Development of the Face and Jaw
CleDevelopment of the Face and Jaw
Adult Anatomy
Hard Palate:
Description: A horizontal bony plate forming part of the palate of the mouth.
Function: Separates the oral and nasal cavities and forms the roof of the oral cavity and the floor of the nasal cavity.
Anterior Part: Palatine process of the maxilla (bone), extending between two sides of the maxillary dental arch to meet two horizontal palatine processes posteriorly.
Can do a lot when producing speech.
Development of Lip and Palate (important to know this)!
Timeline:
4th to 6th Week: Development of the external human face.
6th Week: Completion of face development.
6th to 8th Week: Palate development begins, establishing the distinction between nasal and oral cavities.
12th Week: Completion of palate development.
Early Development (3-4 Weeks)
Oropharyngeal Membrane:
Formation at the site of future face composed of ectoderm (externally) and endoderm (internally).
Mesoderm- cells that develop in the internal structure in the head.
Cells and tissues differentiating in embryo. Messages are being sent. Goes from a general tissue type then branches out and differentiates/ specialises.
Breakdown begins in the 4th week to form future oral cavity, marking the start of the digestive tract.
Sources of External Face Structures:
Frontonasal Prominence: Formed by mesenchymal neural crest cells ventral to the forebrain. (Upper body- brain).
Mandibular and Maxillary Prominences: Parts of the 1st pharyngeal arch. (Lower head). the arches (bumpy parts of the picture) differentiate and grow to more specialised.
Stomatodeum: Space between the maxillary prominences, precursor to the mouth and pituitary gland. (Lower head).
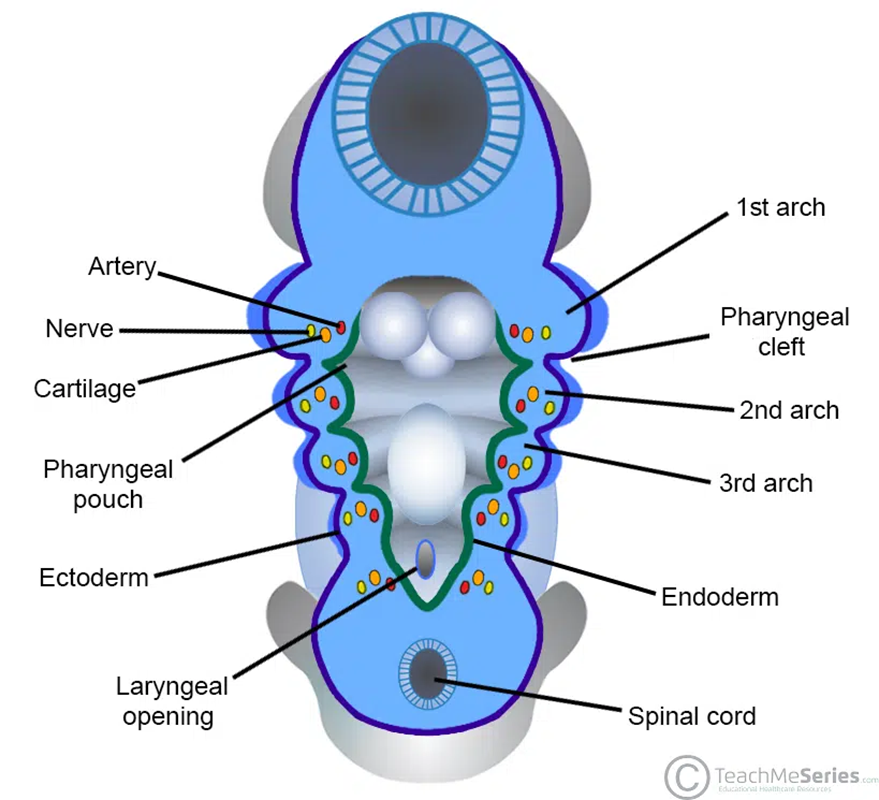
Developmental Structures (4 Weeks)
Tissue Structures for Nose and Face Development:
Pharyngeal Arches: Six arches arising in the 4th week, each associated with a branch of the aorta, a cranial nerve, and a cartilage bar.
