Patterns of inheritance
Gregor Mendel’s experiments on pea plants in the 1860s: laws of meiosis without knowledge of chromosomes.
Locus: a unique chromosomal location of a gene or DNA sequence.
Alleles: alternative versions of a gene.
Genotype: alleles present at one or more loci.
Phenotypes, characters, traits: observable properties of an organism.
DEFINITIONS TO REMEMBER:
Monogenic versus multifactorial inheritance:
What is the difference between oligogenic and polygenic inheritance?
Polygenic inheritance
Many genes are involved (often dozens to hundreds).
🔹 Oligogenic inheritance
Few genes are involved (usually 2–5).
Great question — this slide is contrasting monogenic vs polygenic traits and introducing the idea of dichotomous vs continuous traits. Let’s break it down clearly.
🔹 What does dichotomous mean?
Dichotomous = two mutually exclusive categories.
There are only two possible outcomes, and you’re either in one or the other.
Think:
Yes / No
Affected / Not affected
Present / Absent
There is no in-between.
Examples of dichotomous traits:
Huntington's disease (you either have it or you don’t)
Cleft palate (present or absent)
Blood type A vs not A
🔹 Mendelian (Monogenic) Traits = Usually Dichotomous
Monogenic traits are caused by one gene with a strong effect.
Because one gene determines the outcome, the trait often looks:
Clear-cut
Binary
Either present or absent
That’s why the slide says:
Mendelian traits: dichotomous (mutually exclusive)
🔹 Polygenic Traits = Usually Continuous
Polygenic traits involve many genes, each contributing a small effect.
Instead of two categories, you get a range.
Continuous traits (quantitative traits):
Height
Weight
Blood pressure
Intelligence
You don’t fall into just two groups — you fall somewhere along a spectrum.
These are influenced by:
Many small-effect genes
Called Quantitative Trait Loci (QTLs)
🔹 But Some Polygenic Traits Are Still Dichotomous
This is an important point.
Some diseases (like type 2 diabetes) are:
Influenced by many genes
BUT still diagnosed as yes/no
You either:
Have diabetes
Or don’t
However, genetically, it’s not caused by one gene — it’s due to many susceptibility genes that increase your risk, not guarantee disease.
So genetically → continuous risk
Clinically → dichotomous outcome
This is called a threshold trait.
🔹 Complex Traits
Some conditions (like diabetes) can:
Be monogenic (rare cases)
Be polygenic (most cases)
Be strongly environmentally friendly
Or a combination
These are called complex traits because:
Multiple genes
Environmental factors
Lifestyle
all interact.
🔎 Simple Summary
Term | Meaning |
|---|---|
Dichotomous | Two possible categories (yes/no) |
Continuous | A spectrum of values |
Monogenic | One gene causes a trait |
Polygenic | Many genes influence the trait |
Susceptibility genes | Genes that increase risk but don’t guarantee disease |
Complex trait | Multiple genes + environment |
🧠 Big Idea
Monogenic → usually dichotomous
Polygenic → usually continuous
Some polygenic traits are dichotomous in diagnosis but continuous in genetic risk.
DEFINITIONS TO REMEMBER:
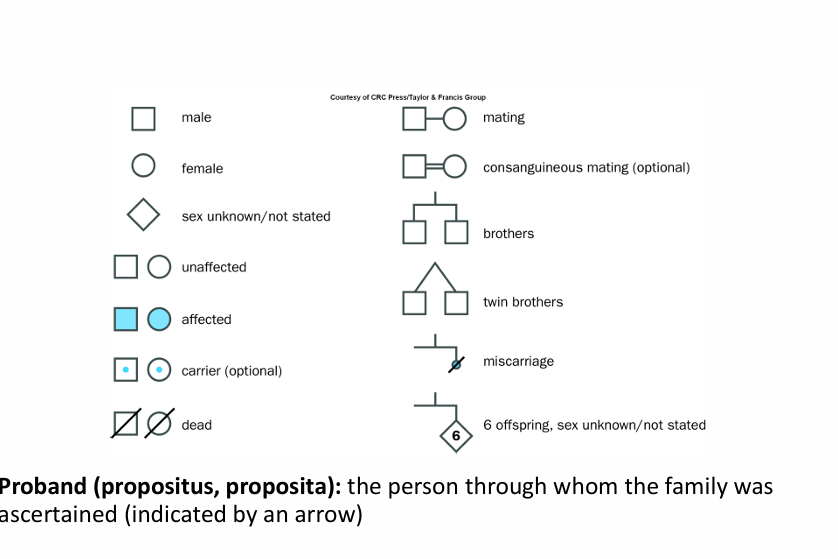
WHAT IS A PROBAND?
