Eyes
The structures of the outer eye work together to protect the eye from light and foreign bodies, while the structures of the inner eye function to optimize vision. Movement of the eyes is controlled by six muscles, which are innervated by three cranial nerves.
Eyelids | Conjunctiva | Lacrimal Gland | Eye Muscles |
|---|---|---|---|
|
|
|
|
Outer fibrous layer – sclera and cornea
Middle layer – choroid and ciliary body/iris
Inner layer – retina
Sclera | Cornea | Uvea – contains iris, ciliary body, choroids | Lens | Retina |
|---|---|---|---|---|
|
|
|
|
|
Innervated by cranial nerves III, IV, and VI. Cranial nerve II (optic nerve) connects the eye to the brain.
Eyelids | Conjunctiva | Lacrimal gland |
|---|---|---|
|
|
|
Sclera | Cornea | Uvea | Lens | Retina |
|---|---|---|---|---|
|
|
|
|
|
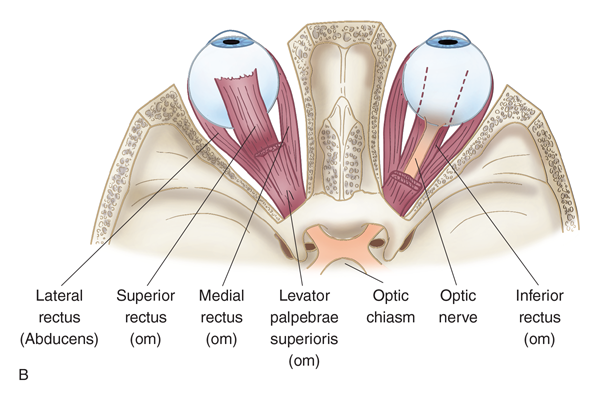
Eye movement is controlled by six muscles:
Superior rectus muscle
Inferior rectus muscle
Medial rectus muscle
Lateral rectus muscle
Superior oblique muscle
Inferior oblique muscle
The muscles are innervated by cranial nerves III, IV, and VI.
Oculomotor (III) – elevates and retracts upper eyelid
Trochlear (IV) – innervates superior oblique muscle
Abducens (VI) – innervates lateral rectus muscle
History of Present Illness: Eyes
question the patient about:
Red eye, conjunctival redness
Difficulty with vision
Pain/headache
Foreign body sensation
Current illness or similar symptoms in other members of the household
Allergies
Secretions
Photosensitivity (sensitivity to light)
Current medications
Onset, Duration, Location | Associated Symptoms | Aggravating/Alleviating Factors, Effort to Treat, Medication | Character, Severity, Predisposing Factors |
|---|---|---|---|
|
|
|
Predisposing factors:
|
Medical Surgical History
ask the patient about a history of:
Eye trauma
Eye surgery
Chronic illnesses affecting vision
Hypertension
Atherosclerotic cardiovascular disease (ASCVD)
Diabetes
Glaucoma
Thyroid dysfunction
Autoimmune disease
Human immunodeficiency virus (HIV)
Family History
question the patient about a family history of:
Headaches (type and character)
Thyroid dysfunction
Retinal cancer (retinoblastoma)
Glaucoma
Macular degeneration
Diabetes
Hypertension and other diseases affecting eye health
Color blindness
Cataracts
Retinal detachment
Retinitis pigmentosa
Allergies
Near/farsightedness
Personal/Social Histo
Personal/Social History | Potential Questions to Ask |
|---|---|
Environmental hazards |
|
Nutrition |
|
Tobacco/alcohol use |
|
Recreational drug use |
|
Physical activity |
|
Protective devices |
|
Corrective lenses |
|
Visual Testing of the Eye
Central Vision (Visual Acuity Testing)
Snellen charts: Pt stands 20 feet from chart. Most accurate way to test central vision. Test each eye independently. Numerator is distance pt is standing and denominator is distance that a normal eye can see.
Lea cards
Landolt C eye chart
HOTV eye chart
If the patient’s vision is less than 20/20, the nurse can use the pinhole test to determine whether vision loss is a refractive error.
Near Vision
Rosenbaum Pocket Vision card
Jager near vision card
Peripheral Vision: tested using the nasal, temporal, superior, and inferior fields of gaze:
Have the patient cover the right eye; the nurse’s left eye is covered.
The nurse and patient look into each other’s eyes.
The nurse fully extends the arm and moves the hand centrally, having the patient report when the fingers are first seen.
External Exam of Eye
Inspection | Palpation |
|---|---|
|
|
Extraocular Muscles
Eye movement is controlled by cranial nerves III (oculomotor), IV (trochlear), and VI (abducens), and the six extraocular muscles.
