Chapter 2 Immunity
Learning Outcomes
Define and apply key immune-related terms
Differentiate innate vs. adaptive immunity
Describe lymphocytes, macrophages, and antigen-presenting cells
Explain primary vs. secondary antibody responses; compare types of T lymphocytes in cell-mediated immunity
Describe immunoglobulin classes (IgA, IgD, IgE, IgG, IgM)
Discuss altered immune function: host defense failure, hypersensitivity, autoimmunity, alloimmunity, immunodeficiency
Apply concepts to clinical models (e.g., lupus, HIV/AIDS)
Stress and Immunity
Stress can negatively affect body homeostasis
Universal experience
Can contribute to development/exacerbation of disease and the tendency to engage in negative behavior
Can arise from many events, including those perceived as positive
Chronic stress weakens immunity, increases disease risk
The Stress Response
Hans Selye observed physiological changes from stress
General adaptation syndrome (GAS)
alarm stage - the initial reaction, activation of fight or flight, increase in stress hormone release, increased HR and BP
resistance stage - adaptation to stress response
exhaustion stage - breakdown of defenses from chronic stress, illness is most likely
Local adaptation syndrome (LAS)
confines damage to one area
inflammation after an injury
predictable
individual variability
past experiences and support system can influence
Stress response is somewhat predictable with individual variability
conditioning factors
some coping strategies can minimize/eliminate effects
Overview of Immunity
Immunity: recognition & neutralization of foreign substances (antigens)
Immunology: study of immune system & its function
Key principles:
Specificity → cells seek & destroy invaders
antibodies for measles only attack measles, useless against the flu
Memory → faster response on re-exposure (basis for vaccines)
Core Components
Antigen = foreign particle that triggers immune response
bacteria, viruses, toxins, abnormal cells
Leukocytes = primary immune cells (innate & adaptive)
white blood cells
Body is constantly under microbial assault
System is self-regulated & self-limiting → must distinguish self from non-self
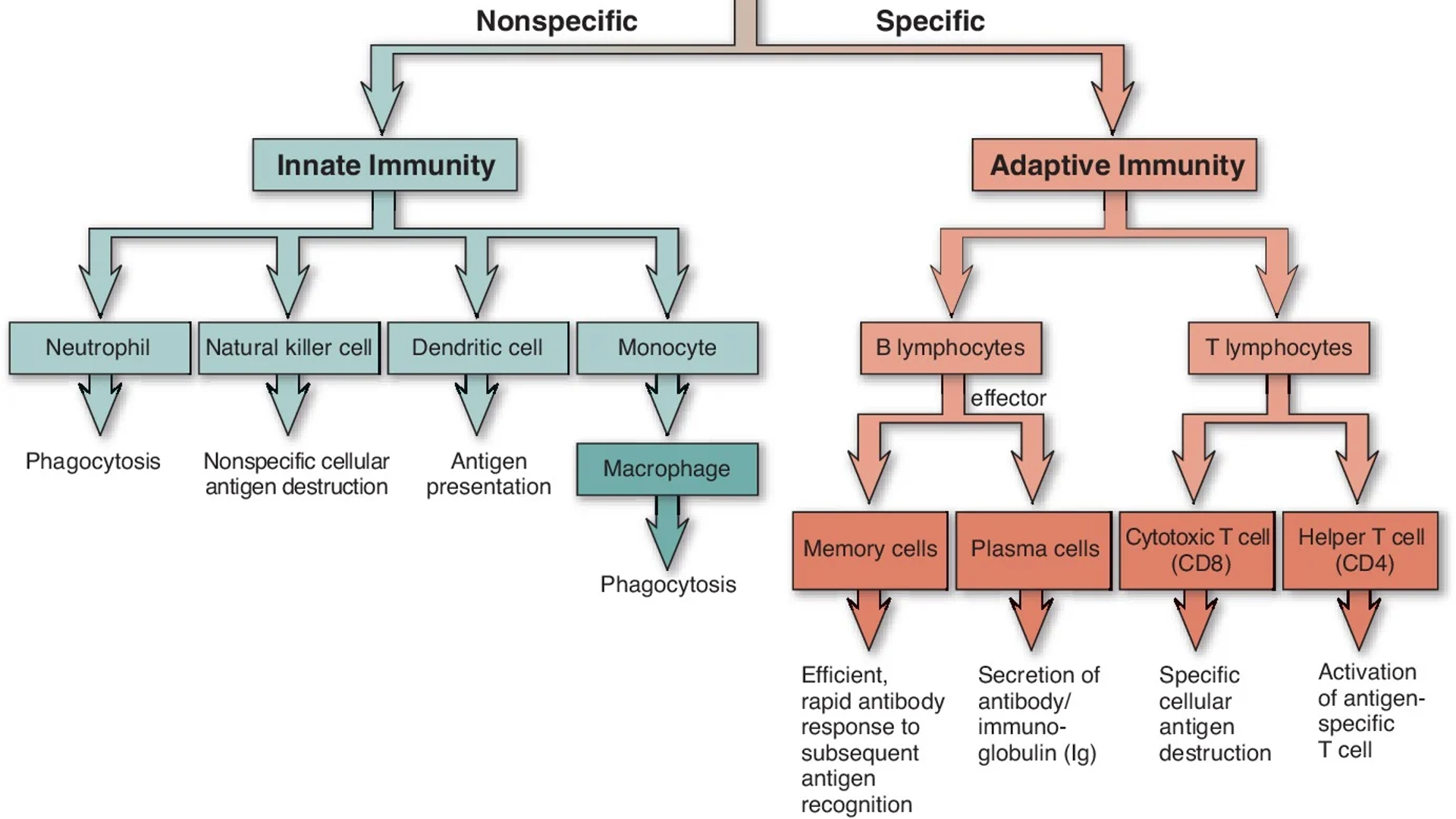
Layers of immunity:
Innate defenses (nonspecific, immediate)
Adaptive defenses (specific, memory)
Lymphatic system (organs/tissues coordinating immune responses)
Lymphocytes and Organs of Immunity
Lymphocytes: basic unit of the immune system
Type of Cell | Description |
|---|---|
T Lymphocytes | Mature in the Thymus (Cell mediated immunity) |
Cytotoxic T cells (CD8+) | Directly destroy virus-infected and abnormal cells, killer cells |
