3. Stomach & Small Intestine Interactions
Stomach – Structure & Mechanical Activity
Muscular layers
Typical GI tract: circular + longitudinal smooth muscle
Stomach adds a third, oblique layer → allows squeeze, shorten AND “wringing/twisting”
Sphincters keep contents contained during churning
Cardiac (gastro-oesophageal) sphincter – entrance
Pyloric sphincter – exit to duodenum
Contracted = closed; relaxed = open
Time course
~5 h for a normal meal to empty completely into the duodenum
Gastric Juice – Composition, Sources & Purpose
Hydrochloric acid (HCl)
Extremely low
Kills most microbes
Denatures (unfolds) protein → exposes peptide bonds
Activates pepsinogen → pepsin
Pepsinogen → Pepsin
Pepsin = protease initiating protein digestion
Secreted by chief cells as inactive “-ogen” for self-protection
Gastric lipase – minor fat digestion
Intrinsic factor (IF)
Required later (ileum/colon) for absorption → essential for erythropoiesis
Mucus
Thick, viscous, alkaline (high )
Produced by surface goblet cells → coats epithelium, buffers acid, lubricates rough chyme
Self-Protection Strategies of the Stomach
Goblet‐cell mucus barrier (thick + alkaline)
Proteolytic enzymes secreted as inactive zymogens (eg. pepsinogen)
Acid/enzymes only released when food is anticipated or present (regulated secretion)
Regulation of Gastric Function – Three Phases
Cephalic phase (“head”)
Trigger: sight/smell/thought of food
Parasympathetic (vagus) ↑ acid, enzyme, mucus secretion & mild motility (stomach “rumbling”)
Gastric phase (“stomach”)
Trigger: food distension & partly digested peptides
Local ENS reflexes + hormone gastrin (from G-cells) ↑↑ secretion & strong mixing waves
Intestinal phase (“small intestine”)
