lecture 11: oral tolerance
 gut epithelial cells are able to express of prrs especially toll like receptors so can bind certain microorganisms through their PAMPs. This means that they can be a target and produce stress signals which intraepithelial lymphocytes can respond to. This means that there is immuno surveillance even in enterocytes.
gut epithelial cells are able to express of prrs especially toll like receptors so can bind certain microorganisms through their PAMPs. This means that they can be a target and produce stress signals which intraepithelial lymphocytes can respond to. This means that there is immuno surveillance even in enterocytes.
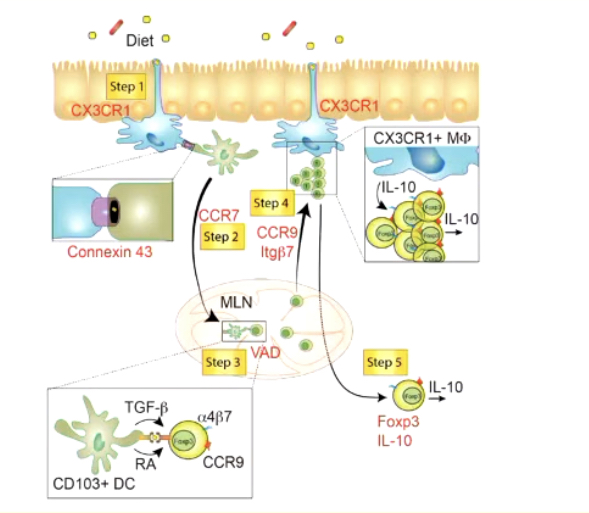
Below enterocytes, there are macrophages. Dendritic cells can grab hold of antigens which can pass through M cells where they are exposed to that antigens. Macrophages can also play a role in this too in this regulatory environment required in the gut. Macrophages are able to get a hold of molecules from our diet and have conversations with lazy dendritic cells. This means that they are only woken up in the presence of significant antigenic cells
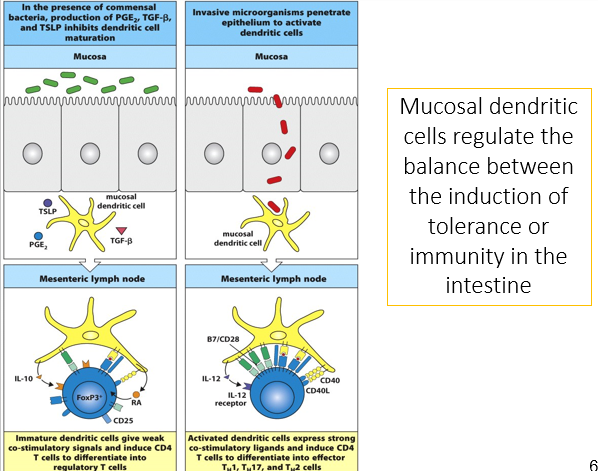
If an antigenic pathogen is detected, the dendritic cells will pass the information into the mesentery lymph node to a T cell. There have been certain cytokine and chemokine profiles generated by the macrophage which tell the dendritic cell that the antigen is pathogenic, however a different one will be generated if it is not - TGF beta which will lead to a suppressive immune cell differentiation such as T reg cells. IL-10 is still expressed by macrophages to show a non danger environment which aid in the proliferation of T reg cells. This suppresses effector T cells (TH 1,2,17). This is the mechanism of oral tolerance and this is peripheral.
There are two types of tolerance:
central tolerance - being able to tolerate our own proteins and cell surface markers
this happens in the thymus and bone marrow in T and B cell maturation which are removed if they recognise
some T and B cells will be released that recognise however, there is peripheral tolerance in lymph nodes
This will create anergic T/B cells which means that they will not mount a full response
Peripheral tolerance
Autoimmune diseases break tolerance and so cells are not tolerant towards own cells.
Enteric pathogens cause a local inflammatory response by PRRs and TLRs that are on epithelial cells recognising a pathogen and ligating to it. This stimulates the release of cytokines and chemokines that attract monocytes, eosinophils and T cells out of the blood and release antimicrobial peptides. Tissue resident dendritic cells are also attracted by stimulation of costimulatory molecules such as B7 and CD40/CD40 ligand to bind to the T cell, overcoming the normal unresponsive state.
There are certain pathogens that targets this process such as salmonellae. Salmonellae enters and kills M cells so can then access underlying tissues and infect macrophage and epithelial cells.
The major role of mucosal immunity is to protect against a variety of enteric pathogens. The response must be able to recognise and respond to any pathogen but not respond or produce the same response to harmless antigens such as food or commensal organisms. The mucosal immune response has to balance these needs
The majority of antigens in the intestinal tract come either from food or commensal bacteria not from pathogenic organisms. Oral tolerance is about tolerating ingested stuff but is not tolerance towards commensal bacteria. These however, do not raise an immune response even though these antigens are considered non self.
