Informatics
Informatics has been defined as the use of information and technology to communicate, manage knowledge, mitigate error, and support decision making. Nursing students as well as novice graduate nurses need to be proficient in nursing informatics, the integration of technology and physical devices with nursing knowledge and nursing clinical decision-making skills. Nursing informatics is “the component of clinical informatics that deals with the roles and activities of individuals in the nursing profession".
The use of informatics in nursing dates back to the years of Florence Nightingale, who in the 1850s used informatics to compile and process data for the purpose of improving sanitation. However, it was not until 1992 that the American Nurses Association established a formal definition for nursing informatics and designated it a specialty, allowing nurses to become certified as nurse informaticians. This designation allows nurses to apply for the certification examination regardless of formal training as long as they have experience in the field.
Simulation
Students are able to acquire knowledge more effectively when they are engaged in the learning process. Exploring new ways to advance undergraduate student performance is vital to preparing nurses who can safely function in a complex, diverse health care system. Simulation is a component of clinical education that allows nursing students to utilize clinical decision-making and nursing skills outside of the typical hospital setting. Simulation is a method used to create a situation that mimics a real experience and is used for the practice, assessment, education, or for acquiring knowledge of systems or a person’s actions. Clinical decision making is an iterative process using nursing knowledge to assess a client situation, identify the priority concern, and then use evidence-based interventions to implement care. Incorporating simulation into the undergraduate curriculum is an effective way to improve student knowledge. Research has shown that students enrolled in nursing programs that included simulations performed better and felt more motivated and competent in what they perceived to be a student-centered learning environment. This strategy increases the number of students who are actively engaged in the activity and may improve student knowledge and student perceptions. They are able to anticipate and respond in real time to client conditions as a result of their actions. Simulation scenarios allow for students to practice leadership roles as well as communication skills, as they can simulate reporting a client’s condition to the provider or receiving critical client information from the lab or pharmacy. They can scan and document in an electronic medical record in real-time, just as they would when working on a busy hospital unit.
As the availability of clinical sites and faculty continues to decrease, simulation will be increasingly used to supplement the clinical experience. Simulation plays a significant role in pre-licensure nursing education and is considered an evidence-based, effective learning technology. It has become an invaluable tool in nursing education and a welcome ally in clinical practice. In the classroom, it is the role and responsibility of the faculty to ensure competent clinical skills as well as the development of sound critical thinking with appropriate rationales for nursing actions with expected outcomes. On-campus simulation-based learning experiences offer students a safe place to practice skills and make errors from which they may learn without harming a live client. In addition to clinical skills and knowledge, undergraduate nursing programs are tasked with developing professional attributes needed to safely practice as competent nurses. Nursing students and novice nurses are able to draw from their clinical experiences to become critical thinkers and better communicators in high-risk scenarios.
Clinical Information Systems
A clinical information system is a computer system that allows for instant retrieval of client information either directly or from data networks. They are those processes used primarily by nurses, providers, and other members of the interprofessional team at the clinical point of care site. To enhance the quality of health services, health care organizations recognize the importance of information technology and user end satisfaction. Information technology is technology and physical devices used to create and store information, including electronic health records. Clinical information systems are comprised of those interface opportunities that take place at the point of clinical care. This can range from barcode scanning, documenting, and medication administration to arm band scanning by ancillary personnel for procedures such as venipuncture lab draws. Health care providers may also utilize order entry systems at the point of clinical care to ensure timely entry of medications, procedures, or treatments.
Health care workers utilize information systems in the form of the electronic health record to obtain histories on their clients in real-time. The electronic health record is a real-time computerized form of a client’s paper chart that can be shared among authorized providers; it includes the client’s medical history, diagnosis, allergies, and diagnostic testing results. Service quality and customer service must also be factored in. Clinical quality depends on its clinical information systems and is considered an indispensable element of routine operations in today's hospitals. A robust clinical decision support system (CDSS) has the ability to shorten critical decision-making periods by providing accurate and reliable client information. The system will be expected to expediently process extensive amounts of client protected health information (PHI) and complex medical information. This decreases health care workers’ response time to clients by allowing for more rapid diagnoses and comprehensive treatment plans, which enhances client satisfaction and ultimately hospital revenue. The concerns for loss of client information, redundancy in forms, and accurate, timely medication reconciliation are just a few examples of how quality is improved with a robust system. With improvement in the quality of care that the system provides, client satisfaction, which greatly impacts the health of any health care system, is greatly improved.