Helper T cells (CD4+) | Coordinate the immune response, activate B cells, cytotoxic T cells, and macrophages |
Suppressor (Regulatory) T cells | Suppress excessive immune responses, help prevent autoimmunity, the brakes of the immune system |
B Lymphocytes | Develop in bone marrow (antibodies) humoral immunity |
Plasma cells | Produce antibodies |
Memory B cells | Provide faster responses to future exposure, long-term protection |
Natural Killer (NK) cells | Part of innate immunity, destroy virus-infected and cancer cells, do not need prior exposure to an illness |
Lymphatic system:
Transports lymphocytes and immune cells
Lymph nodes act as immune checkpoints
Organs of Immunity
Primary (Central): Bone marrow & Thymus
bone marrow - the training center, development
thymus - maturation site
Secondary (Peripheral): Lymph nodes , Spleen , Tonsils, Appendix
Innate Immunity
Category | Details |
|---|---|
First line of defense | Present at birth, lasts a lifetime |
Barriers | Skin |
Inflammatory Response | Vasodilation |
Nonspecific Response | Same response regardless of pathogen, no memory |
Cellular Components | Neutrophils |
Key Substances | Pyrogens: fever-inducing substances |
Adaptive Immunity
Acquired defenses that target specific antigens
Slower to develop, but provides memory for future protection
Key features:
Specificity: immune cells target one specific antigen
Memory: faster, stronger response on re-exposure
Self vs. non-self recognition prevents autoimmunity
Cellular players:
B lymphocytes: humoral immunity (antibodies)
T lymphocytes: cell-mediated immunity (Helper T, Cytotoxic T, Regulatory T)
Activation of Adaptive Immunity
Antigen enters the body
APCs like dendritic cells and macrophages engulf the foreign particle
Antigen-presenting cells recognize the antigen
through the MHC molecules
T and B cells become activated
Clonal expansion occurs
multiplication of T and B cells
all cells are programmed to respond to the same antigen
B cells → plasma cells
Cytotoxic T cells → directly attack
Helper T cells → support
Effector cells attack the pathogen
Memory cells remain for future protection
Recognition → Present → Activation → Expansion → Attack → Memory
Humoral vs. Cell-Mediated Immunity
Humoral Immunity
B Cells → Antibodies → Extracellular Pathogens
Body Fluids and antibodies
Cell-Mediated Immunity
T Cells → Infected Cells → Intracellular Pathogens
Target infected cells
Type of Immunity | Description |
|---|---|
Humoral Immunity | Mediated by B lymphocytes Produce antibodies (IgG, IgA, IgM, IgD, IgE) Antibodies neutralize toxins, coat pathogens, activate complement Provides defense mainly against extracellular pathogens Most effective for extracellular pathogens |
