Substance stuff
REVISIT W/D SX FOR DIFF SUBSTANCES AND TX AND CONSIDERATIONS FOR SAME, CHECK SUPP VIDS*
GABA sensitive receptors, post synaptic - mediate phasic inhibition, caused by gaba in the synapse on receptors
GABA insensitive receptors, extra synaptic - mediate tonic inhibition, caused by incidental floating GABA and glia GABA
Monoamine hypothesis - 5HT, DP, and NE, low leads to dpn, no compelling evidence but we use it in practice.
Treatment of Opioid addiction
Gamma-Hydroxybutyrate (GHB) - one of the date rape drugs. mechanism of action of GHB is as an agonist at its own GHB receptors and at GABAB receptors. Treats narcolepsy by improving sleep during sleep hours
When taken chronically, opioids readily cause both tolerance and dependence because adaptation of opioid receptors occurs quite readily. This adaptation hypothetically correlates with the migration of behavioral control from ventral circuits to dorsal habit circuits.
w/d sx: irritable, and having signs of autonomic hyperactivity such as tachycardia, tremor, and sweating. Pilo-erection (“goose-bumps”)
Methadone is a full agonist at μ-opioid receptors and can suppress withdrawal symptoms completely given orally and usually administered daily at a clinic. does not cause high.
Buprenorphine is a μ-opioid partial agonist that has less powerful agonist effects, yet can suppress withdrawal symptoms especially when mild withdrawal has already begun after stopping abused opioids. sublingual. can be implantable 6 month or 1 month injection
The injection of the combination of buprenorphine and naloxone results in no high and may even precipitate withdrawal, so prevents diversion for intravenous abuse of the sublingual preparation
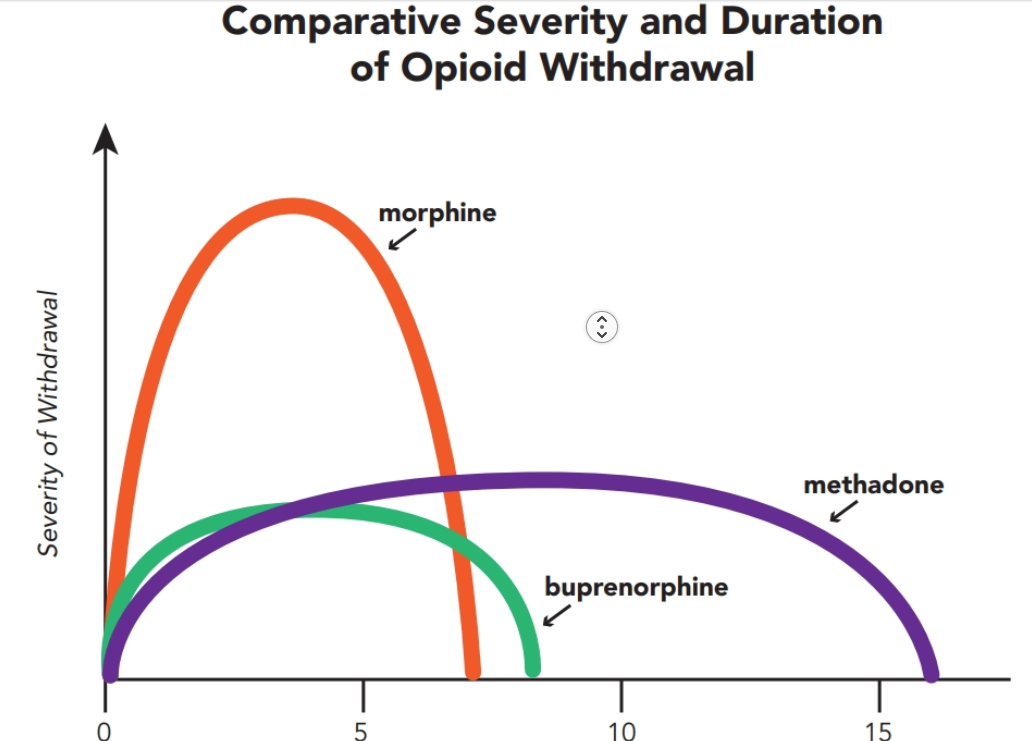
Both clonidine and lofexidine are α2-adrenergic agonists that reduce signs of autonomic hyperactivity during withdrawal and aid in the detoxification process. Can reduce severity NOT duration of bup and methadone w/d
Naltrexone opioid antag can be injected in the SHORT term to reduce w/d DURATION of meth/bup detox. In the long term especially if 30 day injections means can’t stop taking pills to relapse bc you’re being blocked.
best executed in a controlled clinical setting w/ aid and random urine drug tests
Article: Because of the rapid increase in opioid overdose, injectable Naltrexone is utilized to prevent death.
