Week 8 - Chpt.33 - Allergy Disorders
IMMUNOLOGIC DEFINITIONS
Allergen – substance that causes manifestations of allergy
Allergy – an exaggerated/inappropriate immune response to substances that are normally harmless
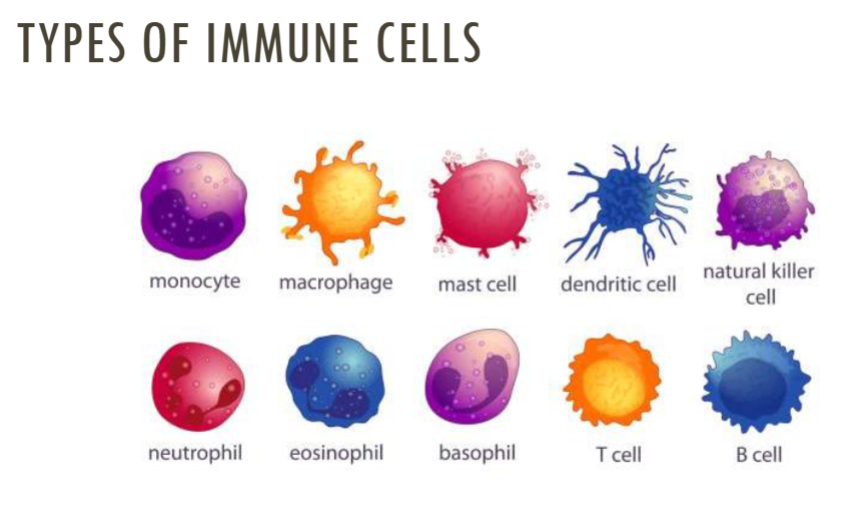
Antigen – substance that the body identifies as a foreign invader, induces production of antibodies
Antibody – protein substance developed by B cells in response a specific antigen
Histamine – substance in the body that causes increases gastric secretion, dilation of capillaries, & constriction of the bronchial smooth muscle
feeling flushed due to dilated capillaries
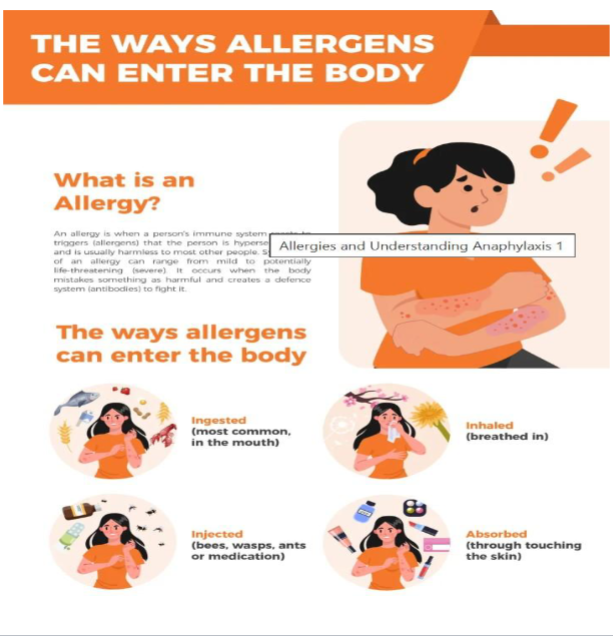
ingest → ate something
inhale → breathed something in
injected → some type of bite that goes into your blood stream
absorbed → something that touched your skin that gets absorbed into the body
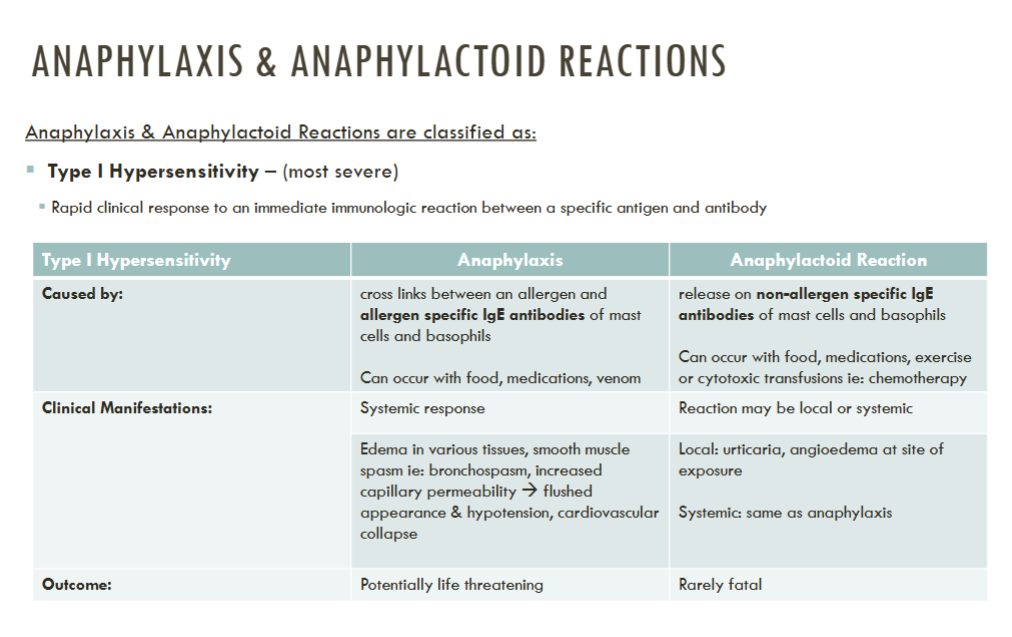
cytotoxic infusion → like chemotherapy or a hemolytic transfusion
if a patient has never had a medication before it is best to monitor closely incase of an allergy reaction
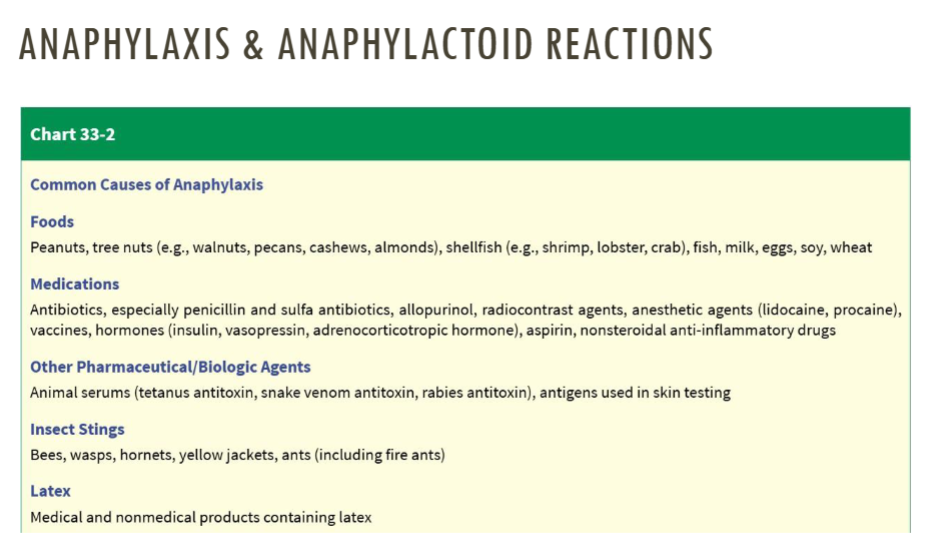
people allergic to shellfish or kiwi have increased risk of allergy to radiocontrast dye
always be mindful of latex allergy
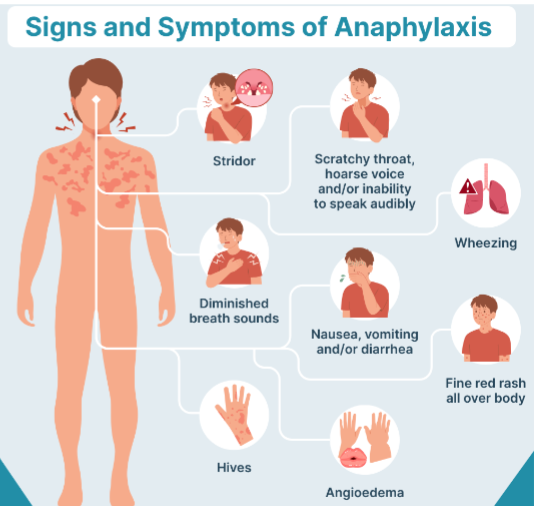
ANAPHYLAXIS & ANAPHYLACTOID REACTIONS
Clinical Manifestations – based on severity
Mild – within two hours of exposure
Peripheral tingling, warm sensation, feeling of fullness in mouth/throat, nasal congestion, periorbital swelling, pruritis, sneezing, eye tearing
Moderate - within two hours of exposure