Internal Eye Inspection: ophthalmoscope
Red reflex: Reddish glow of eye. Stand 10 ft away, use opthalmoscope and observe for red reflex
Fundus
Blood vessel characteristics (follow blood vessels distally looking for crossing of arterioles and venules)
Disc characteristics
Retina
Macula characteristics
Normal Findings
Eye Inspection | Eye Palpation | Ophthalmoscope Examination |
|---|---|---|
|
|
|
Eye Variations in Children
Between 3 and 5 years of age, vision is typically 20/40. It reaches 20/30 or better by age 6.
Eye Variations: Older Adult
Weakened accommodation due to progressive weakness
Loss of lens clarity
Cataract formation
Decreased/distorted central vision
Excess tearing
Dry eyes
Yellow color or brown spots on sclera
Nocturnal eye pain
Abnormal Findings
Myopia: a common refractive error where close objects appear clear but distant objects are blurry, usually caused by the eyeball growing too long or the cornea curving too steeply
Amblyopia:a visual development disorder where the brain fails to process input from one eye, often resulting in reduced vision in that eye. It can be caused by strabismus, significant differences in refractive error between the two eyes, or other issues that interfere with clear vision during early childhood.
Presbyopia: a gradual loss of the eye's ability to focus on nearby objects, commonly associated with aging, typically beginning in the early to mid-40s when the lens becomes less flexible.
Limited field of vision temporally, 50 degrees superiorly, 70 degrees inferiorly
Hyperopia: a common refractive error also known as farsightedness, where distant objects can be seen more clearly than nearby objects due to the light entering the eye being focused behind the retina. This condition can be corrected with glasses, contact lenses, or refractive surgery.
Strabismus: a disorder in which the eyes do not properly align with each other when looking at an object. This misalignment can lead to double vision or the brain ignoring input from one eye, potentially resulting in amblyopia (lazy eye) if left untreated.
Exophthalmos: Eyes protrude. Surprised look
Enophthalmos: Sunken eyes, which can be caused by various factors including aging, dehydration, or certain medical conditions that lead to loss of fat or tissue around the eyes.
Blepharitis: Inflammation of eyelids, often characterized by red, swollen eyelids, crusted eyelashes, and discomfort. It can result from bacteria, skin conditions, or malfunctioning oil glands.
Chalazion: A localized swelling on the eyelid caused by a blocked meibomian gland, leading to a firm lump that may be painless, though it can cause discomfort and cosmetic concerns.
Hordeolum: An acute infection of the sebaceous glands of the eyelid, commonly known as a stye, presenting as a red, painful bump near the edge of the eyelid, often resulting from bacterial infection.
Dacryocystitis: A condition characterized by the obstruction of the nasolacrimal duct, leading to tear accumulation and potential infection, often resulting in excessive tearing and swelling in the inner corner of the eye.
Monocular Blindness: Pupils won’t respond to light in blind eye. Light shined in good eye will cause both pupils to constrict
Eye Inspection
Eyebrows asymmetrical, ending short of outer canthus, coarse texture
Orbital edema, puffiness, sagging tissue below orbit, xanthelasma (slightly raised, oval, yellow-tinted fatty deposit lesions)
Ectropion (lower lid turned away from the eye) or entropion (lid turned toward the globe)
Exophthalmos (bulging of the eyes, indicative of hyperthyroidism)
Fasciculations of eyelid when lightly closed
Ptosis (drooping eyelid)
Lagophthalmos (closed lids do not completely cover the eye)
Flakiness, redness, swelling in eyelid margin
Conjunctivae erythematous
Sclera yellow, green, dark, or rust-colored
Exudate
Pterygium (abnormal growth of conjunctiva that extends over cornea)
Corneal opacity
Enlarged lacrimal gland
Dry eyes
Inability to blink
Visible blood vessels
Miosis (pupil constriction to less than 2 mm)
Mydriasis (pupil dilation of more than 6 mm and failure to constrict with light)
