Learning and Memory
What is Memory?
Montreal Neurological Institute
If you recall, at the beginning of this course, you learned about Wilder Penfield and the Montreal Neurological Institute. That institute is famous in the field of neuroscience for reasons beyond Penfield’s groundbreaking research. Back in the 1950s, neurosurgeons there were working on a new treatment for severe epilepsy. They would identify where in the brain a seizure was originating and remove that part of the brain to prevent future seizures. Back then, they did not have the kinds of medications we have today to treat epilepsy.
Henry, Patient H.M.
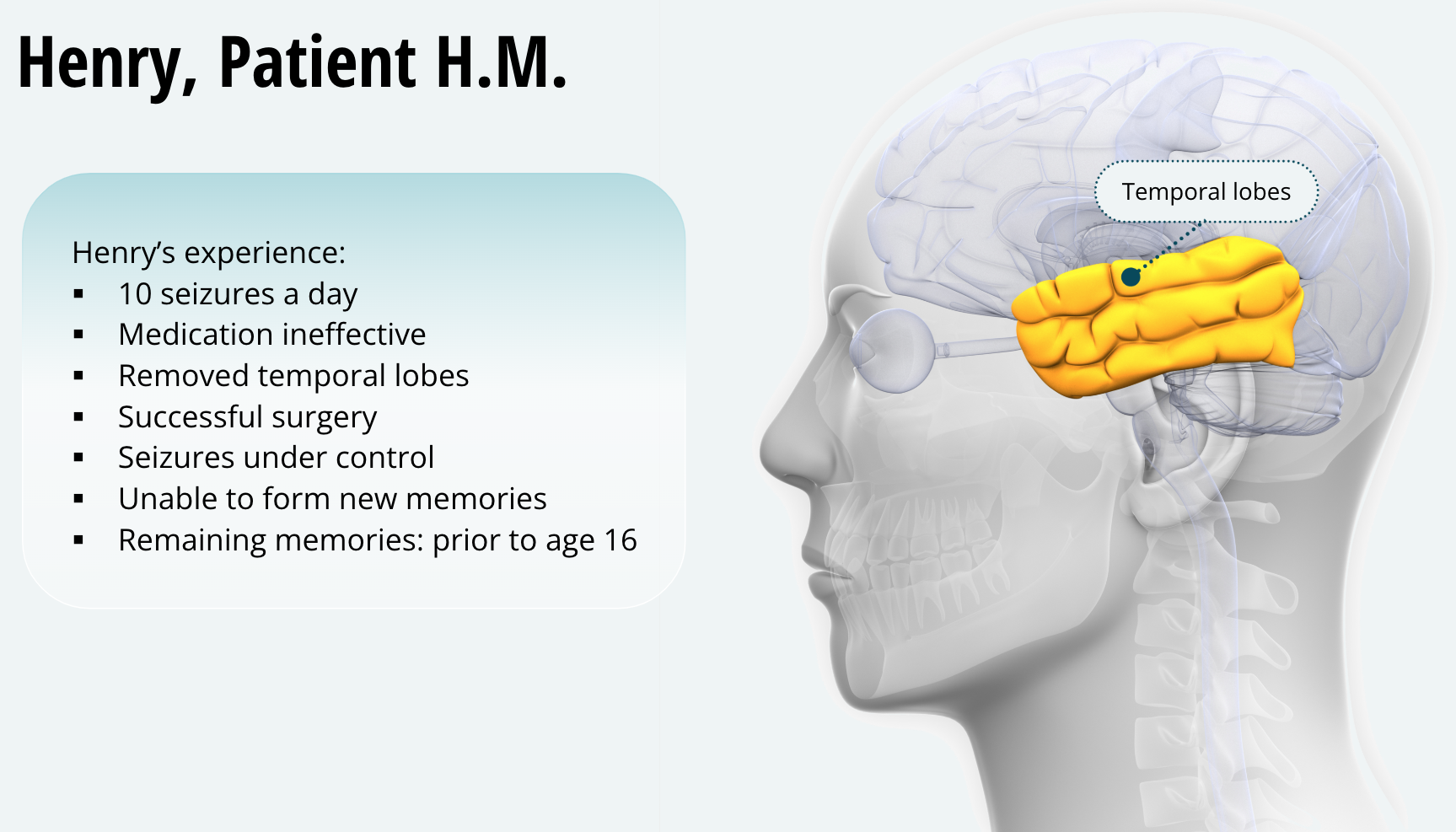
Around that time, a man named Henry checked in for treatment. He had been having about ten seizures a day and medication was not helping. The doctors figured out that his seizures were originating in both his temporal lobes and proceeded to remove that area of the cortex. The surgery was a success, and Henry’s seizures were now under control. Henry, or “Patient H.M.,” as he was known during his lifetime, was about to become the most studied human being ever, with hundreds of research reports published about him. As it happens, Henry’s seizures were much better after his surgery, but there was one problem — Henry was unable to form any new memories. For him, every day was like the movie Groundhog Day. In fact, after the surgery, he was unable to recall something that occurred a few minutes ago, and for the rest of his life, the only memories he had, were those prior to age 16.
Amnesia and the Hippocampus
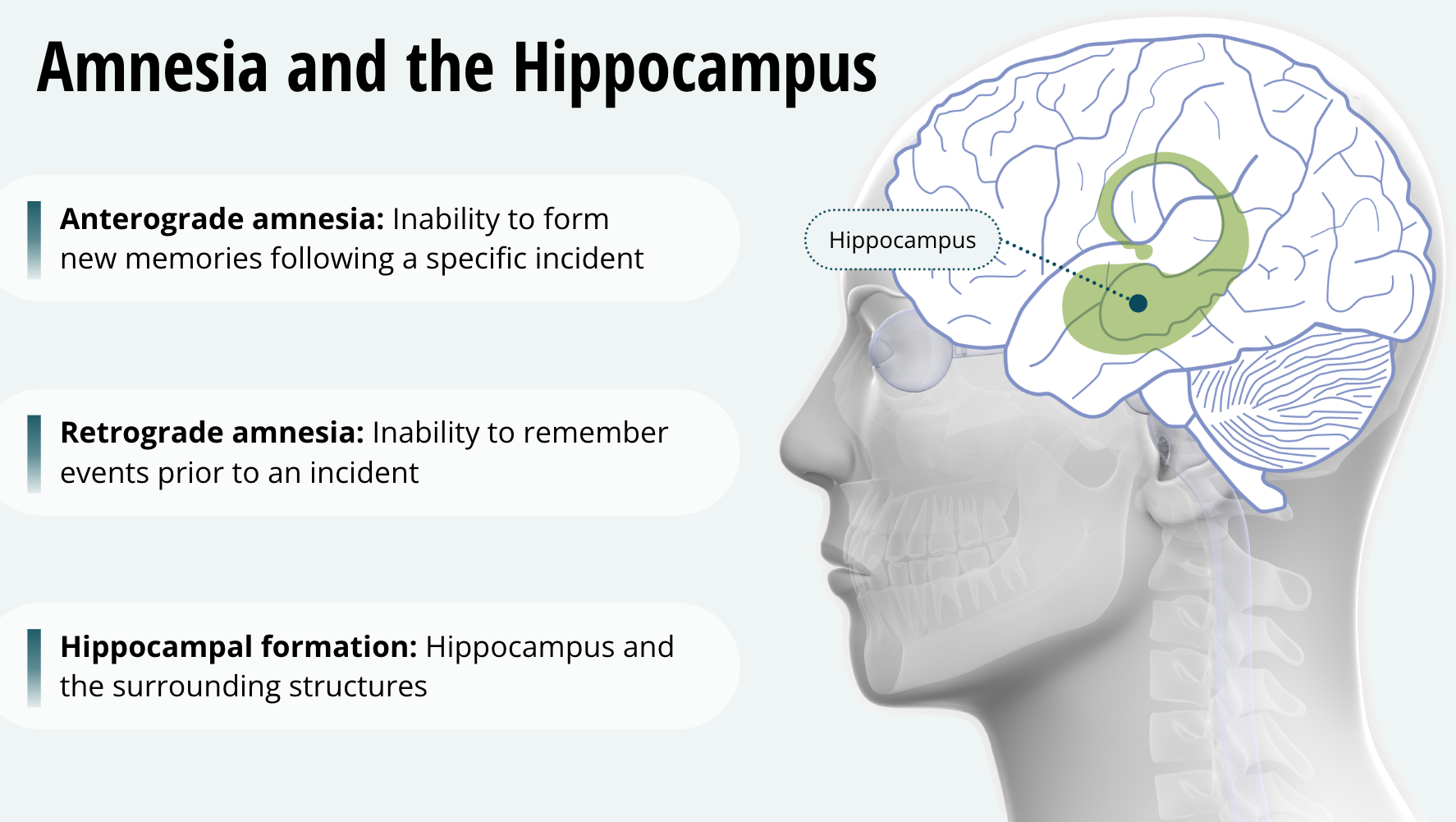
The inability to form new memories following a specific incident is called anterograde amnesia. Henry was not only unable to form new memories, but also had problems with memories prior to the surgery. He was 27 when he had the surgery. The inability to remember events prior to an incident is called retrograde amnesia. Given such severe memory deficits, neuroscientists were very interested in precisely what areas of the brain the surgeons had removed. They had removed his hippocampus and the surrounding structures known collectively as the hippocampal formation. As it turns out, we need our hippocampal formation to form new memories.
