Lecture 4: Soft and Hard Tissue Considerations for Future Implant Placement
Saving Teeth
If you can save the tooth, don’t think about an implant!
Endodontic TX
Endodontic surgical TX
Endo Retreat
Periodontal TX
periodontal Regeneration
Before removing any tooth (except 3rds) you should have a plan and give options to your patient
Ridge Preservation
How much shrinkage horizontally and vertically, grafted vs non grafted
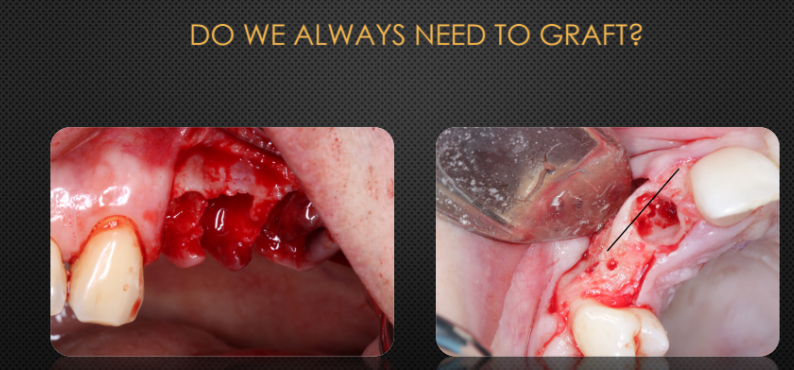
Do we always need a graft?
Do we need a graft?
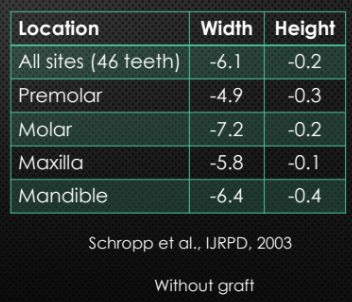
Ridge changes 1 year after single tooth extraction
greatest loss was ridge width
Greatest loss happens in the first 6 months to 1 year
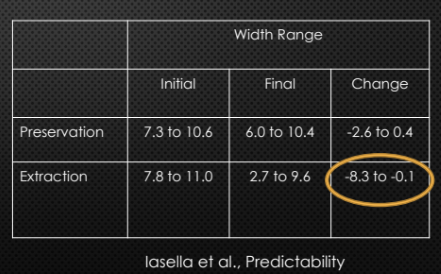
Ranges is the major problem. Loss of width can be unpredictable
graft is the key to predictable management
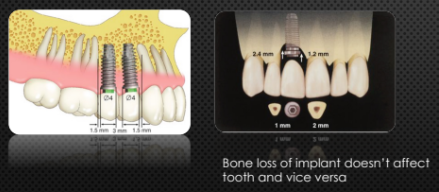
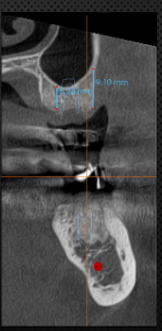
Minimum Required Bone
Mesial and distal: 1.5mm from natural teeth and 3mm between implants
2mm safety zone from anatomical structures8mm long implant, 10 mm from IAN canal
Facial bone: 1 mm facial and lingual
Bone graft in minimum exposure of implant threads, submerge and primary closure
Platform of implant: 2mm bellow the CEJ (3mm for ant teeth)

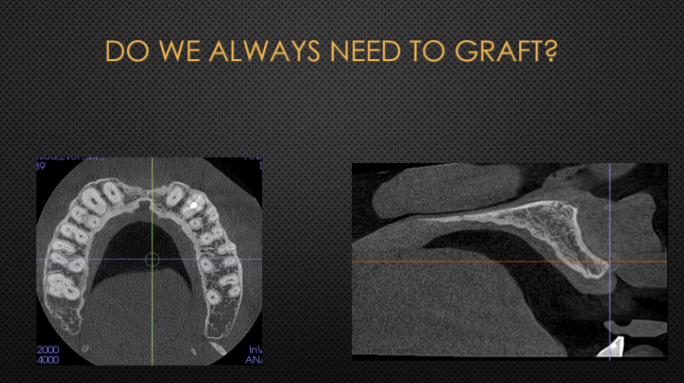
Do we always need to graft?
Type of the bone and Maxilla vs Mandible:
type of the bone may not matter as much as the thickness of the walls
thickness of facial bone!
Facial fenestration, dehiscence, loss of facial bone, infection around the tooth