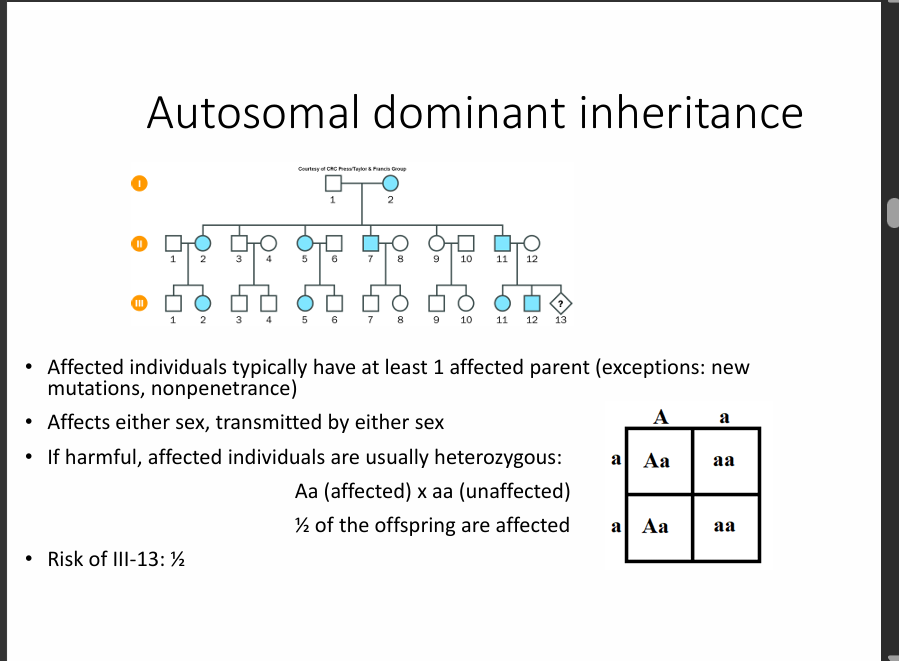
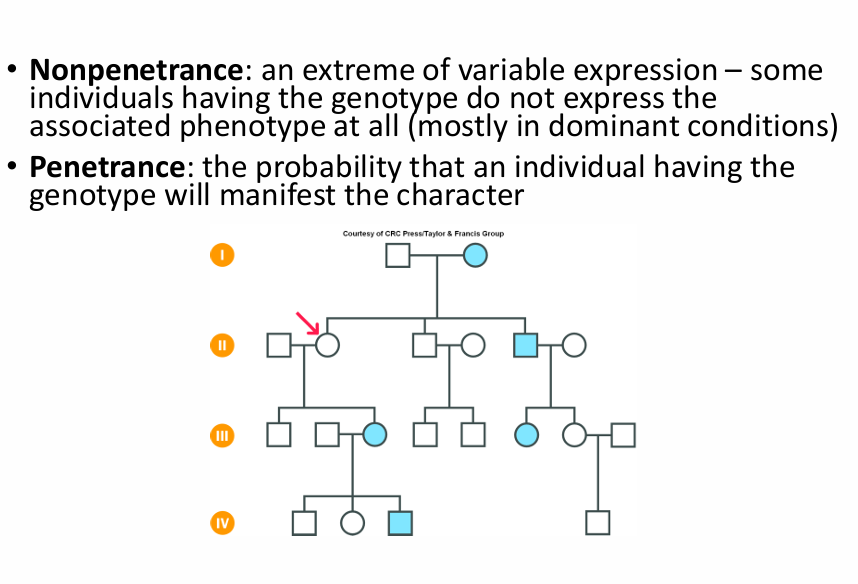
How do you know it is Autosomal dominant inheritance?
Autosomal because both sexes are affected equally.
Dominant because there is an affected individual in every generation.
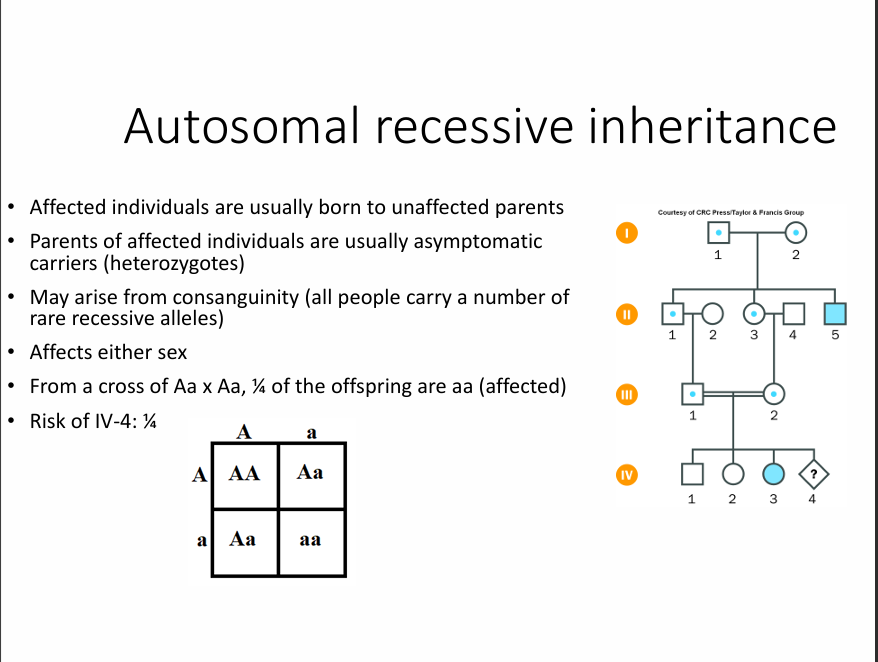
How to know it is autosomal recessive inheritance:
Autosomal because both sexes are affected equally.
Recessive because not every generation has an affected individual in every generation.
Key notes:
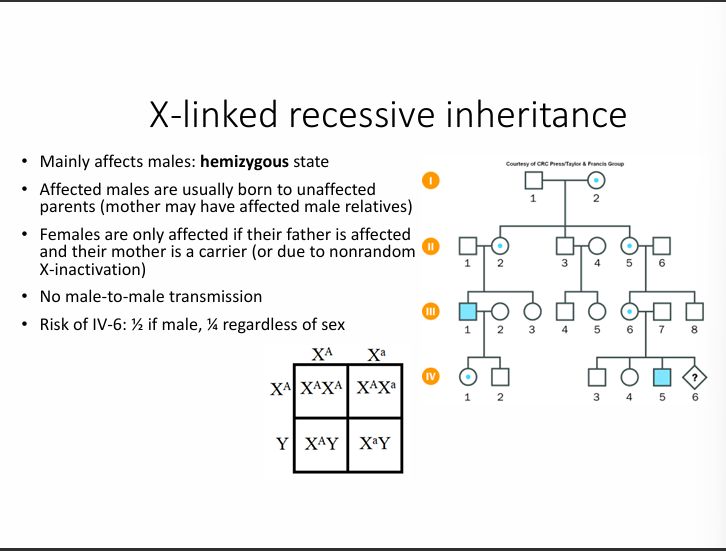
It mainly affects males: a hemizygous state.