Neural Crest Cells: Originate from neuroectoderm and migrate to form various structures in the body, including pharyngeal arches derivatives.
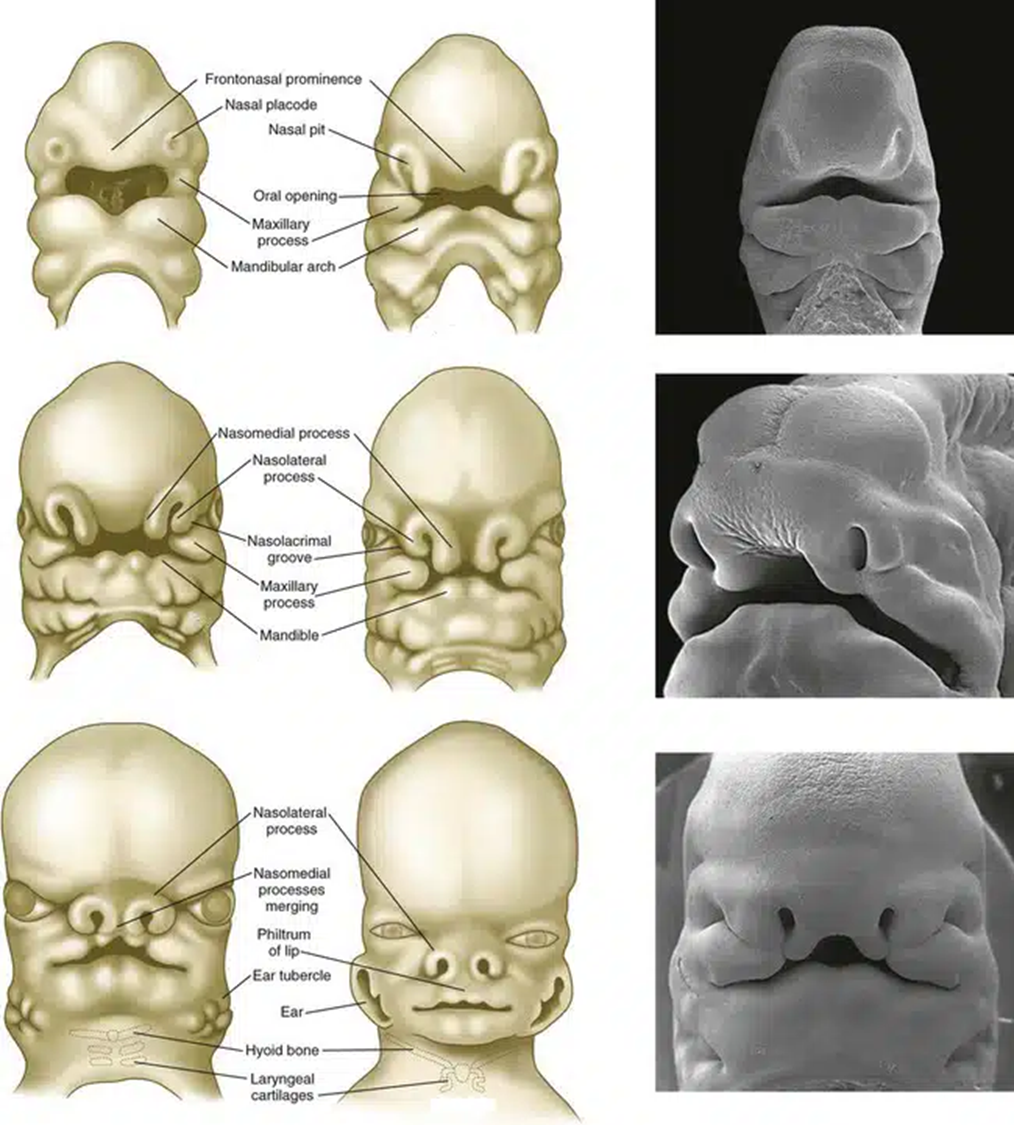
Derivatives of Early Structures
Prominence Derivatives:
Frontonasal: Forehead, bridge of nose, medial and lateral nasal prominences.
Medial Nasal: Philtrum, primary palate, upper four incisors and associated jaw.
Lateral Nasal: Sides of the nose.
