Clinical LEC 2.5 - Cognitive Behavioural Therapy and REBT Insights (need to go over)
Instructor: Dr Ruth Hurley
Contact: r.hurley@lancaster.ac.uk
Page 6: Understanding Psychotherapy
Focus: Psychological treatments for Common Mental Health Conditions (CMHC).
Page 7: Importance of CBT
Rationale for Coverage:
Competency requirements in DClinPsy programs emphasize knowledge of therapy models and their applications in practice.
For example, Unit 1 on CBT includes knowledge of its principles and rationale for treatment.
Emphasis on psychotherapy as a core competency in DClinPsy training programs.
Page 8: Recommendations by NICE
CBT Recommendations:
The National Institute for Health and Care Excellence (NICE) recommends CBT for mild to moderate depression and specific anxiety disorders.
Report: 1.76 million referrals to NHS Talking Therapies for Anxiety and Depression (TTAD) programs in England during the year 2022/23.
Page 9: Implicit Processes and Conscious Awareness
Cognitive Processing: Much of cognitive processing is implicit, occurring outside of conscious awareness.
Freudian Concepts: There are three levels of awareness: conscious, preconscious, and unconscious.
Therapeutic Goal: Therapy aims to make implicit thoughts explicit, enabling conscious decision-making.
Page 10: Defining Cognitive Behavioural Therapy (CBT)
Description: CBT is a type of talking therapy focusing on changing unhelpful thoughts, feelings, and behaviors by modifying negative beliefs and thinking patterns.
Applications:
Healthcare settings (self-referred, hospital, or residential care).
Relationship contexts (families, romantic).
Educational settings (schools and universities).
Sports and exercise contexts (athletes and exercisers).
Forensic settings (custodial and prison systems).
Organisational applications (business employees).
Page 11: Overview of CBT’s History and Evolution
Key Figures:
Dr. Albert Ellis (1913-2007)
Dr. Aaron Beck (1921-2021)
Further Reading: For detailed historical insights, refer to Rachman (1997).
Page 12: Evolution Timeline of CBT
Overview
1920s - 1950s: Dominance of Psychoanalysis/Psychodynamic theories.
1950s - 1970s: Emergence of Behavioural Therapy (First Wave).
Techniques based on Learning Theory, including classical and operant conditioning.
Key Contributors:
Joseph Wolpe’s (1958) studies on neurotic behavior and fear-reduction techniques like desensitization.
Hans Eysenck’s (1960) findings on behavioral therapy.
Focus on unlearning maladaptive behaviors using methods such as token economy and systematic desensitization.
1970s: Critiques of therapy effectiveness, highlighting Behavioral Therapy's limitations in treating depression.
1960s: Introduction of Second Wave - Cognitive Therapy (CT) emphasizing cognitive processes in treatment.
Founders: Aaron Beck (1964 onward) and Albert Ellis (1958 onward).
Late 1980s: Merge of Cognitive Therapy and Behavioral Therapy into CBT, integrating cognitive and behavioral homework practices.
Late 1990s: Development of Third Wave therapies incorporating Mindfulness-based CBT techniques.
Page 13: Further Evolution Details (1920s - 1970s)
Psychoanalysis and Behavioral Therapy
1920s - 1950s: Exploration of unconscious processes through psychoanalysis (Freudian methods: dream analysis, free association).
1950s - 1970s: Behavioral Therapy dominated therapy landscape focusing on behavior modification.
The approach based on unlearning maladaptive behaviors, emphasizing the need for learning theory methodologies.
Notable Techniques: Desensitization for fear reduction.
Page 14: Second Wave: Cognitive Therapy
Key Concepts and Developments
1960s: The emergence of Cognitive Therapy focusing on changing maladaptive thought patterns.
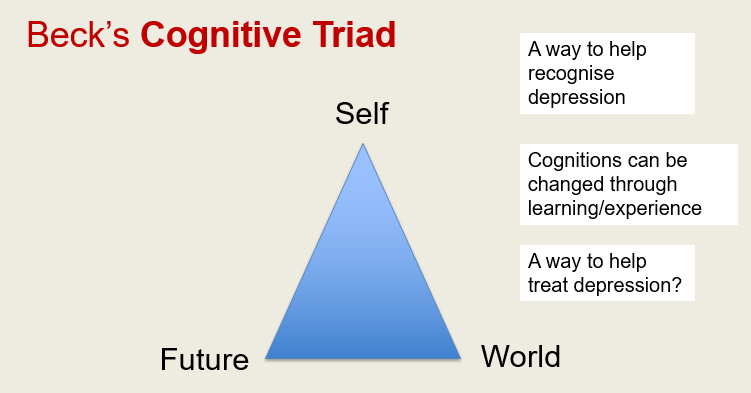
Beck’s Theory of Depression: Identifies negative triad of self, world, and future contributing to depression.
