CSDS 131 Exam 3 Study Guide
CSDS 131 Exam 3 Study Guide
1. Know what acoustic immittance is:
- Objective measure of the ME function
- Allows description and quantification of how well the ME system is working
- Checking for any abnormalities in the interconnected structures of the ear canal to the inner ear that may alter the measurement
- Include measurement of impedance (something is blocked) and admittance (something allowed to pass)
1. The basic tests of immittance and their definitions:
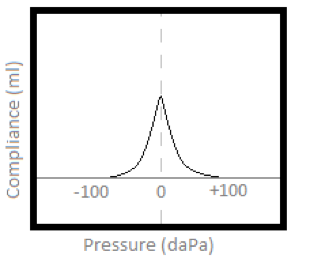
a. Peak compliance:
- Measure mobility of TM in response to a given value of air pressure applied into the ear canal
- Measure compliance or stiffness of the ME system at rest (atmospheric pressure or 0 daPa)
- Measurement at eardrum of the amplitude (height) of pressure change
b. Tympanometry:
- Measurement of ME pressure
- Determine TM mobility as a function of various + or - pressure
- Produce a graph (tympanogram) showing compliance of the TM system as pressure is changed within the extended ear canal
- Graph represents changes in stiffness or compliance of the TM as air pressure manipulated with the ear canal
c. Ear Canal Volume:
- Measure the space (volume) from the probe test to the end point (TM)
- Value taken with +200 daPa of air pressure, thus stiffening TM and thus measures the admittance of OE only (if TM is intact)
d. Acoustic Reflex:
- Sonomotor response= contraction of muscles upon sound
- ME muscles= Tensor Tympani and Stapedius (responsible for contractual reflexive response to high intensity sound)
- Elicit bilaterally between 70-100dB above t'hold
- Measure increase in ME stiffness associated w/ contraction of stapedius muscle in association with relatively high intensity sound
- Lowest intensity level at which AR can be activated
- Tells you: status of ME, site of lesion, and hearing sensitivity
2. Describe the point of maximum compliance:
- When pressure on both sides of TM are approximately equal
- Use in peak static acoustic compliance
3. What are the typical values for static acoustic admittance?:
- 0.25-0.92 mmho for infants
- 0.25 - 1.05 mmho for children from (3-10 years)
- 0.30-1.7 mmho for adults
What information is gathered when values are outside the normal range?:
- Value too low? (below .25): there is more stiffness (eardrum unable to move) ex: otitis media or air going through a hole in eardrum.
- Value too high? (above 1.7): there is too much compliance (too much movement or flexible) ex: ossicular chain broken
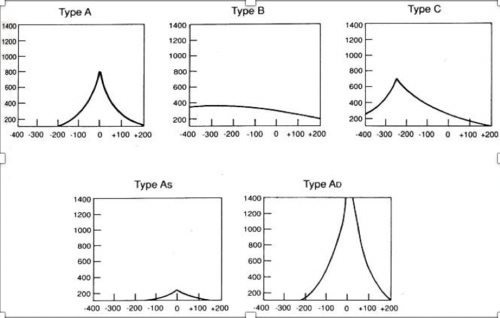
4. Be able to define Jerger’s classification system: Tympanogram is a graph of compliance measures…
- Compliance (admittance) along Y axis (in mmho or cc)
- Air Pressure along X axis (in daPa)
What does each type of tympanogram suggest?:
Type A:
- Normal ME pressure and admittance = Normal ME function
- +50daPa to -150daPa
- Admittance: rage of 0.3 to 1.5 *Note: Some consider -200 daPa to be acceptable
Type As:
- Normal middle ear pressure with reduced admittance
- Peak at or near 0 daPa
- Shallower peak than Type A
- Suggests stiffness
- Restriction in flexibility or an increase in stiffness of the ME system
- Cause: Ear infection or scar tissue, maybe fluid
Type Ad:
- Normal middle ear pressure with markedly increased admittance; highly compliant ME system or TM
- Similar to type A, but amplitude is unusually high
- Positive and negative sides may not meet
- “D” for discontinuity or deep
- Cause: TM membrane is thin or rupture and usually don't affect hearing
Type B:
- No identifiable point of maximum admittance; no clear peak
- May appear slightly rounded, or look like a flat line
- Consistent with extreme stiffness of the OE and/or ME system
- No point of greatest compliance
- Cause: Can be caused by debris/ cerumen in external ear canal plugs one or more of the small tube in the probe ; ear infection, hole in eardrum, fluid behind eardrum
Type C:
- Pressure in ME is outside normal negative range (<-150 daPa) with normal or near normal admittance
- TM is most compliant with negative pressure
5. What information is gathered by ear canal volume?:
Normative finding for ECV are generally smaller value in children and females…
- Children= 0.3-0.9 cc (3-10 years)
- Adult = 0.9 - 2.0 cc (adults 18+)
What does it mean when values are outside the normal range?