Health care delivery is shifting to a value-based delivery model, which utilizes clinical pathways to guide client care. Clinical pathways, also called care maps or integrated care pathways, are a standardized method of health care delivery for a specific group of clients, through the use of practices based on evidence-based guidelines. Clinical pathways are decision support tools that outline specified steps related to a predetermined clinical problem and present the anticipated clinical course. As the health care industry focuses on quality improvement and efficiency, the use of clinical pathways has led to improved client outcomes and effectiveness of client care while simultaneously managing expenses and maintaining quality care. As health care costs have continued to rise, and as insurance companies have shifted to value-based models of health care delivery, clinical pathways have flourished. High-value client care is defined as safe, effective, efficient, unbiased, and client-centered. Clinical pathways of specific client groups are comprehensive and use evidence-based treatment protocols for providing care to clients with certain medical conditions and stages of disease.
Health care organizations can implement clinical pathways that are on paper or use computer software that generates and manages electronic clinical pathways. Increased paperwork, which leads to inefficiency and decreased accuracy in client care practices, is associated with the use of paper-based clinical pathways. Use of a software-based clinical pathway is more effective in decreasing length of stay, major complications, and total costs per client when compared to the use of paper-based clinical pathways. Clinical pathways systems have been found to facilitate the monitoring of protocols and the efficiency of the nursing unit. For the clinical pathways management system to be effective and successful, nurses must accept the use of clinical pathways in providing client care.
Health Insurance Portability and Accountability Act (HIPAA)
Client health care information is both protected and sensitive under the Health Insurance Portability and Accountability Act (HIPAA) of 1996. HIPAA is a federal law enacted to safeguard clients’ medical health information when it is being accessed or shared electronically without the clients’ consent or knowledge. The purpose of HIPAA is to reduce fraud and deter inappropriate use of client health care information.
There are several regulatory components that are covered under HIPAA. These components include the Privacy Rule, which defines the standards under which protected health information in any form could be used and disclosed; the Security Rule, which establishes safeguards for electronic PHI; and the Breach Notification Rule, which mandates that clients are notified about a breach of their unsecured PHI.
Privacy Rule
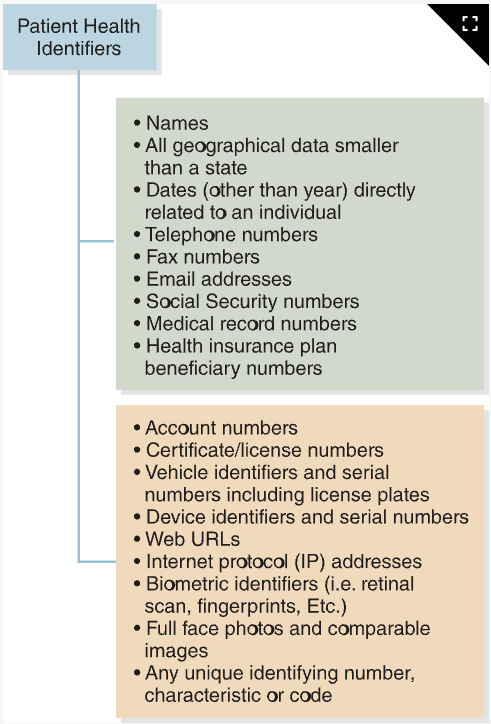
The Privacy Rule defines protected health information (PHI) as “any information held by a covered entity for health care that can be linked to an individual". The Privacy Rule requires that unique client identifiers (e.g., Social Security number, date of birth), which can link a client to their PHI, be coded for the purpose of transmission. The rule requires these safeguards to protect client privacy, set limits and conditions for disclosure, and prevent unauthorized release and use of PHI. The Privacy Rule also gives clients rights over their PHI, as well as the right to obtain copies of their health records. and provides a mechanism for clients to request corrections to their PHI.
The HIPAA Privacy Rule and Security Rule mandate HIPAA education and training of health care providers as a requirement of compliance. There are several requirements of the training, including the regulative history, reason for HIPAA, and a review of the principles and essential provisions of the Privacy Rule. HIPAA training is a yearly requirement for all health care providers.