The recommended dose of extended-release injectable naltrexone is 380 mg, delivered intramuscularly approximately every 30 days, alternating buttocks for each subsequent injection.
Article/question: Benzos and methadone produce sedative effects that are heightened and made more severe when both drugs are used simultaneously (increased opioid effect)
ALCOHOL
an overly simplified view of alcohol’s mechanism of action is that it enhances inhibition at GABA (γ-aminobutyric acid) synapses and reduces excitation at glutamate synapses
Alcohol actions at GABA synapses hypothetically enhance GABA release via blocking presynaptic GABAB receptors and also by positively allosterically modulating postsynaptic GABA receptors
Alcohol also hypothetically acts at presynaptic metabotropic glutamate receptors (mGluRs) and presynaptic voltage-sensitive calcium channels (VSCCs) to inhibit glutamate release. possible disrupt action at post-synaptic NMDA receptors for glutamate
The net result of alcohol actions on opioid synapses is thought to be the release of dopamine in the nucleus acccumbens. Alcohol may do this by either directly acting upon μ-opioid receptors or by releasing endogenous opioids such as β-endorphin.
Wernicke encephalopathy may develop due to a thiamine deficiency associated with alcohol abuse
Treatment:
long term opioid antagonist, can’t feel the opioid high. injection better. naltrexone, nalmefene
Oral Naltrexone - Patients are ineligible for naltrexone if they have poor liver function or a history of liver disease, have recent prescribed or nonprescribed opioid use, and, for women, are pregnant or not using adequate birth control. Absolute contraindications to naltrexone use include acute hepatitis, liver failure, active opioid withdrawal, and the current use of methadone or opioid-containing medications prescribed to manage pain and treat serious medical conditions, such as heart disease, severe arthritis, sickle cell anemia, and recurrent congestive heart failure
Extended-Release Injectable Naltrexone - medication is contraindicated in patients who have previously exhibited hypersensitivity to naltrexone, polylactide-co-glycolide, carboxymethylcellulose, or any other components of the diluent. potent opioid antag, same contra as oral version
Acamprosate is a derivative of the amino acid taurine and interacts with both the glutamate system to inhibit it, and with the GABA system to enhance it, a bit like a form of “artificial alcohol”. Has direct blocking actions on certain glutamate receptors, particularly mGluR receptors. Stopping drinking creates a state of glutamate overexcitement and even excitotoxicity as well as GABA deficiency. Acam makes that effects less intense.
Acamprosate is contraindicated in patients with severe renal impairment and requires a dose reduction for patients with moderate renal impairment. However, this medication may be particularly useful in patients with hepatic impairment and/or liver disease
Disulfiram is the classic drug for treating alcoholism. It is an irreversible inhibitor of the liver enzyme aldehyde dehydrogenase that normally metabolizes alcohol. When alcohol is ingested in the presence of disulfiram, alcohol’s metabolism is inhibited and the result is the build-up of toxic levels of acetaldehyde. This creates an aversive experience with flushing, nausea, vomiting, and hypotension, hopefully conditioning the patient to a negative rather than positive response to drinking. Compliance issues. not prescribed often today.
Disulfiram hepatitis is a very rare, sometimes fatal complication that particularly affects women. Patients with cardiovascular or cerebrovascular disease are excluded from treatment because hypotension can occur during a disulfiram–alcohol interaction. Disulfiram has been reported to cause fetal abnormalities, so pregnant women should not use it.
Psychosis is a possible side effect of Disulfiram and can worsen preexisting psychosis
Unapproved agents that may be effective in treating alcoholism include the anticonvulsant topiramate and the 5HT3 antagonist ondansetron
TIP 49 focuses on the best currently recognized clinical practices for the medical maintenance of patients with alcohol use disorders (AUDs), using the four medications (disulfiram, oral naltrexone, injectable naltrexone, and acamprosate)
combos: Disulfiram Combined With Acamprosate, Acamprosate Combined With Naltrexone
A major finding of the COMBINE study was that patients who received medical management with naltrexone or with behavioral intervention or the combination of both fared better on drinking outcomes than those on acamprosate.