Categories of Memory
Henry was able to learn to trace a drawing in a mirror over time
Henry was unable to remember learning such tasks
Henry was able to learn some new things, such as tracing a drawing in a mirror, over time and with practice, although he could not remember learning the task. This shows that there are at least two categories of memory.
Nondeclarative Memory
Skills
Emotional learning
Stimulus-response learning
The fact that Henry could get better at some tasks with training meant he did have intact nondeclarative memory, which involves memory for skills, emotional learning, or stimulus-response learning. An example of nondeclarative memory is remembering how to ride a bike.
Declarative Memory
Facts
People
Events
Henry’s problem was with declarative memory. This involves memories of facts, people, and events that people can verbalize or declare. Examples of declarative memory would be what the name of an apple is or what you ate for breakfast this morning.
Types of Declarative Memory
Episodic Memory — Events
Semantic Memory — Specific Facts
Autobiographical Memory — Personal Information
Spatial Memory — Places and Locations
We can break declarative memory down into different subtypes. The memory for events, like a party you attended, is called episodic memory. The memory for specific facts, like the capitol of Canada is Ottawa, is called semantic memory. Memories that relate to yourself, such as your favourite food is pickled herring, is called autobiographical memory. And finally, the memory of the space around you and the objects located in that space is called spatial memory. An example of using spatial memory is going to the store but the normal, direct route is blocked so you have to use your spatial memory of the neighbourhood to figure out an alternative route to the store.
Multiple Memory Systems in the Brain
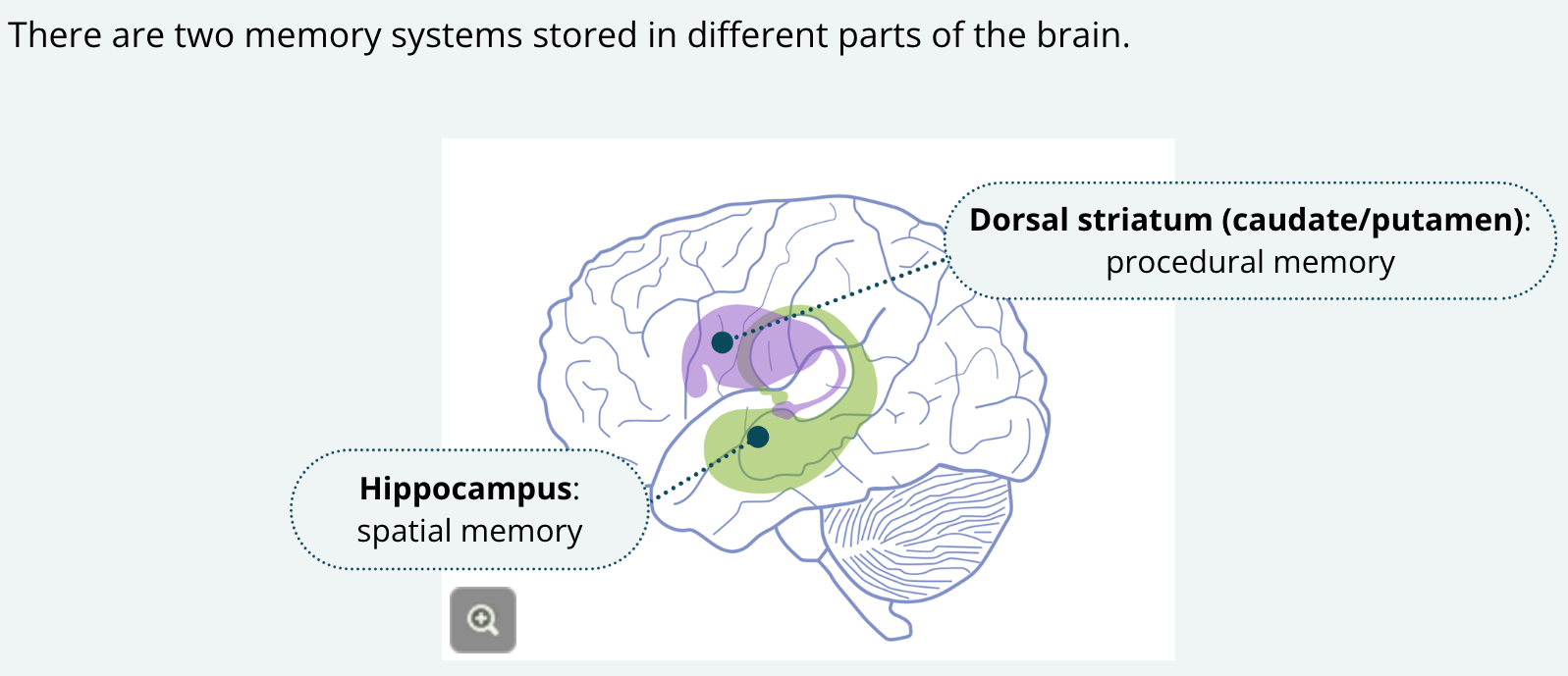
The fact that Henry was impaired with regard only to declarative memory but not nondeclarative memory, led neuroscientists to realize that these two memory systems must be stored in different parts of the brain. The evidence that we may have multiple memory systems and different brain regions responsible for each came from seminal studies by Dr. Norman White and his then student R.J. McDonald, and here’s a big surprise, those studies were carried out here in Montreal. They showed that, in the rat, the hippocampus is important for spatial memory and the striatum is important for procedural memory. Do you recall from earlier lessons what else the striatum (a.k.a. the caudate/ putamen) is important for? Research in my own lab at Concordia examines how these two memory systems in female rats are influenced by levels of the hormone estrogen.
Hippocampus vs. Striatum
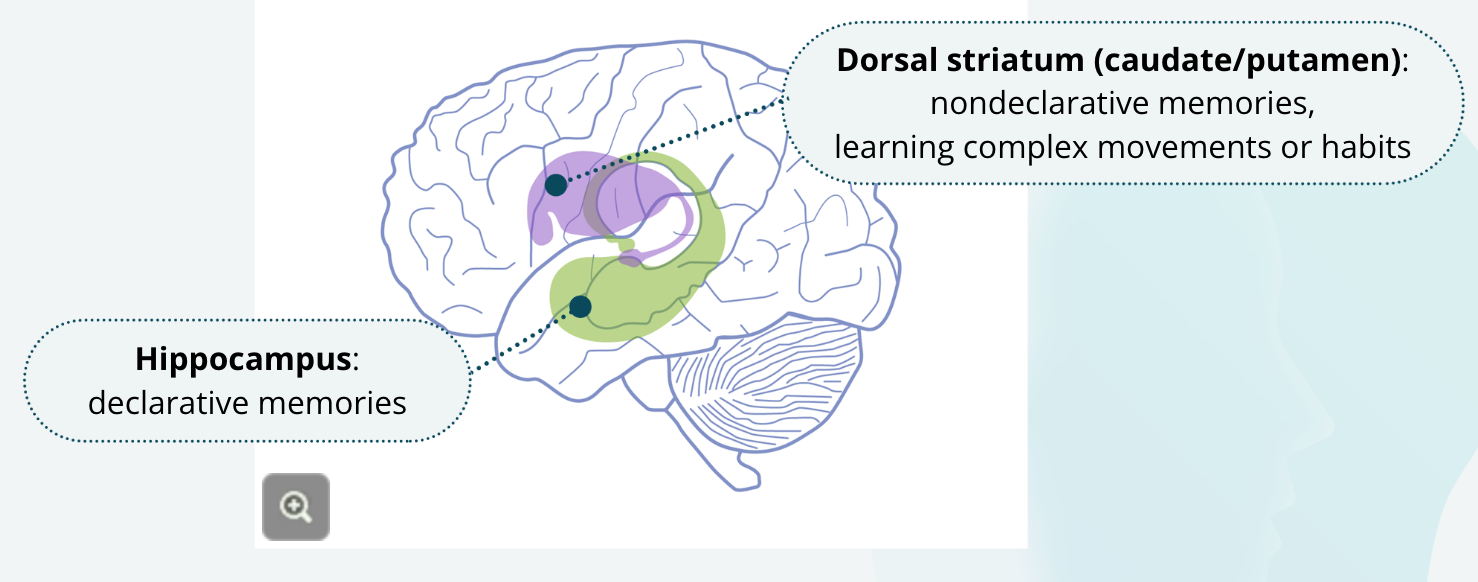
We now generally accept that, in humans, the hippocampal formation is important for learning declarative memories and the striatum is important for developing nondeclarative memories, but this should be intuitive to you after completing the previous unit. There we learned the importance of the striatum as part of the basal ganglia for learning complex movements, in a way that’s what nondeclarative memory largely is. Learning complex movements or habits.
