1d: Clinical Diagnosis copy
Diagnosis
not a single decision made at one point in time
a broader process
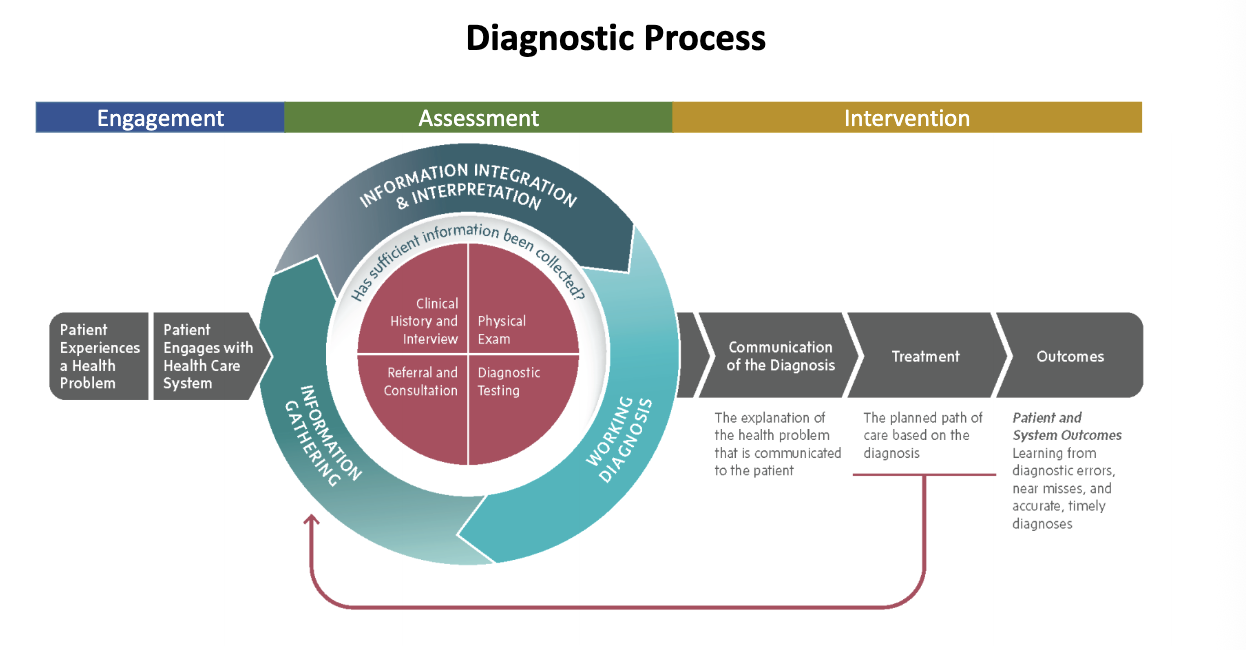
Engagement
Patient Experiences a Health Problem
Patient engages with the health care system through a diagnostic process.
Diagnostic Process Assessment
Gathering information from multiple sources:
Clinical History and Interview
Referral and Consultation
Physical Exam
Diagnostic Testing
Communication of the Diagnosis
Explanation of the health problem communicated to the patient.
Intervention
The planned path of care based on the diagnosis.
Outcomes
Patient and System Outcomes
Learning from diagnostic errors, near misses, and accurate, timely diagnoses.
Making a Diagnosis
Signs: Observable characteristics that accompany a disorder (e.g., flat affect, sleep difficulties).
we can see or measure
Symptoms: Subjective experiences that accompany a disorder (e.g., worry, hopelessness, hallucinations).
Syndrome: A cluster of signs and symptoms that commonly co-occur (e.g., panic attacks, anxiety, hyperventilation, tension).
signs + symptoms
Assumptions of the Medical Model:
Classifying abnormal behavior caused by underlying pathological processes.
Purpose of a Diagnosis
A diagnosis aims to:
Describe
Cause
Behavior (clinical characteristics and functional impairment)
Prediction (e.g., marital distress)
possible underlying mechanisms
Communicate
can communicate clearly with other including the patient
Legitimise
recognises patient experience in a formal system
Research
Diagnostic Classification Systems
International Statistical Classification of Diseases and Related Health Problems (ICD)
Originally created in 1900.
Morbidity added in 1948.
Currently in its 11th edition (2018).
Diagnostic and Statistical Manual of Mental Disorders (DSM)
Kraepelinian dichotomy of psychosis:
Manic depression
Dementia praecox
Originally published in 1952, currently the 5th edition (2013).
The Current Diagnostic System
Definition (American Psychiatric Association, 2013, p.20):
“A mental disorder is a syndrome characterized by clinically significant disturbance in an individual’s cognition, emotion regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes underlying mental functioning. Mental disorders are usually associated with significant distress or disability in social, occupational, or other important activities. An expectable or culturally approved response to a common stressor or loss, such as the death of a loved one, is not a mental disorder. Socially deviant behaviors (e.g., political, religious, or sexual) and conflicts that are primarily between the individual and society are not mental disorders unless the deviance or conflict results from a dysfunction in the individual, as described above.”