This is important for vaccine development as if you’re trying to produce an oral vaccine, you have to be able to overcome oral tolerance to produce an immune response against that antigen or pathogen. This is important for creating vaccines against gut immune protection. These vaccines generate local IgA responses as well as systemic IgG responses. This process can also be used to overcome certain allergies such as food allergies by slowly introducing small amounts of the protein to build up tolerance
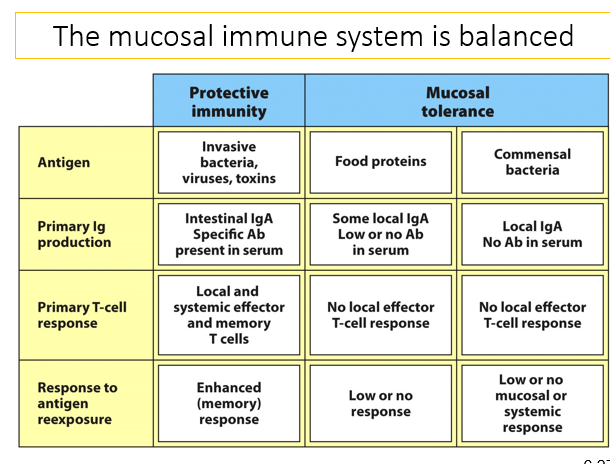
The mucosal immune system is balanced between protective immunity and mucosal tolerance. There is protective immunity against invasive bacteria and viruses and toxins and primarily produce intestinal IgA and specific antibodies. There are also local and systemic effector and memory cells which enhances the memory response. In mucosal tolerance, there is tolerance against commensal bacteria and food proteins. Towards food proteins, there is some local IgA but low or no antibodies and local effector T cell responses. This is also the same for commensal bacteria and have low or no response to antigen reexposure. Commensal bacteria have low or no mucosal or systemic response. This is because you still need to be able to produce an immune response to commensal bacteria that might be found in the wrong compartment - E coli in the gut wont make an immune response however will if the E coli was found in a cut.
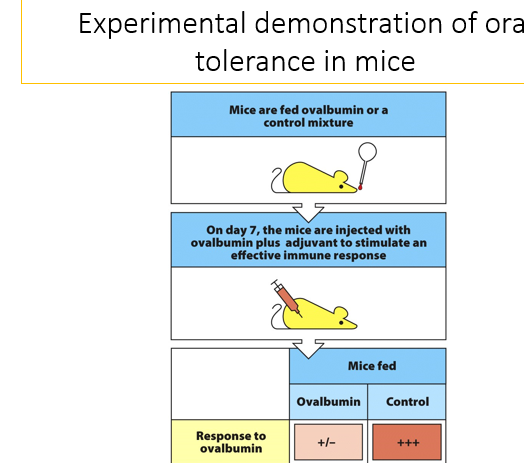
Showing the process of oral tolerance in mice
Mice are first fed ovalbumin or a control mixture and over the course of 7 days, are given little bits of this protein. On day 7, they are injected with an ovalbumin plus adjuvant to stimulate an effective immune response in the systemic system. In the mice that were fed ovalbumin, there is a very small immunological response as they have been given peripheral tolerance to create a systemic tolerance. Control mice who were not exposed to ovalbumin has a huge immune response. This means that you can create systemic tolerance through oral tolerance routes which means that you can provide tolerance towards food proteins in allergies.
If a commensal bacteria was used and fed orally, it would be seen as being in a separate compartment which would cause an immune response.
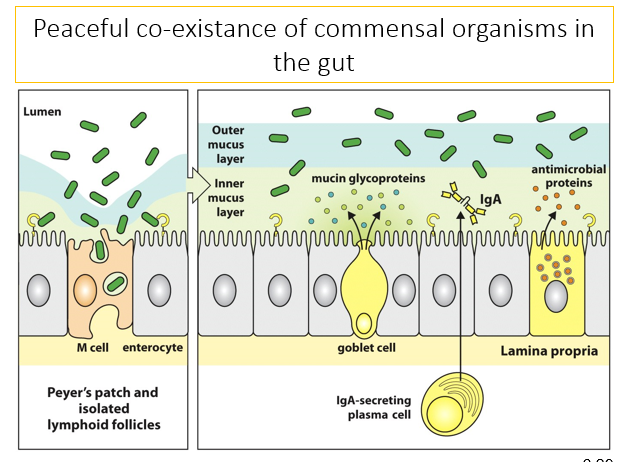
Goblet cells produce and secrete mucin glycoproteins to the inner mucous layer. there is also IgA secreted from inside the peyer’s patch by plasma cells from low level stimulation as well as Paneth cells which secrete antimicrobial proteins. These features act to protect against pathogens and continual bombardment by commensal bacteria. Commensal organisms make up the outer mucus layer however, sometimes they can get through into M cells and into the Peyer’s patch and isolated lymphoid follicles. They don’t activate dendritic cells as they dont have PAMPs or other danger signals so although are taken up by dendritic cells, they don’t snap them out of their sleepy state. When this is presented to T cells, it will allow differentiation of the T cells into regulatory cells. This all prevents overstimulation by the commensal organisms.
In the presence of commensal bacteria, the production of PGE2, TGF beta and TSLP that inhibit dendritic cell maturation- this is what stimulated by the commensal bacteria and suppresses the immune response and create a regulatory response. This means that the dendritic cells giveweak co-stimulatory signals and induce CD4 T cells to differentiate into regulatory cells. These generate anti inflammatory cytokines and stimulate an IgA class switching
Since no cytokines are released, there is no inflammatory response so no full immune response. This also applies for food antigens
When you induce and oral or mucosal tolerance, the levels of TGF beta is increased so more T regulatory cells are produced as well as an immunosuppressive properties. Generation of mucosal tolerance in animal models of inflammatory diseases has protective properties for that disease which raises the possibility of using induced oral tolerance treatment in human inflammatory disease - trials have not been promising for the treatment of establishes diseases.