Amygdala and Emotional Learning
Another area of the brain that is important for memory is the amygdala, which is involved in emotional learning, such as learning to fear something. The amygdala is also important for enhancing declarative memories. Studies have shown that if you include something very emotionally charged in an otherwise boring story, people will remember it better. Evidence suggests that the amygdala works with the hippocampus to store these more emotionally charged memories better.
Working Memory
Another type of memory is called working memory. Working memory provides a temporary register of information while it is being used. One way to think about working memory is that it is like random access memory or RAM in a computer. The RAM holds information temporarily while it is being used. I like to use the example of someone preparing a meal. While you are chopping the vegetables, you have to keep in mind that the sauce needs to be stirred, and you can’t let the roast burn. Keeping all this ‘in mind’ while you are working is what your working memory does.
Prefrontal Cortex and Working Memory
Seminal research conducted by Patricia Goldman-Rakic and her students using nonhuman primates showed that neurotransmitter dopamine in the prefrontal cortex is important for working memory. This research was not conducted in Montreal for a change, but at Yale in New Haven, Connecticut. Unfortunately, Dr. Goldman-Rakic’s important research on working memory was cut short because she was struck by a car and killed while crossing a street in 2003 in a small town in Connecticut. I am guessing you will now remember this potentially boring story much better because of the tragic and emotionally charged ending about Dr. Goldman-Rakic. You can thank your amygdala for helping out your hippocampus for that.
The Neurobiology of Learning
Memory Consolidation and Retrieval
Consolidation — the process of forming new, long-term memories, which involves forming a permanent representation of a memory in the brain
Retrieval — the process of accessing that stored memory or remembering it
The patient, Henry, with his memory impairments had two memory problems really. First, he couldn’t form new memories, that is, he had anterograde amnesia, and second, he couldn’t retrieve many of the old ones, in other words, he also had retrograde amnesia. The process of forming new, long-term memories is called consolidation. Consolidation involves forming a more or less permanent representation of a memory in the brain. Retrieval is the process of accessing that stored memory or remembering it.
Short-Term vs. Long-Term Memory
Our memories can be either short-term or long-term. When we first learn something, we hold it in short-term memory for a brief time. Unless we do something with that shortterm memory it can be lost forever. For example, when you look up an address, unless you write it down or so called, ‘memorize it’ you will forget it. If you do somehow ‘memorize’ it, then you turn it into a long-term memory using consolidation. Until a memory has been consolidated, it is very fragile.
Memory Storage in the Brain
As you can imagine from the previous lesson, the hippocampal formation is important for consolidation of new declarative memories. It appears that it can also play a role in memory retrieval, but its role in retrieval may be limited. We will get to mechanisms of how the brain likely consolidates memories in a moment but first it is important to review where memories are stored in the brain. While the hippocampus is important for learning new memories, memories are not permanently stored there. Evidence suggests that the hippocampus stores information temporarily in the hippocampal formation but later a more permanent, long-term memory is consolidated elsewhere in the brain.
Location of Long-Term Memories in the Brain
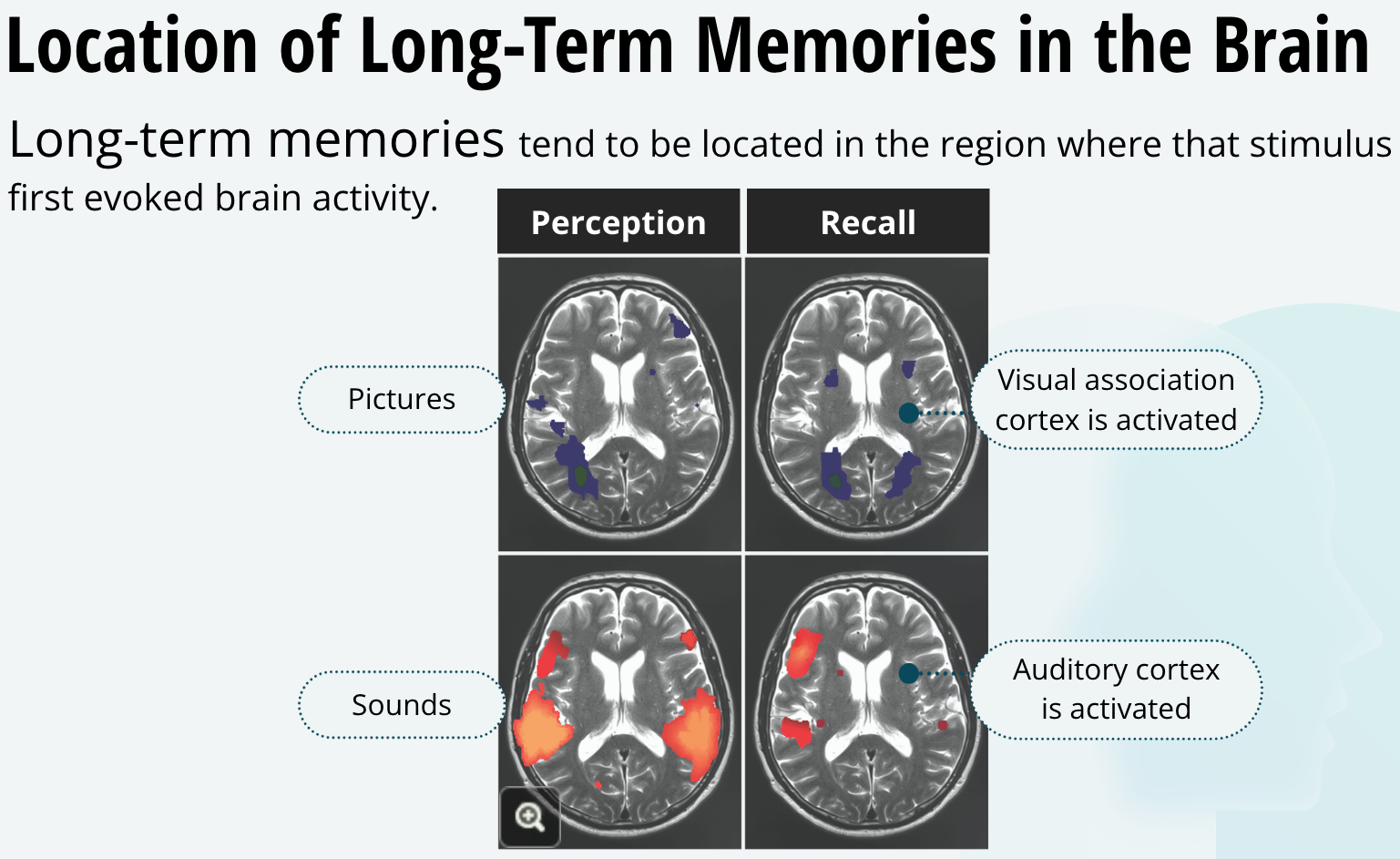
In general, long-term memories tend to be located in the region where that stimulus first evoked brain activity. For example, memories of sounds evoke brain activity in the auditory cortex where that sound itself initially activated brain activity. Similarly, memories of pictures activate areas of the visual association cortex where initially looking at the picture itself activated the brain.
Donald O. Hebb
Around the time that Penfield was establishing the Montreal Neurological Institute, a failed teacher from Nova Scotia heard about his fascinating work and wrote to him. Something in that letter must have caught Penfield’s attention, because he invited Donald Olding Hebb to come to Montreal to work with him. To be fair, after failing at being a teacher, Hebb did complete his Doctorate in Psychology at Harvard before writing to Penfield. Nonetheless, it would prove to be an auspicious partnership, as Hebb himself would make remarkable advances in how we understand the neurobiology of learning. At this point, it must sound like I am biased toward Montreal; one city with so many firsts for the field of neuroscience. All these people are highlighted for their contributions to neuroscience. Half a century ago was an exciting time for neuroscience discovery in Montreal. It still is!
The Hebb Rule
Hebb is most famous for his theories on the neurobiology of learning. He initially stated what we now call the Hebb rule. That is, if an axon of a presynaptic neuron is active while the postsynaptic neuron is firing, the synapse between them will be strengthened. By this idea Hebb was hinting, because they understood so little about synapses back then, that during learning synapses could be strengthened. Another way to think of the Hebb rule is the rhyme, “Neurons that fire together, wire together.” Most neuroscientists now believe that the Hebb rule is what mediates learning in the brain. The idea is that learning is a form of neuroplasticity that changes behaviour by remodeling neural circuits. Neuroplasticity is a general term we use when talking about changes in neural pathways or synapses. It is particularly helpful in understanding the changes that take place in the brain as a consequence of learning.
Classical Conditioning
To illustrate how the Hebb rule may work in the context of learning. Let’s look at a very simple form of learning called classical conditioning. It was Ivan Pavlov who, at about the turn of the century, discovered classical conditioning. This is when a behavioural response to a strong biological stimulus becomes paired with a previously neutral stimulus. When Pavlov would present his dogs with food, they would naturally salivate in anticipation of eating. After repeatedly ringing a bell just prior to presenting the food, eventually the dogs learned to salivate when they heard the bell – even in the absence of food.