Major DSM-5 Mental Disorders
Categories:
Neurodevelopmental/Elimination
Neurocognitive
Substance-Related and Addictive Disorders
Schizophrenia Spectrum and Other Psychotic Disorders
Bipolar and Related Disorders
Depressive Disorders
Anxiety Disorders
Obsessive-Compulsive and Related Disorders
Trauma and Stressor-Related Disorders
Dissociative Disorders
Somatic Symptoms and Related Disorders
Sexual/Gender/Paraphilic Disorders
Feeding and Eating Disorders
Sleep-Wake Disorders
Disruptive/Impulse-Control and Conduct Disorders
Personality Disorders
Specificities and exclusions for diagnosis:
Causes clinically significant distress or impairment.
Not due to medical condition or substance.
Advantages of Diagnosis
Advances the search for causes.
Guides treatment selection.
Reliability of assessment.
Communication between individual and health professionals.
Cornerstone of clinical care.
provides shared language
Issues in Diagnosis and Classification
Concerns:
diagnosis is socially constructed
Labels, stigma, and discrimination
Overlooks the lived experience
Common underlying processes
Decision making
Categorical vs. dimensional
Sensitivity and specificity
Reliability and validity
Comorbidity complicates classification
Decision Making in Diagnosis
False Positives: Occur when one identifies or predicts a situation (like a diagnosis) incorrectly.
diagnose a disorder not present
False Negatives: Occur when one incorrectly identifies a condition as absent.
fail to identify a disorder present
especially serious, may miss out on treatment needed for a disorder present
hence, sensitivity is crucial for diagnostic tools
Sensitivity and Specificity
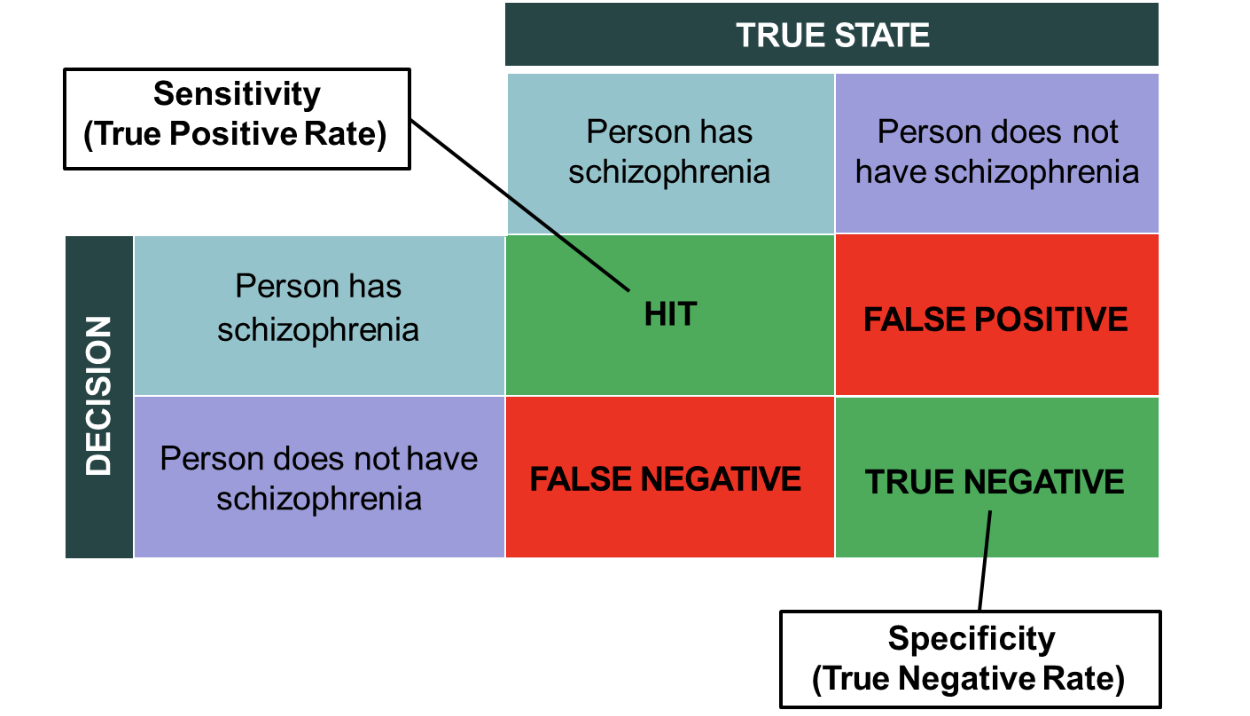
Sensitivity (True Positive Rate):
True State (Person has schizophrenia):
HIT
FALSE POSITIVE
True State (Person does not have schizophrenia):
FALSE NEGATIVE
TRUE NEGATIVE
Specificity (True Negative Rate): Measures the accuracy in identifying those without the disorder.
Categorical vs. Dimensional Approaches
Categorical:
Disorders are distinct; e.g., Major Depression differs from schizophrenia.