Cell-Mediated Immunity | Mediated by T lymphocytes Helper T cells (CD4+): coordinate immune responses Cytotoxic T cells (CD8+): directly kill infected/abnormal cells Regulatory T cells: suppress excessive immune activity Provides defense mainly against intracellular pathogens (viruses, cancer cells) |
Innate vs. Adaptive Immunity: Across the Life Span
Infancy:
maternal IgG provides temporary passive immunity
breast milk provides IgA protection
vaccinations build active immunity
Adolescence:
hormonal changes influence immune responses
increased risk for some autoimmune disorders
Older Adults:
immune senescence (aging of the immune system)
reduce B- and T-cell function
increased susceptibility to infection
reduced vaccine response
Inflammatory Response
Purpose:
eliminate the cause of injury
removed damaged tissue
generate new tissue
Types
acute → rapid, short-term
swelling, heat, localized redness, pain, loss of function
chronic → prolonged, ongoing
may come from unresolved inflammation, persistent infection, autoimmune infection
Medical Terminology
suffix “itis” = inflammation
examples: cellulitis, appendicitis
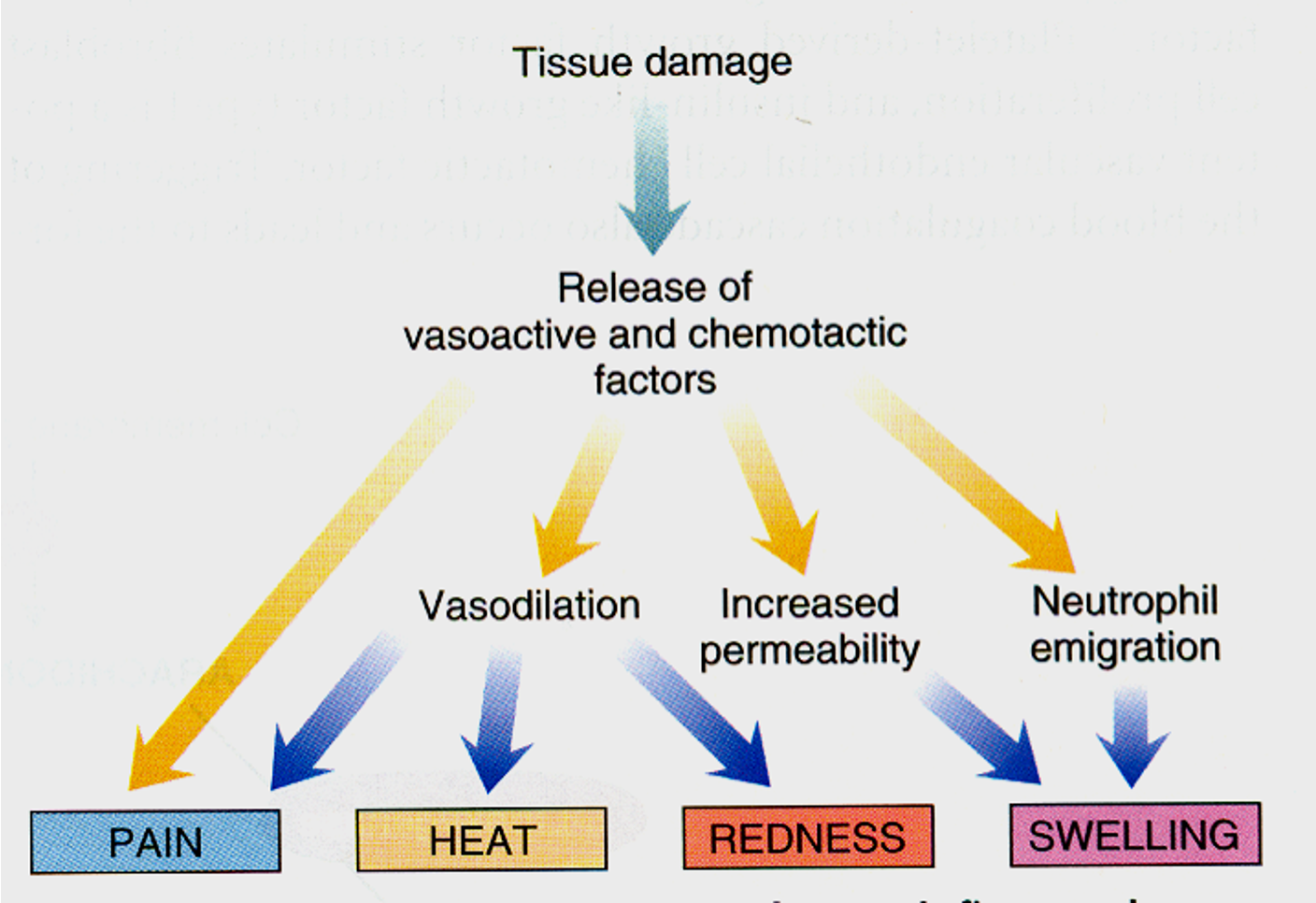
Key Inflammatory Mediators
Histamine - causes dilation of arterioles and increases permeability of venules (redness, warmth, swelling)
Prostaglandins - induce inflammation and potentiate effects of histamine (pain and fever)
Cytokines - induces priming and aggregation of neutrophils, mediators of systemic responses including fever, hypotension, and increased levels of corticosteroid hormones (cell communication and fever)
Cellular Response in Inflammation
Margination (move toward vessel wall) → Transmigration (diapedesis = leave bloodstream) → Chemotaxis (follow chemical signs, guide neutrophils to where they are needed) → Phagocytosis (engulf and destroy pathogens)
Neutrophils: The First Responders
First responder (~90 minutes)
Perform Phagocytosis
Increase during bacterial infections
immature - bands
mature - segs
Other Key White Blood Cells in Inflammation
Eosinophils (allergies and parasites)
increased during allergic reactions
control the release of chemical mediators
Monocytes (clean up crew)
second white cell to arrive
released to act as macrophages
Basophils/Mast Cells (histamine release)
release chemical mediators
histamine - increased vasodilation and vascular permeability
heparin
Alterations of the Immune System
Immune system requires all components to function properly
Failure leads to increased risk of disease and death