How Pavolv’s Dog Learned
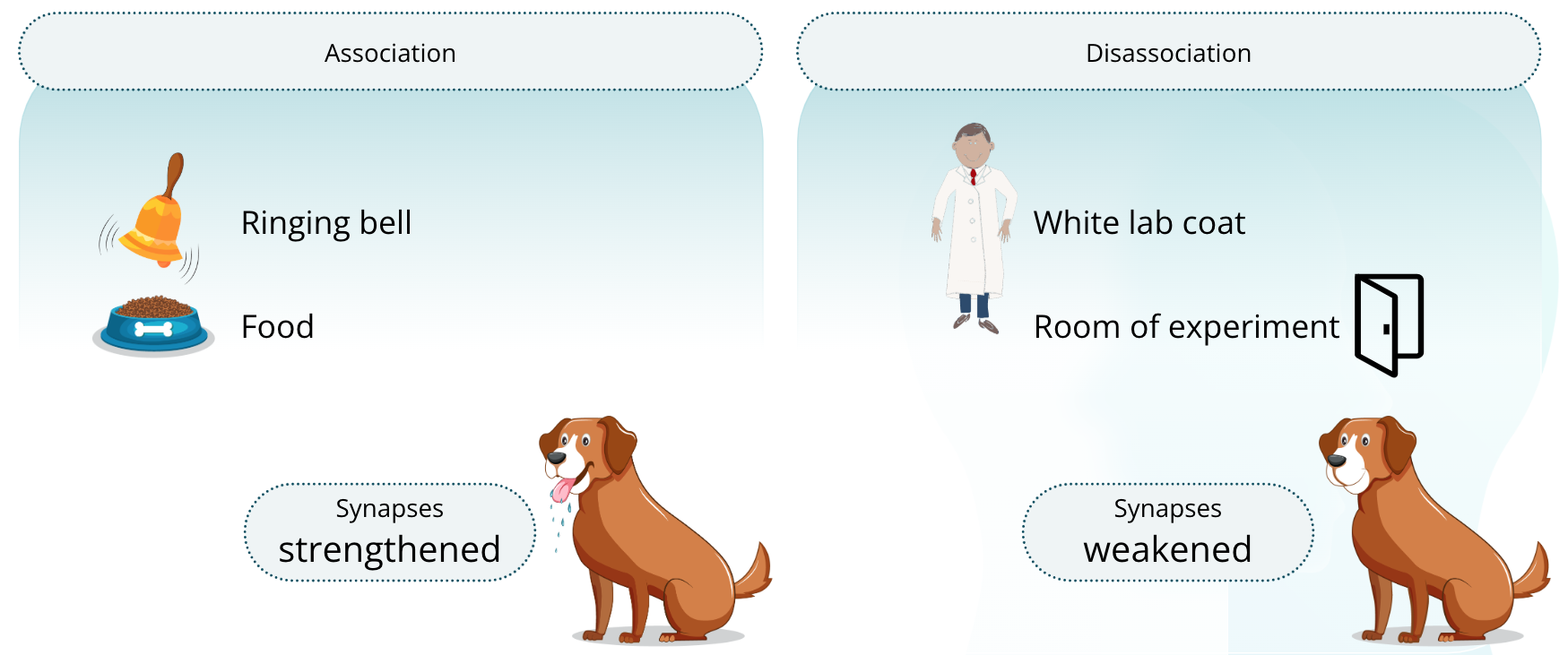
Just think a moment about what the dog needed to learn for this to happen. The dog had to associate the bell ringing with soon eating food, but it also had to learn that the dude in the white lab coat wasn’t associated with eating food– because he was there all the time whether the dog got food or not.
The dog also had to learn that the room in which the experiment took place, and many other variables did not predict food – because the dog wasn’t always fed in that room; only the bell always predicted food. So, the dog had to strengthen the association between the food and the bell while at the same time weaken the other associations. In neurobiological terms, it is hypothesized that the synapses between neurons encoding the stimulus of the bell, and the stimulus of the food were strengthened. On the other hand, the synapses between the neurons encoding the food and the neurons encoding the other irrelevant stimuli, like the dude in the white coat, were weakened. Let’s take this back to Hebb’s idea, if the bell rings exactly when the food is to be presented, then the neurons for the bell and the neurons for the food are firing at the same time. If they fire at the same time, according to the Hebb rule, the synapses will be strengthened.
Long-Term Potentiation (LTP) and Long-Term Depression (LTD)
LTP — an increase in synaptic strength resulting from the simultaneous activation of presynaptic neurons and post-synaptic neurons
LTD — a decrease in the strength of a synapse when stimulation of the presynaptic neuron is insufficient to activate the postsynaptic neuron
How the Hebb Rule Works
Video Summary:
Definition — LTP is a process by which synaptic connections between neurons become stronger with frequent activation. LTP is thought to be a way the brain changes in response to experience, and thus may be a mechanism underlying learning and memory.
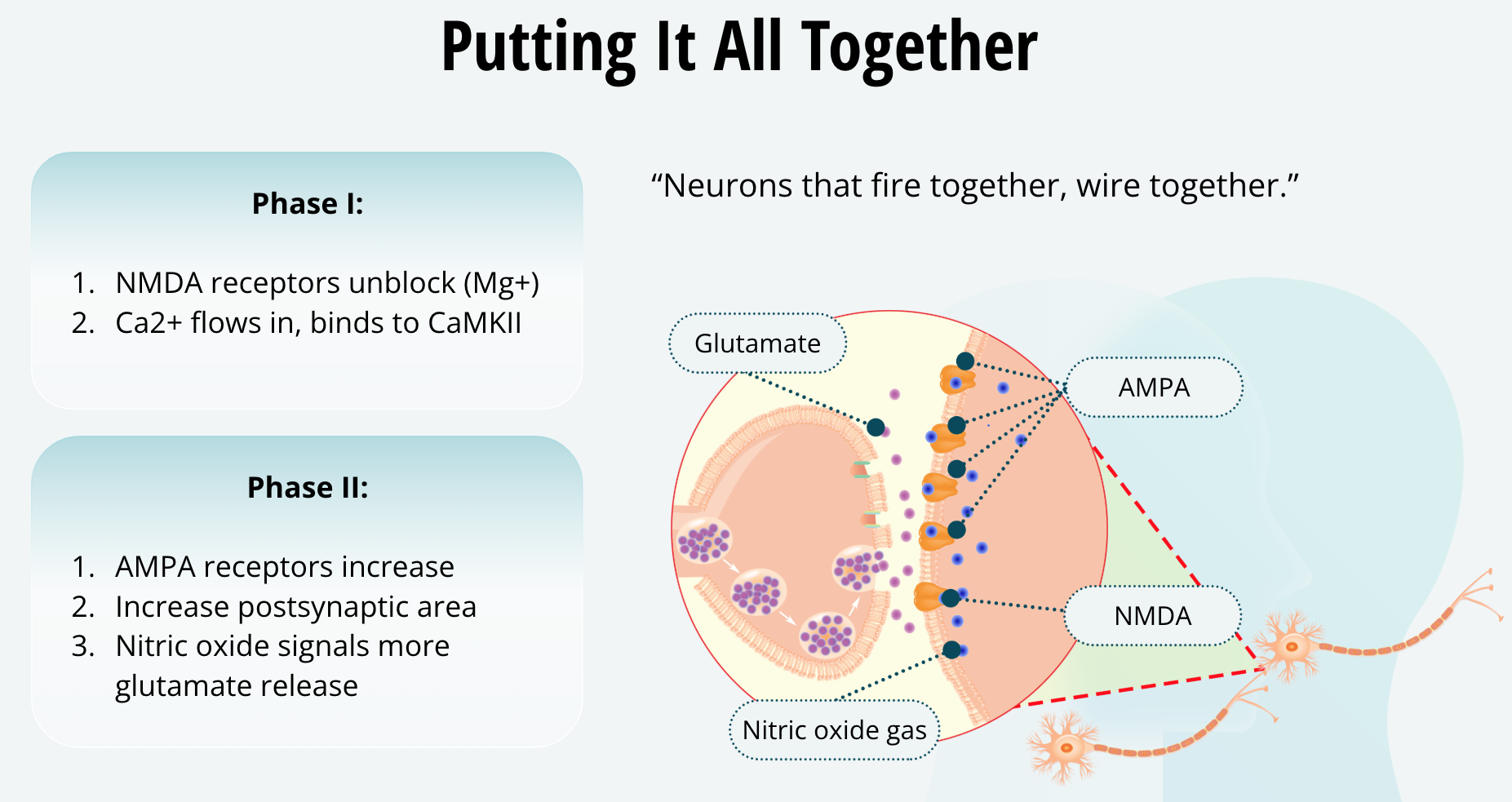
Mechanism — Glutamate release activates AMPA receptors, but not the nearby NMDA receptors because the latter has a voltage-gated magnesium ion blockage. If frequent action potentials cause greater stimulation of AMPA receptors, this will cause the postsynaptic neuron to depolarize, which will in turn remove the magnesium ion blocking the NMDA receptor. Once unblocked, calcium ions can flow into the cell via the the NMDA receptors. The influx of calcium ions initiates cellular processes involving CaMKII that insert additional AMPA receptors in the postsynaptic membrane, which are more sensitive to glutamate and allow more positively charged ions into the cell when activated. This makes the postsynaptic cell more sensitive to glutamate due to having more receptors to respond to it. Moreover, it’s believed that signals travel back across the synapse to stimulate greater levels of glutamate release.