Anisocoria (unequal pupil size)
Pupils continue to dilate when the light shines into them
Extraocular movements:
Sustained, jerking nystagmus, suggestive of extraocular weakness
Exposure of sclera from lid lag
Inability to move eye in all directions
Eye moves during cover-uncover test
Eye Palpation
Nodules on eyelids
Firm eye that resists palpation
Drooping
Ophthalmoscope Examination
Cloudy, opaque lens
Shallow chamber
Mydriasis
No red reflex
Discrete areas of pigmentation away from disc
Lesions
Drusen bodies
Hemorrhages
Nicking, tortuosity
Myelinated nerve fibers
Papilledema
Glaucomatous cupping
Documentation of History of Present Illness
Discomfort or photophobia
Redness
Watery discharge with or without crusting
Cloudy, blurry vision
Faded colors
Headlights, lamps, or sunlight being too bright
Halos around lights
Poor night vision
Double vision (diplopia)
Loss of peripheral vision
Exophthalmos: bulging of eye anteriorly out of orbit
Strabismus: both eyes do not focus on an object simultaneously, but either eye can focus alone
The nurse should document the patient’s report of:
Trauma that can cause complete or partial dislocation of the eye
The nurse should document the patient’s report of:
Poor vision
Sudden onset of double vision
Report of eye deviation
Documentation of Medical, Surgical, Family, and Personal/Social History
Employment risk: exposure to fumes, chemicals, particulates
Stress and coping mechanisms
Injury risk
Nutrition: excessive sugar
Use of alcohol, recreational drugs
Tobacco use (pack-year history), type of tobacco (cigarettes, chewing tobacco, snuff)
Sports played, new activities, use of protective eyewear
Corrective lenses – glasses, contacts
Trauma
Eye surgery
Chronic illness that can affect vision
Hypertension
Diabetes
Glaucoma
Inflammatory bowel disease
Thyroid dysfunction
Autoimmune disease
HIV
Retinoblastoma
Glaucoma
Color blindness
Nearsightedness, farsightedness
Strabismus
Amblyopia
Objective Data
Eyelids (loose, wrinkled)
Quality of the eyes (sunken, protruding)
Discharge
Eye movement
Ocular pressure
Hemorrhaging
Exophthalmos
Strabismus
Cataracts
Glaucoma
Apparent eye protrusion
Lids do not reach iris
Measurement of degree of exophthalmos performed using exophthalmometer
Eye will not move in the direction controlled by affected muscle
Abnormal cover-uncover test result
Cloudy lens, may be obvious without equipment
Optic nerve damage, clearly seen during dilated eye examination
Characteristic cupping of optic nerve
Visual field test showing loss of peripheral vision
Key Notes
• The eyes carry visual data that are crucial for survival, education, and pleasure. More than half of our neocortex is involved with processing visual information.
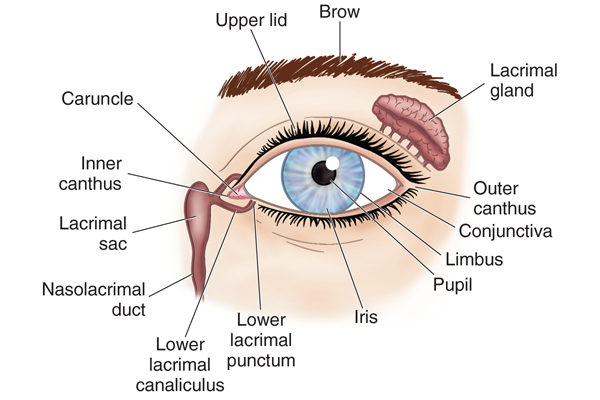
• The external anatomy of the eye includes many structures. Each eye is protected by the bony orbital cavity surrounded with a cushion of fat.
• The eyelids further protect the eye from injury, strong light, and dust. The upper eyelid is larger and more mobile. Eyelashes curve outward from the lid margin to filter out dust and dirt. When closed, the lid margins approximate completely.
• The canthus is the corner of the eye, where the lids meet. The caruncle (a small fleshy mass containing sebaceous glands) is located at the inner canthus. A stripe of connective tissue, the tarsal plate, gives shape to the upper lid. The tarsal plates contain Meibomian glands, which secrete an oily lubricant onto the lids.
• The conjunctiva, a thin mucous membrane, is a transparent protective covering of the exposed part of the eye. The lacrimal apparatus provides constant irrigation. Tears drain into the puncta, visible on the upper and lower lids at the inner canthus.
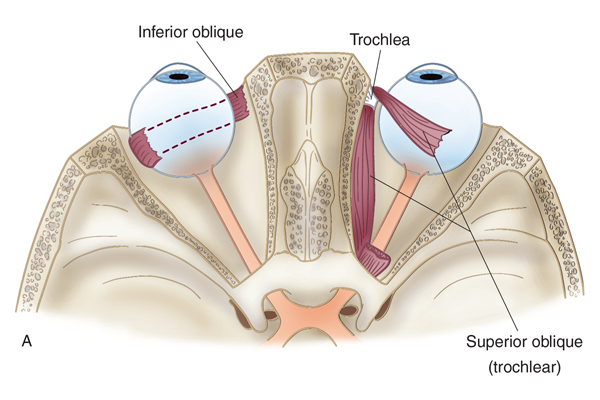
• Six muscles attach the eyeball to its orbit and serve to direct our eyes to points of our interest: the superior, inferior, lateral, and medial rectus muscles and the superior and inferior oblique muscles. The movements of the extraocular muscles are stimulated by cranial nerves III, IV, and VI.
