Flashcards
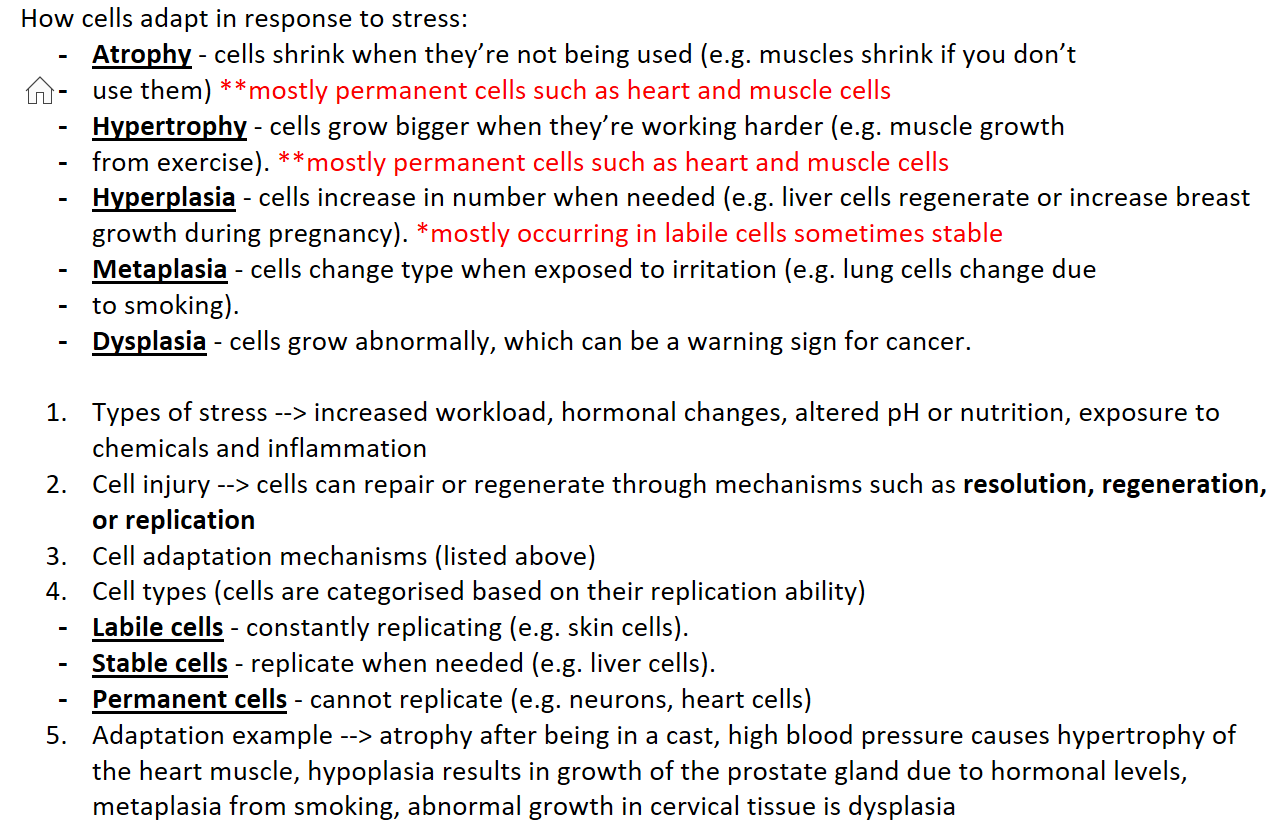
How cells adapt in response to stress:
Atrophy - cells shrink when they’re not being used (e.g. muscles shrink if you don’t
use them) **mostly permanent cells such as heart and muscle cells
Hypertrophy - cells grow bigger when they’re working harder (e.g. muscle growth
from exercise). **mostly permanent cells such as heart and muscle cells
Hyperplasia - cells increase in number when needed (e.g. liver cells regenerate or increase breast growth during pregnancy). *mostly occurring in labile cells sometimes stable
Metaplasia - cells change type when exposed to irritation (e.g. lung cells change due
to smoking).
Dysplasia - cells grow abnormally, which can be a warning sign for cancer.
