across and acting at a given joint also innervate the joint.
Innervations:
Flexors: Anterior aspect of the hip joint is innervated by the femoral nerve.
Lateral Rotators: Innervated by the obturator nerve (inferior aspect) and the nerve to the quadratus femoris (posterior aspect).
Abductors: Innervated by the superior gluteal nerve (superior aspect).
Knee Joint
Description: Largest and most superficial joint.
Type: Hinge type of synovial joint: allows flexion and extension combined with gliding, rolling, and rotation about a vertical axis.
Implications of Hyperextension: Impairment of the knee joint; particularly relevant in contact sports such as ice hockey and football.
Articulations and Articular Surfaces of the Knee Joint
Articulations: Three articulations exist within the knee joint:
Two femorotibial articulations (lateral and medial) between the femoral and tibial condyles.
One intermediate femoropatellar articulation between the patella and the femur.
Fibula Involvement: Not involved in the knee joint.
Stability of the Knee Joint
Weakness of Joint: Stability relies on the strength and actions of:
Muscles and their tendons.
Ligaments connecting the femur and tibia.
Preventing Sport Injuries: Proper conditioning and training are key to preventing sports injuries.
Quadriceps Femoris: The most important muscle in stabilizing the knee joint, particularly the vastus medialis and lateralis.
Joint Capsule of the Knee Joint
Structure: Composed of an external fibrous layer and an internal synovial membrane.
Fibrous Layer Functions: Forms intrinsic ligaments.
Extracapsular Ligaments of the Knee Joint
Types: Five extracapsular (intrinsic) ligaments exist:
Patellar ligament.
Fibular collateral ligament (FCL).
Tibial collateral ligament (TCL).
Oblique popliteal ligament.
Arcuate popliteal ligament.
Specific Ligaments
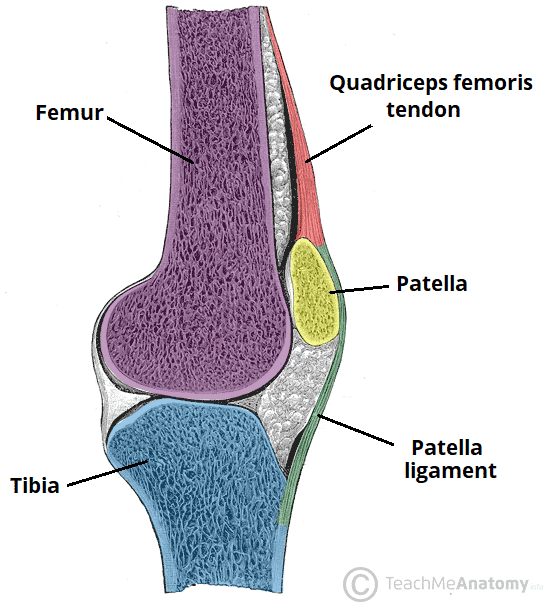
Patellar Ligament:
Distal part of the quadriceps femoris tendon.
Strong, thick fibrous band passing from the apex and margins of the patella to the tibial tuberosity.
Represents the anterior ligament of the knee joint.
Fibular Collateral Ligament (FCL):
Strong cord-like extracapsular ligament that extends from the lateral epicondyle of the femur to the lateral fibular head.
Separates from the lateral meniscus by the tendon of the popliteus.
The tendon of biceps femoris is split into two parts by the FCL.
Tibial Collateral Ligament (TCL):
Strong, flat, intrinsic band from the medial epicondyle of the femur to the superior part of the medial surface of the tibia.
Deep fibers attach to the medial meniscus.
Generally weaker than FCL and more frequently damaged during contact sports.
Additional Ligaments
Oblique Popliteal Ligament:
Extension of the tendon of the semimembranosus.
Reinforces the joint capsule posteriorly; arises posteriorly to the medial tibial condyle.
Arcuate Popliteal Ligament:
Strengthens the joint capsule posterolaterally.
From the posterior aspect of the fibular head; also contributes to posterolateral stability of the knee.
Intra-Articular Ligaments of the Knee Joint
Composition: Comprised of cruciate ligaments and menisci.
Functionality of Cruciate Ligaments:
Crisscross within the joint capsule but outside the synovial cavity.
Cruciate ligaments wind around each other during medial rotation of the tibia on the femur to act as a pivot for rotatory movements at the knee.
Anterior Cruciate Ligament (ACL)
Description: Weaker of the two cruciate ligaments; arises from the anterior intercondylar area of the tibia.
Poor Blood Supply: Leads to difficulty in healing.
Attachment: Connects to the lateral condyle of the femur.
Function: Prevents posterior displacement of the femur on the tibia and hyperextension of the knee joint.
Posterior Cruciate Ligament (PCL)
Description: Stronger of the two cruciate ligaments; arises from the posterior intercondylar area of the tibia.
Attachment: Connects to the medial condyle of the femur.
Function: Prevents anterior displacement of the femur on the tibia or posterior displacement of the tibia on the femur; also helps prevent hyperflexion of the knee joint.
Main Stabilizing Factor: The PCL primarily stabilizes the femur in a weight-bearing flexed knee position.
Menisci of the Knee Joint
Description: Crescentic plates of fibrocartilage that deepen the articular surface of the tibia and play a role in shock absorption.
Structure: Thicker at external margins, tapering to thin in the interior.
Coronary Ligaments: Portions of the joint capsule that link the menisci and tibial condyles.
Transverse Ligament of the Knee: Joins the anterior edges of the menisci.
Specific Menisci
Medial Meniscus:
C-shaped, broader posteriorly than anteriorly.
Anterior end attaches to the anterior intercondylar area of tibia, and posterior end attaches to the posterior intercondylar area.
Adheres to the deep surface of the TCL; less mobile on the tibial plateau than the lateral meniscus.
Lateral Meniscus:
Nearly circular, smaller, and more freely movable than the medial meniscus.
Involvement of the tendon of the popliteus, having two parts related to it.
Posterior meniscofemoral ligament joins the lateral meniscus to the PCL and medial femoral condyle.
Movements of the Knee Joint
Primary Movements: Flexion, extension, and rotation.
Knee Locking: Occurs when fully extended with the foot on the ground due to medial rotation of the femoral condyles on the tibial plateau, rendering the limb a solid column for weight-bearing.
Knee Unlocking: Achieved when the popliteus contracts, rotating the femur laterally approximately 5° on the tibial plateau, allowing for flexion.
Blood Supply of the Knee Joint
Main Vessels:
Genicular branches of the femoral, popliteal, and anterior/posterior recurrent branches of the anterior tibial and circumflex fibular arteries.
Middle genicular branches of the popliteal artery supply cruciate ligaments, synovial membrane, and peripheral margins of menisci.
Innervation of the Knee Joint
Innervation Sources:
Articular branches from the femoral, tibial, and common fibular nerves supply anterior, posterior, and lateral aspects, respectively.
Obturator and saphenous nerves provide innervation to the medial aspect.
Bursae Around the Knee Joint
Major Bursae: Prepatellar and infrapatellar bursae at the convex surface of the joint.
Communication: Four bursae that communicate with the synovial cavity of the knee joint include:
Suprapatellar bursa.
Popliteus bursa (located deep to the distal quadriceps).
Anserine bursa (located deep to the tendinous attachments of sartorius, gracilis, and semitendinosus).
Gastrocnemius bursa.
Clinical Note: Infections in the suprapatellar bursa may spread to the knee joint cavity.