Maxillary (1st Pharyngeal Arch): Cheeks, lateral upper lip, secondary palate, lateral upper jaw.
Mandibular (1st Pharyngeal Arch): Lower lip and jaw.
Palate and Lip Development (6-8 weeks)
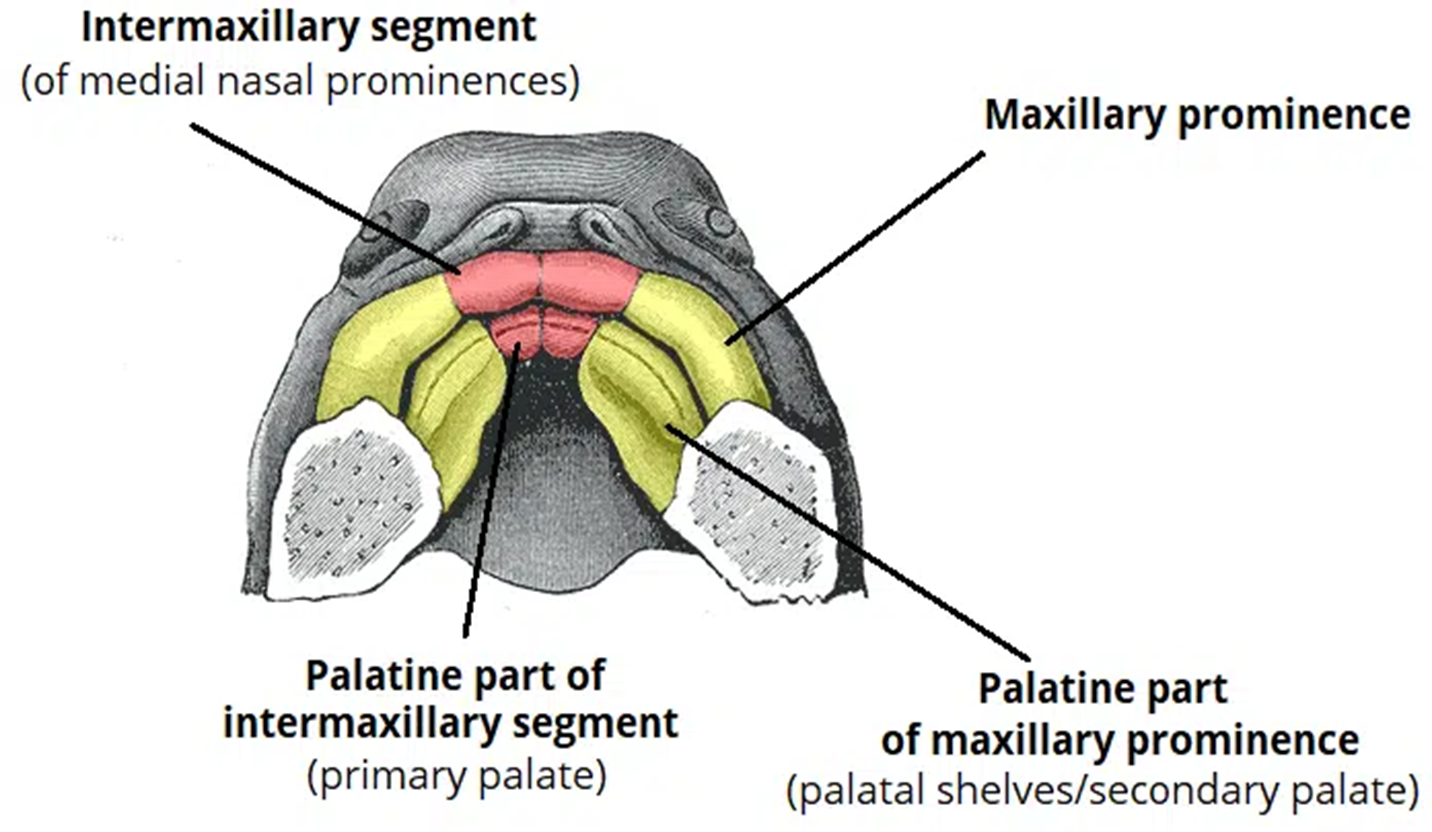
Stepwise Separation of Nasal and Oral Cavities:
Initial continuity between nasal cavity and oral cavity, separation leads to palate formation.
