Lung Cancer (MORE)
LEARNING OBJECTIVES
Describe the 4 main types of lung cancer: etiology, pathology, staging, treatment and prognosis.
Distinguish small cell carcinoma from non-small cell carcinoma.
Outline the evidence linking smoking and lung cancer.
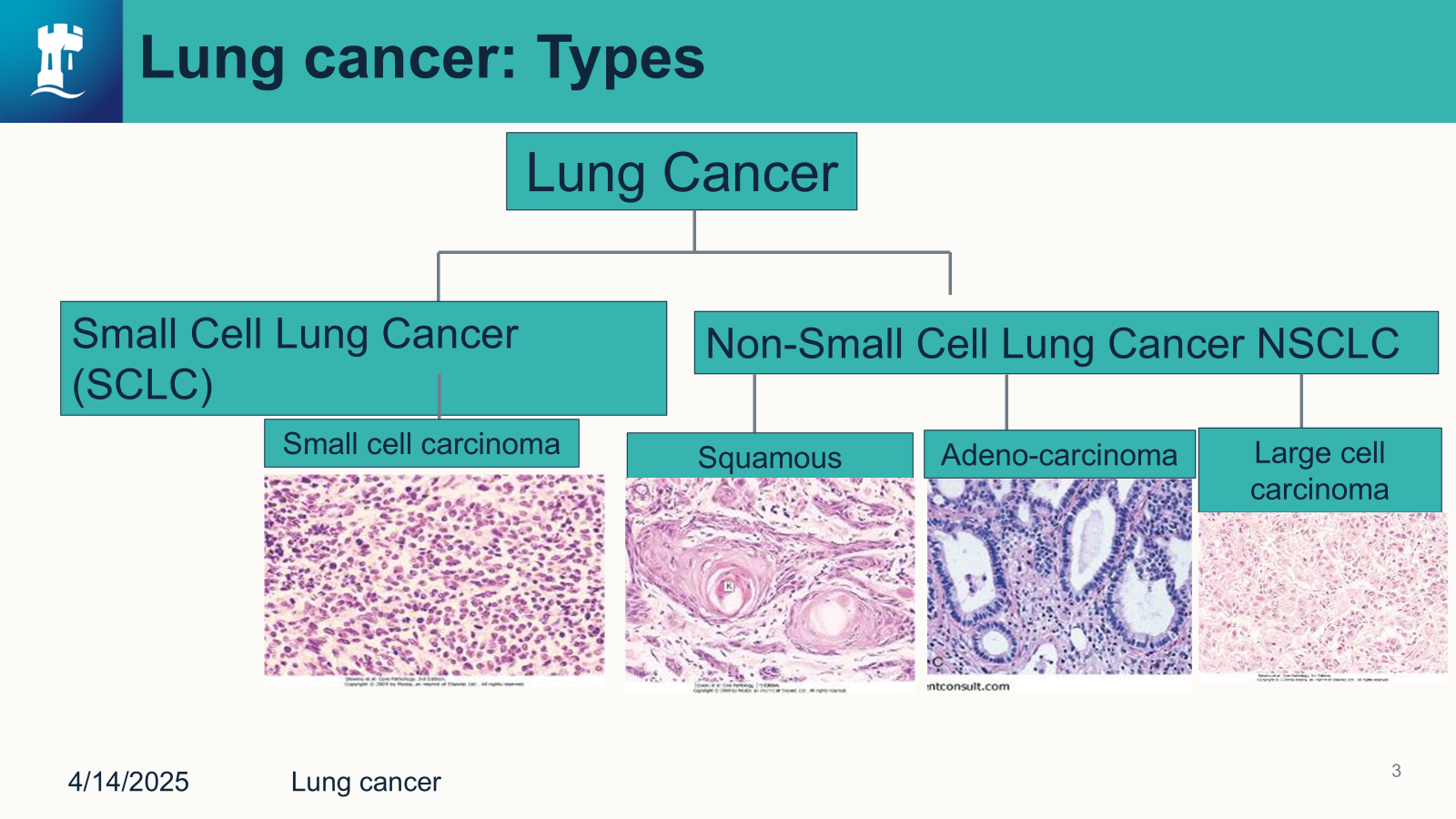
Non-Small Cell Lung Cancer
Squamous Cell Carcinoma
Etiology
Tobacco smoking - 90% of cases.
Occupational and environmental exposure e.g asbestos
Genetic factors e.g EGFR mutations
Chronic Inflammation - COPD
Infection - HPV/HIV.
Pathology
Found mainly in central part of the lung - the hilum or main bronchi.
Individual cell keratinization with abundant eosinophilic cytoplasm.
Pleomorphic cells with hyperchromatic nuclei
Stain more deeply than normal.
Squamous metaplasia → Dysplasia → invasive carcinoma
Penetrates the basement membrane and spreads to adjacent lung tissue.