Types of stress --> increased workload, hormonal changes, altered pH or nutrition, exposure to chemicals and inflammation
Cell injury --> cells can repair or regenerate through mechanisms such as resolution, regeneration, or replication
Cell adaptation mechanisms (listed above)
Cell types (cells are categorised based on their replication ability)
Labile cells - constantly replicating (e.g. skin cells).
Stable cells - replicate when needed (e.g. liver cells).
Permanent cells - cannot replicate (e.g. neurons, heart cells)
Adaptation example --> atrophy after being in a cast, high blood pressure causes hypertrophy of the heart muscle, hypoplasia results in growth of the prostate gland due to hormonal levels, metaplasia from smoking, abnormal growth in cervical tissue is dysplasia
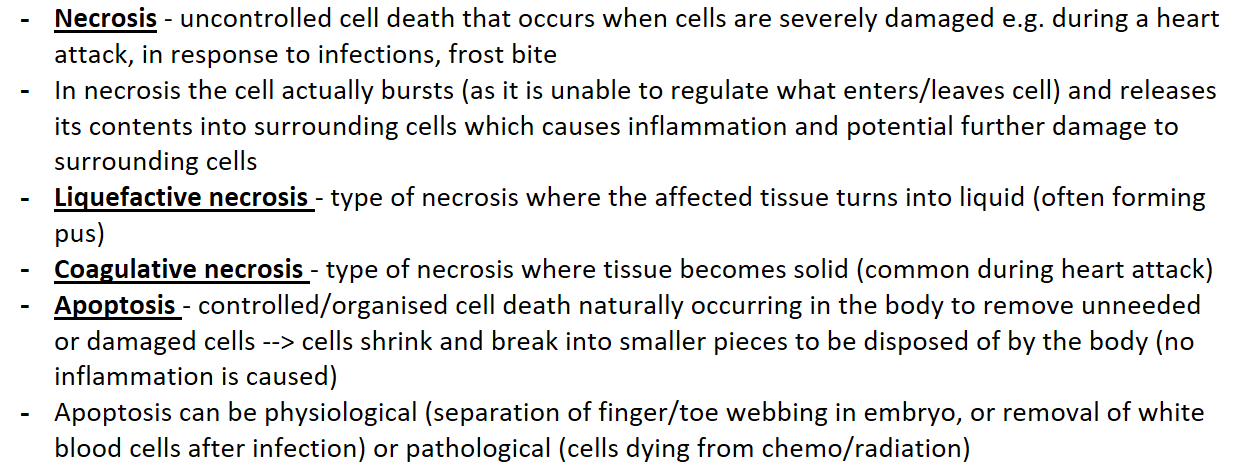
Necrosis - uncontrolled cell death that occurs when cells are severely damaged e.g. during a heart attack, in response to infections, frost bite
In necrosis the cell actually bursts (as it is unable to regulate what enters/leaves cell) and releases its contents into surrounding cells which causes inflammation and potential further damage to surrounding cells
Liquefactive necrosis - type of necrosis where the affected tissue turns into liquid (often forming pus)
Coagulative necrosis - type of necrosis where tissue becomes solid (common during heart attack)
Apoptosis - controlled/organised cell death naturally occurring in the body to remove unneeded or damaged cells --> cells shrink and break into smaller pieces to be disposed of by the body (no inflammation is caused)