Trigger: chyme enters duodenum (low , hypertonic, fatty acids, amino acids, stretch)
Duodenal hormones:
Secretin → ↓ gastric motility/secretion; ↑ pancreatic
CCK (cholecystokinin) → ↓ gastric activity; ↑ pancreatic enzymes & bile release
Enterogastric reflex (neural) reinforces inhibition
Why Is Chyme Released Slowly?
Chyme features: low , hypertonic, partially digested nutrients
Small intestine tasks = finish digestion + absorb
Too large a bolus would:
Overwhelm enzyme supply → incomplete digestion/absorption
Create major osmotic pull → water shifts from blood → lumen → ↓ blood volume, hypotension, rapid transit
Deliver excessive acid → mucosal injury (needs buffering to )
Small Intestine – Anatomy & Functions
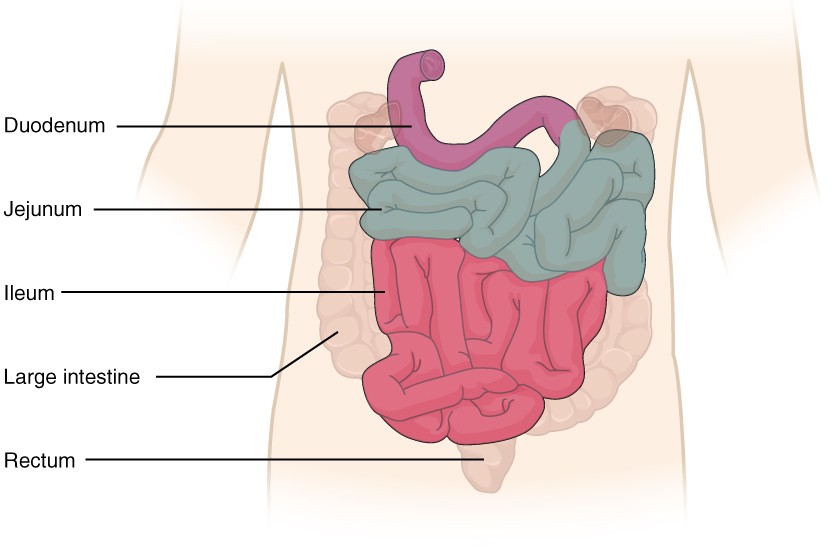
Regions (proximal → distal)
Duodenum (~25 cm) – finishes chemical digestion
Jejunum (~2.5 m) – bulk nutrient absorption
Ileum (~3.5 m) – remaining absorption; bile salts & –IF complex
Total length ≈ 5–6 m, yet internal surface ≈ tennis-court sized due to folds
Accessory Organ Inputs
Liver → bile production
Gallbladder → bile concentration & storage; contracts when signalled
Pancreas (99 % exocrine) → pancreatic juice
to neutralise acid
Enzymes: amylase (carbs), lipase (fats), protease zymogens (trypsinogen, chymotrypsinogen, etc.), nucleases
Sphincter of Oddi (hepatopancreatic ampulla) regulates common entry into duodenum
Zymogen Activation Cascade in the Duodenum
Pancreatic acinar cells release inactive enzymes
Brush-border enterokinase on mucosal microvilli:
Activates trypsinogen → trypsin
Trypsin then activates chymotrypsinogen & other pro-proteases
Protection rationale: prevents autodigestion of pancreatic & ductal tissues
Bile – Composition & Role
Made in hepatocytes, stored in gallbladder
Constituents
