Scrotum and Testes Ultrasound Tutorial Notes
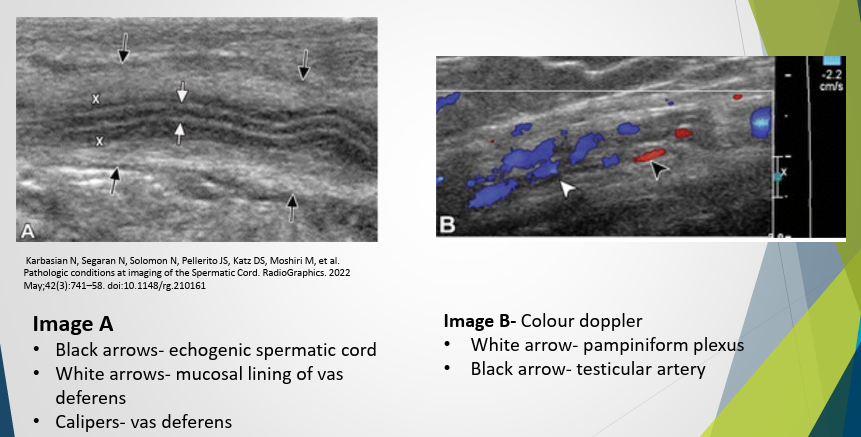
Ultrasound Appearance – Spermatic Cord
Common Indications for Scrotal/Testes Ultrasound
Pain (acute/chronic)
Associated with redness/swelling
Accompanied by fever
Associated with abnormal lie of testes
Trauma
Lump/mass
Swelling
Looking for undescended testes
Evaluate for infertility
Testes/Scrotal Ultrasound Procedure
Maintain professionalism and patient privacy.
Explain procedure and gain consent.
Allow patient to change and position supine on the bed.
Obtain full clinical history.
Use warm gel (to avoid cremasteric reflex, which can cause contraction, wrinkles, thickness and poor attenuation).
Elevate the scrotum with a towel underneath or resting on closed thighs.
Place penis on patient’s abdomen, held by gown or patient, and keep still.
Disinfect transducer post-procedure.
Leave patient to change in privacy with towels to clean off gel.
Ultrasound Images Required
High-frequency linear probe (be prepared to change frequency or to curved probe to obtain accurate length or demonstrate relationship of pathology to anatomy).
Image in transverse of both testes to document lie.
Image both testes in two planes:
Transverse (upper/mid/lower)
Longitudinal (med/mid/lat)
Measurements taken in long and trans, generate volume (LxHxW).
Assess epididymis in entirety with images of head/body/tail.
Evaluate and image spermatic cord
Assess testes and epididymis with color Doppler and PW Doppler trace to assess blood flow.
Take a color image in trans of both testes at once for any flow discrepancy/torsion.
Take comparison view of right and left testes as beneficial.
Palpate, localize, and image any particular lump the patient can feel.
Document any pathology found in two planes including measurements and vascularity.
Perform the Valsalva manoeuvre when evaluating for varicoceles or hernias
Assess groin if necessary for lymphadenopathy.
Kidneys may be required in some workplaces, especially looking for a renal tumour causing compression of the renal vein if a varicocele is found.
Normal Testes Ultrasound Images
Testes oval, smooth, homogenous.
Usually vertical lie unless bell clapper deformity.
Surrounded by thin echogenic fibrous band representing visceral component of tunica vaginalis.
Normal volume between 12-19cc post-puberty, then decreases with age
Normal size approximately 3-5cm length, 2-3cm width and AP measurement
Normal Color Doppler Image
Assess for torsion.
Make sure low PRF and high color gain set first on asymptomatic side.
Also need a spectral Doppler trace of arterial and venous flow.
Flow must be intratesticular to rule out torsion.
Normal Epididymis
Moving transducer posterior and lateral allows assessment of body and tail of epididymis.
Ultrasound Normal Anatomy
Epididymal head
Epididymal body
Scrotal wall
Testicle
Mediastinum testis
Tunica albuginea
Vas deferens
Epididymis
Appendix epididymis
Appendix testis
Tunica albuginea
Skin
Parietal layer tunica vaginalis
Visceral layer of tunica vaginalis
Cremaster muscle
Normal Variant - Rete Testis
Tubular ectasia - dilated testicular mediastinal bubbles.