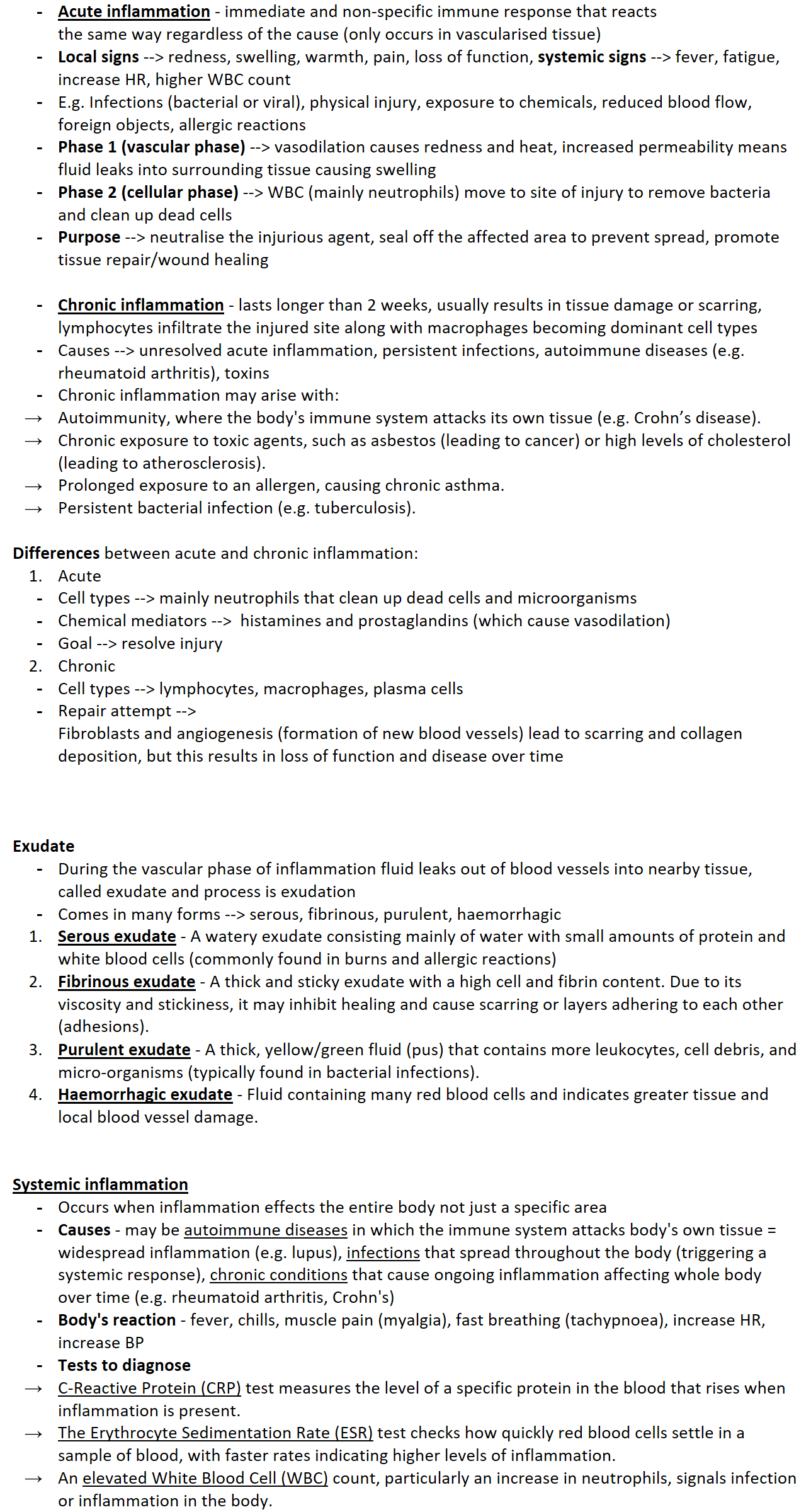
Apoptosis can be physiological (separation of finger/toe webbing in embryo, or removal of white blood cells after infection) or pathological (cells dying from chemo/radiation)Acute inflammation - immediate and non-specific immune response that reacts
the same way regardless of the cause (only occurs in vascularised tissue)
Local signs --> redness, swelling, warmth, pain, loss of function, systemic signs --> fever, fatigue, increase HR, higher WBC count
E.g. Infections (bacterial or viral), physical injury, exposure to chemicals, reduced blood flow, foreign objects, allergic reactions
Phase 1 (vascular phase) --> vasodilation causes redness and heat, increased permeability means fluid leaks into surrounding tissue causing swelling
Phase 2 (cellular phase) --> WBC (mainly neutrophils) move to site of injury to remove bacteria and clean up dead cells
Purpose --> neutralise the injurious agent, seal off the affected area to prevent spread, promote tissue repair/wound healing
Chronic inflammation - lasts longer than 2 weeks, usually results in tissue damage or scarring, lymphocytes infiltrate the injured site along with macrophages becoming dominant cell types
Causes --> unresolved acute inflammation, persistent infections, autoimmune diseases (e.g. rheumatoid arthritis), toxins
Chronic inflammation may arise with:
Autoimmunity, where the body's immune system attacks its own tissue (e.g. Crohn’s disease).