Fusion of medial nasal prominence creates the intermaxillary segment, forming the primary palate (anterior 1/3 of current palate) and contributes to the philtrum and upper four incisors. Main features of the nasal cavity.
Palatal Development:
Maxillary prominences expand to form palatal shelves which fuse above the tongue.
Fusion occurs in the horizontal plane of palatal shelves and vertical plane of nasal septum to form secondary palate.
Mouth and jaw.
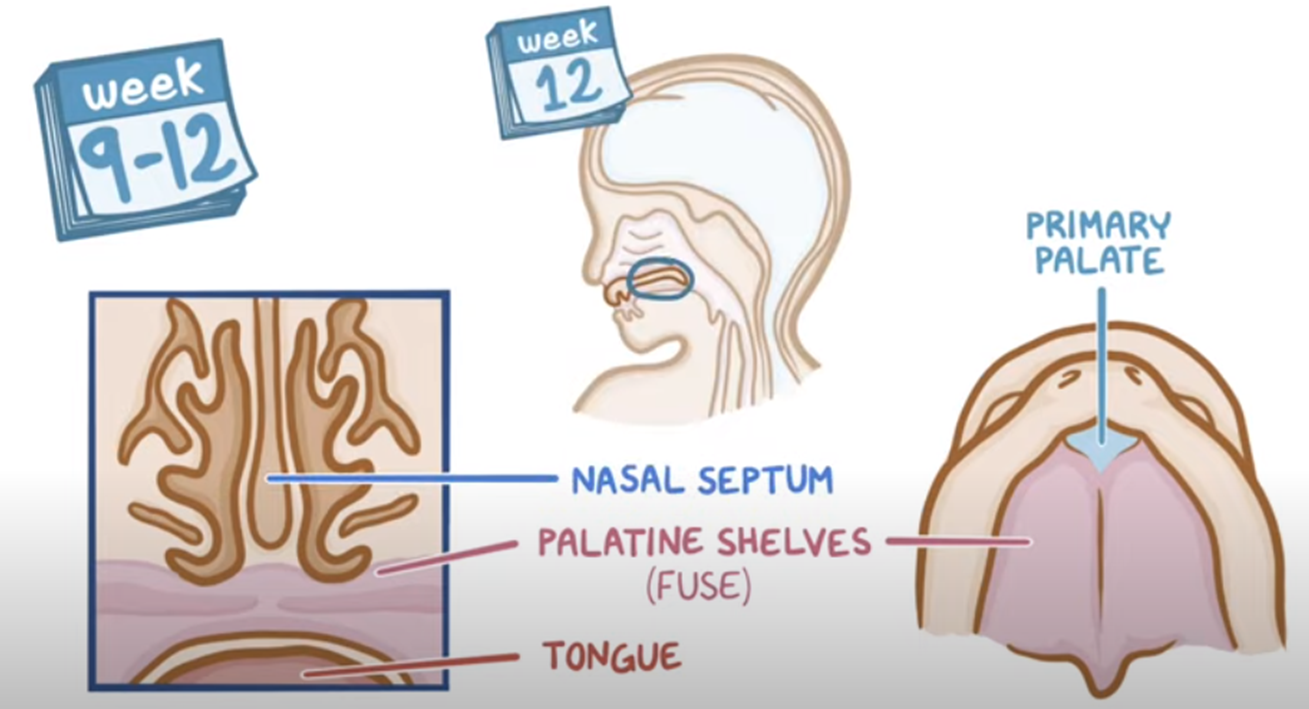
Development Timeline
Weeks 8-9: Formation of primary palate and palatine shelves begins.