Multiple small cystic or tubular anechoic structures that replace and enlarge the testicular mediastinum.
No specific shape.
No mass effect.
No internal vascularity
Normal Variant - Mediastinum Testis
Supports the rete testis and testicular vessels as they enter and exit the testis.
Appears as a linear echogenic band at posterior part of testis on ultrasound
Normal Appendix Epididymis or Appendix Testis
A developmental remnant of the Mullerian duct on the upper pole of testis inside a groove between testis and epididymal head.
Best seen when there is a hydrocele.
Usually oval, isoechoic with testis and can have blood flow within.
Most Common Pathology
Extratesticular lump or swelling
Hydrocele (pyocele or haematocele)
Epididymitis/orchitis/epididymo-orchitis
Epididymal cysts
Varicocele in pampiniform plexus
Cryptorchidism (undescended testes)
Scrotal pearl (free floating calculus within tunica vaginalis)
Scrotal swelling with pain
Torsion
Infection/inflammation
Haemorrhage
Strangulated hernia
Intratesticular lumps
Germ cell tumor (most common)
Seminoma
Non-seminoma
Hydrocele
Two main types
Communicating: fluid collects around the patent processus vaginalis which communicates with the peritoneum
Spermatic cord hydrocele: can be encysted (no communication with peritoneum – spermatic cord cyst), or funicular (communicates with peritoneum at internal ring but doesn’t surround the testes)
Clinical Presentation
Painless scrotal swelling/mass or enlargement
Can become painful if infected (pyocele - complication of epididymo-orchitis, testicular abscess, trauma, or surgery)
Haematocele - usually from trauma to scrotum or surgery
Epididymal Cyst
Epididymitis and/or Epididymo-Orchitis
Clinical Presentation
Gradual onset swelling and pain
Very tender to touch
Can be caused by STD or UTI
Infection begins in bladder or prostate, spreads through ductus deferens and lymphatics of spermatic cord to epididymis
Infection begins at the tail then progresses to body/head/testis
Epididymo-orchitis less common initially
Ultrasound Appearance
Epididymis is increased in size
Epididymal tail most affected
Can get reactive hydrocele and scrotal wall thickening
Can have hypo/hyper or heterogeneous appearance depending on the time of the scan
Increased vascularity in epididymis or both testis and epididymis
Varicocele
Abnormal dilatation of the pampiniform plexus (>3mm)
Primary (majority) are from incompetent or absent valves in testicular vein
Left affected > Right.
Can be due to the left testicular vein being longer and inserting into the left renal vein at a right angle.
Right testicular vein is short and inserts into IVC, therefore less backpressure.
Secondary - from increased pressure in testicular vein from compression (lymphadenopathy, renal mass, renal vein compression in nutcracker syndrome)
Clinical Presentation
Can be asymptomatic
If symptomatic
Scrotal mass/swelling
Scrotal pain
Infertility
Ultrasound Appearance
Dilated veins >3mm with Valsalva within pampiniform plexus
Can also have dilated veins at epididymal head, laterally and inferiorly to testis
Treatment
Often no treatment or surgery to seal off the affected vein
If chronic pain can’t be managed
Testicular Trauma
Rupture
Fracture
Torsion
Intratesticular haematoma
Clinical Presentation
Can be from a blunt or penetrating injury or surgery
Pain/swelling
Ultrasound Appearance - Rupture
Can have haematocele
Disruption of tunica albuginea (echogenic line covering testes is irregular, not continuous or retracted
Ultrasound appearance infarct/ischemia
Heterogenous patchy testis
Can present similar to torsion, however, infarct is due to increase intra-testicular pressure, causing venous obstruction and infarction
Testicular Rupture
Disruption of tunica albuginea
Hypoechoic avascular area
Testicular Torsion
Three types
Intravaginal (most common) due to bell clapper deformity
Extravaginal – torsion at the level of the external ring
Long mesorchium – twist in the tissue overlying the vasculature anteriorly between the epididymis and tunica vaginalis
Torsion occurs when the testis torts on the spermatic cord cutting off the blood supply
Bell clapper Deformity
tunica vaginalis has abnormally high attachment to the spermatic cord, leaving the testis free to rotate.
Gives predisposition to intravaginal torsion
Clinical Presentation
Testicular torsion is usually spontaneous or in the setting of minor/incidental trauma.