CANNABIS
Upon release of these endocannabinoids into the synapse, they travel retrograde to presynaptic CB1 receptors and “talk back” to the presynaptic neuron where they can inhibit the release of the classic neurotransmitter
Both CB1 receptors and CB2 receptors are localized in brain, with CB1 receptors present in greater density. Both receptors bind both endocannabinoids, 2-AG with high efficacy and anandamide with low efficacy.
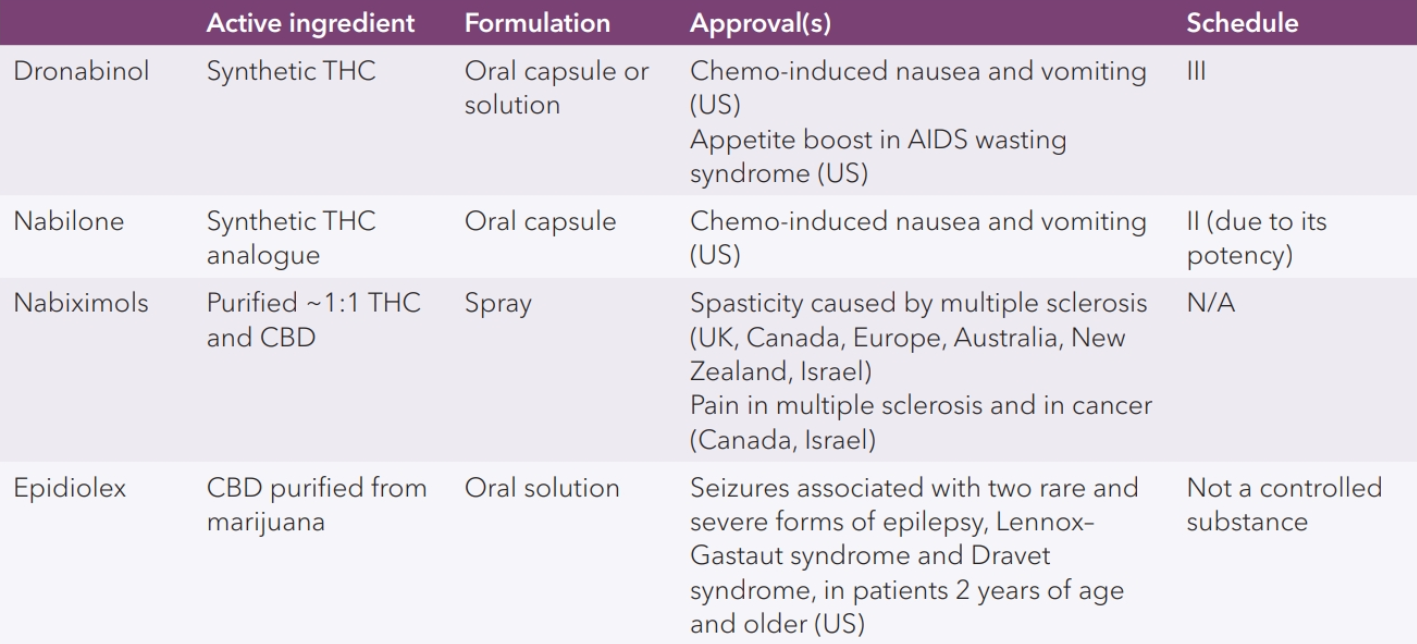
The most important of these are tetrahydrocannabinol (THC) and cannabidiol (CBD) (Figure 13-25). THC interacts with CB1 and CB2 receptors and has psychoactive properties
CBD does not have psychoactive properties and its mechanism of action is really unknown. relatively inactive and CB1-2
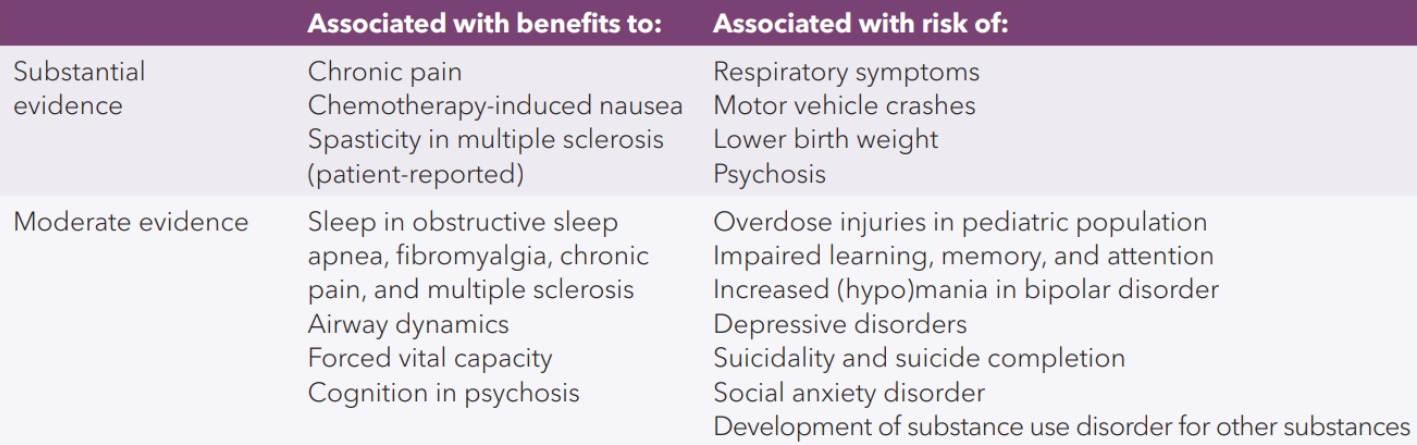
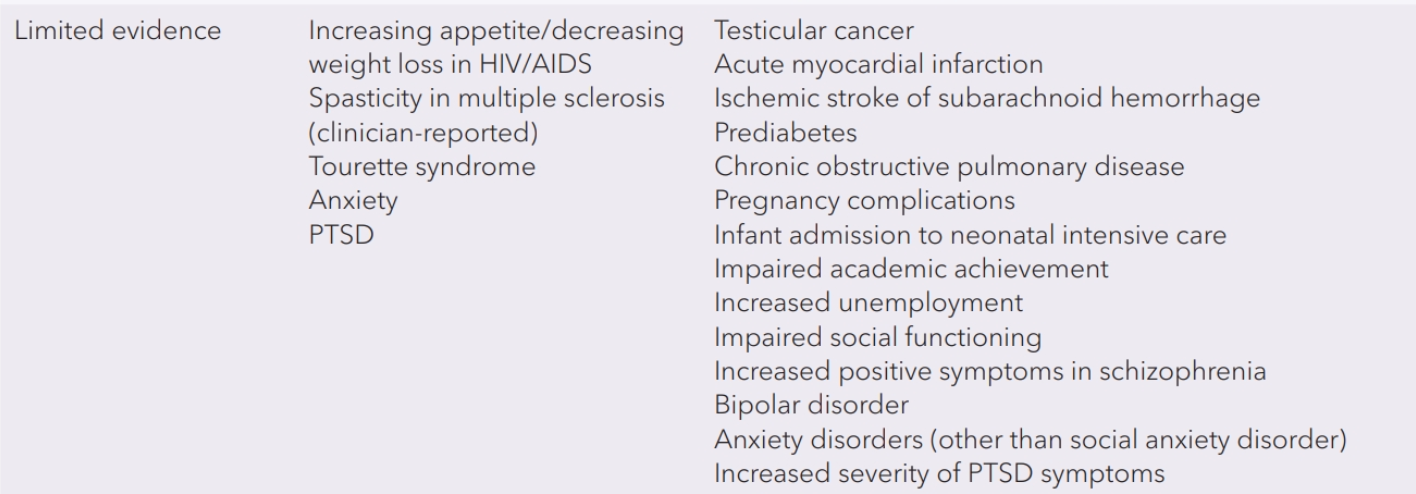
Over time, cannabis has become more potent in terms of more THC and less CBD, with resultant higher risk of hallucinations, delusions, anxiety, and memory impairment.Cannabis can also exacerbate psychosis in patients who already have a psychotic illness. Pure CBD has been studied for its potential use as an antipsychotic agent or anxiolytic
Addiction takes reward circuits from ventral to dorsal. Awarded for preparing to use rather than using itself. No associated activities don’t trigger dopamine. High concentration leads to PHASIC dopamine firing which is assoc w/ reward.
Faster entry into brain is stronger high bc you get a burst of DAT disruption. Smoking is a strong route bc massive surface area of lung, but any route that bypasses first pass metab is used.
Amphetamine, methamphetamine, and cocaine are all inhibitors of the DAT and the NET. Cocaine also inhibits the serotonin transporter (SERT).