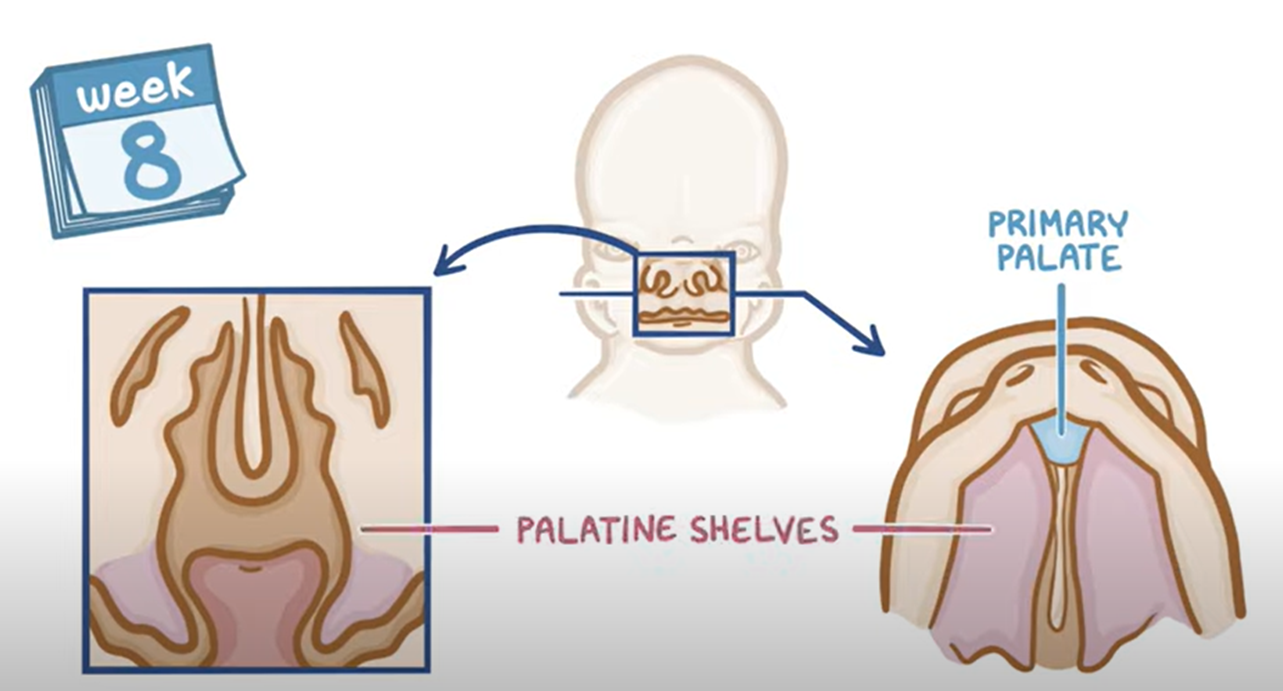
Weeks 9-12: Palatine shelves fuse with the nasal septum, establishing separation between oral and nasal cavities.
Airway not fully formed.
Small tongue.
Brain not fully formed (only basic functions).
Jaw Development
Mandible Development:
Occurs around 8 to 14 weeks of gestation, with trabecular bone formation providing muscular attachments for mastication muscles.
Separation from Meckel cartilage and formation of condyle blastema.
An Infants Mouth
Soft palate is really long for protection and to aid suckling.
Dome shaped palate.
Newborn Key Points
Mouth and throat structures in close proximity.
Limited open space within mouth and throat areas.
A small, slightly pulled back lower jaw.
Wide ‘u’ shaped palate.
Flexible/ moveable palate.
Nose breathing
Large tongue
Deeply cupped tongue when suckling.
Enlarged gums to assist latch.
Ample sucking pads in the cheeks.
Horizontally positioning of the Eustachian tubes (middle ear to the back of the nose).
