Lung Pathology
Pulmonary Infections
Pneumonia - infection and inflammation in the lung parenchyma
Bronchitis – inflammation in the bronchi
Factors predisposing to pulmonary infections:
General weakening of the organism
Chronic diseases
Immunosuppression / immunodeficiency
Hypoproteinemia
Leukopenia
Decreased local protection
Diminished cough reflex: coma, anaesthesia, chest pain
Decreased phagocytic and bactericidal activity of pulmonary macrophages: Alcohol, Smoking, High or low oxygen concentration
Damage of mucociliary clearance
Smoking
Inhalation of hot or corrosive gases
Viral infections - ARVI!!
Immotile cilia syndrome
Pulmonary blood congestion and oedema
Congestion of sections
Cystic fibrosis
Bronchial obstruction
Classification of pneumonias
By etiologic agent
By the clinical setting: pneumonia syndromes
Community – acquired acute pneumonia
Community – acquired atypical pneumonia
Hospital – acquired pneumonia
Aspiration pneumonia
Chronic focal inflammation
Necrotising pneumonia and lung abscess
Pneumonia in the immunocompromised host
By anatomic distribution:
Lobar: Lobar pneumonia s. pleuropneumonia
Stages of Lobar pneumonia
Congestion
Red hepatisation: 2-3 days, fibrinous pleuritis
Grey hepatisation: several days
Resorption: 8th – 9th day, in pre-antibiotic era, resolution by crisis
Lobular: Lobular bronchopneumonia
Focus/ foci 3 - 4 cm
Acute purulent inflammation in the bronchi and alveoli
By clinical manifestations:
Classic
Atypical
Complications of pneumonia
Abscess
Purulent inflammation in the pleura
Purulent inflammation in the pleura
Bacteraemia
Metastatic abscesses in distant organs
Sepsis
Septic shock
Fibrosis
Sepsis
SIRS – systemic inflammatory reaction syndrome
Sepsis: SIRS + proved or possible infection
Severe sepsis: dysfunction of distant organs
Septic shock: sepsis + arterial hypotension + no reaction to fluid infusion
Obstructive lung diseases
Decreased air flow in the airways
Includes:
Chronic bronchitis
Lung emphysema
Chronic bronchitis + lung emphysema = COPD
Bronchectasis
Bronchial asthma
Bronchectasis
Permanent dilation of bronchi and bronchioles: Saccular, Cylindrical
Destruction of muscle and elastic tissue
Mechanisms:
Obstruction, e.g. by mucus in cystic fibrosis
Infections
Morphology:
Preferred location: lower lobes
Intense acute and chronic inflammation
Ulcers
Metaplasia
Fibrosis of bronchial walls and peribronchiolar tissues: subtotal or total bronchiolar obliteration
Clinical Course:
Severe, persistent cough
Triggered by change of body position
More severe in the morning
High amount of foul-smelling sputum
Sputum can be bloody
Life- threatening haemoptysis is occasionally possible
Later: respiratory insufficiency, amyloidosis etc.
