Cardio lec 9 - secondary Hypertension and Its Management: Key Concepts and Mechanisms
Primary Hypertension: 90-95% of cases, with no identifiable cause (also known as essential or idiopathic hypertension), typically associated with lifestyle factors and genetic predisposition.
Secondary Hypertension: 5-10% of cases, arises from identifiable causes like renal or endocrine issues, stressing the importance of recognizing and addressing underlying health conditions. Is often more severe than primary.
Secondary Hypertension Mechanisms
Key causes of secondary hypertension:
Renal Issues: Primary mechanisms involve impaired kidney function affecting blood pressure regulation; conditions such as chronic kidney disease can lead to secondary hypertension.
Endocrine Problems: Particularly the adrenal glands, Abnormalities in hormone secretion from adrenal glands influence blood pressure. For instance, excess aldosterone can lead to fluid retention.
Recognizing Secondary Hypertension
Age Factor: Typically seen in patients before 20 or after 50 whereas primary hypertension is more common in middle-aged patients,
Hypertension Severity: Secondary hypertension results in very high blood pressure (>210/120mmHg) compared to primary hypertension,
Additionally patient may present with low K+ levels (hypokaleamia) or symptoms of SNS overactivation which include variable pressure with tachycardia, sweating and tremors.
Response to Treatment: Lack of response to standard antihypertensive therapy may indicate secondary cause of hypertension. ,
Renal Causes of Secondary Hypertension
Normally the kidneys regulate extracellular fluid volume and blood pressure by modifying the glomerular filtration rate, reabsorption of Na+ and water and the Renin-Angiotensin-Aldosterone System (RAAS).
Most of the functions of the kidney is under the control of the RAAS therefore defects results in :
inappropriate rennin secretion - more angiotensin 2 production so more aldosterone is produced. AG2 is a potent vasoconstrictor , it constricts the efferent arteriole ,impacting kidney function and filtration thus contributing to elevated blood pressure levels. AG2 also induced Na+ reabsorption in the PCT and Aldosterone increases Na+ and H20 reabsorption in the DCT and collecting ducts.
These cause more Na+ retention and water retention - increasing extra cellular fluid/ blood volume and vasoconstriction consequently increasing the blood pressure (hypertension)
Causes of RAAS mediated hypertension (what causes RAAS defects)
Most common is Renal Artery Stenosis Impact- narrowing of one or both renal arteries.
Rarer causes include renin secreting tumours or oestrogen induced hypertension (if on contraceptive pill).
Renal Artery stenosis Diagnosis, causes and Effects:
Cause of stenosis
Atheroma narrowing of artery, 50% of the elderly (>70) have renal artery atheroma with 17% of these cases develop to completely blood the artery after 3-4 years
Other cause is fibro-muscular dysplasia (in younger patients)- where smooth muscle cells of arterial walls become stiffer causing narrowing of artery .