Potential Developmental Issues
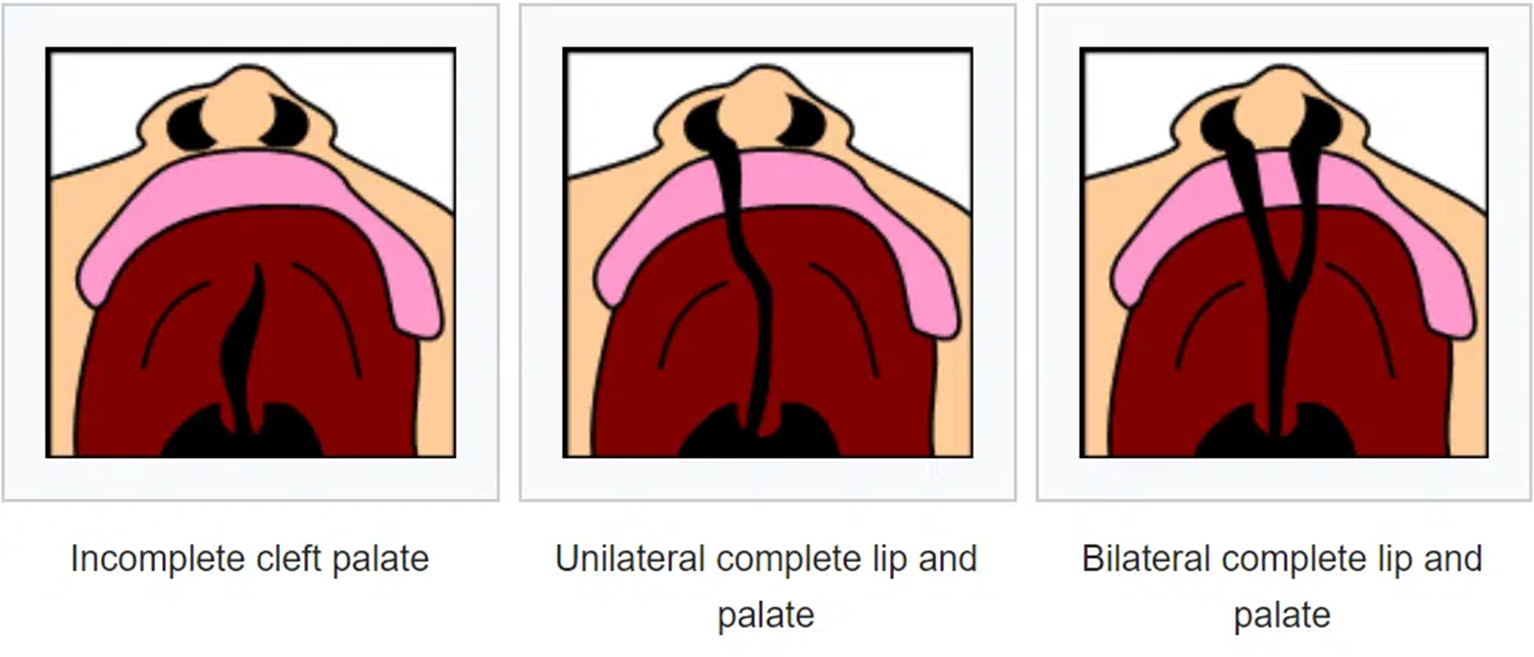
Cleft Palate:
Types: Incomplete cleft palate (can get it at any point), unilateral complete lip/palate, bilateral complete lip/palate.
That is why it is called cleft lip and palate.
Micrognathia (when the jaw doesn’t develop):
Doesn’t receive the signaling to grow.
‘Small jaw’.
Over compensatory movements.
Causes include genetic conditions: Achondrogenesis, Pierre Robin Syndrome, Stickler syndrome, etc.
Treatment Approaches
Micrognathia:
No treatment needed if self-correcting, typically resolves by 6 to 18 months.
Severe cases may require a feeding tube or surgery for airway management and jaw alignment or to enlarge.
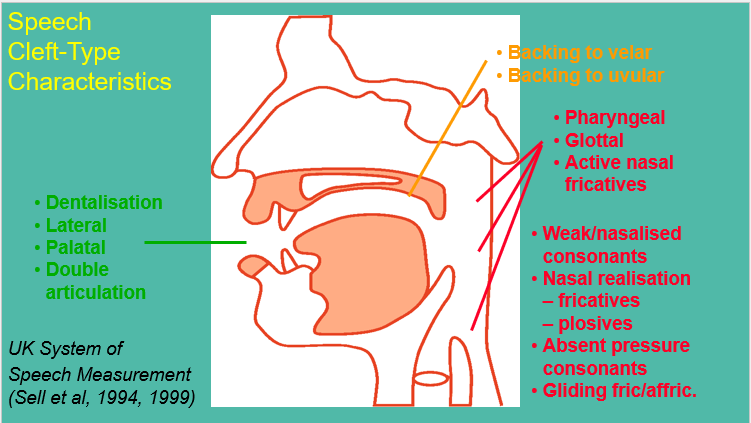
Speech Difficulties:
Various speech disorders associated with cleft conditions, including hypernasality and articulation errors.