Affected males are usually born to unaffected parents because the parents are heterozygous.
Females are only affected if their father is affected and their mother is a carrier.
No male-to-male transmission
The males get their X chromosome from the mothers and the Y chromosome from the fathers.
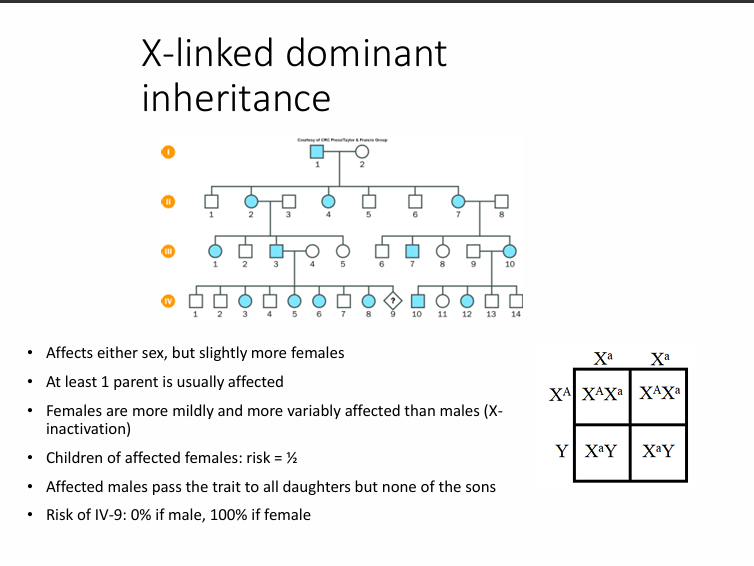
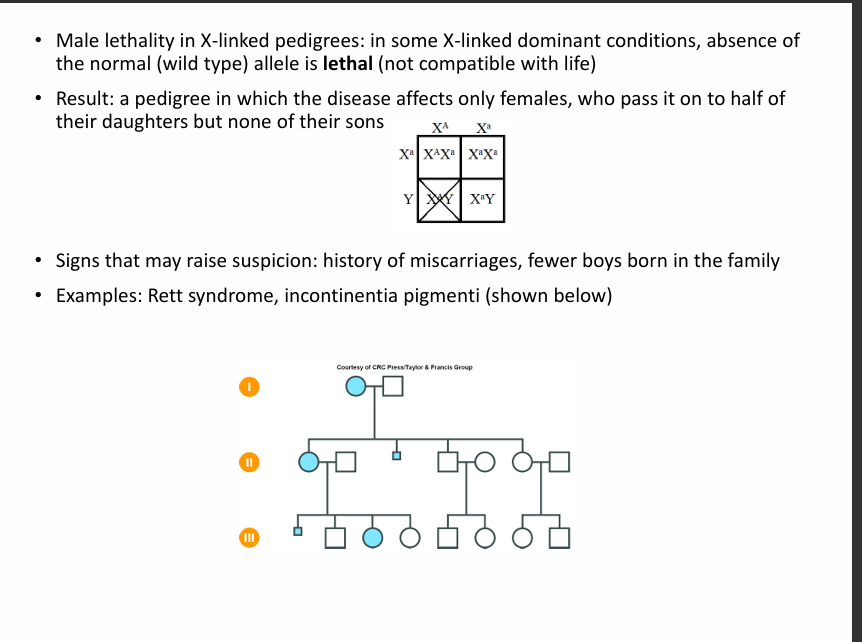
Affects either sex, but slightly more females.
At least 1 parent is usually affected.
Females are more mildly and more variably affected than males.
Children of affected females.
Affected males pass the traits to all daughters but none of the sons.
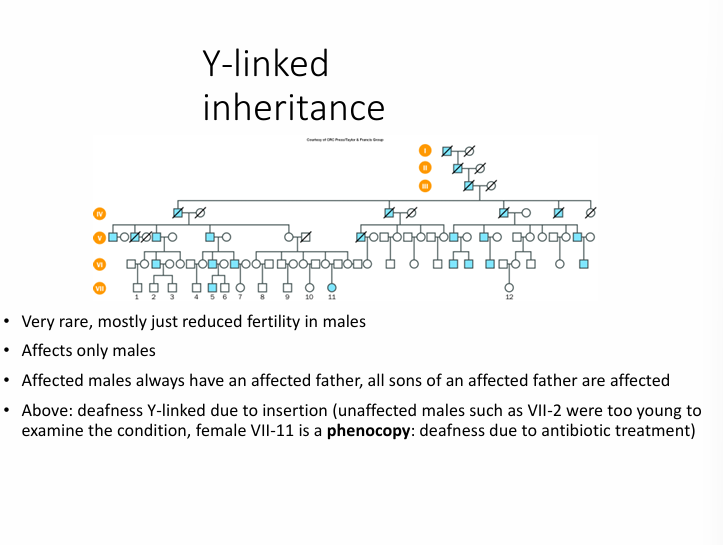
This is very rare
Affects only males.
Affected males always have an affected father; all sons of an affected father are affected.