Major categories of dysfunction
host defense failure: inability to protect against pathogens
hypersensitivity: excessive or inappropriate immune response
autoimmunity: immune system attacks self-tissues (SLE)
alloimmunity: reaction against foreign tissue (ie transplant rejection)
immunodeficiency: weakened immune response (congenital or acquired)
Hypersensitivity Reactions - General Overview
Definition: exaggerated or inappropriate immune response that causes tissue injury or disease
Occurs when normal protective immune mechanisms become harmful
Can be antibody-mediated (Types I-III) or T-cell mediated (Type-IV)
Responses may be immediate (minutes to hours) or delayed (days)
Clinical Significance: contribute to allergy, autoimmunity, and transplant rejection
Types of Hypersensitivity
Type I (Immediate/Allergic) | Type II (Cytotoxic) | Type III (Immune Complex-Mediated) | Type IV (Delayed/Cell-Mediated |
IgE mediated, mast cells, and basophils involved T-helps stimulate B cells to produce IgE that sensitizes mast cells and basophils Immediate, local, or systemic Symptoms: vasodilation, bronchoconstriction, edema | Immediate (usually), target single cells IgG/IgM antibodies attack self cells IgG/IgM antibodies bind to antigen on host cells. activating complement and causing cell destruction Results in cell lysis and destruction | Antigen-antibody complexes deposit in tissues Activated complement → inflammation and tissue damage Widespread inflammation | Delayed, two phases: sensitizing and effector 24-72 hours T-cell mediated, delayed response Cytotoxic T cells and cytokines cause tissue damage |
Examples: allergies, anaphylaxis | Examples: transfusion reaction, Graves disease | Examples: lupus, rheumatoid arthritis | Examples: contact dermatitis, TB skin test |
Pathology of Anaphylaxis
Event | Description |
Initial Exposure | Allergen stimulates IgE production IgE binds to mast cells and basophils |
Re-Exposure | Allergen binds to IgE Mast cell degranulation occur |
Mediator Release | Histamines Leukotrienes Prostaglandins |
Clinical Effects | Vasodilation → Hypotension Increased permeability → Angioedema Bronchoconstriction → Wheezing Increased mucus → Respiratory distress |
Potential Outcomes | Airway obstruction Anaphylactic shock |
Diagnosis of Anaphylaxis
Clinical diagnosis is based on rapid onset of symptoms after allergen exposure
History of allergen exposures (food, drug, insect sting)
Key Findings
skin and mucosal changes (hives, angioedema)
respiratory compromise (wheezing, stridor)
hypotension or syncope
Labs (not acute): serum tryptase, allergy testing (later)