Long-Term Potentiation (LTP)
Long-Term Potential (LTP)
One idea of how memories are stored in the brain is long-term potentiation. This is the idea that as we make associations and learn things, the connections or synapses between the neurons that encode those events become enhanced. Thus, it is believed that LTP represents a biological means of learning.
Simulating LTP in the Lab
In the lab we can artificially induce LTP by stimulating the presynaptic neuron with a pulse of high-frequency electricity using a stimulating electrode. When we do this for a few seconds the postsynaptic neurons will also start firing. In addition, when we later stimulate the presynaptic neuron with a regular pulse of electricity, the response of the post-synaptic neuron is much greater or potentiated. Moreover, this exaggerated response of the post-synaptic neuron lasts for months, hence the term, long-term potentiation. Most LTP experiments have been conducted in the hippocampus where it is relatively easy to induce, but LTP can occur elsewhere in the brain including the auditory, visual, and motor cortices. Basically, LTP can occur in any part of the brain where learning and memory are thought to occur. If we stimulate a neuron but use a low frequency pulse of electricity, the opposite occurs. That is, the response from the postsynaptic neuron becomes lower or depressed. So, by providing a weak stimulus, we can induce long-term depression or LTD.
Theta Rhythms, LTP, and Learning
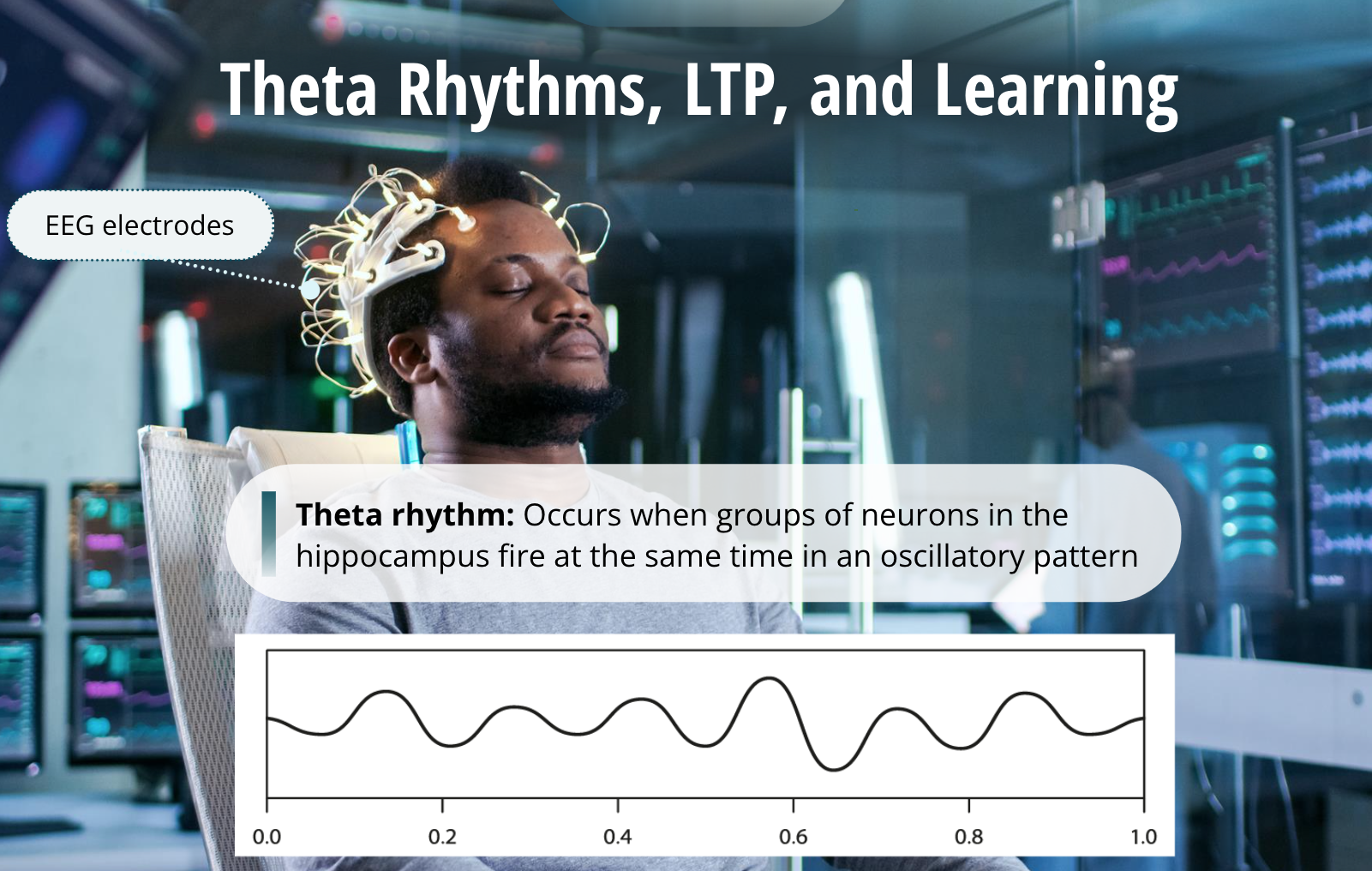
Of course, using a stimulating electrode in the lab is not the natural way this occurs. In the brain, LTP likely occurs in response to theta rhythm. Theta rhythm occurs when groups of neurons fire at the same time in an oscillatory pattern. Theta rhythm can be measured by recording electrodes in the brain or by electrodes placed on the scalp, that is, using an EEG. Theta rhythm often occurs in the hippocampus, and it can be observed in the rodent hippocampus when the rat is learning something new. When researchers suppressed theta rhythm in the hippocampus with a sedative drug, they were able to impair the rat from remembering where it had earlier went in a maze.
Mechanisms of LTP
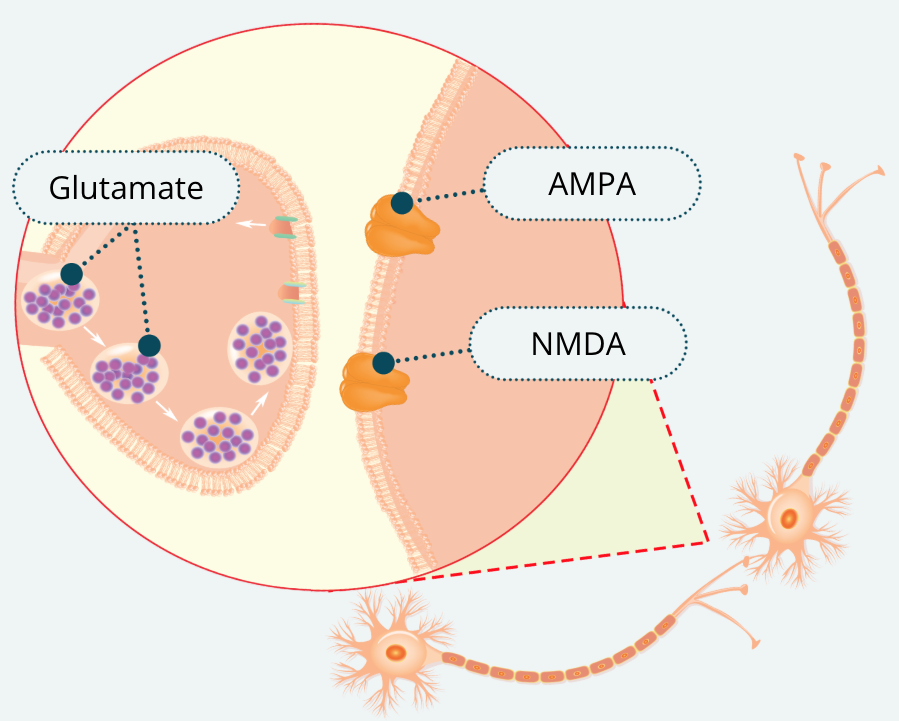
There are probably several different ways that LTP can happen at the synapse, and it is probably different depending on where in the brain you look. However, there are some basic changes that occur to strengthen the connection between two neurons. There are two basic phases during which this occurs. In most cases, the neurotransmitter involved in LTP, and therefore thought to be very important for learning and memory, is glutamate. Glutamate binds to several types of receptors on the postsynaptic neuron. Two important ones for LTP are NMDA and AMPA. NMDA stands for N-methyl-daspartate and AMPA stands for alpha-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid. Aren’t you happy that we just call them NMDA and AMPA and that you won’t have to remember their full names?
Phase I
NMDA receptors unblock Mg+
Ca2+ flows in and binds to CaMKII
These two glutamate receptors are similar in that when glutamate binds to them, a channel opens that allows Na+ ions and K+ ions to flow across the cell membrane, depolarizing the neuron. They differ in that the central channel in NMDA receptors is initially blocked by a magnesium ion. Thus, during phase I of LTP when the presynaptic neuron releases glutamate, it binds to both receptors but only the AMPA receptors allow ions to pass. During LTP, activation of the AMPA receptors in the first few electrical pulses slightly depolarizes the membrane because of the Na+ flow through the AMPA channels. The magnesium ion only stays lodged in the channel of the NMDA receptor when the membrane is fully polarized. As it becomes slightly depolarized, the magnesium ion is eventually dislodged and now NMDA receptors are unclogged.