How does this increase BP?
Macular dense cells can sense sodium and chloride levels in the blood at the afferent arteriole.
Each afferent arteriole has a built in baroreceptor so it can sense and regulates its own pressure through a baro reflex.
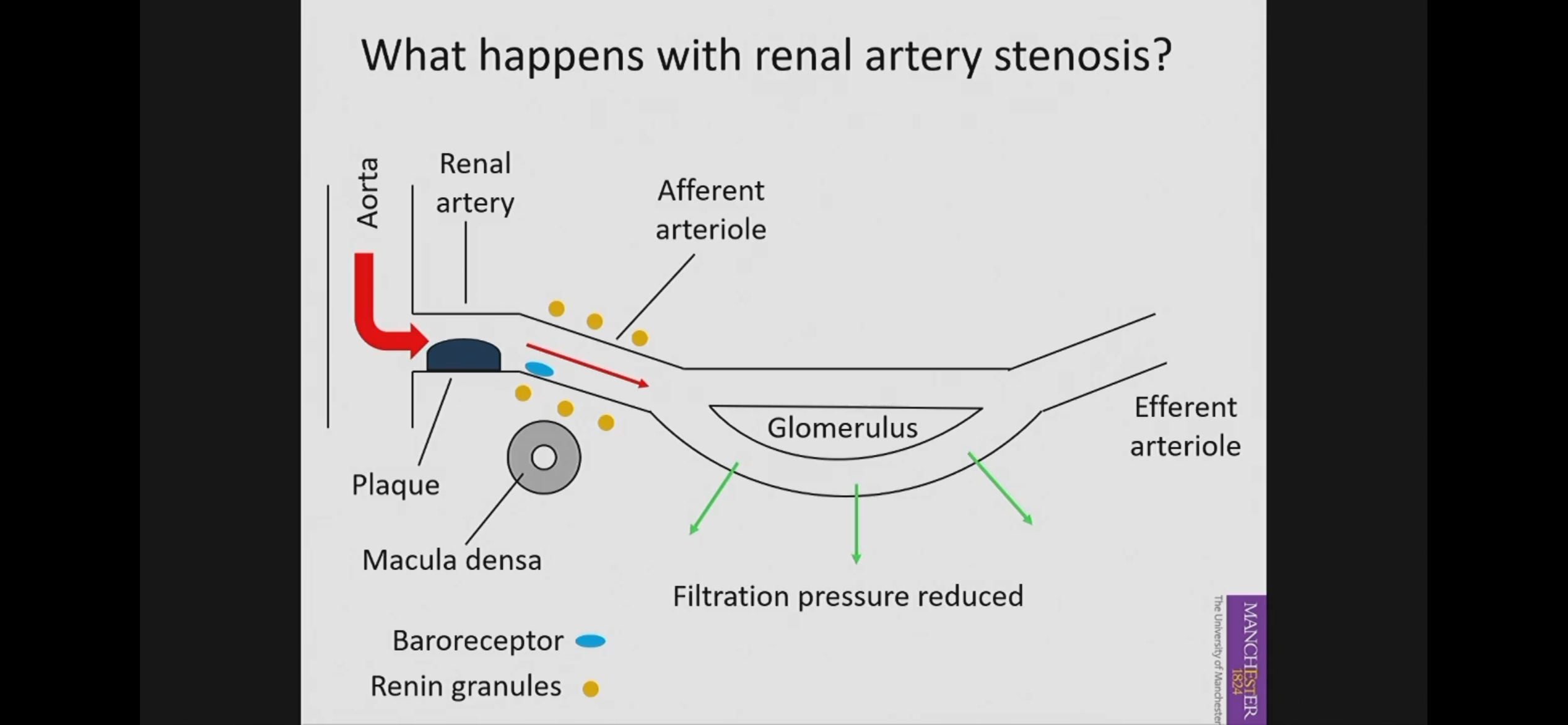
blood comes into the renal artery at normal pressure
When blood reaches plaque/stenosis it reduces the renal blood flow downstream of the stenosis
Consequently, there is reduced blood flow and pressure in the afferent arteriole and the glomeruls
Therefore there will be a reduction in filtration pressure and not enough filtration will occurs.
Baroreceptors in afferent arteriole detect the reduced BP and they stimulate renin secretion.
Renin is an enzyme that cleaves angiotensin to Ang I
Angiotensin converting enzyme (ACE) cleaves Ang Ito Ang II
Ang II is constricts the efferent arteriole reducing the blood flow but increasing BP downstream.
Consequences of RAAS activation :
Unilateral stenosis
Narrowing in one kidney leads to increased renin secretion to maintain GFR and results in Aldosterone secretion causing increased Na+ and H20 reabsorption causing increase in pressure. This would cause hyper filtration of the unaffected kidney maintaining normal renal function (so the unaffected kidney compensates by working more)
Bilateral stenosis
Narrowing in both kidneys reduces renal plasma flow overall and because the efferent Arterioles of both kidneys are constricted there is increased filtration fraction (so more plasma entering the glomerulus is going to be filtered more than normal) thus concentrating the plasma allowing fluid to be pulled from elsewhere which would increase the blood volume and subsequently BP. Increase in blood volume inhibits further renin secretion but hypertension is maintained due to over activation of the SNS.
Effects on salt and water balance
Unilateral stenosis :
Normal salt and water balance (salt intake matches salt excreted) because increased Ang II increases Na+ reabsorption in the PCT of the affected side and increased aldosterone secretion from adrenal glands increases Na+ reabsorption in DCT and collecting ducts on both sides of the kidney. Consequently increasing the pressure which causes pressure naturiuresis in the unaffected kidney which inhibits further Na+ reabsorption so more is excreted.
Bilateral stenosis:
Increased aldosterone causes increased Na+ reabsorption on both side but no pressure natriuresis, so excess Na+ can not be excrete so there is more water retention. This results in pulmonary oedema , ventricular failure and hypokalaemia
Treating renal caused hypertension.
Antihypertensive medication prior to angioplasty or by-pass graft surgery to remove plaque/ stenosis because surgery can’t be down when the BP is high.
Antihypertensive medications included alpha/beta blockers, diuretics (to reduce blood volume )or Ca2+ channel blockers (to reduce smooth muscle contraction) (ACE inhibitors is not ideal as ACE is needed to make sure BP is not too low.)
Adrenal cortex secretes mineralocorticoids (aldosterone) and glucocorticoids (cortisol).