Chronic exposure to toxic agents, such as asbestos (leading to cancer) or high levels of cholesterol (leading to atherosclerosis).
Prolonged exposure to an allergen, causing chronic asthma.
Persistent bacterial infection (e.g. tuberculosis).
Differences between acute and chronic inflammation:
Acute
Cell types --> mainly neutrophils that clean up dead cells and microorganisms
Chemical mediators --> histamines and prostaglandins (which cause vasodilation)
Goal --> resolve injury
Chronic
Cell types --> lymphocytes, macrophages, plasma cells
Repair attempt -->
Fibroblasts and angiogenesis (formation of new blood vessels) lead to scarring and collagen deposition, but this results in loss of function and disease over time
Exudate
During the vascular phase of inflammation fluid leaks out of blood vessels into nearby tissue, called exudate and process is exudation
Comes in many forms --> serous, fibrinous, purulent, haemorrhagic
Serous exudate - A watery exudate consisting mainly of water with small amounts of protein and white blood cells (commonly found in burns and allergic reactions)
Fibrinous exudate - A thick and sticky exudate with a high cell and fibrin content. Due to its viscosity and stickiness, it may inhibit healing and cause scarring or layers adhering to each other (adhesions).
Purulent exudate - A thick, yellow/green fluid (pus) that contains more leukocytes, cell debris, and micro-organisms (typically found in bacterial infections).
Haemorrhagic exudate - Fluid containing many red blood cells and indicates greater tissue and local blood vessel damage.
Systemic inflammation
Occurs when inflammation effects the entire body not just a specific area
Causes - may be autoimmune diseases in which the immune system attacks body's own tissue = widespread inflammation (e.g. lupus), infections that spread throughout the body (triggering a systemic response), chronic conditions that cause ongoing inflammation affecting whole body over time (e.g. rheumatoid arthritis, Crohn's)