There is another important difference between AMPA and NMDA receptors, the NMDA receptor also allows calcium ions through its channel. Once the channel is unblocked, sodium, potassium, and calcium flow across the membrane. Not only does this depolarize the neuron more, but calcium also acts on a second messenger called CaMKII (pronounced: Cam Kinase Two) that starts off a cascade of events in the postsynaptic neuron leading to LTP.
Phase II
AMPA receptors increase
Increase in postsynaptic surface area
Release of nitric oxide signals more glutamate release
The specific interactions of CaMKII in LTP is too advanced for this course, and quite frankly, we haven’t figured out all the steps yet. Nonetheless, as a consequence of this signaling cascade three important changes happen at the synapse during phase II of LTP. First, the postsynaptic neuron increases the number of AMPA receptors in its membrane at the synapse. This way, when glutamate is released from the presynaptic neuron, the postsynaptic neuron is depolarized even more because more sodium ions can now flow through the more abundant AMPA receptors.
Another thing that occurs during phase II of LTP is that the postsynaptic neuron actually grows more surface area to increase the physical size of the synapse. Think about that, when you are learning something new, your brain is actually growing in a way. It isn’t technically growing - your brain doesn’t get bigger overall - it is just redistributing the area dedicated to a particular neural connection. Keep in mind that other connections are being reduced at the same time – like the example of Pavlov’s dogs in the last lesson.
A third change that occurs during phase II of LTP, is that the postsynaptic neuron signals the presynaptic neuron by releasing nitric oxide gas, which can diffuse across the cell membrane. This gas signals the presynaptic neuron to release more glutamate.
So now we have a larger synapse, with more glutamate being released, and more AMPA receptors to open and let sodium flow in. You can understand how these changes would strengthen the synapse. After LTP, the presynaptic neuron will cause a greater depolarization in the postsynaptic neuron and the postsynaptic neuron will more likely have an action potential. In another word, “Neurons that fire together, wire together.” So, there you have it, your memory of mom’s homemade apple pie is a result of calcium ions signaling CaMKII and making your brain rearrange its synaptic connections.
Bringing it All Together
So now we have a larger synapse, with more glutamate being released, and more AMPA receptors to open and let sodium flow in. You can understand how these changes would strengthen the synapse. After LTP, the presynaptic neuron will cause a greater depolarization in the postsynaptic neuron and the postsynaptic neuron will more likely have an action potential. In another word, “Neurons that fire together, wire together.” So, there you have it, your memory of mom’s homemade apple pie is a result of calcium ions signaling CaMKII and making your brain rearrange its synaptic connections.
Memory Disorders
Memory Decline with Age
The ability to form memories is a wonderful and complex feature of our brain and like anything complex, it can go wrong. Until recently, it was thought that memory impairments during old age were inevitable. We now realize that we can have some control over maintaining our memory as we age, and memory decline isn’t automatic. For example, university professors in their 60’s typically perform as well as their colleagues in their 30’s on learning and memory tasks.
Maintaining Healthy Learning and Memory
Cardiovascular health
Sleep
Challenging the brain
There are a number of factors that contribute to maintaining healthy learning and memory as we age. Obviously, health is important, especially cardiovascular health, our brain will always need that constant flow of oxygen and energy is gets from the circulatory system. Exercise is also thought to be important for maintaining good cognitive health as we age. At any age, we all need a good night’s rest for our memory to function best. In fact, it appears that sleep is critical for the consolidation of some memories. One other factor that may seem surprising is that our brain works much like our muscles, in the sense of “use it or lose it.” Studies suggest that the more we challenge our brain during our lifetime the better our learning and memory will be as we age. For example, people working in an assembly line job for most of their lives that requires little mental effort and who do not challenge their brains in other ways will on average see an earlier cognitive decline compared to those who spend their whole lives and even retirement learning new things. By learning new things, I don’t simply mean reading books, although that too is really helpful. But this could be anything from taking university courses in your 20’s to learning a second language or learning how to play a musical instrument after you retire. We must always keep our brain active and challenged if we want to keep it sharp as we age.
Alzheimer’s Disease
Overview
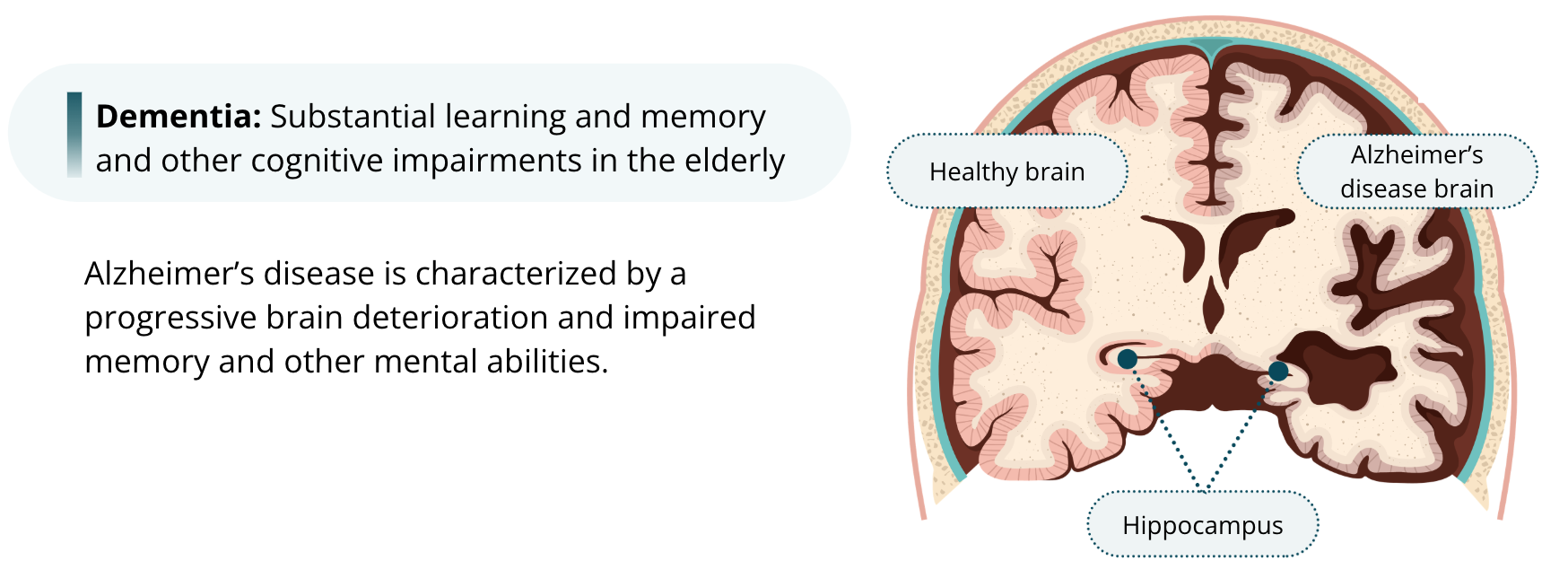
When there are substantial learning and memory and other cognitive impairments in the elderly, it is called dementia. The most common form of dementia, typically but not necessarily, in the elderly, is called Alzheimer’s disease. Alzheimer’s disease is characterized by a progressive brain deterioration and impaired memory and other mental abilities. You learned that a stroke can impair memory by damaging neurons within the hippocampus. Alzheimer’s is thought to impair memory by also damaging the hippocampus.