Adrenal Causes of Secondary Hypertension
Primary Hyperaldosteronism (Conn’s Syndrome): Excess aldosterone secretion resulting in fluid volume expansion and hypertension, typically identified through laboratory tests measuring plasma aldosterone.
- caused by aldosterone secreting adenoma (mainly unilateral) and benign adrenal hyperplasia (mainly bilateral) .
- features of this is severe hypertension and hypokalaemia.
Cushing's Syndrome: Caused by increased glucocorticoids, leading to hypertension through various mechanisms including fluid retention, insulin resistance, and alterations in vascular responsiveness.
increased glucocorticoids can be caused by increased pituitary ACTH secretion and glucocorticoid production and therapeutic misuse of glucocorticoids or ACTH.
Patients present with weight gain, central obesity , stretch marks on abdomen, rounded face sexual dysfunction and severe hypertension.
Pheochromocytoma: Tumour of adrenal medulla (chromaffin cells)causing episodic or continuos hypertension due to catecholamine (noradrenaline/ adrenaline) overproduction. Treatment involves surgical removal after controlling blood pressure with alpha-adrenergic antagonist (antihypertensive) to manage acute episodes.
Excess adrenaline or NA secretion causes severe hypertension by increasing the total peripheral resistance (TPR) and CO
Episodes can be induced by tumour compression ie posture causing adrenaline production which increases. Frequency of episodes vary from several times a week or day for about 15 mins.
How does excess aldosterone secretion cause hypertension: Primary Hyperaldosteronism (Conn’s Syndrome):
Increased aldosterone secretion increases Na+ reabsorption in DCT and Cd which subsequently increases Water reabsorption.
Increased Na+ and water and absorption suppresses renin secretion.
Increased water and Na+ reabsorption causes ECFV and then plasma volume to increase which increases the cardiac output causing hypertension
Excess aldosterone also have a positive ionotropiceffect which increases contractility resulting in increased cardiac output exacerbating the hypertension.
Excess aldosterone stimulates K+ excretion from kidneys resulting in hypokalaemia. Low K+ in plasma is a vasoconstrictor thus further exacerbating hypertension,
Additionally, the increased Na+ increases the amount of total exchangeable sodium in addition to the extra ECFV expansion lead to the secretion of atrial natriuetic pepetide(ANP) which inhibits the Na+/K+ Atpase in the kidney thus inhibiting Na+ reabsorption (excess Na+ excreted)
Additioonally ANP inhibits NCX reversal in cardiac smooth muscle thus reducing electrochemical gradient for ca2+ exchange so rather than ca 2+ being excreted it is absorbed into the cell increasing vasoconstriction of the smooth muscle exacerbating the hypertension
How does excess cortisol/ACTH secretion cause hypertension: Cushing’s syndrome
Normally metabolising enzymes in the MR inhibit cortisol binding to the mineral-allocortisol receptors(MR) keeping the levels low but excess Cortisol secretion overwhelmed the enzymes allowing the receptor to be occupied by cortisol.
Additionally excess cortisol/ ACTH production increases the amount of deoxycortisone (an intermediate precursor to aldosterone production) which also binds to the MR further increasing MR occupancy
Consequently MR activity increases which causes incereased fluid and Na+ reabsorption which increases plasma volume and subsequently cardiac output causing hypertension.
Cortisol increases the shift from ICFV to ECFV thus increasing he plasma volume and subsequently increasing the CO , further exacerbating hypertension.
Cortisol increases the activity of phenylanalaminemethytransferase (PNMT) in the adrenal medulla which is an enzyme important for the production of catecholamines (adrenaline). This increases adrenaline production which increases contractility therefore increasing the cardiac output exacerbating the hypertension.
Excess cortisol also increases the amount of renin substrates thus increasing renin activity which in ur increases Ang II production which is a potent vasoconstrictor
Additionally excess cortisol reduces catecholamie (adrenaline) metabolism which exacerbates vasoconstriction and cardiac output
Excess cortisol also increases increases sensitivity of vessels to vasoconstrictors exacerbating vasoconstriction
Excess cortisol also reduces the secretion of vasodilators(kinins/PGs) which worsens vasoconstriction
Exacerbated vasoconstriction causes increased total peripheral resistance which further exacerbates hypertension .
Treatment Adrenal Causes:
Caused by adenoma or tumour - surgical removal of tumour on adrenal gland
Caused by carcinoma- surgery, pharmacotherapy (adrenolytic and chemotherapy), and radiotherapy
Caused by pituitary tumour - Removal of anterior pituitary (transphenoidal hypophysectomy)
In the case of adrenalectomy lifelong steroid replacement therapy is required.