Stim s/e has the excitatory expected memes, plus resp dpn. between stimulant doses, the individual experiences not only the absence of a high, but also withdrawal symptoms such as sleepiness and anhedonia
no approved drugs for stim addiction
burn out - over time depleted DA lvls and axonal degen
huffing, intox like effect, direct releasers of dopamine in the nucleus accumbens. can be deadly, arrest
NICOTINE

Cigarettes last long enough to desensitize nicotonic receptors. At the moment of resensitization, craving occurs, smokes again. About controlling craving as much as DA release.
One tx option is nicotine in non-smoked form. No dopamine high but desensitizes resensitized receptors to curb craving/withdrawal
nicotinic partial agonists (NPAs) - stabilize channel in a less freq opened state, not desensitized
norepinephrine–dopamine reuptake inhibitor (NDRI) - bupropion, helps boosts DA to east the lack of same
Quit rates for bupropion are about half that of the NPA varenicline. Quit rates for nicotine in alternative routes of administration such as transdermal patches are similar to those of bupropion
NPA varenicline triples or quadruples the 1-month, 6-month, and 1-year quit rates compared to placebo; the bad news is that this means only about 10% of smokers who have taken varenicline are still abstinent a year later
STROKE AND DRUGS
Stimulants inc blood pressure can cause stroke/hemorrhage. Stim vasoconstriction can cause ischemia.
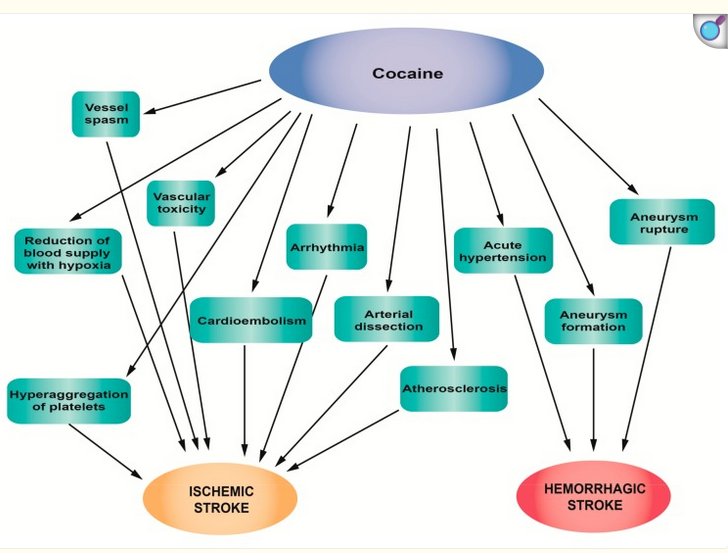
The main mechanism of action of cocaine is the blockage of noradrenaline reuptake. The side effect is increased norepinephrine release, also causes moderate release and blocking the reuptake of serotonin and dopamine. Stimulates the central nervous system, especially the limbic system where it potentiates dopaminergic transmission in the basal ventral nuclei, producing the sensation of pleasure, which has led to its widespread use
Cocaine use is associated with myocardial infarction, vasoconstriction, chronic uncontrolled hypertension, nervous system stimulation and stroke
Cocaine is associated with vascular toxicity. Various mechanisms are involved, such as hypertension, disturbance of platelet aggregation and homeostasis, effects on cerebral blood flow, and thromboembolism
Risk of stroke 2x as high in cocaine users. Stroke assoc w/ large and intracranial vessel atherosclerosis, increased platelet activation, bradyarrhythmias. Acute htn leading to hemorrhage.