Can spread to supraclavicular lymph nodes.
Prognosis depends on the histological grade, tumor size and molecular markers
TP53 mutations are associated with resistance to therapy.
Staging
T- Tumor (Primary Tumor Size and extent)
T1: Tumor <3 cm in greatest dimension, surrounded by lung or visceral pleura, without invasion into main bronchus.
T2: Tumor >3 cm but ≤ 5cm or involving the main bronchus with carina involvement, invading visceral pleura, or causing atelectasis/obstructive pneumonia.
T3: Tumor >5 cm ≤ 7cm or invading chest wall, phrenic nerve or parietal pericardium.
T4: Tumor >7 cm or invading mediastinum, diaphragm, heart, great vessels, trachea, esophagus or recurrent laryngeal nerve.
N- Lymph Node Involvement
N0: No regional lymph node involvement.
N1: Metastasis in ipsilateral peribornchial or hilar lymph nodes.
N2: Metastasis in ipsilateral mediastinal or subcarinal lymph nodes.
N3: Metastasis in contralateral mediastinal, contralateral hilar, or supraclavicular lymph nodes.
M - Metastasis (Distant Spread)
M0: No distant metastasis
M1: Distant Metastasis Present
SCC is staged as:
Stage 0 (carcinoma in situ): T1, N0, M0
Stage 1: T1/T2, N0 and M0
Stage II: T2/T3, N0/N1, M0
Stage III: T1-T3, N2/N3, M0
Stage IV: Any T, Any N, M1
Treatment
Depends on the stage
Stage I/II → Surgery and adjuvant therapy.
Stage III → combination of chemotherapy, radiation therapy, and sometimes surgery.
Stage IV → Chemotherapy, immunotherapy, and targeted therapies.
Adenocarcinoma
Pathology
Accounts to approximately 40% of lung cancers → especially in non-smokers and females.
Can be subdivided into preinvasive, minimally invasive and invasive adenocarcinoma.
Arises from the epithelial cells of the alveoli and terminal bronchioles.
Formation of glandular structures lined by columnar or cuboidal epithelial cells.
Mucin production, which can be identified using mucin stains.
Usually stain positive for cytokeratin 7 , thyroid transcription factor-1, and Napsin-A, but they stain negative for cytokeratin 20.
Cells with enlarged, hyperchromatic nuclei.
Can spread to adjacent lung parenchyma, pleural, and chest wall.
Early involvement of hilar and mediastinal lymph nodes.
Frequently metastasize to the brain, liver, bones, and adrenal glands.
Staging/Treatment
Same as squamous cell carcinoma
Large cell carcinoma
Pathology
Characterized by high mitotic rate and necrosis: large, bulky undifferentiated tumor cells with abundant cytoplasm.
Poorly differentiated carcinoma, making it difficult to diagnose accurately.
Due to its aggressive nature and lack of specific histological features, LCC often presents at advanced stage with poor prognosis.
Can occur anywhere in the lung but is more frequently found in the peripheral lung.
Common sites of spread include the regional lymph nodes, liver, bone, brain and adrenal glands.
Small Cell Lung Cancer
Small cell lung Cancer
Etiology
Rare in non-smokers
Mainly characterized by rapid growth, early metastasis, and poor prognosis.
Smoking is an important risk factor > 90% of all cases.
Originate for neuroendocrine Kulchitsky cells in the bronchial epithelium.
Kulchitsky cell are scattered specific cells which lie close to the basement membrane of the bronchi and bronchioles.
These cells respond to chemical or mechanical stimuli by releasing neuropeptides and neurotransmitters, implicating them as airway sensors.
Angiogenesis and immune evasion play a crucial role in progression.
Pathology
Typically arise in the central (hilar) region of the lung.
Soft, friable, and poorly circumscribed masses - associated with extensive necrosis and hemorrhage.
Small, round to oval cells with scant cytoplasm.
Hyperchromatic nuclei with fine granular chromatin (“salt and pepper” appearance)
Frequent vascular invasion and lymphatic spread.
Almost all cases relapse due to chemotherapy resistance.
Staging
Staged using two primary systems:
Veterans Administration Lung Study Group (VALG)
TNM (Tumor, Node, Metastasis) Staging system
VALG: Classifies SCLC in two stages
Limited-stage SCLC (LS-SCLC)
Cancer is confined to one hemithorax and can be encompassed within a single radiation field.
Involvement of ipsilateral (same side) hilar and mediastinal lymph nodes is allowed.
May include limited supraclavicular lymph node involvement.
No distant metastases.
Accounts for approximately 30-40% of SCLC cases.
Extensive-Stage SCLC (ES-SCLC)
Cancer has spread beyond ipsilateral hemithorax.
Includes distant metastases to the liver, brain, bones, adrenal glands, and contralateral lung.
Malignant pleural or pericardial effusion is classified as extensive-stage.