Extended IPA:
Labioalveolar- bottom lip on the alveolar ridge.
Lingolabial- using the tongue instead of the bottom lip. Both due to the underdeveloped structure.
Cleft Lip and Palate Overview
Prevalence: About 1 in 700 children born with cleft lip and/or palate annually in the UK (CRANE Database, 2012).
Management: Lifelong, interdisciplinary approach, addressing speech, hearing, appearance, facial growth, and psychosocial aspects. Audiologists, surgeons, orthodontists, psychologists also in the team working with the child. Also speech and feeding. Measures of facial symmetry, speech assessments (specific), psychosocial well-being analysis.
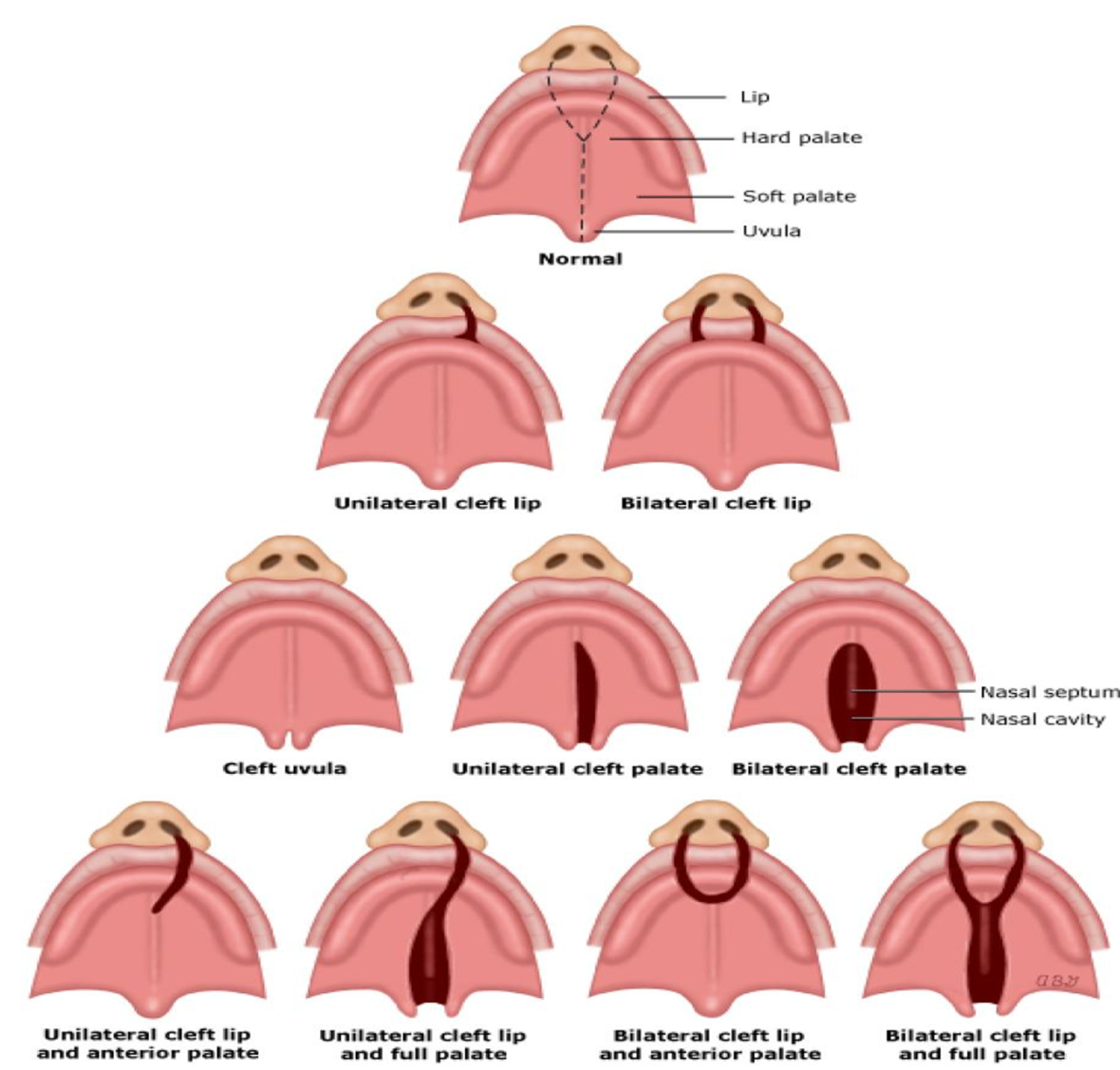
Definition of Cleft Palate:
A gap or split in the upper lip and/or palate due to improper joining during fetal development.