- If borderline findings, may want to compare 2 ears
- Too high value = from the tip to eardrum there might be a hole
- Too low = flat, it means we have wax or blockage
* Other factors to consider for ECV: Age, Body Size, Gender, Size of probe…
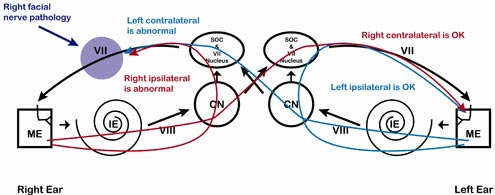
6. The Acoustic Reflex Arc pathway will be provided.
a. What nerves are involved in the pathways?
- Ipsilateral Pathway of AR—OE, ME, IE, VIII, CN, Cochlear Nucleus, Superior Olivary Complex, Facial Nerve, ME, OU (mark present or absent)
- Contralateral Pathway of AR—OE, ME, IE, CN VIII, Cochlear Nucleus, Superior Olivary Complex, to opposite ear Superior Olivary Complex, Facial Nerve, ME, OE (mark present or absent)
b. Know what the findings would be for specific types of hearing loss for ipsi and contra
Outcome of CHL on ipsi and contralateral AR—Slight degrees of CHL will cause AR to be absent because it is not able to measure change in admittance.
Outcome of SNHL on ipsi and contralateral AR—Ear being stimulated prevents intensity to elicit the reflex. Elevated in those with mild and moderate HL or may be absent.
- Conductive hearing loss: Even the slightest degree of conductive component most likely cause the AR to be absent because not able to measure change in admittance * (SAME FOR MIXED HL)
- Sensorineural Hearing Loss: Often absent when the degree of hearing loss in the ear being stimulated prevents adequate intensity to elicit the reflex. Elevated in those with mild or moderate hearing losses or be present
* NORMAL 70 to 100 dB HL
7. What is the purpose of acoustic reflex decay?:
- Optional, additional test
- Can only be performed if AR are present.
- Test that assists in identifying a retrocochlear pathology
- When tone is presented for 10 seconds, should not decay beyond half the change in compliance amount
- If more than 50%, suggests retrocochlear pathology (auditory nerve or the auditory brainstem)
What is retrocochlear?: Used to describe a neural or central hearing loss which occurs beyond the Cochlea affecting the vestibulo cochlear nerve of the central auditory system. Problem beyond the cochlea.
8. Know the types of speech tests used and their purpose or how are they used.
a. SRT: Speech Recognition Threshold
- Lowest level in dB at which a subject can barely understand speech with a 50% criteria
- Preferred material: spondaic words or “spondees”. Def.: Two syllable words with equal stress and effort on both syllables. I.E. Hot dog, baseball, cupcake, airplane
- Formerly known as spondee threshold (ST) and Speech reception threshold (SRT)
- For young children, SRT may be performed prior to pure tone testing to provide some estimate of hearing sensitivity
- Picture pointing task may be preferred
- Identifying body parts
b. SDT: Speech Detection Threshold aka Speech Awareness Threshold (SAT):
- Lowest level in dB at which a subject can barely detect the presence of speech
- Test stimuli may be words, phrases, syllables, nonsense words or sounds
Who uses SDT/SAT?: Limited speech, not able to repeat. Very young, or children or adults with special needs. Often finding on SDT is closest to the best threshold on the audiogram. May use a “threshold” procedure.
c. WRT: Word Recognition Testing
- Tests performed to determine an individual’s understanding of speech stimuli that are presented at hearing levels above threshold
- Formerly known as “speech discrimination” testing AKA speech recognition testing
- Establish a word recognition score
- Monosyllabic words–dog, cat, book, tree, sun
- Many lists: need to be reliable and valid
9. Know the relationship between SRT, SAT and PTA:
- SDT should be lower than SRT
- SRT and SDT should be no more than 12dB difference (SDT around 6-10dB better than SRT)
- SRT and PTA should be within 10dB of each other
10. Know the different methods used for presenting speech material to the patient. Know the advantages and disadvantages.
- 1. CD (consistency & allows control of presentation speed)
- 2. Digital speech (consistency)
- 3. Monitored Live Voice with Volume Units (VU) meter (young children and elderly adults) (flexibility & allow control of presentation speed)
- 1 and 2 give consistency
- 3 gives flexibility; sometimes preferred by Audiologists
- 2 and 3 allow control of presentation speed
*Recorded speech material are recommended
- Verbal Response: most common method used; (-) risk of misinterpretation by listener (+) less time consuming
- Written: (+) eliminates listening errors, but (-) may not be illegible, (-) poor spelling; (-) more time consuming
- Identifying Pictures: (-) limited to number of items (close set); (+) appropriate for children with special needs
11. Know word recognition testing and what information is gathered by performing this test.:
- Determine the extent of speech recognition difficulty
- Aids in site of the disorder
- Assists in determining need for and proper selection of amplification
- Helps to make a prognosis for the outcome of treatment
12. What is the purpose of the different intensity levels used for word recognition testing?:
- PI=Performance Intensity
- Purpose is to find the intensity level the individual performs maximum speech understanding
What information is gathered at the various intensity levels.:
- Identify possible rollover evidence of retrocochlear (neural) pathology
- PI rollover occurs when increasing intensity results in decreasing word recognition
Know the level that is considered for conversational speech.: Others may use 45 dB HL as its normal conversational speech level.