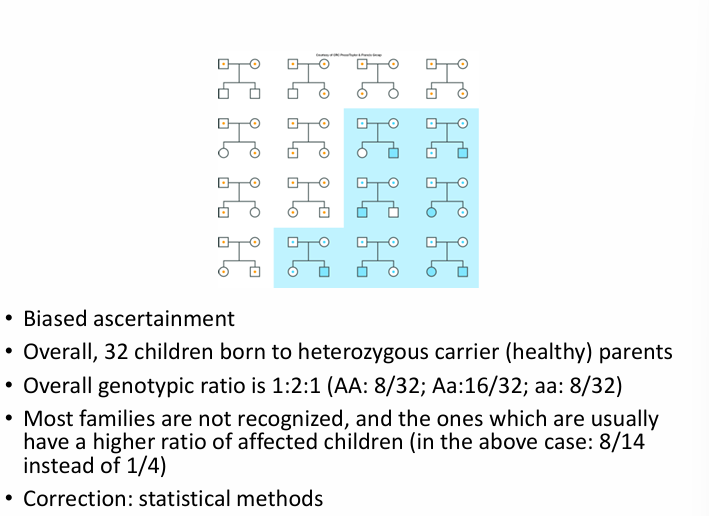
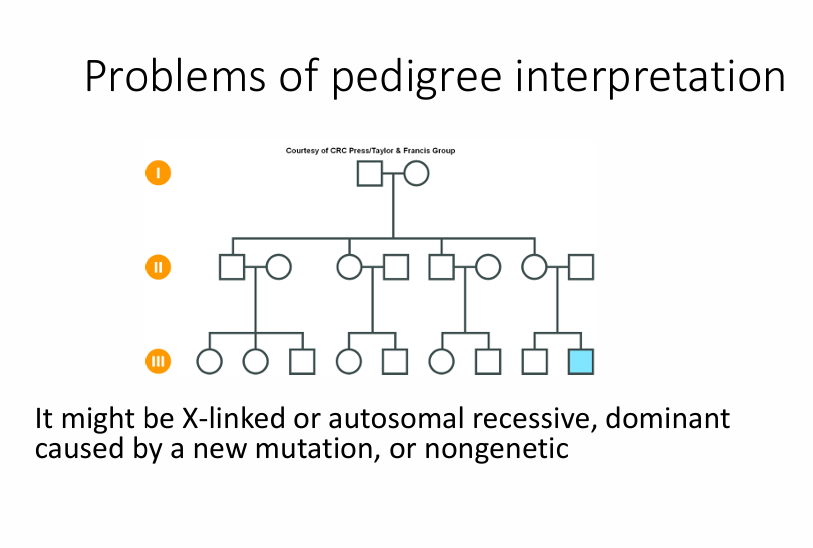
🔎 1. Why identifying inheritance can be tricky
“Human families are often too small…”
Unlike pea plants (Mendel), human families:
Have a few children
Don’t produce clear ratios (like 3:1)
Also, we often study families because someone is affected, which creates ascertainment bias (we’re not sampling randomly).
So patterns are sometimes harder to see.
🔹 2. Dominant diseases: why are most affected people heterozygous?
In autosomal dominant diseases:
One mutant allele is enough to cause disease.
Most affected individuals are heterozygous (Aa).
Why not homozygous (AA)?
Because:
A homozygous dominant is often very severe or lethal.
Or extremely rare.
📌 Example: Huntington'sis disease
In Huntington's disease:
Homozygotes and heterozygotes look very similar clinically.
So it behaves as a classic dominant disorder.
🔹 3. Achondroplasia example
Achondroplasia (short-limbed dwarfism):
Heterozygous (Aa) → short stature
Homozygous (AA) → usually lethal shortly after birth
This shows:
The condition is dominant
But the homozygous state is much more severe
This helps explain the next concepts.
🔹 4. Incomplete dominance (semi-dominance)
Definition:
The heterozygote has a phenotype between the two homozygotes.
Example pattern:
Genotype | Phenotype |
|---|---|
AA | Severe |
Aa | Moderate |
aa | Normal |
So the heterozygote is intermediate.
Achondroplasia shows this at the biological level:
aa = normal
Aa = dwarfism
AA = lethal (more severe)
🔹 5. Codominance
Definition:
Both alleles are expressed independently.
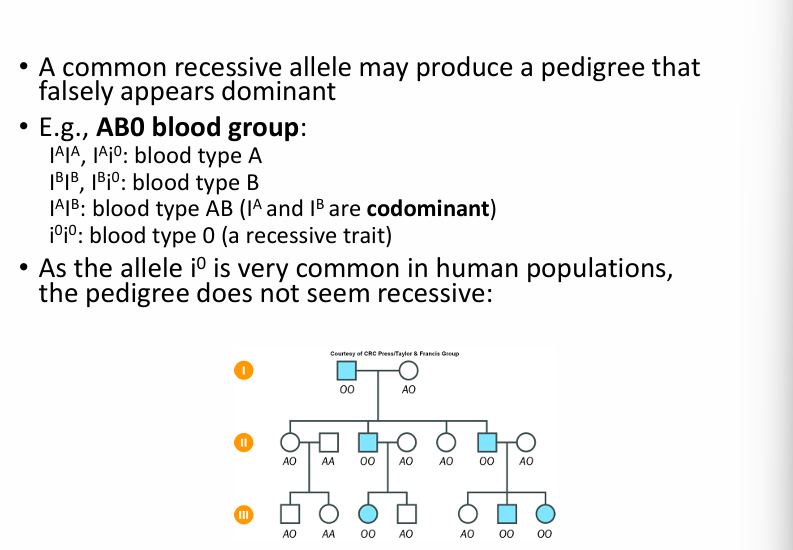
Classic example:
ABO blood group
IA and IB are both expressed
Here:
No blending
Both products are visible
🔹 6. Why is achondroplasia still called dominant
Even though:
Homozygotes are more severe (lethal)
Clinically:
If you have one mutant allele, you have the disease.
So in practice:
It is labelled autosomal dominant.