Types of Clefts:
Including unilateral/bilateral cleft lip, cleft palate types (hard, soft, or both), and submucous cleft palate (bony parts and muscles have not formed).
Reasons for Cleft Formation
Etiology: Undefined causes with potential genetic factors (e.g., TBX22), nutritional imbalances, and various maternal risk factors (drug/alcohol use, obesity, etc.).
Associated Syndromes
Syndromes Correlated with Cleft/VPI: DiGeorge syndrome, Pierre Robin Sequence, Treacher Collins syndrome, among others.
Velopharyngeal insufficiency (VPI): oral pressure to produce sounds, problems closing the nasal cavity.
Hyponasal speech: problems opening the nasal cavity. Too little air.
Hypernasal speech: lots of air coming through the nose.
Impact Assessment
Effects on Quality of Life: Facial appearance, feeding and speech difficulties, psychosocial issues, and dental problems.
Multidisciplinary Team Involvement
Team composed of various specialists: SLT, maxillofacial and plastic surgeons, psychologists, psychiatrists, orthodontists, and community services.
Treatment Protocols
Primary Treatment: Surgical repair of hard and soft palate, typically between 6-12 months.
Secondary Surgery: Required at skeletal maturity (14-17 years) for additional corrections or improvements.
Key Surgical Procedures
Early Palate Repair: Typically done between 6-12 months, focuses on closing gaps and re-arranging palate muscles.
Secondary Surgical Options: Include alveolar bone grafts, maxillary distraction osteogenesis, and aesthetic corrections.
Speech and Language Therapy
Types of Therapy and Interventions: Direct and indirect approaches designed for early intervention, articulation improvements, and addressing specific developmental errors related to cleft conditions.
Early intervention: monitor and influence infant phonetic development, monitor overall communication and interaction development, monitor hearing, tune parents into speech development, parental advice- verbal and written and input modelling therapy.
Input modelling therapy: psycholinguistic model of intervention working on input only, targets phonological representations, SLT/ parent provides clear model/ auditory bombardment in play, multisensory approach (visual, auditory, tactile) and pressure free, child not expected to respond.
Assessment (GOS.SP.ASS)
Get them to say numbers
Say sentences and they repeat.
WI and WF separate, assess these separately.
All trained to hear the different cleft sounds- to score them and need to be in agreement.
Cul de sac: can’t do it.
Nasal emission: hear air coming out through the nose in certain sounds. Known as obstruents (obstacles).
Nasal turbulence: nasal snort.
Grimace- structures around the lip alinged.
Posterior: back
Anterior: front
Passive: can’t get the pressure. /s/>[n] and /d/>[n]. Sonorants and gliding. Not much what SaLT can do if they can’t physically get the sound. Back to surgery.
Speech errors (cleft): dentalisation (tongue between the teeth), palatilisation (/j/ sounds and laterlisation /ll/ and backed to velar/ uvular- /ch/.
Error Type | Intervention |
Anterior Errors | Therapy |
Posterior Errors | Therapy |
Non-Oral Errors | Therapy |
Passive Errors | Surgery |
Cleft Specific Thoughts
Always consider hearng status- glue ear
Always consider other speech/ language impairements
Oral structure is crucial
May have to wait for a VF
May only achieve best possible production
Visual tools important
Further specialist assessments/ second opinion
Family may have to travel for specialist support
Good liaison and training vital locally.
NHS links for EHCP etc.