Ellis’s Rational Therapy: Emphasizes changing irrational beliefs.
Late 1980s: Combination of cognitive and behavioral methods in formalized CBT framework, addressing a wide range of psychological disorders.
Inclusion of cognitive theories explaining panic, OCD, phobias, and PTSD.
Page 15: Summary of Therapy Forms
Behavioral Therapy (BT): Focuses on classical and operant conditioning techniques for anxiety and behavior change.
Examples: Exposure therapy based on Pavlov's classical conditioning and reinforcement principles of Skinner.
Cognitive Therapy (CT): Addresses irrational/maladaptive beliefs and utilizes attribution theory.
Cognitive Behavioural Therapy (CBT): Incorporates strategies from both cognitive and behavioral therapies.
Notable figures: Albert Ellis and Aaron Beck, key in developing REBT and Beck’s CBT approach.
Page 16: Similarities Between Beck and Ellis
Comparison of Theoretical Approaches
Both were pioneers in Cognitive Therapy originating from the U.S.
Both emphasized the connection between thinking and emotional disturbances.
Proposed that many psychological issues arise from faulty cognitions.
Both approaches involved:
Challenging irrational beliefs through dialogue and behavioral exercises.
Focus on present context instead of past experiences.
Development based on therapeutic practices rather than pure theoretical frameworks.
Page 17: Later Developments in CBT
Third Wave Therapies
Late 1990s: Introduction of so-called “third wave” therapies such as:
Mindfulness-based Stress Reduction (MBSR)
Mindfulness-based Cognitive Therapy (MBCT)
Acceptance-Commitment Therapy (ACT)
Dialectical Behaviour Therapy (DBT)
These therapies focus on client awareness and thoughts' relationship to emotional responses and behaviors.
Page 18: Optional Extended Reading on Third Wave Therapies
Hays and Hofmann (2021): Overview of the evolution of third wave therapies (available at PMC).
Critical Accounts: Ron Purser’s (2019) critique on mindfulness in therapy (available in The Guardian).
Page 19: Introduction to Rational Emotive Behaviour Therapy (REBT)
Page 20: Terminology in REBT
Different Names for REBT:
“Rational Psychotherapy” (1955)
“RET” Rational Emotive Therapy (1961)
“REBT” Rational Emotive Behaviour Therapy (1993)
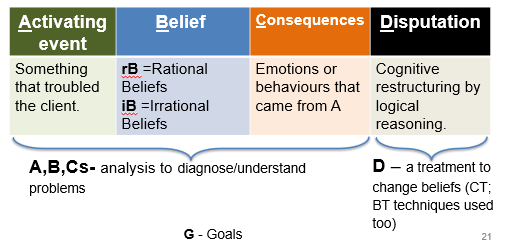
Page 21: Key Terms in REBT
Activating Event (A): Something that troubled the client.
Belief (B):
rB = Rational Beliefs
iB = Irrational Beliefs
Consequences (C): Emotions or behaviors resulting from beliefs.
Disputation (D): Changing irrational beliefs through cognitive restructuring.
Goals (G): Long-term objectives in therapy.
Page 22: The Image of the Person in REBT
Client Perspective: Each person pursues various goals and their definitions of happiness differ.
Rational and irrational thinking are viewed as biological tendencies which drive healthy or unhealthy emotions.
Empowerment in Change: Individuals have the potential to modify maladaptive thinking patterns through willpower, emphasizing free will in emotional disturbance rather than deterministic perspectives.
Page 23: Philosophical Influences on REBT
Core Principle: "People are disturbed not by things, but by their view of things" (Epictetus).
Therapeutic Aim: Identify and change illogical thinking patterns to alter emotional responses and behaviors.
Key Influences on REBT:
G. Kelly’s Personal Construct Theory (relationship between thoughts and behaviors).
Seligman’s Attribution Theory (attributes that affect individual interpretation of events).
Korzybski’s General Semantics Theory (importance of precise language in influencing thought and behavior).
Emphasis on humanistic approaches to foster individuality and self-acceptance.
Page 24: Beck’s Cognitive Triad
Concept Overview
Dimensions of Cognition:
Self
Future
World
Influences on Cognition:
Seligman’s Attribution Theory.
Korzybski’s idea on the non-absolute language's psychological impact.
Therapeutic Insight: Recognizing cognitive distortions can facilitate understanding and treatment of depression.
Page 25: Psychological Health in REBT
Health Concept: Acceptance of one’s impermanent nature and rational beliefs correlating to healthy emotional states.
Core Values: Self-acceptance, flexibility, tolerance for discomfort, and the understanding of one’s emotional landscape.
Page 26: Route to Therapeutic Change in REBT
Key Steps
Diagnosis (ABC analysis): Understanding client goals and identifying irrational beliefs and their consequences (A, B, and Cs).