🧠 Big Concepts From This Slide
Dominant diseases usually involve heterozygotes
A homozygous dominant may be rare or lethal
Incomplete dominance = intermediate phenotype
Codominance = both alleles expressed
Real human genetics is often more complex than simple Mendelian patterns
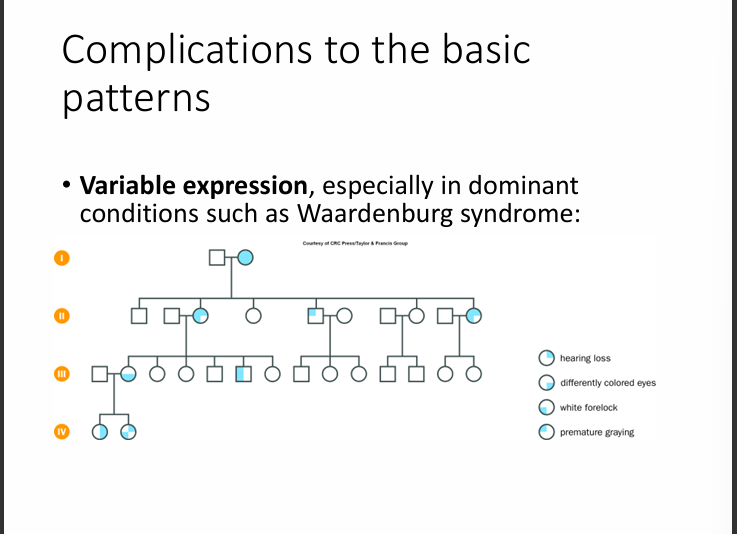
Waardenburg Syndrome
Waardenburg syndrome (WS) is a genetic condition that mainly affects:
👂 Hearing
🎨 Pigmentation (eyes, hair, skin)
It is most commonly autosomal dominant, though some rare types can be autosomal recessive.
🧬What is Variable Expression?
Variable expressivity means:
People with the same genetic condition can show different degrees or types of symptoms.
They all have the mutation.
They all technically “have” the disease.
But the severity and features vary.
Anticipation
This is the tendency of a disease to become more severe and/ or have an earlier onset in successive generations.
True anticipation: characteristic of dynamic mutations.
False impression of anticipation: due to a systematic bias of ascertainment in the dominant conditions showing variable expression (parents only turn to genetic counselling when their child is more severely affected than they are, while severely affected individuals may not have children at all.
Solutions: statistical methods or direct molecular evidence.
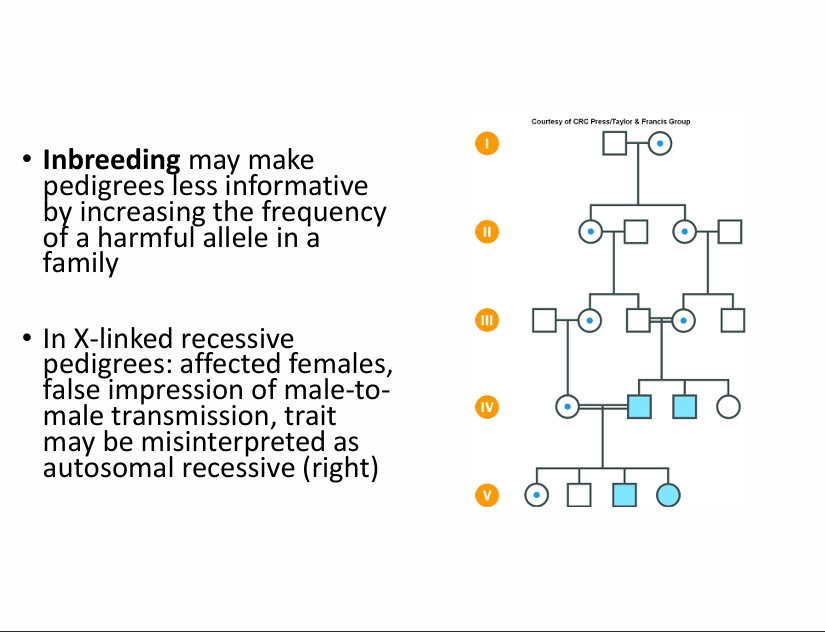
“Inbreeding may make pedigrees less informative”
What is inbreeding?
Mating between relatives (e.g., cousins).
Relatives share genes from common ancestors.
So if there is a harmful recessive allele in the family:
It becomes more common
The chance of two carriers mating increases
More affected children appear
This can make the pattern look misleading.
🔹Why this matters in X-linked recessive disorders
Normally, in X-linked recessive:
Mostly males affected
No male-to-male transmission
Females are usually carriers
But with inbreeding:
🔸 A female can become affected
How?
If:
Her father is affected (XᵃY)
Her mother is a carrier (XᵃX)
She can inherit:
Xᵃ from dad
Xᵃ from mom
→ XᵃXᵃ = affected female
This is rare in the general population, but more likely with consanguinity.
🔹 False impression of male-to-male transmission
Normally:
X-linked recessive has NO father → son transmission
But in consanguinity:
You might see:
An affected male
His male cousin was also affected
This can look like father → son transmission
But actually:
The mutation is coming through carrier females
The males just share the same inherited mutation from a common ancestor
So it can look autosomal recessive, even though it’s X-linked.
🔹Why it may be misinterpreted as autosomal recessive
Autosomal recessive traits:
Affects males and females equally
Often appear in consanguineous families
If you see:
Affected males
Affected females
Related parents
You might think: autosomal recessive.
But it could actually be:
X-linked recessive + consanguinity
🧠 Big Takeaway
Inbreeding increases the chance that:
Rare harmful alleles meet
Females become affected in X-linked disorders
Pedigrees look “non-classical”
So inheritance patterns may be misleading.
