lect 10: vector-borne diseases // plasmodia
Introduction
usually done by arthropods
focus is on plasmodium as a pg - causes diff types of malaria
vectors act as carrier and the pg goes thru some part of its life cycle in the vector
can be passive (carried on body that is transferred to host) or direct (involves bite to transfer)
ex of diseases that’re vector borne: malaria, plague, sleeping sickness, yellow fever
ex of vectors: ticks, mites
Malaria
protist disease caused by plasmodium
mosquitoes are vectors - specifically anopheles mosquito
disease usually found in tropical and subtropical areas
relatively easy to treat and not that expensive BUT usually abundant in low income / less dev countries so not “economically incentivized” to help
diagnosed via blood smears to ID plasmodium infected erythrocytes (RBCs)
can recur years after the infection was treated
Plasmodium
complex life cycle:
infected mosquito dev sporozoites in it
releases them into blood stream into host, then go to liver
goes thru cycle of dev to become schizont and infect phagocytes
get into blood stream again
infect erythrocytes and grow inside them, then change their morphology and physiology
lyse cells and release more merozoites → infect more cells
some of them differentiate into male and female gametocytes (haploid) that are picked up by other mosquitoes to pass on
get fertilized in mosquito and cont cycle
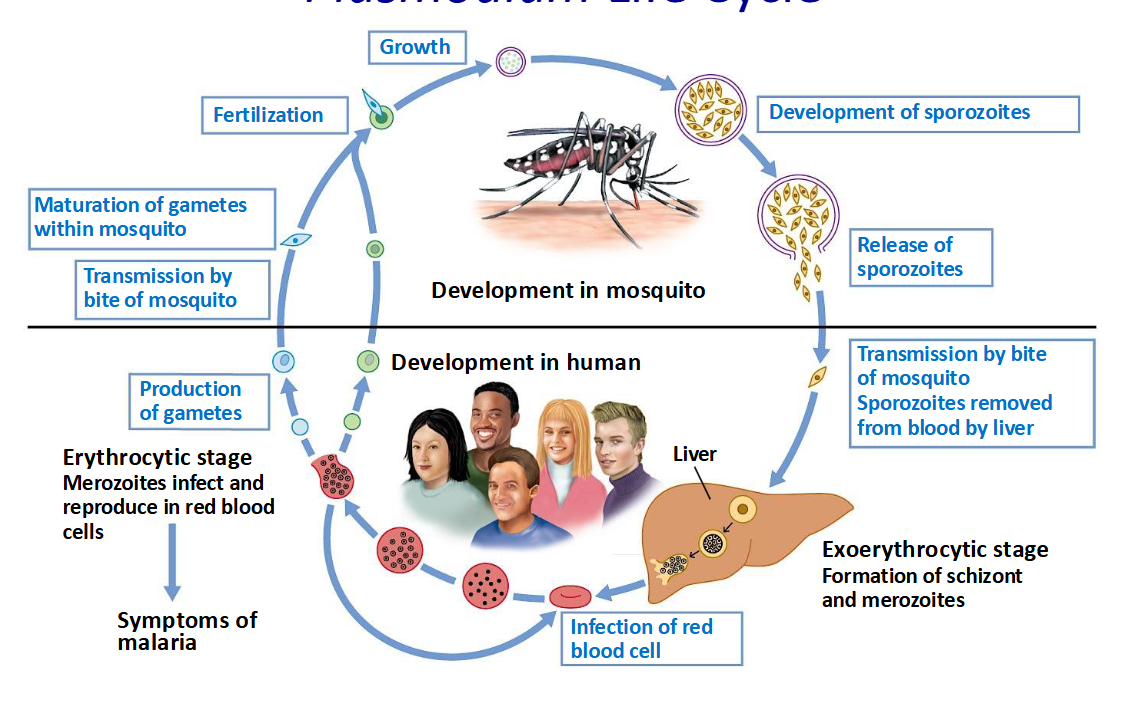
has T dept fertilization and humans too warm for fertilization, so only happens in mosquitoes
diff species of plasmodium have varying age of RBCs they prefer, fever periodicity, and if they have a dormancy period or not
vaccines target the major life stages: sporozoite, merozoite, or gametocyte
Disease Manifestations
parasite changes:
morphology → surface changes, affects behavior and ability to circulate, form clots, etc → tissue anoxia (damages)
metabolism → anemia, Fe imbalance → tissue anoxia
lyses RBCs → anemia
infection affects RBCs behavior and where they go → cause issues with peripheral tissues, kidney, and random clot formation
become less flexible and more likely to bind to the endothelial cells in the capillary beds
normal RBCs can form a “rosette” around infected RBCs → clots in microvasculature → tissue anoxia, inflammation
Prevention
vector control - spraying for mosquitoes, using bed nets, braining standing water that they use to lay eggs, insecticides
access - test for malaria, vector control items, meds, disease surveillance
chemoprevention - monthly treatments when pregnant, seasonal treatments for kids
Future Challenges
resistance to insecticides and parasite treatments
controlling the vector
inc mobility - disease introduced to US, inc exposure of previously immune indiv to new versions of disease
Focus On
life cycle
pros and cons of vaccine strat for 3 major targets
pg of malaria