Psychoeducation & Cognitive Restructuring: Promoting motivation to change, fostering self-acceptance, and applying logical exploration to irrational beliefs in pursuit of rational beliefs.
Internalization: Clients practice cognitive, emotive, and behavioral methods, recognizing the connections between beliefs and consequences.
Session Length: Typically, 5 sessions for simple, well-defined problems; longer for complex issues.
Page 27: Summary of REBT Theory
Source of Psychological Disturbances: Arises from individual thoughts, behaviors, and feelings.
Concept of Psychological Health: Defined by acceptance and compassion, with a tolerance for discomfort.
Differentiation from Psychoanalysis: Distinctions of responsibility, emphasizing personal cognitions over parental or historical factors.
Helping Clients Achieve Psychological Health: Fostering awareness of helpful vs. unhelpful emotions and facilitating the dispute of irrational thoughts.
Page 28: Psychological Disturbance: Cognitions
Focus on the cognitive components of psychological disturbances.
Page 29: Rational vs. Irrational Beliefs
Examples and Definitions
Rational Beliefs (rB):
Example: “Some people like me, some people don’t—it doesn’t make them bad.”
Characteristics of rBs: logical, reality-consistent, helper in goal achievement, tied to healthy emotions.
Irrational Beliefs (iB):
Example: “Everyone hates me—they are all awful people.”
Characteristics: rigid, reality-inconsistent, hindrance to goal achievement, linked to unhealthy emotional experiences.
Page 30: Core Types of Irrational Beliefs
Unhelpful Cognitive Patterns
Demandingness: Rigid musts and shoulds.
Awfulizing: Viewing unfortunate events with extreme negativity.
Frustration Intolerance: High demands for comfort and ease.
Global Evaluations of Worth: Devaluation of oneself or others as worthless.
Page 31: Additional Examples of Rational vs. Irrational Beliefs
Source: From Dryden & Neenan (2020), Rational Emotive Behaviour Therapy: 100 Key Points and Techniques.
Focus on distinguishing between rational and irrational belief systems to foster emotional clarity.
Page 32: Task 1 for Reflection
Construct Personal Insights
Reflect on demands placed on oneself or others.
Identifications: “I must…” “You must…” “The world must…”
Analyze potential conclusions drawn from these demands regarding self-worth and perceptions of others.
Page 33: Components of Irrational Beliefs
Structure: Irrational beliefs contain:
(i) Premise: Logical rules guiding thoughts (musts, shoulds).
(ii) Conclusion: Evaluations stemming from the premise.
This model assists in challenging irrational beliefs through logical reasoning.
Page 34: Revisiting the Components of Irrational Beliefs
Dual Structure: Reiterating the premise-conclusion dynamic within irrational beliefs to reinforce understanding and dispute techniques.
Page 35: Type-Specific Irrational Beliefs
Additional Examples
Recapping the irrational beliefs patterns, emphasizing the impact of demandingness, awfulizing, low frustration tolerance, and devaluation of human worth within personal experiences.
Page 36: Emotional Disturbance
Focus on Emotional Health and Management
Emphasizing balance between maladaptive (ME) and adaptive (AE) emotions, fostering acceptance and healthy emotional expressions.
Page 37: 'Maladaptive' Emotions Analysis
Goal of REBT Therapy: Transitioning maladaptive emotions to adaptive emotions through cognitive restructuring.
Comparison of emotional states e.g., from anxiety to concern, depression to sadness, etc.
Recognition that scientific definitions of maladaptive emotions can be subjective and contextual.
Page 38: Link between Beliefs and Emotions
Important Connections
Ellis’s Belief Model: Identifies how specific irrational beliefs correlate with unhealthy emotional outcomes (anxiety, shame, depression, etc.).
Page 39: Task 2 for Practical Application
Identify the rational beliefs and healthy emotions that therapists aim to cultivate in clients experiencing irrational beliefs.
Shift from demandingness to a more flexible mindset (e.g., “I prefer…” instead of “I must…”).
Compare mapping between unhealthy emotional responses and healthier cognitive reframing.
Page 40: Lecture Summary
Key Points of REBT Therapy:
Understanding ABCs: Activating events, beliefs, and consequences.
Distinguishing between rational and irrational beliefs and their emotional outcomes.
Recognizing the B-C connection (Beliefs leading to Consequences).
Utilization of diverse cognitive, emotive, and behavioral techniques in therapy.
Page 41: Preparation for Next Week
Reading and Note-Taking
Encouragement to analyze strengths and weaknesses of REBT therapy for deeper understanding in continual learning.
Page 42: Conclusion and Closing Thoughts
End of Lecture Notes:
Look for connections to future discussions and coursework!
Page 43: Encouragement for Student Engagement
Take the opportunity for fresh air and connection!