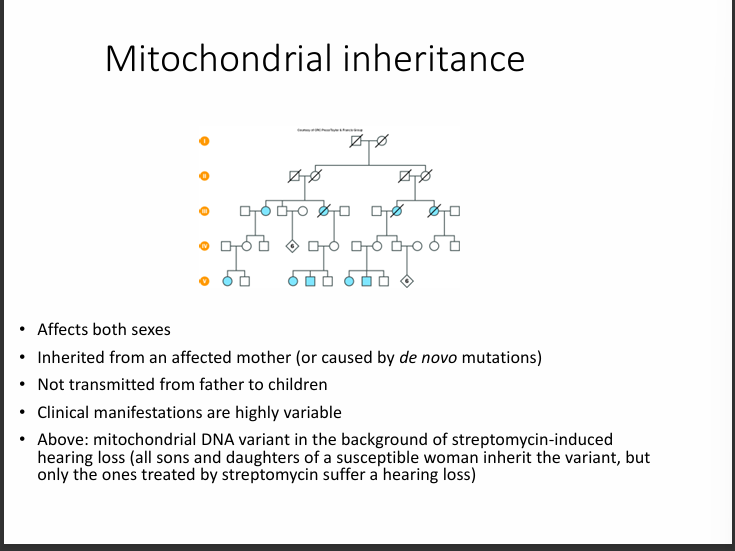
PATTERNS OF INHERITANCE II. MOSAICISM, NEW MUTATIONS, NON-MENDELIAN CHARACTERS:
Classification of genetic changes:
Constitutional: these genetic changes are present in all cells of the body. It originates from a germ-line mutation.
Mosaic: present only in a particular cell line due to an event at some point during development; may be somatic, gondal or germinal or gonosomal (i.e. involving both somatic and germline cells.
MOSAICISM
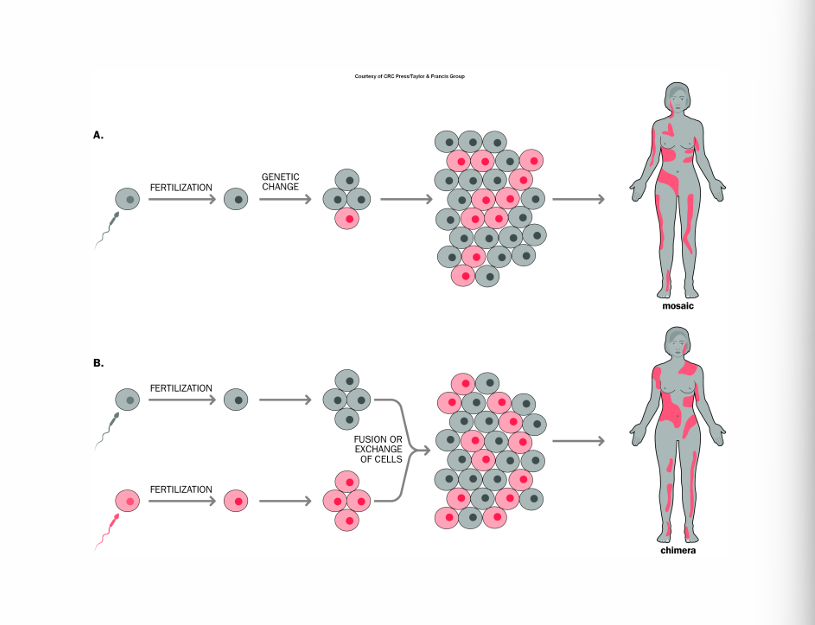
🧬 What is Mosaicism?
Mosaicism = one person has two (or more) genetically different cell populations.
This happens when:
A mutation occurs after fertilisation (not in the egg or sperm),
During early cell divisions of the embryo.
So some cells carry the mutation, and others don’t.
🔹 “The number and type of affected cells depend on timing”
The earlier the mutation happens:
More cells will carry it
A larger part of the body is affected
The later it happens:
Fewer cells affected
Maybe only one tissue is
involved
Example:
Mutation at 2-cell stage → ~50% of body cells affected
Mutation later → maybe only skin cells affected
So timing determines:
How many cells are mutant
Which tissues are involved
🔹 “Lethal conditions may be compatible with life in mosaic form”
Some mutations are so severe that:
If every cell had it → the embryo would die
But if only some cells have it:
The normal cells compensate
The person survives
So mosaicism can “soften” a lethal mutation.
🔹 Revertant Mosaicism (Back-mutation)
This is fascinating.
If someone has a mutation in all cells (constitutional mutation):
Sometimes:
A cell randomly “corrects” the mutation
That corrected cell divides
It may grow better than the defective cells
So you get patches of normal tissue inside abnormal tissue.
Example:
Some genetic skin disorders show normal skin patches due to revertant mosaicism.
It’s like the body partially fixes itself.
🔹 Diffusible vs Cell-Autonomous Effects
This is about how the gene product works.
🟢 Diffusible gene product
The protein:
Can move between cells
Can help neighbouring cells
Example:
Hormones
Some enzymes
If only some cells produce it, nearby cells might still benefit.
→ The mosaicism effect is milder.
🔵 Cell-autonomous gene product
The protein:
Only works inside the cell, which makes it
Cannot help neighbouring cells
If a cell has the mutation:
That cell alone is affected
No rescue from nearby normal cells
→ The mosaicism effect is more visible.
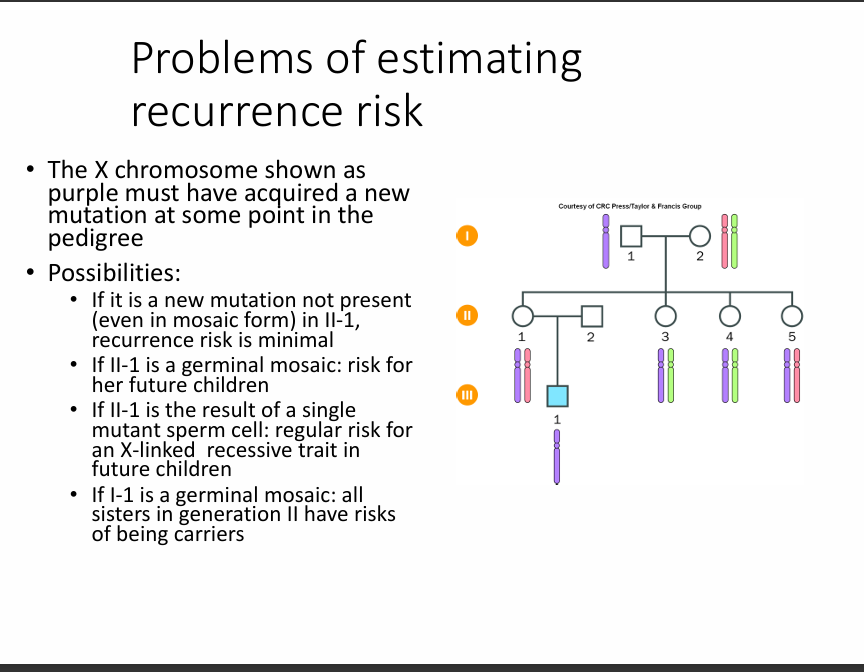
This slide is about new (de novo) mutations and how they affect inheritance patterns.