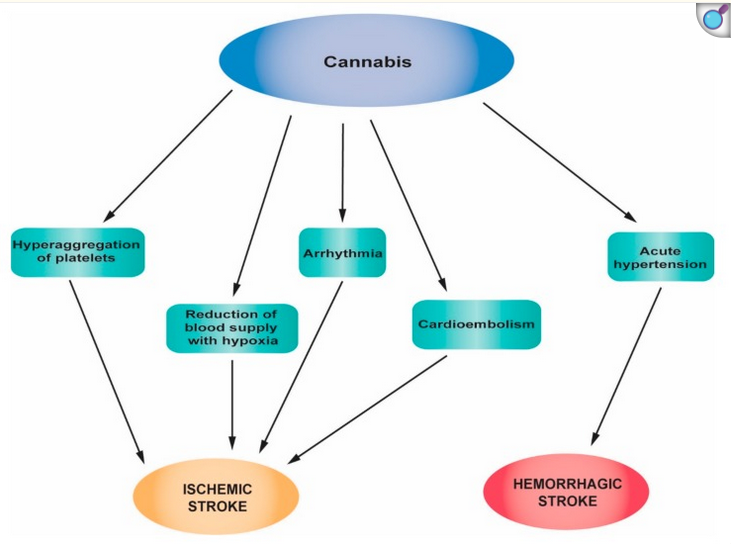
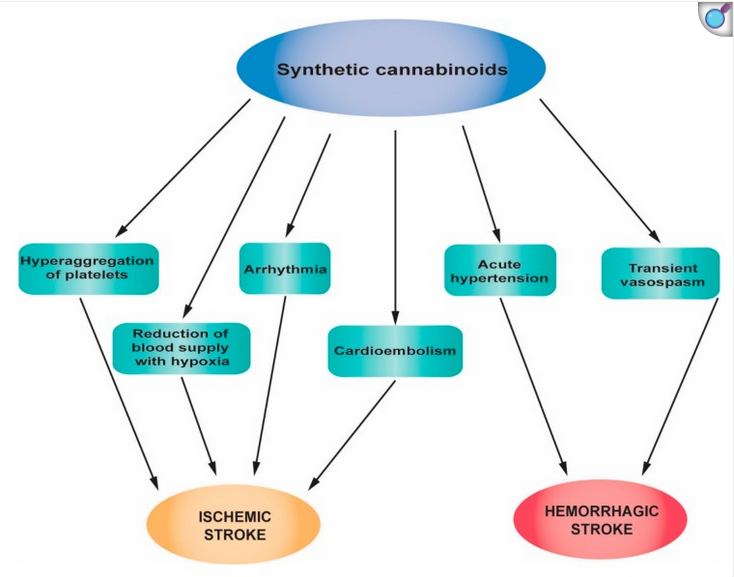
The possible mechanisms through which cannabis can induce stroke include cerebral vasoconstriction, hypotension, vasospasm, impaired cerebral vasomotor function and fluctuations in blood pressure
Stimulant abuse article:
This meta-analysis found that prescription psychostimulants likely promote sustained drug abstinence and may reduce stimulant use throughout trial and extend duration of abstinence when used in treatment of individuals with PSUDs. The overall effect is primarily influenced by studies that used prescription amphetamines, mostly dextroamphetamine, for treatment of individuals with cocaine use disorder. The present analysis offers preliminary evidence that medications with a more "potent" agonist effect (i.e., dextroamphetamine) are more effective than medications that are less "potent" (i.e., modafinil) and that patients treated with higher doses of agonist medications benefit more than patients treated with lower doses, further supporting the hypothesis that the "agonist effect" is mainly responsible for the clinical benefit
Article: SR-dexamphetamine reduces cocaine use and may improve clinically relevant health-related outcomes in patients with cocaine dependence who are participating in heroin-assisted treatment for their comorbid heroin dependence
Article: The most abused prescription drugs in the U.S. are painkillers, and this article reviews the need for an interdisciplinary approach to treating chronic pain.
The Functional Recovery Program utilizes a holistic treatment model that provides a structured setting, enabling patients to improve their functioning while better coping with their chronic pain.
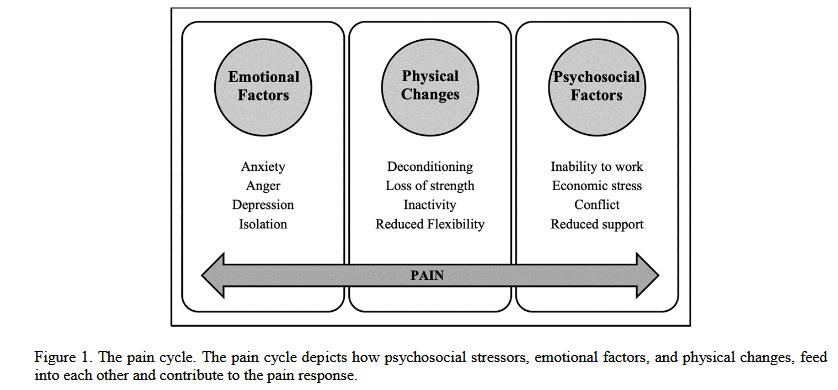
chronic pain responses like central sensitization, pain catastrophizing, and kinseophobia can lead to conditions one-tx biomechanical approaches can’t solve