Flushing, warmth, anxiety, pruritis, edema of airway/larynx, bronchospasm, dyspnea, cough, wheezing, & same as mild
Severe – within seconds, minutes & hour
Same as mild/moderate with rapid progression to bronchospasm, laryngeal edema/dysphagia, dyspnea, cyanosis, hypotension, abdominal cramping, vomiting, diarrhea, seizure
Cardiac arrest or comatose state may follow these symptoms
patients may not recover can die or body will go into a comatose state & shut down
ANAPHYLAXIS & ANAPHYLACTOID REACTIONS: Prevention
Avoidance of potential allergens
Ie: insect bites, snakes/spiders, food items
Screen patients for allergies before prescribing, prior to first dose
Assess whether patient has had previous anaphylactic, or mild reactions to medications/dyes in past
Clients with anaphylactic history should wear medical bracelet
Administer Epinephrine as soon as possible → often done on the thigh
Desensitization therapy for patients that are allergic to medications that are medically necessary
Ie: patients with diabetes & insulin allergy, patient allergic to PCN
ANAPHYLAXIS & ANAPHYLACTOID REACTIONS: Treatment
Medical management – depends on severity
Epinephrine administered 1:1000 dilution – subQ, may be followed by IV admin
Epi 1:1000 is SPECIFIC for allergic reactions
Cardiac arrest → Cardiopulmonary resuscitation (CPR)
Cyanosis/dyspnea → airway management, oxygen administration
Manage inflammatory response → Antihistamines and corticosteroids
Hypotension → IV fluids (crystalloid/colloid),
Nursing
Assess ABC, notify rapid response team
Emergency measures – prepare patient for intubation, admin rescue medications for cardiac/pulmonary support/epi, initiate IV access & instill fluids