Clinical Manifestations of Anaphylaxis
Skin | Respiratory | Cardiovascular | Gastrointestinal | Severe Cases |
Hives (urticaria) Flushing Itching Angioedema (swelling of mouth and tongue) | Dyspnea Wheezing Stridor Throat Tightness | Hypotension Tachycardia Syncope Shock | Vomiting Diarrhea Abdominal cramps | Rapid Airway Obstruction Circulatory collapse Potential Death |
Treatment of Anaphylaxis
First-line: IM Epinephrine (0.3-0.5mg adult: 0.01mg/kg child) in mid-thigh
maybe repeated every 5-15 minutes
Call EMS immediately
Airway and oxygen support, possible intubation
IV fluids for hypotension
Adjunctive meds (used with epinephrine not in place of)
antihistamines (H1 and H2 blockers)
Corticosteroids (reduce late-phase reaction)
Beta-agonists (albuterol for bronchospasm)
Long-term: Epinephrine auto-injector, allergen avoidance, medical alert ID
Autoimmune Disorder: Systemic Lupus Erythematosus (SLE) -Type III Hypersensitivity Reaction
Chronic systemic autoimmune disease
Physical and Emotional Stress may precipitate disease flare ups
stress does not cause lupus
Stressors trigger exacerbations
Production of autoantibodies (ANA, anti-dsDNA)
Immune complexes deposit in tissues → inflammation and organ damage
Multisystem involvement: skin, joints, kidneys, heart, CNS
Diagnosis of SLE
ANA (antinuclear antibody)
screening test
positive result
it is sensitive but not specific to lupus
Anti-dsDNA and anti-Smith antibodies
highly specific and sensitive
Labs
anemia, leukopenia, thrombocytopenia
Urinalysis
proteinuria, hematuria (lupus nephritis)
Clinical Manifestations
Skin | Musculoskeletal | Renal | Cardiac | CNS | Systemic |
Butterfly (malar) rash Photosensitivity | Polyarthritis Joint Pain | Lupus Nephritis → proteinuria Hypertension | Pericarditis Risk of MI | Seizures Cognitive Dysfunction Headaches | Fatigue Fever Weight Loss |
Treatment of SLE
Medications
NSAIDS → joint pain, inflammation
Corticosteroids → reduce inflammation (acute flares)
Immunosuppressants (azathioprine, cyclophosphamide, mycophenolate)
Hydroxychloroquine (Plaquenil) → for skin/joint symptoms
Lifestyle
sun protection
infection prevention
Alloimmunity: Transplant Reactions
Transplant Rejection
Immune system recognizes transplanted tissue as foreign
Better tissue matching decreases rejection risk
Types of rejection:
hyperacute (minutes-hours)
acute (days-months)
chronic (months-years)
Graft-versus-host disease
donor immune cells attack recipient tissues
most common with bone marrow transplants
Recipient attacks graft = rejection
Graft attack recipient = GVHD
Immunodeficiency: HIV/AIDS