Body's reaction - fever, chills, muscle pain (myalgia), fast breathing (tachypnoea), increase HR, increase BP
Tests to diagnose
C-Reactive Protein (CRP) test measures the level of a specific protein in the blood that rises when inflammation is present.
The Erythrocyte Sedimentation Rate (ESR) test checks how quickly red blood cells settle in a sample of blood, with faster rates indicating higher levels of inflammation.
An elevated White Blood Cell (WBC) count, particularly an increase in neutrophils, signals infection or inflammation in the body.
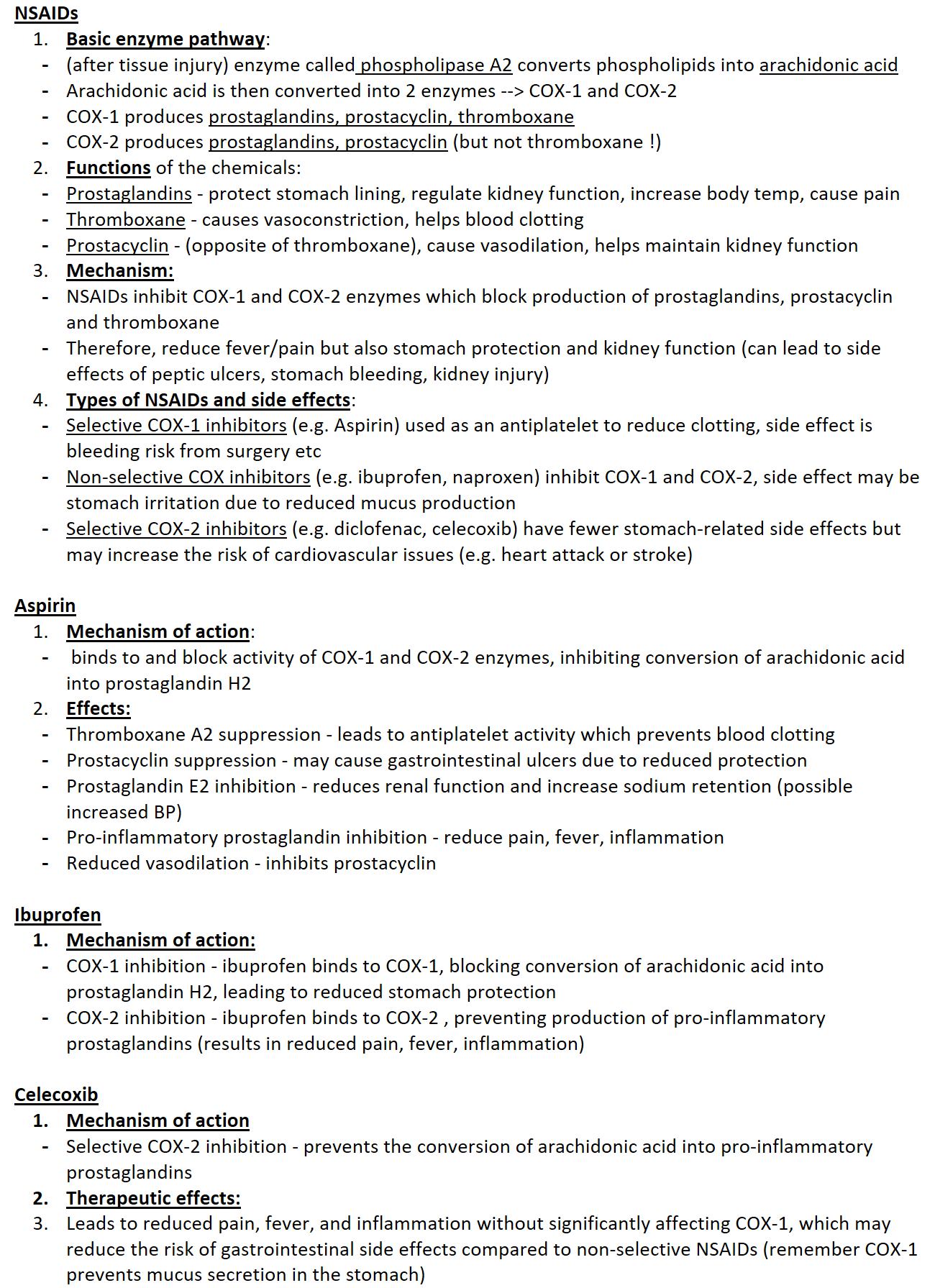
NSAIDs
Basic enzyme pathway:
(after tissue injury) enzyme called phospholipase A2 converts phospholipids into arachidonic acid
Arachidonic acid is then converted into 2 enzymes --> COX-1 and COX-2
COX-1 produces prostaglandins, prostacyclin, thromboxane
COX-2 produces prostaglandins, prostacyclin (but not thromboxane !)
Functions of the chemicals:
Prostaglandins - protect stomach lining, regulate kidney function, increase body temp, cause pain
Thromboxane - causes vasoconstriction, helps blood clotting
Prostacyclin - (opposite of thromboxane), cause vasodilation, helps maintain kidney function
Mechanism:
NSAIDs inhibit COX-1 and COX-2 enzymes which block production of prostaglandins, prostacyclin and thromboxane
Therefore, reduce fever/pain but also stomach protection and kidney function (can lead to side effects of peptic ulcers, stomach bleeding, kidney injury)
Types of NSAIDs and side effects:
Selective COX-1 inhibitors (e.g. Aspirin) used as an antiplatelet to reduce clotting, side effect is bleeding risk from surgery etc
Non-selective COX inhibitors (e.g. ibuprofen, naproxen) inhibit COX-1 and COX-2, side effect may be stomach irritation due to reduced mucus production