13. Know the word recognition scores and their meanings from the Martin reference.
- 90-100% = Normal limits
- 75-90% = Slight difficulty, comparable to listening over a telephone
- 60-75% = Moderate difficulty
- 50-60% = Poor recognition; marked difficulty in following conversation
- Below 50% = Very poor recognition; probably unable to follow running speech
14. Know what closed and open set tests for speech audiometry:
Closed Set:
1. Used with children or adults with special needs, monosyllabic (ex: dog, doll, ball, box)
Identify pictures: limited number of items
2. Give them options of what it will be seeing or saying/showing them pictures or a list of words
Open Set:
1. Not given options
2. They have no idea- the picture or words is not being shown
15. What is signal to noise ratio?:
Difference in intensity between the signal and the noise
Be able to calculate this if given the needed information.: Speech at 50dB HL and noise at 40dB HL, what is SNR? SNR= Speech to Noise. 50dB to 40dB= +10 SNR Speech at 45 dB HL and noise at 45 dB HL, what is the SNR? 0 (exactly the same level). Speech at 45 dB HL and noise at 55 dB HL, what is the SNR? -10 dB SNR
16. Know the objective tests used and be able to describe them.:
OAE:
- Sound generated in the cochlea that can be measured in the ear canal
- Kemp (1978) - many normal cochlear produce sound in absence of external stimulation
- Known as Spontaneous OAE (SOAE)
- 50 to 70% the population with normal hearing; more prevalent in women vs. men
Auditory Evoked Potential:
- Measures electrical activity from cochlea to auditory cortex in response to an auditory stimuli
ABR:
- Auditory Brainstem Response estimates hearing thresholds, used to program cochlear implants etc.
17. Know what evoked OAE test is and what the test might be used for.:
1. Sound generate in the cochlea that can be measured in the ear canal
2. Measure response of OHC of the cochlea in response to auditory stimuli.
3. Preneural response: OE, ME, and IE (especially OHC) not including auditory nerve
4. Tell you about the auditory system but does not measure hearing
5. Use in addition to conventional audiometric data
a. What does present or absent mean?:
- present: normal, cochlea, outer and middle ear are normal
- absent: not hearing well, reason is unknown
b. What would you expect with a conductive hearing loss? Sensorineural hearing loss? Retrocochlear pathology?
- For evoked OAE, what would you expect with SNHL?: Yes, you may measure perfectly normal in the low frequencies, but not usually measure emissions; wouldn't measure flat SN
- For evoked OAE, what would you expect with CHL?: No, because of how we are measuring; stimulus has to get past wax plug and fluid to get in cochlea and would lose dB in stimulus
- Retrocochlear pathology?: N/A, When testing for rollover and we increase the volume and the patient does worse, what does it suggest? Retrocochlear pathology
c. What does refer or pass suggest with EOAE?:
• Pass rules out serious degrees of hearing loss
• Refer indicates risk for hearing loss that could affect communication
18. Know what ABR test is and what the test might be used for.:
Auditory Brainstem Response
1. Recordings were highly consistent and almost identical from one person to the next.
2. Response could be activated by sounds presented rapidly, more than 50 times per
second, so could be recorded quickly.
3. ABR could be elicited with different types of
stimulation, such as click and short bursts of tones
4. Sleep, sedation, or anesthesia had no effect on ABR
•Rule out retrocochlear site of lesion
•Estimate hearing thresholds
•Identify auditory neuropathy
•Intraoperative monitoring
•Hearing screening (AABR)
•Used to program CI’s
***** KNOW THE TYPES OF HEARING LOSS. KNOW THE DEGREES OF HEARING LOSS FOR ADULTS AND PEDIATRICS. KNOW HOW TO CALCULATE PTA. **
CHILDREN
ADULTS | CHILDREN |
|---|---|
- 10 to 25 normal | -10 to 15 normal |
26 to 40 mild | 16 to 25 slight |
41 to 55 moderate | 26 to 40 mild |
56 to 70 moderately severe | 41 to 55 moderate |
71 to 90 severe | 56 to 70 moderately severe |
91 + PROFOUND | 71 to 90 severe |
91+ PROFOUND |
PTA is always AC - 500, 1K, 2K
Rt AC - Add those numbers and divide by 3 to get your right ear PTA
Left AC - Add those numbers and divide by 3 to get you left ear PTA
*Once you get your PTA, that will tell you the degree of hearing loss.
Calculations for PTA
500, 1k, 2k Hz of AC T'holds
(500k+1k+2kHz)/3= PTA