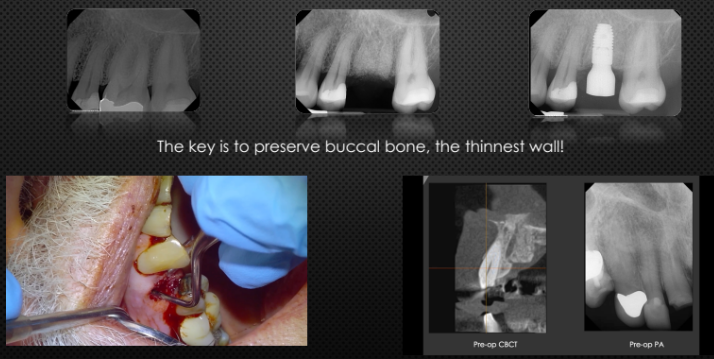
Ridge Preservation
The key is to preserve buccal bone, the thinnest wall!
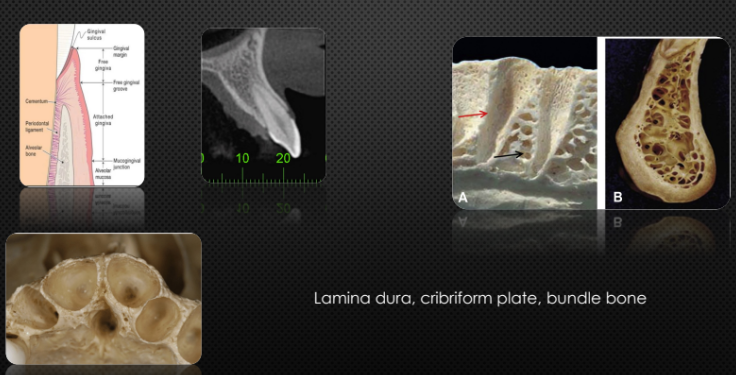
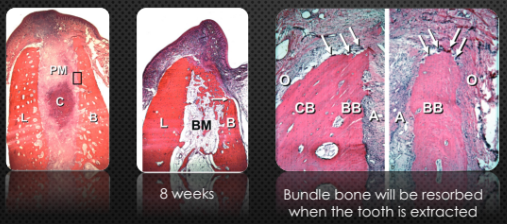
Bundle Bone Resorption
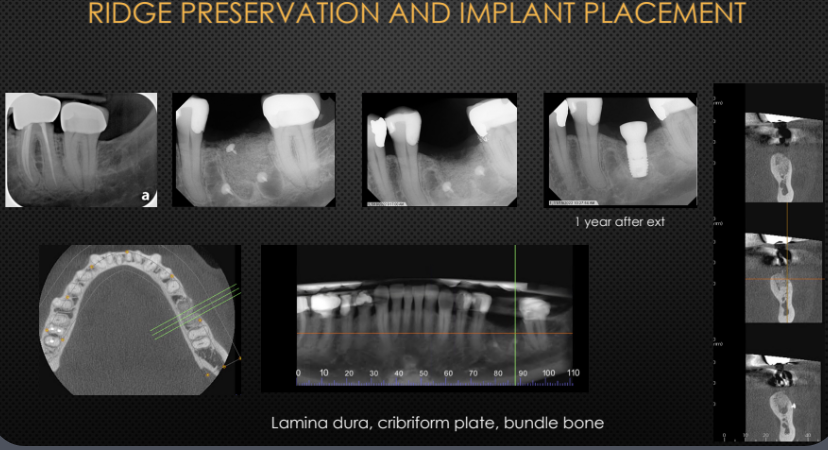
Lamina dura, cribriform plate, bundle bone
Bundle bone resorption after tooth extraction
Bundle bone will be resorbed when the tooth is extracted
same result for immediate implant
bundle bone replaced by woven bone
Atrophy of the edentulous ridge will occur following tooth loss. The contraction of the ridge cannot be prevented by placing an implant in the fresh extraction socket