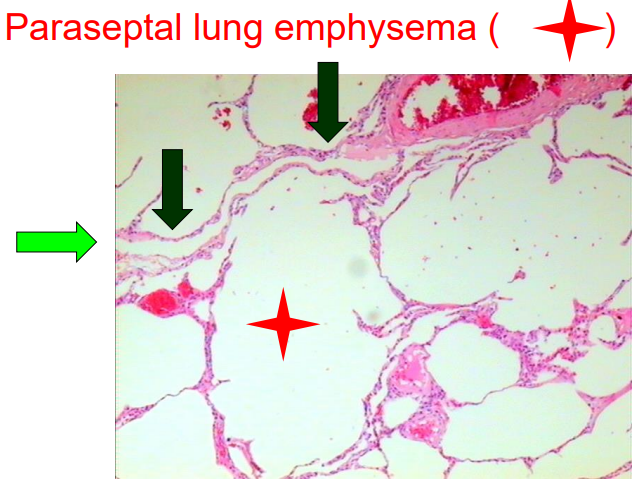
Emphysema = destruction of alveolar walls
Lung Emphysema
Causes: Smoking, alpha 1 antitrypsin deficiency
Pathogenesis:
imbalance between proteases and antiproteases
Neu, mf // alpha-1-antitrypsin
imbalance between oxidants and antioxidants
ROS (Neu, smoking) // superoxide dismutase, glutathione
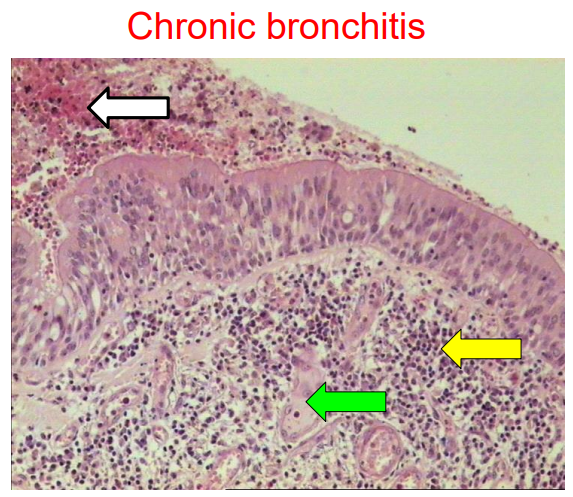
Chronic bronchitis = inflammation and hypersecretion in the bronchial walls
Chronic Bronchitis
Persistent cough with sputum production for at least 3 months in at least 2 consecutive years
Etiology:
Long-standing irritation by inhaled substances
Tobacco smoke
Dust (grain, cotton, silica)
Infections have secondary role:
Maintain chronic bronchitis
Responsible for exacerbations and +/- complications
Morphology
Mucus hypersecretion: Hypertrophy of submucosal glands Reid index exceed 0.4 Increase in goblet cell number
Inflammation: Hyperemia, swelling, oedema of bronhial mucous membranes Inflammatory infiltrate
Epithelial changes: metaplasia, dysplasia
Fibrosis, bronchial deformities
Bronchial obstruction
Complications of chronic bronchitis:
COPD
Respiratory failure
Pulmonary hypertension, cor pulmonale and heart failure
Metaplasia – dysplasia – cancer cascade
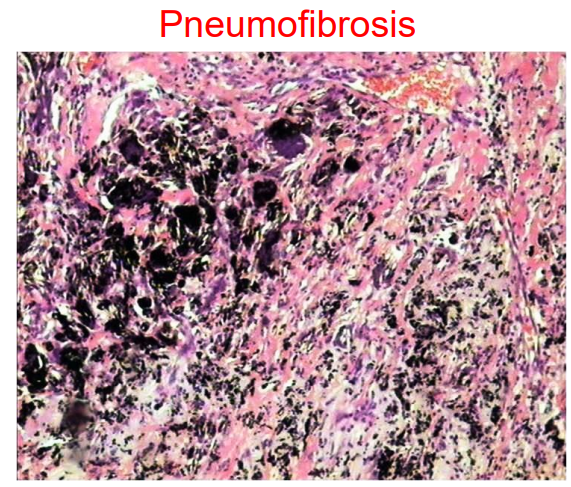
Restrictive lung diseases
Reduced expansion of lung parenchyma
Causes:
Chest wall disorders
Chronic interstitial and infiltrative lung diseases decreasing lung compliance and contribution to the loss of parenchyma
Pneumo-fibrosis
Interstitial lung disease: alveolitis
Pneumo-conioses
Alveolitis: chronic course with deformation of pulmonary architecture
Granulomatous lung diseases
Tuberculosis
Sarcoidosis
Exogenic allergic alveolitis
Foreign body granulomas
Sarcoidosis
Systemic disease of unknown etiology
The most frequent involvement:
Lymph nodes: bilateral hilar lymphadenopathy
Lungs
Other affected sites: skin, eyes, heart

Exogenous allergic alveolitis s. hypersensitivity pneumonitis
Immunologically mediated, mostly interstitial inflammatory reaction to prolonged exposure to inhaled organic antigens
Morphology:
Interstitial inflammation s. interstitial pneumonitis (ly, pc, mf)
Non-caseating granulomas
Interstitial fibrosis can develop
Foreign body granulomas
Occupational lung diseases
Pneumoconioses: restrictive pathologies
Asbestosis
Silicosis
Anthracosis
Berilliosis
Hard metal pneumoconiosis
Occupational bronchial asthma: obstructive lung disease
Vascular lung diseases
Vascular lung diseases
Lung oedema
Pulmonary hypertension
Thrombembolism
Pulmonary Oedema
Classification
By localisation:
Interstitial
Alveolar
By cause and pathogenesis:
Hemodynamic oedema; Causes: Increased hydrostatic pressure, Decreased oncotic pressure, Lymphatic obstruction
Oedema due to microvascular and alveolar injury; Causes: Infections: pneumonia, sepsis Inhaled gases: oxygen, SO2 Aspiration: gastric contents, near-drowning Drugs: bleomycin Shock Radiation
