Sexual Differentiation and Disorders
Learning Objectives
Understand what is meant by sexual differentiation
Define the role of the Y chromosome in determining sexual differentiation
Outline the sequence of sexual differentiation
Explain the possible outcomes when sexual differentiation processes are disrupted
Describe some of the main disorders of sexual differentiation
Sexual Differentiation vs Sexual Determination
Determination: determination is a genetically controlled process that is dependent on the switch on the Y chromosome. This is the determination of male or female (commitment to the male or female pathway and switch on the gene on the Y chromosome).
Differentiation: the process by which internal and external genitalia develop as male or female (develop morphological characteristics). The two processes are contiguous (occur side by side) and consist of several stages.
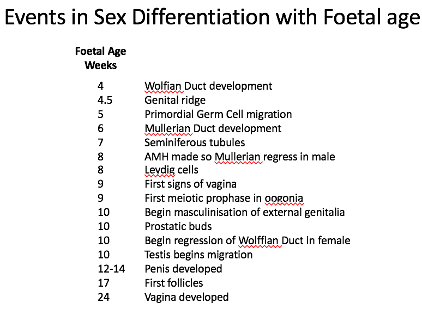
Sequence of Sexual Differentiation
Stages of Sexual Differentiation:
1) Genotypic sex (either XX or XY and there can be some variations).
2) Gonadal sex (either the ovaries or testes and the formation of these is contributive to the rest of the development).
3) Phenotypic sex (the shape and outward appearance of the genital region. These are usually the same as the gonadal sex but not always).
4) Legal sex (what is on your passport, birth certificate and are fixed; what you’re basically assigned at birth).
5) Gender identity (most important and is how you feel and what you identify as).
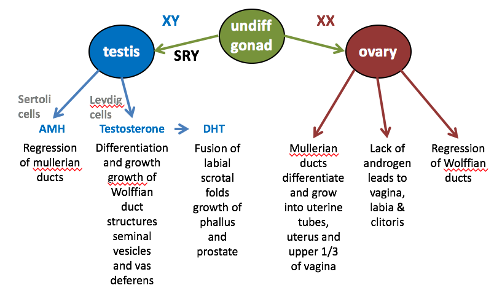
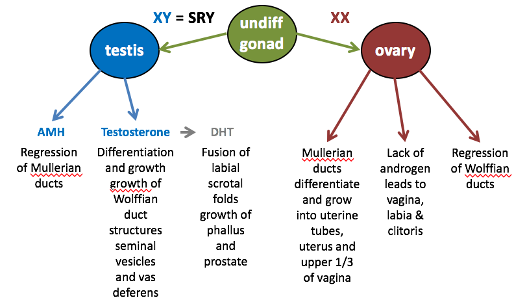
Gonadal Sex:
Y chromosome contains the SRY gene which is a transcription factor which has a positive feedback mechanism which causes the transcription of events linked to testes formation
SRY gene → creates the testis → produces AMH (from Sertoli) and testosterone (from Leydig)
Switched on during week 7 of embryo development
NO SRY → ovaries (even if a Y chromosome is present)
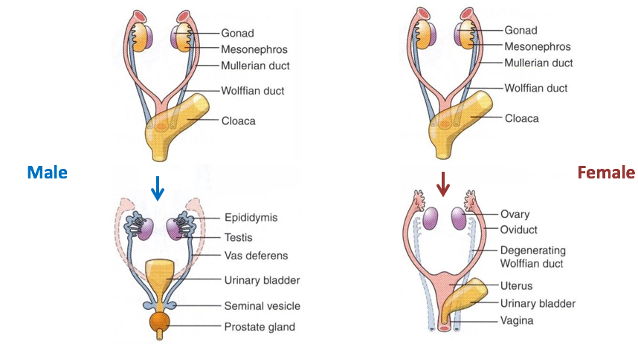
Gonadal Development:
After fertilisation, bipotential gonads develop from the genital ridge primordial which is on the posterior wall of the lower thoracic lumbar region
2 Sets of ducts:
Mullerian (F): develops into the uterus, uterine tubes and upper 1/3 of the vagina
Wolfian (M): developed into vas deferens, epididymis and prostate
Develop depending on which genes are triggered (SRY):
Primordial Germ Cells: Sperm or Oocytes
Migration: An initially small cluster of cells in the epithelium of the yolk sac expands by mitosis at around 3 weeks. They then migrate to the connective tissue of the hind gut, to the region of the developing kidney, and on to the genital ridge—this process is completed in 6 weeks.
Yolk Sac Epithelium → Hind Gut Connective Tissue → Developing Kidney → Genital Ridge
The cluster of cells develops from the yolk sac and colonises the genital regions. These could still be eggs or sperm at this point as they are all totipotent stem cells. Around 6 weeks, they are usually there.