Bile salts (derived from cholesterol) – amphipathic
Bilirubin (heme breakdown product) – excretory pigment
Cholesterol, phospholipids, electrolytes, water
Function: emulsification (NOT hydrolysis) of dietary fat
Breaks large lipid globules → many small droplets → ↑ surface area for pancreatic lipase
Hormonal Coordination of Duodenal Events
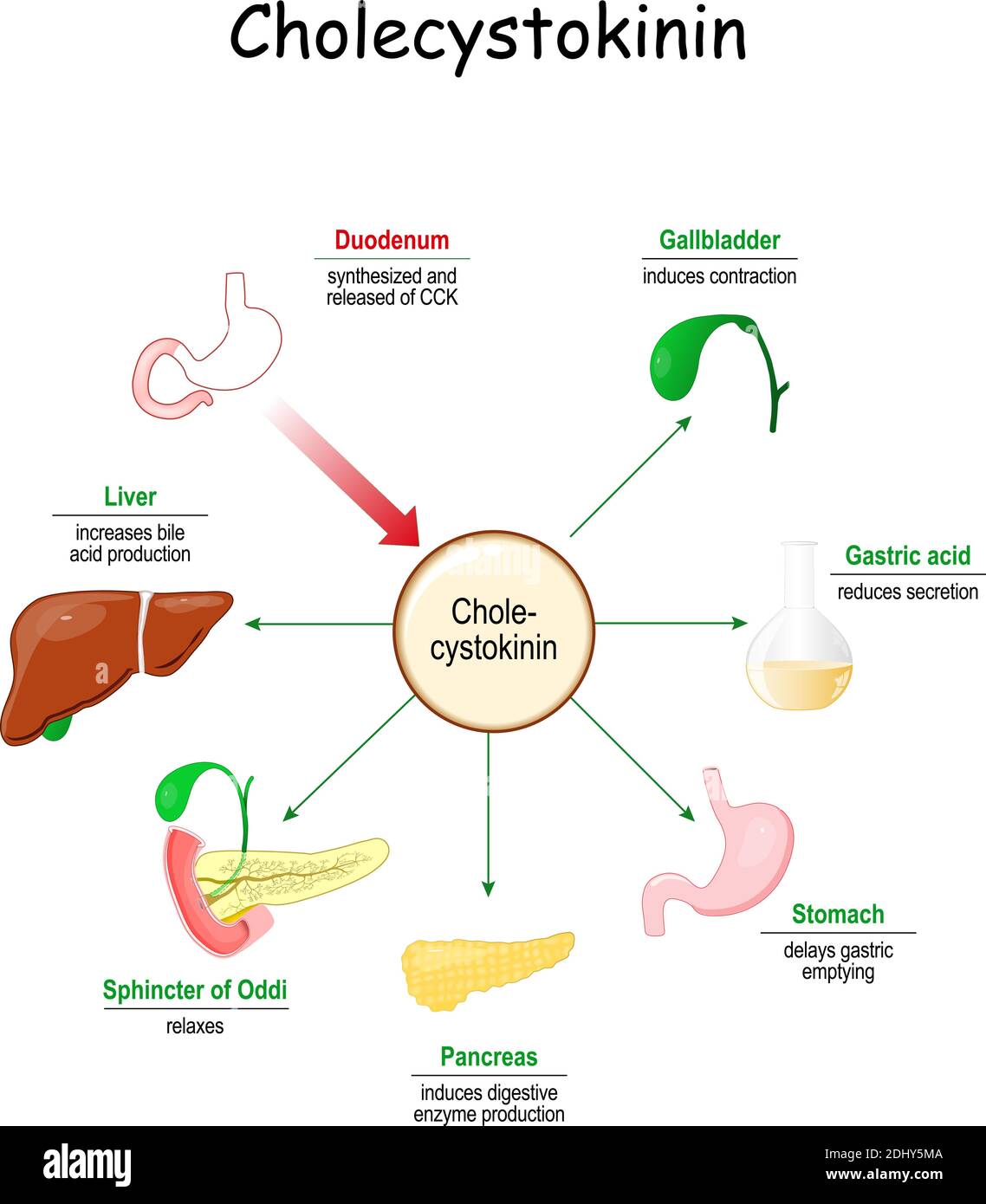
Stimulus: chyme (fatty acids + amino acids, low )
CCK (red dots in diagram)
Source: duodenal I-cells
Targets & actions
Pancreas → enzyme-rich juice
Gallbladder → contraction
Liver → ↑ bile production
Sphincter of Oddi → relaxation
Stomach → ↓ motility & secretion
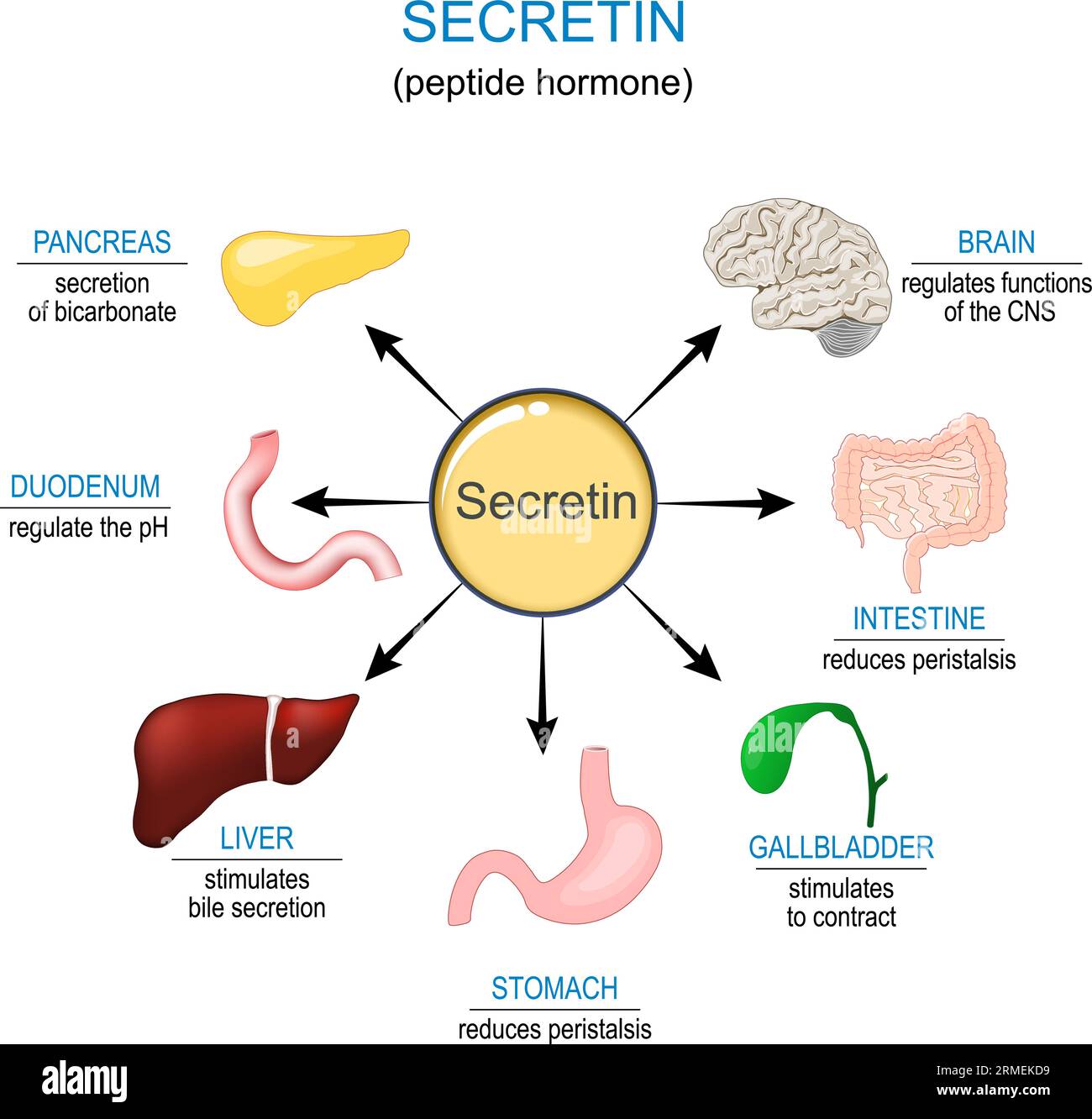
Secretin (yellow dots)
Source: duodenal S-cells (respond to acid)
Actions
Pancreas → bicarbonate-rich juice
Liver → synergises with CCK for bile flow
Stomach → ↓ acid output & motility
Intestinal Motility Patterns
Segmentation (localized circular contractions)
Mixes chyme with enzymes, exposes it to mucosa, slow propulsion
Peristalsis (longitudinal wave)
After most absorption or when new meal arrives -> clears chyme toward colon
Mucosal Adaptations for Absorption
Circular folds (plicae circulares) – large ridges ↑ area ×3
Villi – finger-like projections ↑ area ×10
Each villus contains
Capillary network → carries monosaccharides & amino acids to liver via portal vein
Lacteal (lymphatic capillary) → absorbs lipid-rich chylomicrons
Microvilli (“brush border”) on enterocyte apical membrane ↑ area ×20 & house brush-border enzymes incl. enterokinase
Peyer’s patches (ileum) – aggregated lymphoid nodules → immune surveillance
Mechanisms of Nutrient Uptake
Carbohydrates
Glucose and galactose are absorbed into intestinal cells through SGLT1, which is a sodium-dependent (Na⁺) secondary active transporter.