The HIPAA rules mandate that covered entities have a HIPAA Compliance Officer, or larger organizations can divide the duties between a Privacy Officer and a Security Officer. The Privacy Officer is tasked with developing a privacy program, which includes making sure the policies aimed at protecting PHI are enforced. The Privacy Officer oversees training, completes risk assessments, creates HIPAA-compliant procedures, conducts investigations when PHI has been breached, reports breaches, and ensures that state and federal laws are followed. The HIPAA Security Officer role is similar to that of the Privacy Officer. The HIPAA Security Officer’s main role is to follow the HIPAA security rule, ensuring that protective measures are implemented to provide privacy, integrity, and availability of electronic PHI (ePHI).
Security Rule
In comparison to the Privacy Rule, which primarily deals with the integrity of PHI, the Security Rule specifically addresses the use and disclosure of electronic PHI. During December of 2024, in response to increased cyberthreats, there was a proposed rule to modify the HIPAA Security Rule to strengthen cybersecurity protections for individuals’ electronic PHI. Unintentional data breaches can occur when devices are discarded with ePHI not being appropriately or completely removed. As a result, many health care entities are creating policies and procedures that govern the use of personal technology and devices when providing client care. Safeguards enacted to decrease unauthorized disclosure include administrative, technological, and physical controls.
Breach Notification Rule
Despite applying all of the safeguards and adhering to the regulations under the privacy and security rules, breaches of PHI will inevitably occur. There is very little that can be done to completely mitigate human behavior or human error. Technology will be left in the “on” position, devices will get stolen, and cyberhacks are inevitable. The Breach Notification rule covers the process of reporting and responding to a breach of PHI. It is important to note that if ePHI is encrypted as detailed in the privacy rule, rendering PHI unreadable, it is not necessary to report that PHI as unusable because it is not classified as a breach of PHI. The process for reporting a breach to clients is to notify them via mail. A phone call may be necessary if it has been determined that possible misuse of a client’s PHI is imminent. Breaches should be reported as soon as possible, but no more than 60 days from discovery of the breach, to the Secretary of Health and Human Services as well as the affected individual.
The electronic health record (EHR) is a repository for client information and has a major role in the health care system. The main driver behind the need for EHR is client safety, followed by efficiency and medical record keeping. Student nurses have to be prepared for practice and part of that preparation is to be proficient in utilizing and managing EHRs within clinical information systems. The EHR has become an invaluable tool to manage clients’ medical information, provide timely access to that information, prevent redundancy, and improve health care service quality. Meaningful use of the EHR is needed to maximize efficiency and client safety. Meaningful use is the use of certified EHR technology such as e-prescribing. Electronic prescribing allows health care providers to enter prescriptions electronically using laptops, tablets, or desktop computers using a software program. The use of e-prescriptions provides greater convenience and decreased cost, and is safer for health care providers, clients, and pharmacies. The use of certified EHR technology guarantees the EHR system is capable of meeting the meaningful use criteria to those who purchase and use the EHR system, and that the system is secure and can share information with other systems.
Medication errors and preventable adverse drug events (ADEs) pose a serious risk to clients. An adverse drug event (ADE) is an injury caused from a medical intervention that is linked to a medication A medication error is a preventable error capable of causing harm or death to a client under the care of a health care provider. Medication errors are among the most common medical errors in all health care settings . Safe administration of medications is a core responsibility of the nurse, and EHRs have been shown to aid in the reduction of medication errors when utilized as directed within the globally accepted framework of the rights of medication administration.
Preventable medication errors and ADEs pose significant risks to hospitalized clients. The medication administration process involves multiple health professionals and health consumers within the four phases of the administration process, where errors are likely to occur. The four phases to the process are: ordering, transcribing, dispensing, and administration. Errors in the first three phases are primarily detected prior to reaching the client. The ability of the EHR to aid in clear effective communication between health care providers and ancillary departments has increased the effectiveness of the medication administration process. The implementation of barcode medication administration was designed to reduce the preventable errors in the last phase of the process; mitigating human errors (wrong administration time or wrong dose) that occur within the rights of medication administration. When using barcode technology, the nurse first scans the client’s identification band with the barcode scanner and then scans the barcode on the medication to be administered. Barcode technology automates the rights of medication administration and alerts the nurse to when there is a violation of any component of those rights. Flexibility is required as frequent updates and system changes should be expected as nurses become more technology aware and clinically competent, leading to a truly paper-free clinical information system.