Let’s go through it clearly and logically.
🧬 “A normal parent produced a single mutant gamete… or was mosaic”
When a child has a genetic disease, but:
Both parents are clinically normal
No family history
We often assume:
A new mutation occurred in one sperm or egg.
That’s called a de novo mutation.
BUT — sometimes:
The parent may actually have germline mosaicism.
Meaning:
Some of their egg/sperm cells carry the mutation
Their body cells don’t
They appear completely normal
This explains:
More than one affected child
Despite normal parents
So it wasn’t just “one random sperm” — it may have been mosaic in the parent.
🧬 Natural selection removes severe dominant and X-linked mutations
If a mutation is:
Very harmful
Reduces survival or reproduction
Then affected individuals:
Often don’t reproduce
Don’t pass it on
So the mutation disappears from the population.
But we still see these diseases.
Why?
Because:
New mutations keep happening.
This is calledthe mutation–selectionn balance.
🧬 3⃣ Lethal dominant conditions arise from new mutations
If a dominant mutation is:
Lethal before reproduction
Then:
The affected person cannot pass it on
It must arise as a new mutation each time
Example concept:
Some severe skeletal dysplasias
So:
No inheritance across generations
Only fresh mutations
🧬 X-linked recessive and selection
In severe X-linked recessive diseases:
Affected males often have reduced reproduction
So they don’t pass the mutation on
This means:
Many cases arise from new mutations
Especially in severe conditions
🧠 Big Concepts Behind This Slide
🔹 De novo mutation
A mutation that appears for the first time in a child.
🔹 Germline mosaicismThe parentt is normal but has some mutated reproductive cells.
🔹 Mutation–selection balance
Bad mutations are removed by selection,
But new ones constantly appear.
🔹 Lethal dominant disorders
Usually, only seen as new mutations.
✨ Simple Summary
Situation | What Happens |
|---|---|
Severe dominant mutation | Often new mutation |
Severe X-linked recessive | Often new mutation |
Parent normal, child affected | Could be de novo or germline mosaicism |
Why diseasepersists? | New mutations replace lost ones |
🔎 The Core Message
Even if a disease is genetic:
It doesn’t always come from a family history.
Many severe disorders exist because new mutations keep arising.
🧬 Germline (Germinal) Mosaicism
Definition:
A person has a mutation in some of their sperm or egg cells, but not in their body (somatic) cells.
So:
The parent is healthy.
Blood test = normal.
But they can still have affected children.
Why does the slide say:
“Proportion of mutant sperm cells produced by a normal father (not possible to detect in mother)”
For fathers:
You can directly test sperm.
You might estimate what fraction carries the mutation.
For mothers:
You cannot test egg cells easily.
So maternal germline mosaicism is very hard to detect directly.
That’s why it says “not possible to detect in mother.”
🧬 Testing Different Cell Types
If a blood test is negative, that does NOT rule out mosaicism.
Why?
Because:
The mutation might not be in the blood.
It might only be in:
Skin
Brain
Gonads
A small subset of cells
So sometimes doctors test:
Blood
Skin biopsy
Tumour tissue (in cancer)
Different tissues may show different results.
🧬 Detecting Small Amounts of Mutant DNA
This is a technical problem.
Imagine:
95% normal cells
5% mutant cells
When you test DNA:
The normal DNA overwhelms the mutant DNA.
The mutation signal may be very weak.
So detection depends on:
Sensitivity of the method
Depth of sequencing
This is especially important in:
Cancer tumour cells mixed with normal cells)
Low-level mosaicism
🧠 Big Challenges in Detecting Mosaicism
Problem | Why It’s Hard | |
|---|---|---|
Germline mosaicism | A mutation | on may not be in the blood |
Tissue specificity | Some tissues are affected, others are not | |
Low percentage of mutant cells | The mutation signal is diluted. | . |
Maternal germline | Eggs cannot be sampled easily. |
✨ Core Message of the Slide
A normal genetic test does NOT always mean:
No mutation exists.
It might mean:
The mutation is present in only a small number of cells
Or only in germ cells
🔎 Clinical Importance
This matters because:
Parents with normal testing can still have a recurrence risk.
Cancer detection depends on identifying small mutant clones.
Negative blood tests don’t always exclude mosaicism.
Important parameters of Gaussian curves = mean and variance.
Standard deviation = the square root of variance.
Variances are additive.
Vp = VG + VE
Vp = total variance of a phenotype; Vg = genetic variance. Ve = environmental variance.
h2 = Vg/Vp = Vg/Vg+Ve.
WHAT IS HERITABILITY?
It is the proportion of the overall variance of a character that is due to genetic differences.
🌡 Think of it like a cup filling with water
Everyone has a certain risk level for a disease or trait.
That risk comes from:
Many small-effect genes
Environment (diet, stress, smoking, etc.)
This risk builds up gradually — like water filling a cup.
🚨 The “threshold” is the tipping point
If the water doesn’t reach the top, nothing happens → you’re unaffected.
If the water crosses the top (threshold) → the disease appears.
So even though the outcome is yes or no (you have it or you don’t),
the underlying risk is gradual and continuous.
🧬 Example 1: Cleft palate
Many small genetic + environmental factors increase risk.