Fructose is absorbed via GLUT5, using facilitated diffusion, which does not require energy.
Proteins
Amino acids and small peptides are absorbed using Na⁺-coupled transport and H⁺/peptide cotransporters.
Lipids
Fatty acids and monoglycerides are carried to the intestinal wall by bile salt micelles, then absorbed via simple diffusion into the cell.
Inside the cell, they are re-formed into triglycerides, packaged into chylomicrons, and released by exocytosis into the lacteal (lymph capillary).
From the lacteal, they travel through the thoracic duct and enter the bloodstream.
Water
Water moves by osmosis, following the movement of absorbed solutes.
If the intestinal contents (chyme) are still hypertonic, water may flow back into the lumen, causing dehydration and diarrhoea.
Clinical / Physiological Implications & Connections
Gastrectomy (removal of the stomach) or chronic gastritis can reduce or stop the production of intrinsic factor (IF), leading to vitamin B₁₂ deficiency and pernicious anaemia.
Rapid gastric emptying (also called dumping syndrome) can cause low blood pressure, diarrhoea, and poor nutrient absorption due to fluid being drawn into the gut too quickly.
Pancreatitis risk increases if digestive enzymes (zymogens) are activated too early inside the pancreas, damaging tissue.
Digestive organs are interdependent:
Stomach damage not only affects digestion but also stops IF production.
Duodenum damage can impair hormones like CCK and secretin, leading to uncontrolled stomach activity.
The parasympathetic nervous system (rest-and-digest) stimulates digestion, while the sympathetic nervous system (fight-or-flight) slows it down. This links stress, digestion, and energy balance.