Accounts for approximately 60-70% of SCLC cases at diagnosis.
Treatment
Based on staging
LS-SCLC: chemotherapy, radiation therapy, prophylactic cranial irradiation, surgery.
ES-SCLC: Combination of chemotherapy and immunotherapy, radiation therapy, whole brain radiation therapy.
Rate of recurrence is high
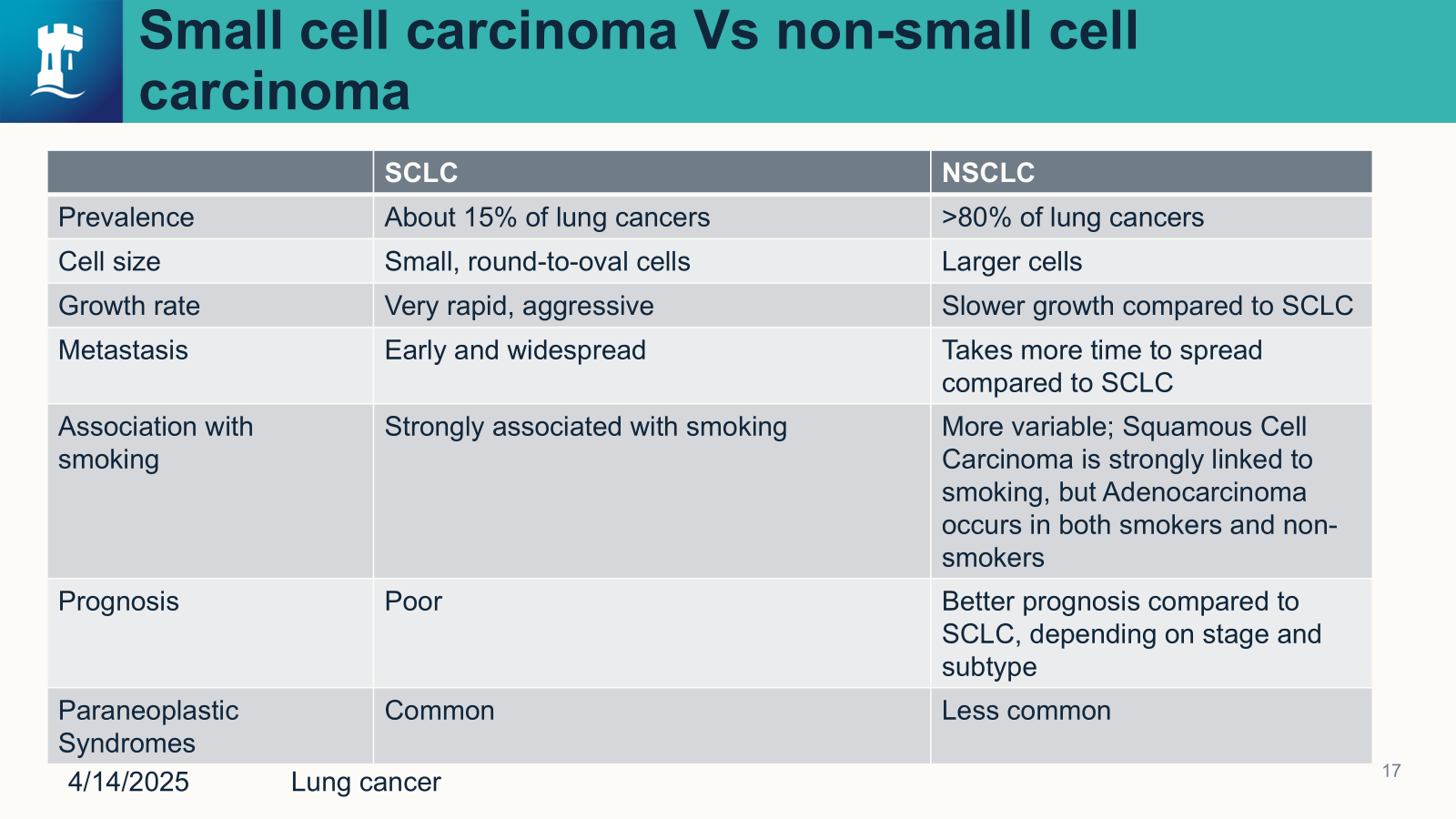
Small cell carcinoma vs Non-small cell carcinoma
Smoking and Lung cancer
Exposure to tobacco has a great effect on the genetic instability of tumor cells.
Reactive oxygen species (ROS) from prolonged tobacco use cause the body to create large amounts of oxygen-free radicals, which directly cause DNA fragmentation and harm purines, pyrimidines, and deoxyribose.
Second hand smoke:
The risk of lung cancer significantly increased with the duration, intensity, and pack-year of SHS exposure.
Exposure to SHS increases by more than 20% the risk of lung cancer among never-smokers, providing definitive evidence of the associated between SHS exposure and lung cancer risk.