Selective COX-2 inhibitors (e.g. diclofenac, celecoxib) have fewer stomach-related side effects but may increase the risk of cardiovascular issues (e.g. heart attack or stroke)
Aspirin
Mechanism of action:
binds to and block activity of COX-1 and COX-2 enzymes, inhibiting conversion of arachidonic acid into prostaglandin H2
Effects:
Thromboxane A2 suppression - leads to antiplatelet activity which prevents blood clotting
Prostacyclin suppression - may cause gastrointestinal ulcers due to reduced protection
Prostaglandin E2 inhibition - reduces renal function and increase sodium retention (possible increased BP)
Pro-inflammatory prostaglandin inhibition - reduce pain, fever, inflammation
Reduced vasodilation - inhibits prostacyclin
Ibuprofen
Mechanism of action:
COX-1 inhibition - ibuprofen binds to COX-1, blocking conversion of arachidonic acid into prostaglandin H2, leading to reduced stomach protection
COX-2 inhibition - ibuprofen binds to COX-2 , preventing production of pro-inflammatory prostaglandins (results in reduced pain, fever, inflammation)
Celecoxib
Mechanism of action
Selective COX-2 inhibition - prevents the conversion of arachidonic acid into pro-inflammatory prostaglandins
Therapeutic effects:
Leads to reduced pain, fever, and inflammation without significantly affecting COX-1, which may reduce the risk of gastrointestinal side effects compared to non-selective NSAIDs (remember COX-1 prevents mucus secretion in the stomach)
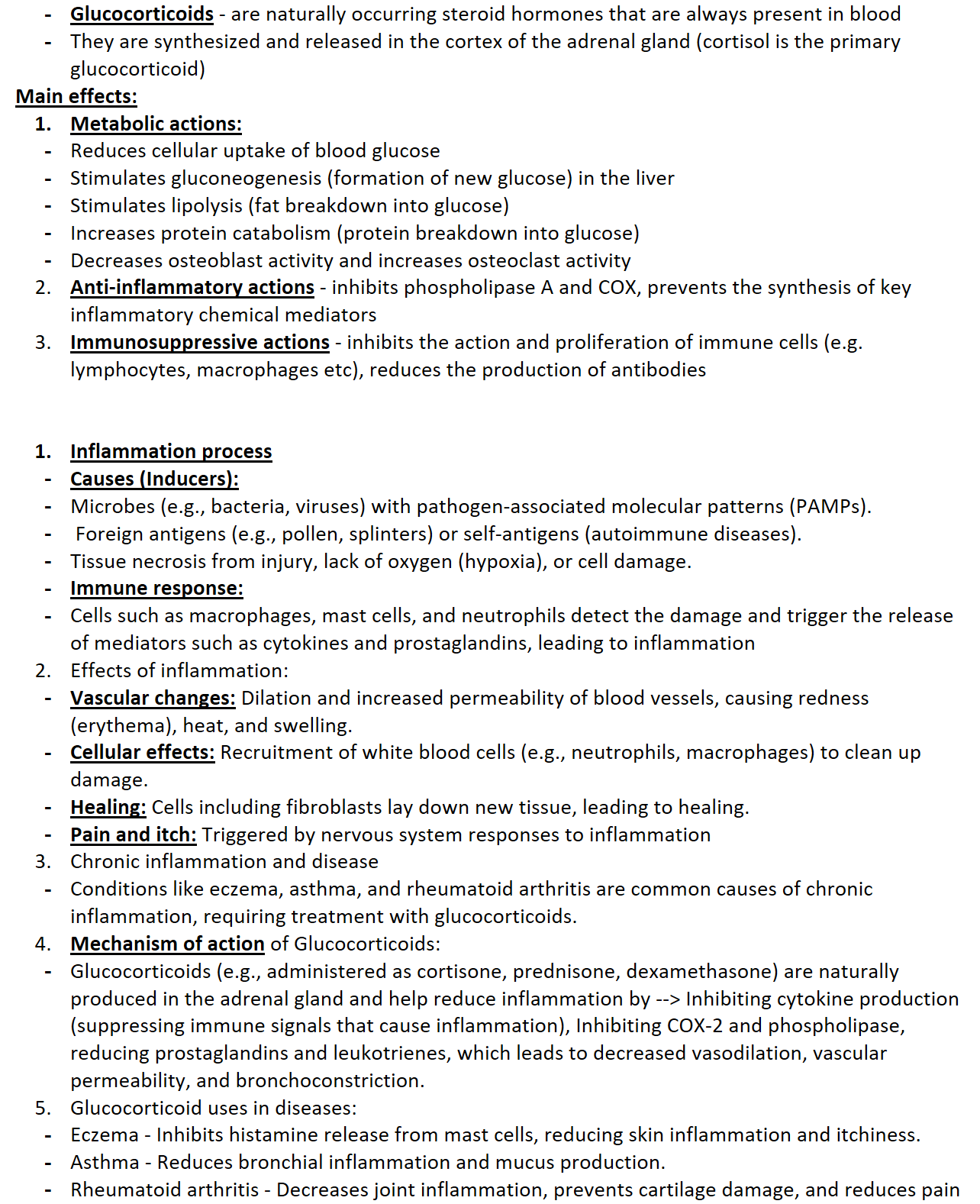
Glucocorticoids - are naturally occurring steroid hormones that are always present in blood
They are synthesized and released in the cortex of the adrenal gland (cortisol is the primary glucocorticoid)
Main effects:
Metabolic actions:
Reduces cellular uptake of blood glucose
Stimulates gluconeogenesis (formation of new glucose) in the liver
Stimulates lipolysis (fat breakdown into glucose)
Increases protein catabolism (protein breakdown into glucose)