Presence/absence of a disorder is binary, either anxious or not.
approach supports strucutre and communication
oversimplifies experience
Dimensional:
Ranks symptoms on a continuous quantitative dimension.
Example: Degree of a symptom on a scale of 1 to 10.
there’s a threshold for diagnosis (e.g. scale 0-10, threshold is 5)
considerable variety across population
Moving Towards a Dimensional Approach
Asks if abnormality presents in degrees.
Differing models of classification include:
Categorical vs. dimensional (e.g., depressed mood).
Considers degrees of sadness and types of depression with varying degrees (e.g., reactive vs. clinical depression).
Comorbidity (simultaneous presence of 2+ conditions) in Diagnosis
Diagnostic Overlap:
E.g., Generalized Anxiety Disorder (GAD) and Major Depressive Disorder (MDD) share overlapping symptoms.
Statistics on prevalence:
Two disorders: 22%
Three disorders: 3%
One disorder: 75%
do diagnostic categories represent truly distinct conditions?
or does it represent partially overlapping processes
Reliability and Validity in Assessment
Inter-Rater Reliability:
Extent to which clinicians agree on a diagnosis.
Test-Retest Reliability:
Consistency of diagnosis over time with the same signs and symptoms.
Generally good for most DSM categories but may be lower in real-world settings than in research.
Beyond Categorical Diagnosis
Need for Alternative Frameworks:
To provide insights on why, how, and what behaviors present.
under a pure categorical framework, some patients may not qualify for a diagnosis
Focus on:
Severity of distress rather than all-or-nothing categories.
Psychological processes underlying distress across diagnoses.
Individual experiences, social context, and meaning-making shaping responses to threat.
Dimensional Framework
Understanding Psychological Distress:
Exists along continum of severity, not as absolute categories.
Mental health difficulties vary in degree rather than kind.
Captures meaningful distress without meeting diagnostic thresholds.
addresses Limitations of Categorical Diagnosis:
Symptoms are rarely simply present or absent; intensity, frequency, and impact vary across individuals.
Focus moves from “Does this person meet criteria?” to “How severe is the distress and how does it affect functioning?”
Dimensional Framework in Practice
Useful when:
Individuals remain highly functional.
They compare themselves to worse cases and believe they don’t need help.
Used alongside diagnosis for:
Access to services.
Formulation, treatment planning, risk assessment, and monitoring change.
Transdiagnostic Framework
Focus on Shared Psychological Processes:
Examines mechanisms that maintain distress rather than categories.
Developed in response to high comorbidity and overlapping criteria of disorders.
Suggests that many disorders reflect common underlying processes rather than distinct conditions.
Transdiagnostic Processes Identified
Common across cognitive, behavioral, and stress-based models:
Heightened threat sensitivity.
Avoidance behaviors.
Emotion regulation difficulties.
Maladaptive beliefs.
Attentional biases.
Stress reactivity.
Power, Threat and Meaning (PTM) Framework
Characteristics:
Focus on purposeful human behavior in social contexts rather than bodily processes.
Abnormal behaviors exist on a continuum with normal behaviors.
Emotional distress is mediated by biological, social, and cultural contexts.
Meaning, narratives, and subjective experiences are crucial.
alternatives to diagnosis need to focus on humans behaving purposeful in social and relational contexts (not on bodily processes or objects in the world)
abnormal behaviours exists on a continuum with normal behvaiour
experiences of emotinoal distress are enabled or mediated by biology
humans are fundamentally social beings whose experience of distress are inseparable from contexts
need to take meaning, narrative and subjective experience seriously
Key Questions PTM Asks:
Instead of:
“What is wrong with you?”
“What problems are you having?”
“What distress are you experiencing?”
It asks:
“What happened to you?” (Power)
“How did it affect you?” (Threat)
“What sense did you make of it?” (Meaning)
“What did you do to survive/cope?” (Threat Response)
Case Study: Alex
Profile:
33-year-old professional with chronic sleep difficulties, irritability, tension, and avoidance of social events.
Experiences persistent feelings of being “on edge” following workplace pressure and relationship breakdown.
Avoidant of seeking help due to perceived functional status.
Dimensional Framework Application:
Symptoms vary in intensity and impact.
Functional status does not negate clinically meaningful distress.
Transdiagnostic Framework Application:
Explores shared mechanisms contributing to Alex's distress and avoids categorical labeling.
PTM Framework Application:
Contextualizes Alex's experiences and tailors understanding to their individual narrative.
Summary
Categorical Models:
Prioritize reliability and structure but risk oversimplification.
Dimensional Models:
Capture severity and variability but are harder to implement in structured systems.
Comorbidity:
Challenges distinctness of diagnostic categories.
Transdiagnostic Frameworks:
Focus on shared psychological mechanisms across disorders.
Power Threat and Meaning:
Reframes distress as meaningful and contextual rather than purely pathological.
Understanding differences among these approaches:
Essential for critically evaluating modern diagnosis in psychology.