Oedema of undetermined origin; Causes: High altitude Neurogenic: central nervous system trauma
Non-cardiogenic lung oedema
Related terms:
diffuse alveolar damage (DAD),
acute respiratory distress syndrome (ARDS)
Basic pathogenetic event: damage of endothelium or pulmonary epithelium
ARDS / DAD: the pathogenetic events
Endothelial damage: increased capillary permeability, formation of microthrombi, ischemic injury
Alveolar cell death
Hyaline membranes
Decreased lung compliance
Ventilation – perfusion mismatch
Imbalance of anti-inflammatory and inflammatory mediators:
Nuclear factor kappa B
30 min.: IL-8
Pulmonary microvascular sequestration and activation of neutrophils
Problems associated with the underlying disease
Dyspnoea, tachypnoea
Hypoxemia, resistant to O2 inhalation
Respiratory failure
Diffuse bilateral infiltrates Mortality rate (USA) 60% - 40%
Secondary pulmonary hypertension
Chronic obstructive and interstitial lung diseases
Hypoxia
Destruction of lung parenchyma and capillaries
Congenital or acquired heart disease: mitral stenosis
Recurrent thrombemboli
Connective tissue diseases / vasculitis
Obstructive sleep apnoea
Primary pulmonary hypertension (PPH)
Primary changes in pulmonary blood vessel structure
Loss of BMPR2 (bone morphogenetic protein receptor 2) function
N: BMPR2 inhibits proliferation and favours apoptosis in vascular smooth muscle
PPH: Medial hypertrophy Plexiform lesions
Prognosis and treatment
Prognosis: death from decompensated cor pulmonale in 2-5 years: 80%
Limited treatment effect:
O2 , Calcium channel blockers, diuretics, digoxin
Specific treatment:
prostacyclin analogues,
endothelial receptor antagonists,
inhaled NO
Lung transplantation
Lung Cancer
Importance of the problem:
Frequent
Potentially preventable
5-year survival 10 – 15 – 18%
The etiological factors of lung cancer
Smoking
Passive smoking
Occupational factors
Chronic lung diseases: tuberculosis, alveolitis
Outdoor air pollution
Hereditary factors:
AR
AD
The pathogenesis of the main clinical symptoms of lung cancer
Systemic manifestations: Non – specific Weight loss Lack of appetite Fever Weakness
Local manifestations: Genesis [ central / peripheral cancer ] Cough, dyspnoea, lung bleeding, chest pain Pleural exudation
Mediastinal damage:
Metastatic manifestations
Paraneoplastic syndromes
WHO classification of lung cancer: the main groups
Squamous cancer
Small cell cancer
Adenocarcinoma
Large cell cancer
Sarcomatoid carcinoma
Carcinoid
Other type
TNM of Lung Cancer
Squamous cell cancer
Small cell cancer
Lung adenocarcinoma
Colloid cancer
Bronchioloalveolar carcinoma
Carcinoid tumour
Chondroid hamartoma
Types of metastatic spread within lungs
Immunohistochemistry in the diagnostics of lung cancer
To lazy to do notes for all these - go through variants 😬