The onset of severe testicular pain is sudden and is not relieved by the elevation of the scrotum.
There should be no fever or urethral discharge.
Sometimes may be intermittent symptoms due to spontaneous detorsion, so-called “intermittent testicular torsion”.
Often results in short periods of acute groin pain accompanied by vomiting and subsequent spontaneous relief may be a typical patient history in these cases.
Physical examination may reveal elevation of the affected testis, an absence of the cremasteric reflex, transverse lie of the testis, anterior rotation of epididymis, and pain relief with successful manual detorsion.
Cremasteric reflex
When the inner thigh is stroked, the cremaster muscle contracts and pulls up the ipsilateral testicle toward the inguinal canal
Ultrasound Appearance:
Compare symptomatic side to the normal side.
No blood flow or altered blood flow to testis - first to disappear is venous flow.
In complete torsion – there is no blood flow to testis or epididymis
‘Whirlpool Sign’ - twisting of the spermatic cord - refers to the mass with concentric layering just superior to the testis representing the “coiled spermatic cord components”.
This is typically visualized using a longitudinal and/or oblique transducer orientation to visualize the course of the spermatic cord
Acute Stages (<6-12 hours)
Increase in the size of the testis and epididymis (especially in acute stages)
Homogeneous echotexture (early finding, before necrosis)
Reactive thickening of the scrotal skin with hyperemia
Later stages (>24 hours)
Heterogeneous echotexture / hypoechoic regions represent necrosis / hyperechoic regions represent heamorrhage
Reactive hydrocele
DDX
It is important to realize that epididymo-orchitis can closely mimic the appearances of torsion as well as spontaneously detorted testis. Correlate clinically.
Treatment
Surgical exploration to assess the ‘twisting’ of the spermatic cord and to untwist it (de-torsion) to restore blood supply.
Time critical as >6 hrs – there will be permanent damage to the testicle.
Nearly most patients require testicle removed (orchidectomy) if surgery is delayed >12 hours.
Torsion treatment within 6 hours – high chance of salvaging testicle.
If the testicle has already infarct – then it needs to be removed because it increases the risk of infection and abscess formation if it is kept.
Surgeons often perform an ‘orchidopexy’ which is fixing the testicle by sutures, so it doesn’t twist in the future (in an attempt to minimize risk due to the bell-clapper deformity).
They often fix the other testis also so it doesn’t run into the same issue in the future.
Case Studies
Case 1
History
Enlarging left testis for 2 ½ months
70 y/o male
Description
Solid
Lobulated/irregular
Hypoechoic
Heterogenous with multiple echogenic foci
Increase in vascularity
Radiologist report
The left testis is almost completely occupied by a lobulated solid mass with some increased vascularity present.
Measures at least 3.4 x 2cm in diameter and appears suspicious for neoplasia.
The epididymis appeared normal.
The right testis, although having even echotexture without mass infiltration, shows a small peripheral calcific density of 1mm diameter. No further microcalcification seen.
Cursory examination of the inguinal regions and pre-aortic regions showed no evidence of lymphadenopathy.
As discussed a urological assessment and CT scan of the chest, abdomen, and pelvis should follow given this suspicious, probably primary germ cell tumour of the left testis.
Case 2
Pathology
Anechoic tubular structures located in the pampiniform plexus
Increase in vascularity and diameter with Valsalva
Radiologist Report
The testes are symmetric and normal in size
Homogenous echotexture and normal vascularity
No testicular mass
No hydrocele seen
There is a small left varicocele 3.2mm
There is no other scrotal pathology
Case 3
History
History of right testicular Ca with surgery.
For surveillance
Description
Anechoic fluid-filled structure
Well circumscribed
Round/oval
Posterior enhancement
Reverberation artefact
Diagnosis
Testis prosthesis
Case 4
History
Rt testicular pain and swelling 5 days
70 y/o male
Epididymis
Heterogenous tubular structure
Mix of hypoechoic and hyperechoic areas
Appears bulky
Increase in vascularity
Abnormal in appearance: epididymitis
Area Around the Epididymis and Testis
Predominantly Anechoic area surrounding epididymis and testis
Contains multiple echogenic septations
No flow
Diagnosis
Possible pyocele as a result of epididymo-orchitis