Primitive Sex Cords: Sertoli (express SRY) or Granulosa (female expression)
In both males and females, there’s a layer of cells (germinal epithelium) covering a structure called the genital ridge. These cells migrate inward in organized groups called primitive sex cords.
In Males:
The cells moving inward activate a gene called SRY (found on the Y chromosome), by penetrating the medually mesenchyme and surrounding PGCs to form the testis cord .
This gene causes the cells to develop into Sertoli cells, which are important for supporting sperm development.
After becoming Sertoli cells, they produce a hormone called Anti-Müllerian Hormone (AMH), which prevents the development of female reproductive structures.
In Females:
The same germinal epithelial cells also migrate inward and condense in the cortex as small clusters around PGCs but do not express SRY (since females don’t have a Y chromosome).
Instead of Sertoli cells, these cells develop into Granulosa cells, which support egg development.
The lack of SRY and AMH production is the first key difference between male and female development.
Mesonephric Cells: Leydig (M) or Theca (F) - blood vessels and can produce androgens
Certain cells originate near the genital ridges in a structure called the mesonephric primordium.
These cells migrate and develop into important tissues and cell types using growth factors and transcription factors.
In Males:
Under the influence of pre-Sertoli cells, which express the SRY gene, these mesonephric cells form:
Vascular tissue (blood supply).
Leydig cells, which make testosterone but do not express SRY.
A basement membrane, which helps form the seminiferous tubules (where sperm develop) and the rete testis.
Sertoli cells produce AMH (Anti-Müllerian Hormone), which, together with testosterone from Leydig cells, supports the development of male reproductive structures.
In Females:
Without SRY, mesonephric cells instead form:
Vascular tissue.
Theca cells, which make androstenedione (later used by Granulosa cells to produce estrogen).
At this stage, females do not produce significant hormones like testosterone or AMH.

Internal Reproductive Organs:
Mullerian Ducts: (F) - inhibited by the AMH in males and regress due to testosterone
Wolfian Duct (M): testosterone and AMH stimulates progression and lack of testosterone stimulation means regression in females.
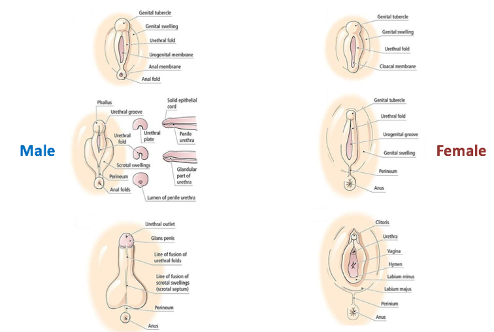
Testosterone Conversion:
In the genital skin, testosterone is converted to DHT under 5-alpha-reductase
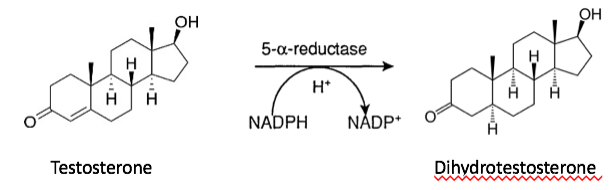
This conversion causes the differentiation of the male external genitalia:
The clitoral area enlarges into the penis
Labia fuse and become rugged to form scrotum
Prostate forms
In the female, if you have no 5-AR, you get no testosterone produced so you have the female being produced.
Disorders
- Gonadal dysgenesis - Sexual differentiation is incomplete. Usually missing SRY in male, or partial or complete deletion of second X in female. Also used as a general description of abnormal development of the gonads. (partially inactive SRY in male).
- Sex reversal - Phenotype does not match genotype, ie may be male genotypically but externally look like a female.
- Intersex - Have some components of both tracts or have ambiguous genitalia. Sex of infant difficult to determine.
Gonadal Dysgenesis:
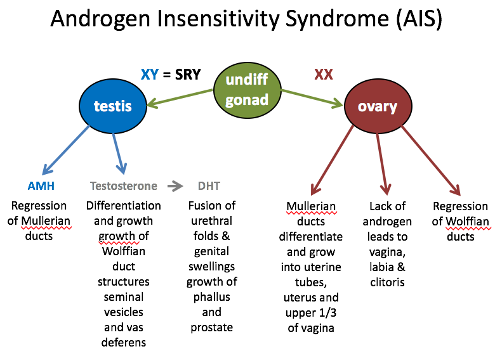
Scenario 1: Androgen Insensitivity Syndrome (AIS)
What happens?
In an XY individual, testosterone is produced, but the body cannot respond due to a mutation in the androgen receptor.
Testes are present, and AMH is produced, causing the Müllerian ducts (female structures) to regress.