Decreases osteoblast activity and increases osteoclast activity
Anti-inflammatory actions - inhibits phospholipase A and COX, prevents the synthesis of key inflammatory chemical mediators
Immunosuppressive actions - inhibits the action and proliferation of immune cells (e.g. lymphocytes, macrophages etc), reduces the production of antibodies
Inflammation process
Causes (Inducers):
Microbes (e.g., bacteria, viruses) with pathogen-associated molecular patterns (PAMPs).
Foreign antigens (e.g., pollen, splinters) or self-antigens (autoimmune diseases).
Tissue necrosis from injury, lack of oxygen (hypoxia), or cell damage.
Immune response:
Cells such as macrophages, mast cells, and neutrophils detect the damage and trigger the release of mediators such as cytokines and prostaglandins, leading to inflammation
Effects of inflammation:
Vascular changes: Dilation and increased permeability of blood vessels, causing redness (erythema), heat, and swelling.
Cellular effects: Recruitment of white blood cells (e.g., neutrophils, macrophages) to clean up damage.
Healing: Cells including fibroblasts lay down new tissue, leading to healing.
Pain and itch: Triggered by nervous system responses to inflammation
Chronic inflammation and disease
Conditions like eczema, asthma, and rheumatoid arthritis are common causes of chronic inflammation, requiring treatment with glucocorticoids.
Mechanism of action of Glucocorticoids:
Glucocorticoids (e.g., administered as cortisone, prednisone, dexamethasone) are naturally produced in the adrenal gland and help reduce inflammation by --> Inhibiting cytokine production (suppressing immune signals that cause inflammation), Inhibiting COX-2 and phospholipase, reducing prostaglandins and leukotrienes, which leads to decreased vasodilation, vascular permeability, and bronchoconstriction.
Glucocorticoid uses in diseases:
Eczema - Inhibits histamine release from mast cells, reducing skin inflammation and itchiness.