Provide patient education about prevention, self admin of epi
URTICARIA (HIVES)
Type I Hypersensitivity reaction characterized by sudden presentation of
pruritic pink/red papules that process to wheals of varying sizes
Acute urticaria – evolves over minutes/hours, resolves within 24 hours
Commonly caused by:
Infections, allergic reactions to food/insect bites/medications
Diagnosed by:
Health history, physical exam
Treatment:
Eliminate causative agent
Administer antihistamines (cetirizine (zertec), fexofenadine (allegra), loratadine (claritin))
Minimize conditions that can worsen urticaria ie: heat, stress, alcohol, tight clothes

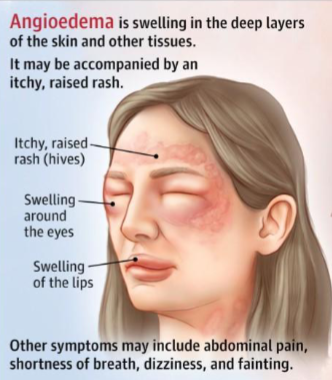
ANGIOEDEMA (MAST-CELL MEDIATED)
Allergic reaction characterized by fluid accumulation within subcutaneous
and mucous membrane’s; often occurs with urticaria and can be life-
threatening when paired with anaphylaxis sxs.
Caused by: allergy to foods/latex/medications/insect bites
Clinical manifestation
Can occur within seconds, minutes, or slowly over 1-2 hours; resolves within 24-48 hours
Nonpruritic (get really puffy face), brawny, wide-spread, nonpitting edema that presents on the lips, eyelids, cheeks, hands, feet, genitalia, tongue
Mucous membranes of the larynx, bronchi, and GI tract can also be affected
Diagnosed by: health history, physical exam
Treatment:
Eliminate causative agent
Administer antihistamines (cetirizine, fexofenadine, loratadine)
If anaphylaxis is present: IM epinephrine
these patients should still go to a hospital incase anaphylaxis takes place
because angioedema & urticaria can be precursors to anaphylaxis