Remote patient monitoring (RPM) is a form of telehealth medicine that assists in the tracking of client information and facilitates the rapid transfer of information to the health care provider. Electronic monitoring devices involve the use of mobile medical devices, sensors, and technology to collect client data and transmit the data to health care providers. The collection and transfer of information is accomplished using personal health technologies such as wireless devices, wearable sensors, implanted health monitors, smartphones, and mobile apps. Typical physiological data that can be collected include heart rhythm, vital signs, blood oxygen saturation level, and blood glucose level. Other types of monitoring devices include those that can detect motion or transmit real-time video. Wearable monitoring device sensors can be placed in clothes and elastic bands directly attached to a client’s body. The devices can be used for real-time monitoring in detecting client falls, observing gait and activity, and assessing sleep patterns
RPM can send information submitted by the user, store data in secure locations accessible to the health care providers, highlight abnormal data, and alert both health care providers and caregivers of unexpected readings by text message or email. Some devices also include the ability to link clients to their health records, provide educational resources and interactive self-care tools, and connect the client to their health care provider. Many RPM devices permit the client to produce patient-generated health data (PGHD), data that is generated, documented, or collected by the client or caregiver to maintain their health. PGHD includes client health history, bodily measurements, symptoms, and individual behavioral factors. Through the use of RPM, clients are better able to manage their health and be active participants in their health care.
According to Healthy People 2030, health literacy is a very important foundational principle and goal. The Healthy People 2030 definitions of health literacy include personal and organizational health literacy. Organizational health literacy is the extent to which organizations equitably assist individuals with understanding, finding, and using information and services to make informed health-related decisions for themselves and others. Personal health literacy is defined as the extent to which an individual can obtain, process, understand, and use services and information to inform health-related decisions for themselves and others.
Health literacy, the ability to read, write, and understand health-related information, significantly impacts client outcomes. Digital health literacy, the ability to search, obtain, understand, and evaluate information from electronic sources and utilize that knowledge to manage a health issue, also impacts client outcomes. Substantial evidence supports the association between lower health literacy, lower digital literacy, poor self-care, and increased mortality. Health care technology, with its potential to improve the health and well-being of the population, is a game-changer. From obtaining a client’s PHI to telehealth visits, health tracking, and self-monitoring devices, messaging with health care providers, and requesting appointments online, these technologies have transformed health care interactions. They can potentially enhance health care systems’ efficiency, quality, and reach. However, as technology advances, there is a growing concern about low digital literacy among ethnic minorities, the older population, and clients with low socioeconomic status. Low health and digital literacy affect an individual’s health status, pose a significant health care access barrier, and increase health inequities.
Lower health literacy can lead to increased use of emergency services and less frequent use of preventative services such as mammograms and flu shots. Clients with lower health literacy levels are also more likely to wait to seek medical care until they are considerably ill. These factors are associated with higher costs and poor health outcomes. Despite the challenges related to technology, the benefits are undeniable. Therefore, health care professionals, including nurses, are responsible for assessing the client’s health literacy and digital literacy. This assessment is crucial for planning interventions and providing adequate client education during teachable moments. Teachable moments often occur at pivotal times in clients’ lives. For example, pregnant clients represent an increasing need for adequate health literacy levels due to the abundance of information they receive throughout pregnancy. Pregnancy has been identified as an opportune time for change, as clients are often highly motivated to make choices that will help them achieve a healthy outcome for themselves and their babies. Nurses can play a significant role in improving client health literacy through strategies such as speaking slowly, using simple language, using the teach-back method, encouraging questions, and showing examples.
The responsible use and management of health information technology has a significant impact on both nursing and client outcomes, while presenting numerous opportunities for improving and transforming health care. Client safety is an important component of health care, and the use of information management technology optimizes client safety by reducing human errors, facilitating care coordination, and improving practice efficiencies and nursing compliance with practice guidelines, thereby improving clinical outcomes).
Information management technology also supports clinical decision making. For example, the use of medication barcodes and smart infusion pumps has been associated with a decrease in medication errors. Smart pumps are intravenous infusion pumps that are equipped with medication error-prevention software. The software contains a built-in medication library that calculates the infusion rate based on nurse-entered client information. This software has the ability to alert nurses when the infusion setting is outside of pre-configured safety limits. Although the use of smart pumps is associated with decreased medication errors, errors still occur when nurses override drug error alerts, work around the drug libraries, or incorrectly program the smart pump. Therefore, nurses should refrain from using workarounds or shortcuts when administering medications. Nurses must use clinical judgment and always follow the rights of medication administration. With continued assessment, evaluation, and improvement in information management systems, the expectation is that client and nursing outcomes will continue to be positively impacted.