Asthma - Reduces bronchial inflammation and mucus production.
Rheumatoid arthritis - Decreases joint inflammation, prevents cartilage damage, and reduces pain
Topic 1.4: Wound healing
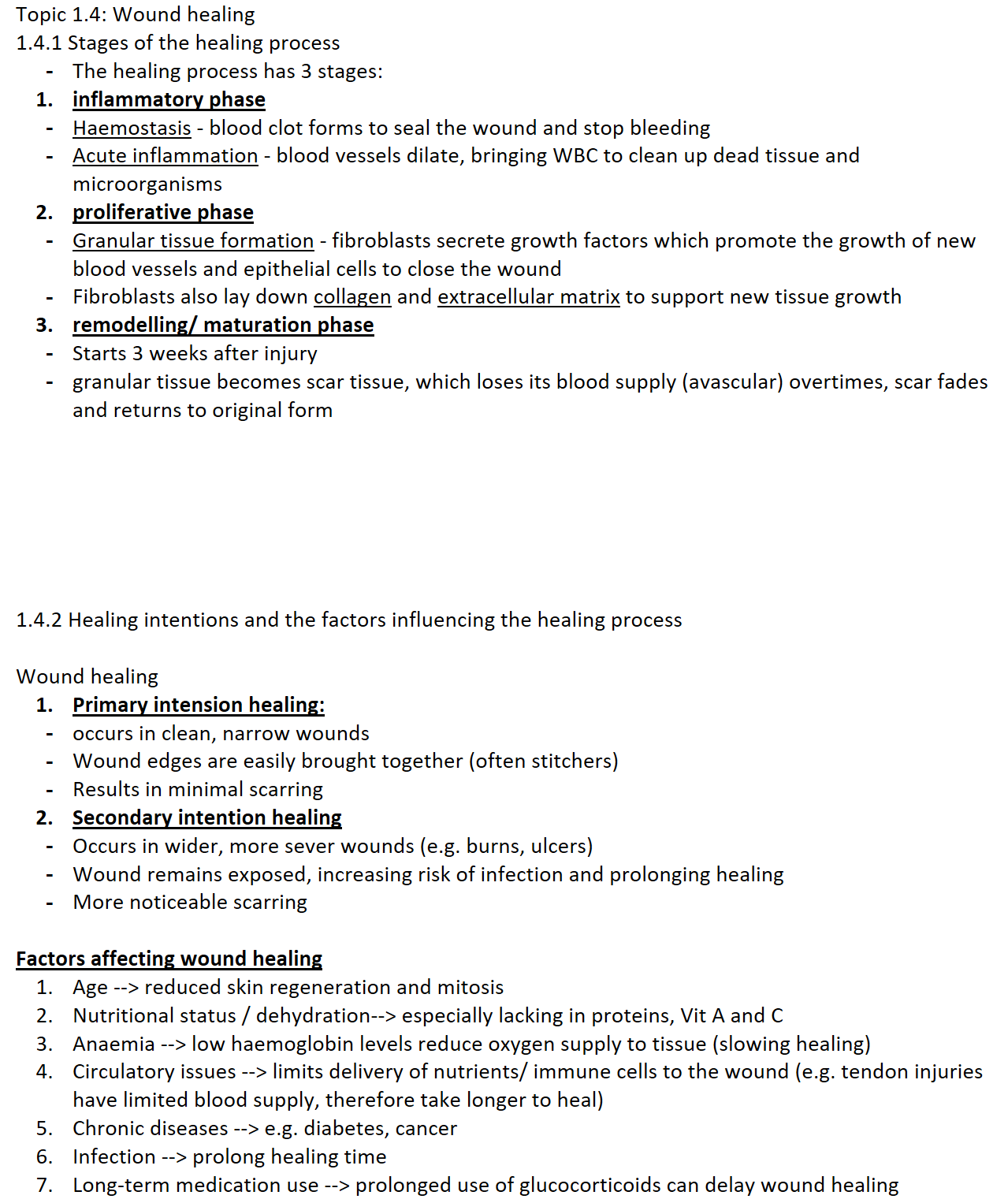
1.4.1 Stages of the healing process
The healing process has 3 stages:
inflammatory phase
Haemostasis - blood clot forms to seal the wound and stop bleeding
Acute inflammation - blood vessels dilate, bringing WBC to clean up dead tissue and microorganisms
proliferative phase
Granular tissue formation - fibroblasts secrete growth factors which promote the growth of new blood vessels and epithelial cells to close the wound
Fibroblasts also lay down collagen and extracellular matrix to support new tissue growth
remodelling/ maturation phase
Starts 3 weeks after injury
granular tissue becomes scar tissue, which loses its blood supply (avascular) overtimes, scar fades and returns to original form
1.4.2 Healing intentions and the factors influencing the healing process
Wound healing
Primary intension healing:
occurs in clean, narrow wounds
Wound edges are easily brought together (often stitchers)
Results in minimal scarring
Secondary intention healing
Occurs in wider, more sever wounds (e.g. burns, ulcers)
Wound remains exposed, increasing risk of infection and prolonging healing
More noticeable scarring
Factors affecting wound healing
Age --> reduced skin regeneration and mitosis
Nutritional status / dehydration--> especially lacking in proteins, Vit A and C
Anaemia --> low haemoglobin levels reduce oxygen supply to tissue (slowing healing)
Circulatory issues --> limits delivery of nutrients/ immune cells to the wound (e.g. tendon injuries have limited blood supply, therefore take longer to heal)
Chronic diseases --> e.g. diabetes, cancer
Infection --> prolong healing time
Long-term medication use --> prolonged use of glucocorticoids can delay wound healing