Diminished/absent immune response → infections
Categories
primary: present at birth due to inherited immune problems
secondary: develops later in life from external factors
General Features
HIV is the most common acquired immunodeficiency disorder
HIV destroys CD4+ (helper T) cells
Decreased CD4+ count → increased risk for opportunistic infections
ART suppresses viral replication and improves outcomes
Pathophysiology of HIV/AIDS
HIV is a retrovirus that targets CD4 helper T cells
Transmission:
blood
sexual contact
perinatal (mother to infant)
HIV enters and replicates inside CD4 cells
Progressive loss of CD4 cells weakens immunity
Increased susceptibility to opportunistic infections
AIDS develops when CD4 count falls below 200 cells/mm3 or an AIDS-defining illness occurs
Diagnosis and Monitoring of HIV
Screening | Viral Load (amount of virus) | CD4 Count (Strength of Immune System) | AIDS Diagnosis |
HIV antibody/antigen testing | Measures amount of HIV in the blood Used to monitor treatment effectiveness | Measures immune function Lower count = greater risk for infection | CD4 < 200 cells/mm3 Or an opportunistic infection is present |
Clinical Manifestations of HIV/AIDS
Acute Infection
flu-like illness
fever, sore throat, rash
high viral load
Clinical Latency
often asymptomatic
Gradual decline in CD4 cells
AIDS
CD4 < 200 cells/mm3
opportunistic infections
increased risk for certain cancers
HIV progresses from acute infection → latency → AIDS
Classic clues that HIV has progressed to AIDs
oral candidiasis (thrush)
pneumocystis jirovecii pneumonia (PCP)
Tuberculosis
Kaposi sarcoma
Treatment of HIV/AIDS
Goals of Treatment
suppress viral replication
increase/maintain CD4 count
prevent opportunistic infections
improve quality of life
Antiretroviral Therapy (ART)
lifelong treatment
combination of medications
must be taken consistently
decreases viral load and infections, increases CD4
Patient Education
medication adherence is critical
safe sex practices reduce transmission
regular follow-up and monitoring
Immune Response: Disease Prevention and Management
Vaccines and Immune Protection
vaccines expose the immune system to antigens
stimulate antibody production and memory cell formation
provide active immunity
reduce risk of infection and severe disease
help protect individuals and communities (herd immunity)
Vaccines work by creating immune memory before exposure to the real pathogen
Practice appropriate infection prevention while allowing normal environmental exposures
Lifestyle strategies:
smoking cessation
proper nutrition
regular exercise
moderate alcohol consumption
stress management