Early Stage
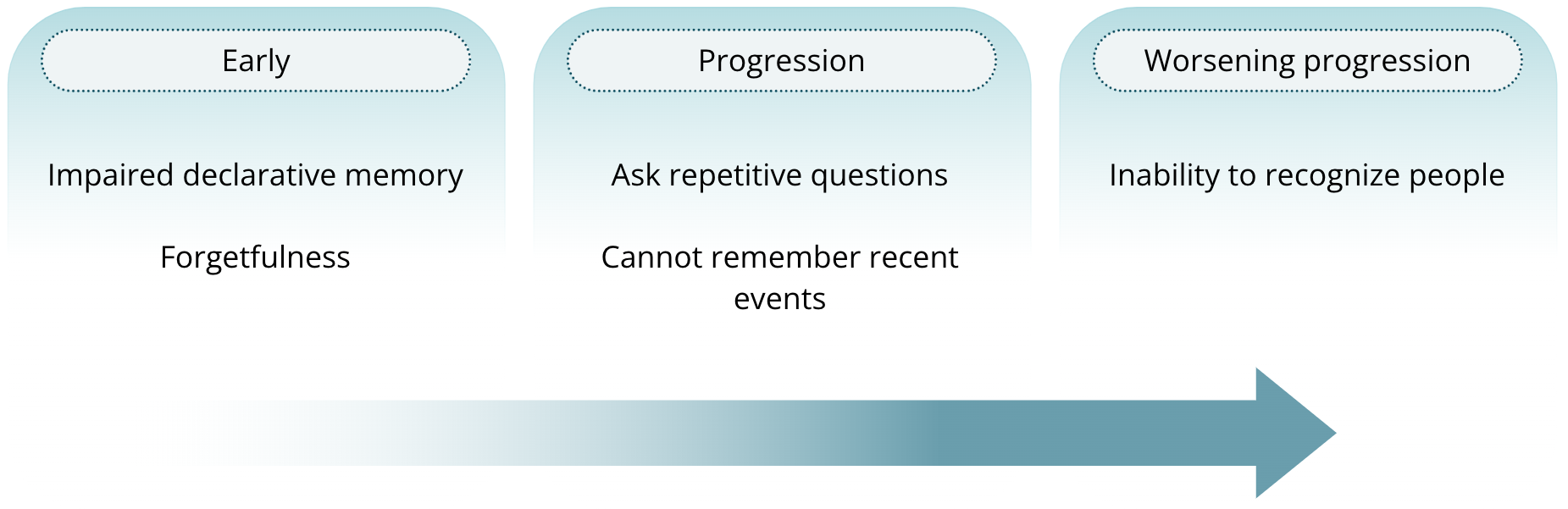
Early in the course of the disease it is characterized by impaired declarative memory. Very early in the disease the person simply starts to forget things that most of us can forget, like where they put their keys or a fact in a story that somebody told them. As the disease progresses the person may start repeating questions they have already asked in a conversation or have trouble remembering events from the day before. As the disease worsens, they eventually have trouble recognizing people they know, even family members
Late Stage
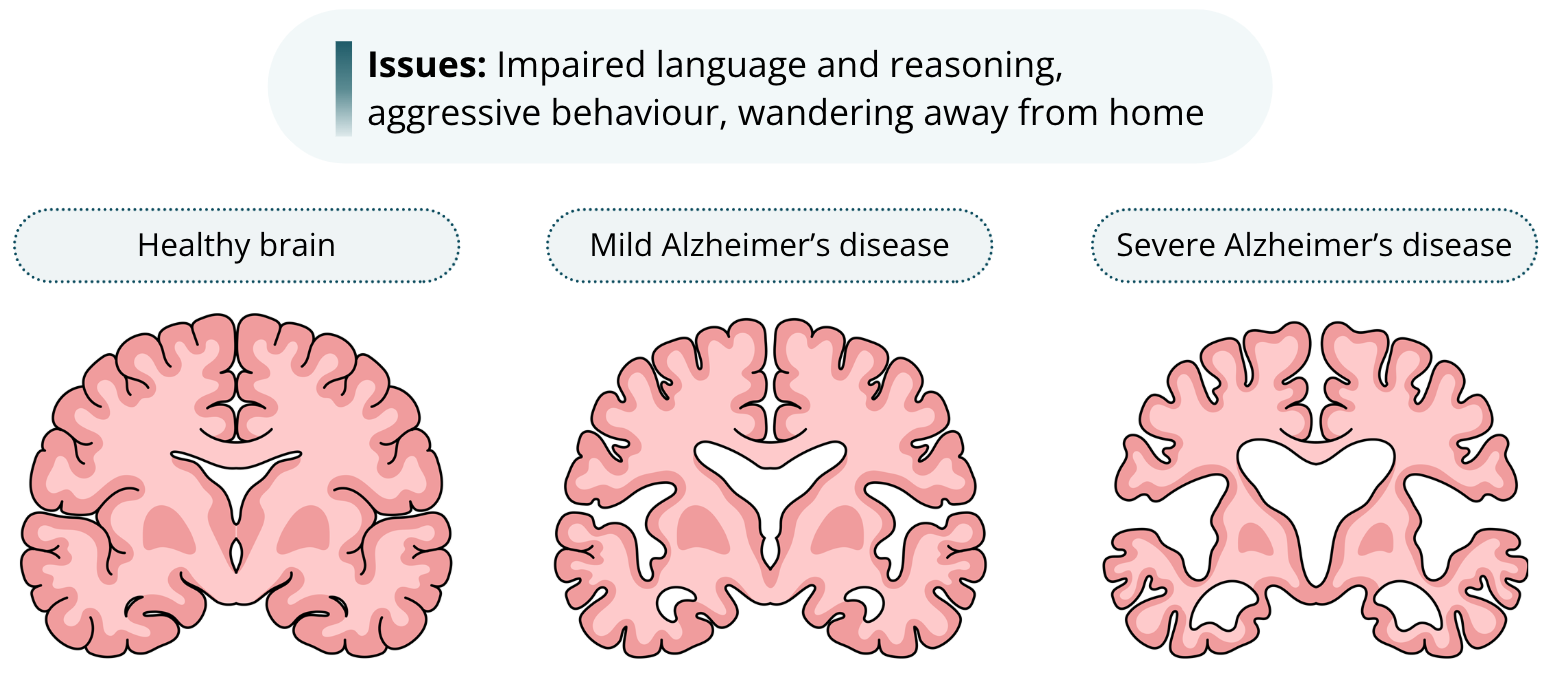
Because Alzheimer’s disease eventually affects the entire brain - it tends to only affect the hippocampus in early stages - eventually other behaviours become impaired like language and reasoning. Other behavioural problems may occur such as aggressive behaviour or wandering away from home. Alzheimer’s disease is fatal, and it is the 6th leading cause of death in the US.
Brain Pathology
Beta amyloids
Neurofibrillary tangles
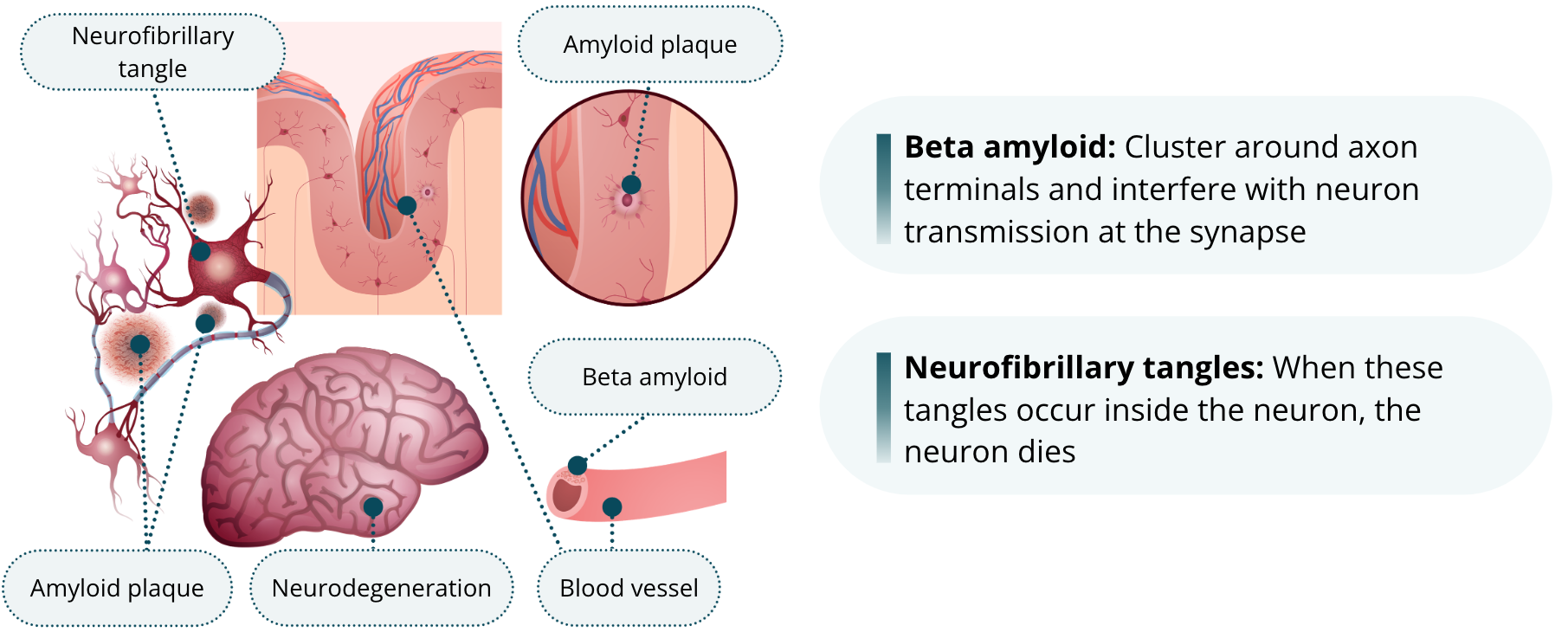
It has been known for some time that, upon post-mortem examination under a microscope, the brains of Alzheimer’s patients have distinct looking clumps called amyloid plaques. Plaques are aggregates of a ‘sticky’ protein called beta amyloid. Beta amyloid will cluster around axon terminals and interfere with neuron transmission at the synapse. In addition, another protein called tau will form neurofibrillary tangles within neurons. When these tangles occur inside the neuron, the neuron dies. Thus, there are two things possibly impairing normal brain function in Alzheimer’s disease.