However, Wolffian ducts (male structures) fail to develop because testosterone has no effect.
No male external genitalia form, so the individual appears female.
Types of AIS:
Complete AIS (CAIS):
Incidence: 1 in 20,000.
Individual appears fully female at birth and is typically assigned female.
Symptoms: Undescended testes, lack of menstruation (primary amenorrhea), minimal body hair.
Diagnosis: High androgen levels despite no response to them.
Partial AIS (PAIS):
Incidence: Unknown (spectrum of severity).
Presents with varied genital development, ranging from ambiguous genitalia to a larger clitoris.
Treatment: Surgery is now often delayed to allow for informed decisions later in life.
Scenario 2: 5-Alpha Reductase Deficiency
What happens?
In an XY individual, testosterone is made, but it cannot be converted into DHT (a more potent androgen) due to a deficiency in the 5-alpha reductase enzyme.
Internal male structures form (e.g., Wolffian ducts) since testosterone is effective.
External male genitalia do not develop, so the individual is typically assigned female at birth.
At puberty:
High testosterone levels can cause virilization (development of male traits), depending on the severity of the enzyme deficiency.
Scenario 3: Turner Syndrome (XO)
What happens?
Individual has one X chromosome instead of two (XO).
Müllerian ducts form, so they present with female genitalia.
Ovaries do not develop properly, forming streak ovaries (ovarian dysgenesis).
Symptoms:
Incidence: 1 in 3,000.
Short stature, underdeveloped reproductive structures, other growth/development issues.
May be fertile in cases of mosaicism (some cells with XX chromosomes).
Require hormone therapy for bone health and reproductive organ support.
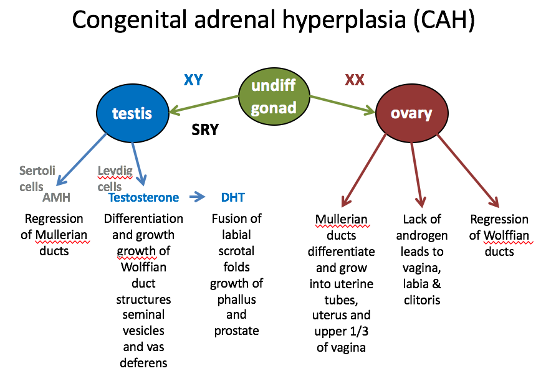
Scenario 4: Congenital Adrenal Hyperplasia (CAH)
What happens?
In an XX individual, high androgen levels are produced in utero due to a block in the 21-beta-hydroxylase enzyme (needed to make cortisol).
Lack of cortisol causes a build-up of androgens like testosterone, leading to ambiguous genitalia or virilization.
Key Points:
Steroid hormones (like testosterone, cortisol, and estrogen) are derived from cholesterol and require specific enzymes for their production.
21-beta-hydroxylase deficiency blocks cortisol production, increasing ACTH levels, which overstimulate the adrenal gland and increase androgen production.
Symptoms:
Ambiguous genitalia or incorrect gender assignment at birth.
Risk of salt-wasting (life-threatening loss of sodium due to low aldosterone).
Treatment: Glucocorticoids to correct hormone feedback and support proper development.
Scenario 4: Congenital Adrenal Hyperplasia (CAH)
What happens?
In an XX individual, high androgen levels are produced in utero due to a block in the 21-beta-hydroxylase enzyme (needed to make cortisol).
Lack of cortisol causes a build-up of androgens like testosterone, leading to ambiguous genitalia or virilization.
Key Points:
Steroid hormones (like testosterone, cortisol, and estrogen) are derived from cholesterol and require specific enzymes for their production.
21-beta-hydroxylase deficiency blocks cortisol production, increasing ACTH levels, which overstimulate the adrenal gland and increase androgen production.
Symptoms:
Ambiguous genitalia or incorrect gender assignment at birth.
Risk of salt-wasting (life-threatening loss of sodium due to low aldosterone).
Treatment: Glucocorticoids to correct hormone feedback and support proper development.
Summary of Gonadal Dysgenesis Scenarios:
Scenario Key Problem Effect Appearance | |||
1. AIS | Non-functioning androgen receptor | No response to testosterone. No male structures or external male genitalia. | Female (complete) or ambiguous (partial). |
2. 5-alpha Reductase Deficiency | Cannot convert testosterone to DHT | Internal male structures form, but no external male genitalia. | Female or ambiguous. |
3. Turner Syndrome (XO) | Missing a second X chromosome | Ovarian failure, small uterus and tubes, possible infertility. | Female, short stature. |
4. CAH | Excess androgen production due to enzyme block | Ambiguous genitalia or virilization. Risk of salt-wasting crisis. | Female or ambiguous. |