Ridge preservation and implant placement

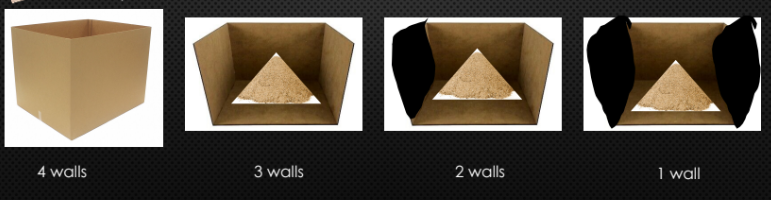
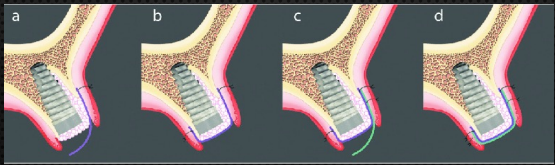
Defect Types
4 wall defect is the most predictable site to graft
3 wall defect → when there is no facial wall
When the ridge is completely collapsed → no wall defect! →vertical GBR (very difficult and not predictable)
We don not have 4 wall defect around an existing tooth, the 4th wall is the tooth!
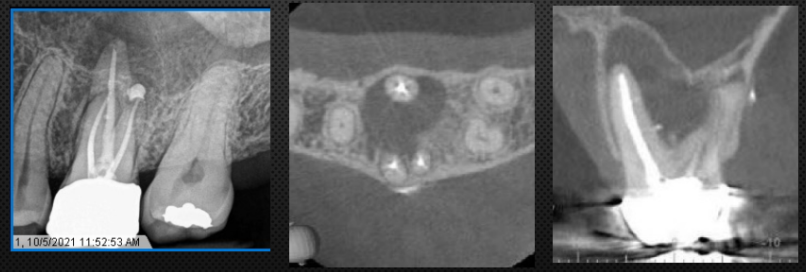
Grafting after extraction of tooth with infection
Is it a contradiction for grafting?
No!
Tooth with infection usually have more bone loss (Radiolucency on the radiograph)
No bone graft in case of infection that has spread to facial spaces or patient has systemic symptoms such as fever
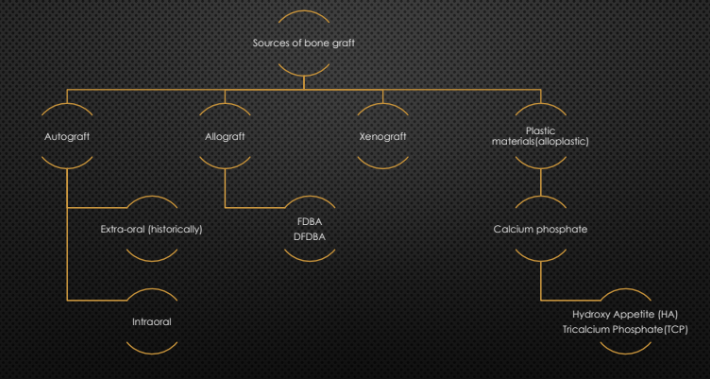
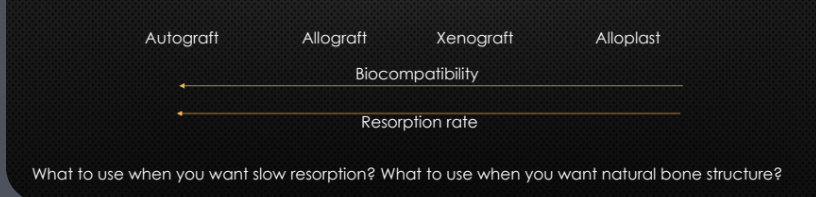
Different Materials
Different Graft types- Adv and disadv
Types of Grafts
More predictable outcome
Less number of the walls → More bone resorption
Thinner walls→ more bone resorption
infection around the tooth→ more bone resorption (larger defect)
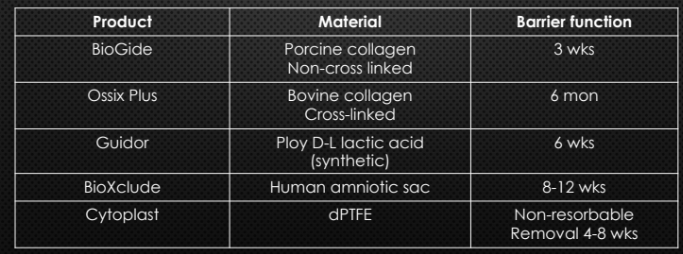
Do we need a membrane? What are the types?
Soft tissue grows much faster than bone tissue
soft tissue encapsulation of the bone graft
Types of membranes:
Resorbable
Collagen (Tendon) vs Synthetic
cross-linked vs non cross-linked
Cross-linked membrane will last longer
Non-resorbable
dPTFE (Titanium reinforced / no Titanium)
Good for maintaining spaces
big grafts cases or missing facial bone
DO NOT MEMORIZE THIS CHART
Different Techniques
Flap or flapless
Ice cream cone technique vs grafting of the facial out side of the socket
What to expect after ridge preservation, implant placement and sinus augmentation
Why do we graft after extraction?
What will happen if I don’t graft site #14?
Ext and Internal sinus augmentation? Min 5 mm is needed for internal

Soft tissue around implant
Peri-implant mucosal thickness and marginal bone loss
>2mm of thick tissue at the time of implant placement results in less marginal bone loss

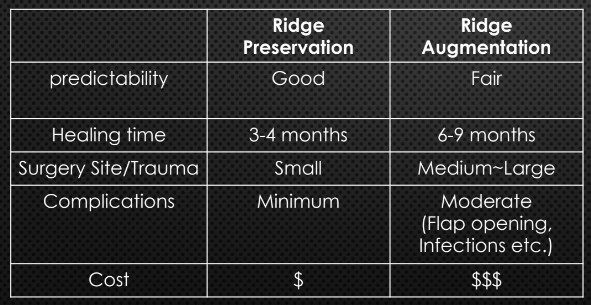
Ridge Preservation vs Ridge Augmentation (GBR)
Make sure you plan ahead to avoid ridge augmentation