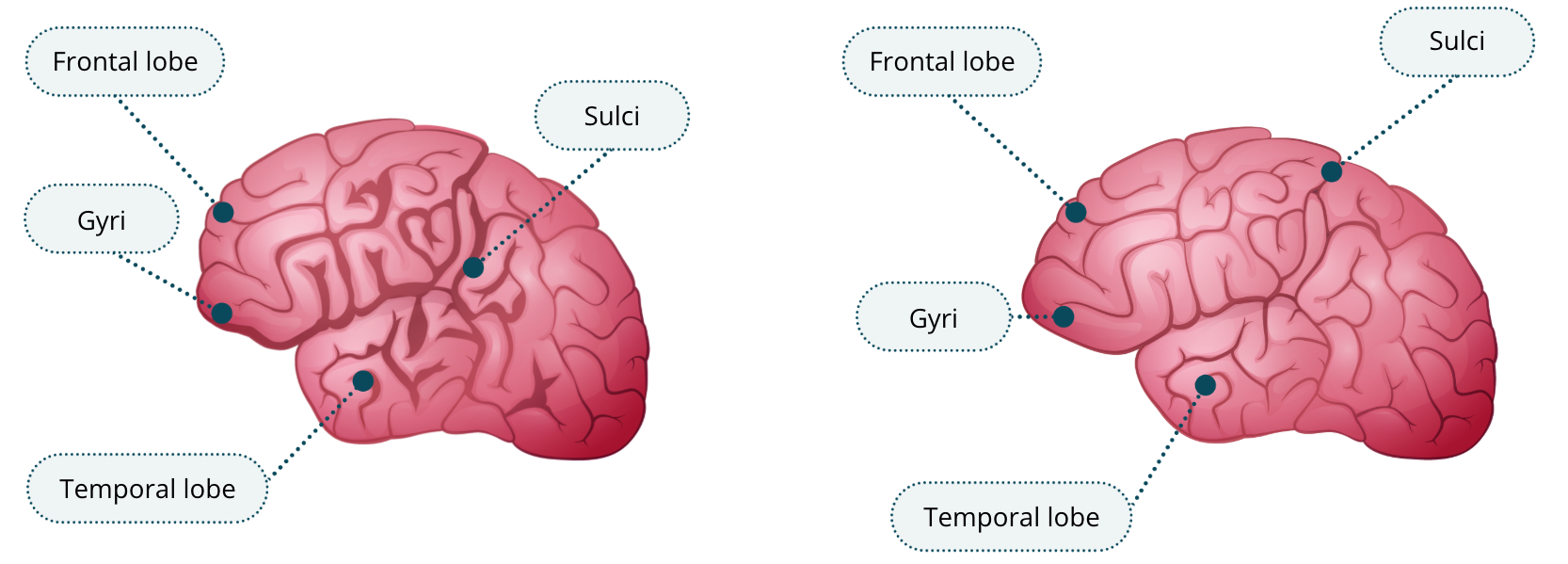
As you can see in this image of a brain of a late-stage Alzheimer’s patient and a healthy brain, neuron loss is evident by the fact that the gyri are reduced in size and the sulci are increased compared to the healthy brain. The temporal lobe is particularly affected, which accounts for the severe memory impairments observed in the disease. Yet, other lobes including the frontal lobes are also affected accounting for the other behavioural effects that occur as the disease progresses.
Probability
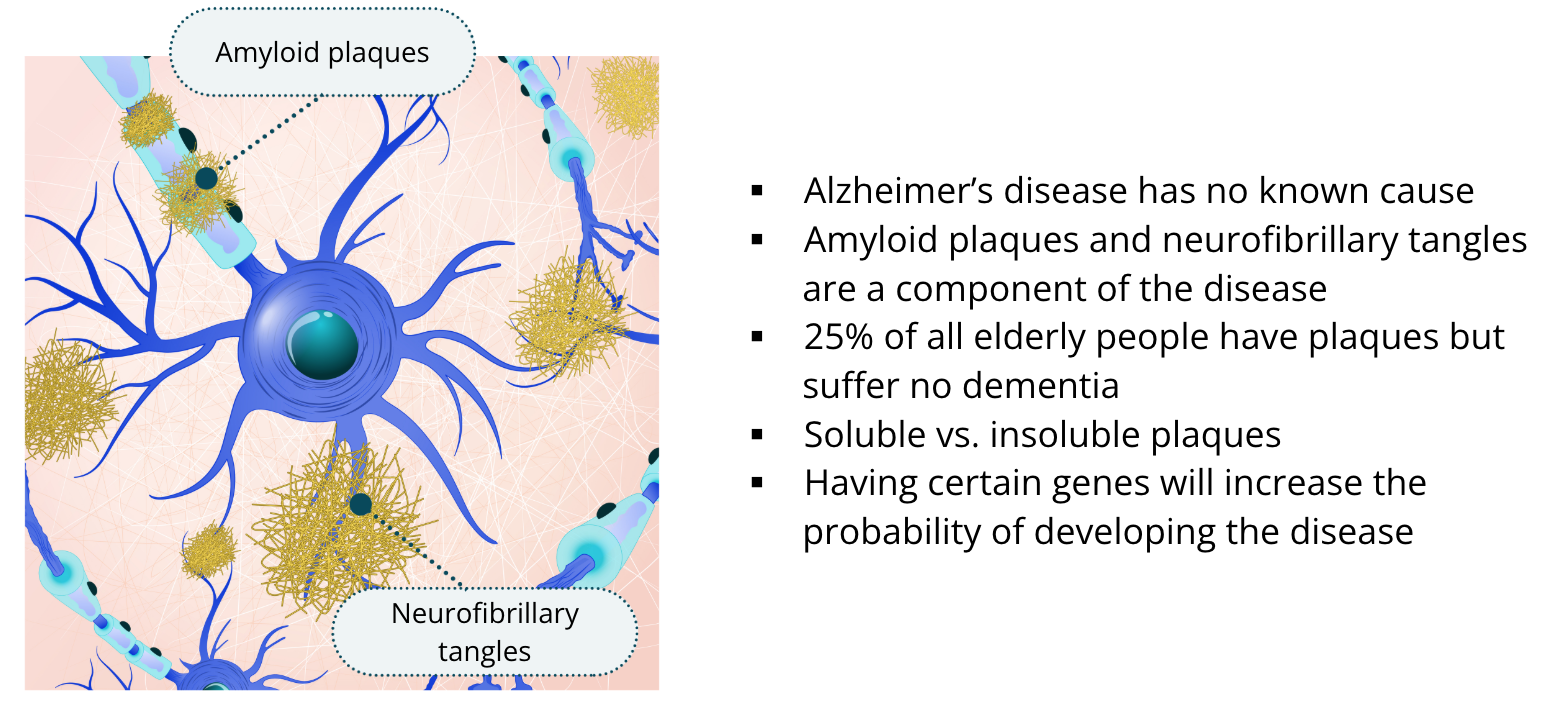
It is important to note that we still do not understand exactly what causes Alzheimer’s disease. Although amyloid plaques and neurofibrillary tangles are clearly a component of the disease, the number of plaques in the brain does not always correlate with cognitive impairments. Also, about 25% of all elderly people have plaques but suffer no dementia. So, the presence of plaques isn’t the whole story. We now know that there are differences in amyloid plaques such that some are categorized as soluble and some are categorized insoluble plaques, these differences in the type of plaque probably accounts for whether the presence of plaques will lead to Alzheimer’s disease. We also know now that having certain genes will also increase the probability of developing the disease. But we are still far from figuring it all out.
Treatment
There is no known cure for Alzheimer’s disease and the current treatments aren’t very good. A major neurotransmitter in the hippocampus that is known to regulate memory – other than glutamate – is acetylcholine. This is the same neurotransmitter that you have learned regulates muscle movement in the peripheral nervous system at the neuromuscular junction. Within the central nervous system, it is shown to be important for memory formation in the hippocampus. It is the neurons that release acetylcholine that to die off early in Alzheimer’s disease.
Drugs that are commonly used to treat Alzheimer’s are called cholinesterase inhibitors. Cholinesterase is an enzyme that breaks down the neurotransmitter acetylcholine in the synapse. By inhibiting this enzyme, these drugs prolong the time acetylcholine is active in the synapse thereby increasing its neurotransmission and compensating for those other acetylcholine neurons that have died. Unfortunately, this treatment only buys the Alzheimer’s patient a month or two of improved memory.
The Reserve Hypothesis
There is some hopeful news in all of this. There is some evidence for compensation in the elderly who spend their lives learning new things. Studies show that people who spend their lives learning and regularly challenging their brain in new ways have half the chance of developing Alzheimer’s disease compared to people who don’t. This led to a controversial idea called the reserve hypothesis. The reserve hypothesis posits that people with higher brain capacity can compensate for brain changes that may occur from normal aging, brain damage, or even Alzheimer’s disease.
Your Brain: Use it or Lose it!
One way to think of this is to imagine a lifelong athlete who develops a physical injury, they are much more likely to recover successfully from the injury than a sedentary, unathletic person. Equally, a lifetime of learning new things, developing new skills, and regularly challenging your brain appears to be protective against disorders that may impair your ability to learn and remember later in life or in response to disease