But in the end, the baby either:
Palatal shelves fuse → normal
Don’t fuse → cleft palate
The fusion only fails if the risk passes a certain threshold.
❤ Example 2: Blood pressure
Blood pressure varies continuously.
But we call it hypertension only if it crosses a certain number (e.g., 140/90).
That number acts like a threshold.
🧠 One-line summary:
The threshold model means many small risk factors add up quietly — and only when they pass a certain limit does the disease show up.

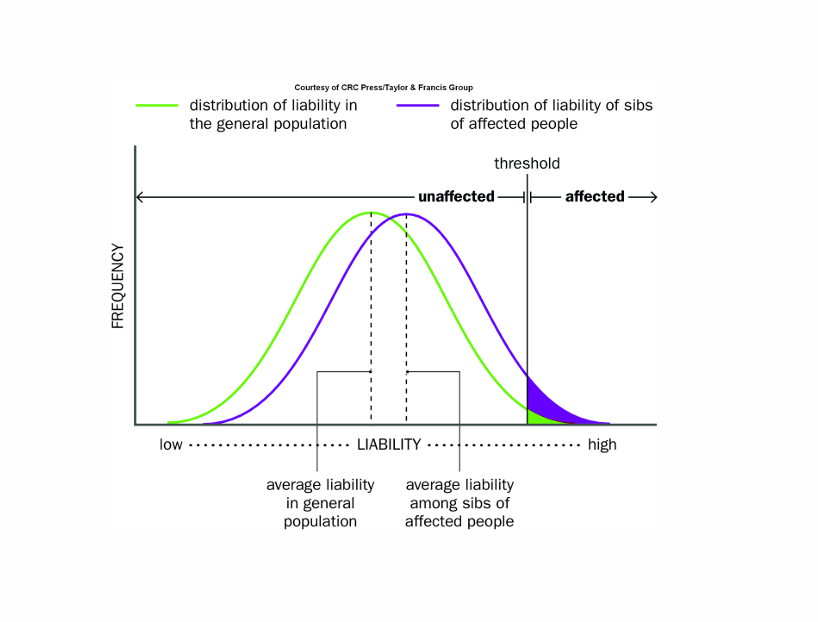
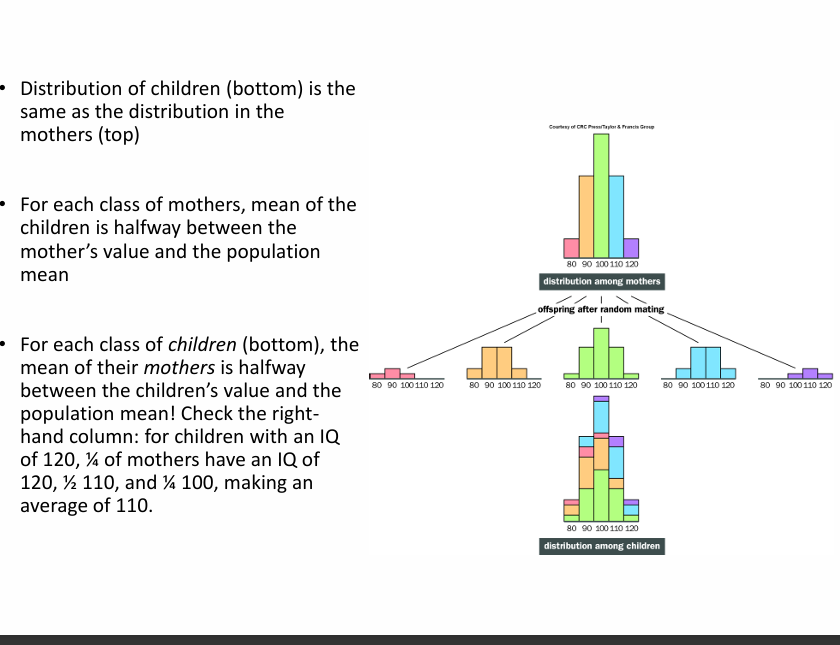
What happens to the siblings of an affected person?
Compared to the general population;
Their entire bell curve is shifted slightly to the right.
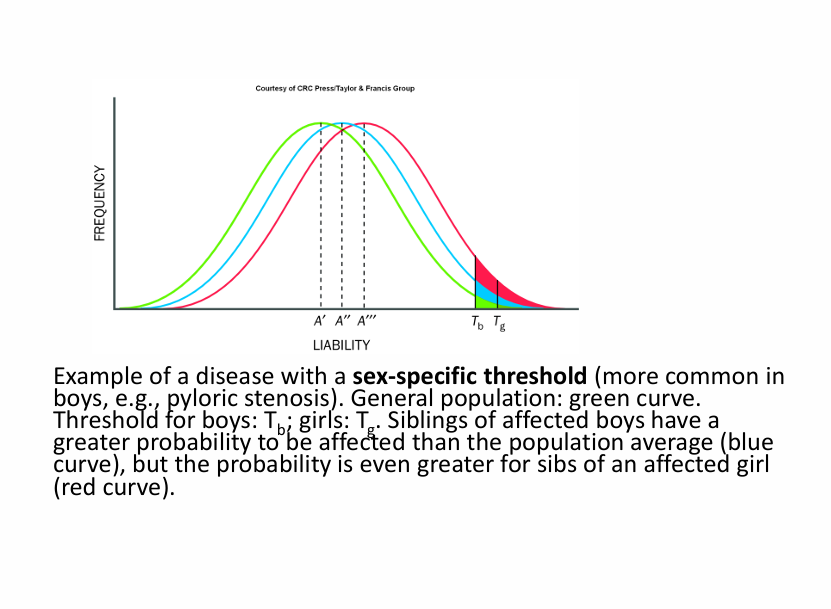
Key Note:
Compared to the general population, the probability for the sibling to be affected is more to the right.
The probability that the sibling of an affected girl is affected is much higher than the probability that the sibling of an affected boy is affected.