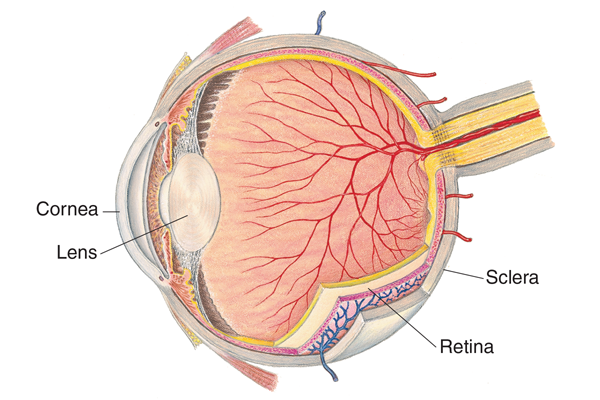
• The internal anatomy of the eye also includes many structures. The eye has three concentric coats or layers.
The outer layer is the sclera, a tough, fibrous protective, white covering that is continuous anteriorly with the smooth, transparent cornea. The cornea, which is part of the refracting media of the eye, covers the iris and pupil.
The middle layer is the choroid, which has dark pigmentation to prevent light from reflecting internally and is heavily vascularized to deliver blood to the retina. The choroid is continuous with the ciliary body and the iris. The ciliary body controls the thickness of the lens. The iris serves as a diaphragm, varying the opening at its center. Its muscle fibers contract and dilate the pupil, controlling how much light enters the retina.
The inner layer is the retina, which is the visual receptive layer of the eye. In the retina, light waves are changed into nerve impulses. The area of sharpest and keenest vision is the fovea centralis. The macula, a slightly darker pigmented region surrounding this area, transduces light from the center of the visual field.
• Visual reflexes include the pupillary light reflex, fixation, and accommodation.
The pupillary light reflex is the normal constriction of the pupils when bright light shines on the retina. Should be direct and consensual.
Fixation is a reflex direction of the eye toward an object attracting a person’s attention.
Accommodation is the adjustment of the eye for near vision. It is accomplished by ciliary muscle movement.
• The eyes undergo age-related changes.
At birth, eye function is limited. Peripheral vision is intact in newborns. The macula is absent at birth but is mature by age 8 months. Eye movement is poorly coordinated but matures by age 3 to 4 months. The eyeball reaches adult size by age 8.
With aging, lacrimal gland involution causes decreased tear production and dry, burning eyes. Pupil size decreases and the lens loses elasticity, causing presbyopia. The transparent fibers of the lens begin to thicken and yellow, resulting in cataract. Visual acuity may diminish gradually after age 50. In older adults, the four most common causes of decreased visual functioning are cataracts, glaucoma, age-related macular degeneration, and diabetic retinopathy.
• Culturally based variability exists in the color of the iris and retinal pigmentation, with darker irises having darker retinas behind them.
• Visual impairment is not being able to see letters on the line 20/50 or below on the eye chart. Racial disparities exist among major eye diseases and in visual impairment.
• Visual screening in children is crucial to detect strabismus and amblyopia. This section presents critical points about subjective and objective assessments of the eyes.
• To obtain subjective data, ask questions that investigate these topics:
Vision difficulty, including decreased acuity, blurring, and blind spots
Eye pain, burning or itching
Strabismus or diplopia
Redness or swelling
Watering or discharge
A history of ocular problems
Glaucoma
Use of glasses or contact lenses
Patient-centered care
Medications, systemic or topical
History of smoking
Vision loss
Additional history for infants and children should include vaginal infections in the mother at time of delivery, developmental milestones of vision noted by the parent, routine vision testing at school, and awareness of safety measures to protect the child’s eyes from trauma.
Aging adults should be asked about visual difficulty with driving or night vision, glaucoma testing, history of cataracts, dry or burning eyes, and decrease in usual activities.
• To obtain objective data, first test central visual acuity with a Snellen or other eye chart. For those over age 40 or who have difficulty reading, also test near vision.
Next, assess visual fields for loss of peripheral vision using the confrontation test: Stand arm’s length away and eyes length. Pt covers one eye; you cover same eye. Stare at each other’s nose and move finger into field of vision, you and patient should see finger at the same time.
Continue by observing extraocular muscle function. To do this, assess the corneal light reflex using the Hirschberg test (Used to see if pt has strabismus. Pt looks straight, Light 12 in away into pt eye. Light should be centered in both eyes). Also perform the diagnostic positions test, which is known as the six cardinal positions of gaze. Note any nystagmus.
Then inspect external eye structures. After a general inspection, specifically assess the eyebrows, eyelids and lashes, eyeball alignment, conjunctiva and sclera, upper lid eversion, and lacrimal apparatus.
Move on to inspect anterior eyeball structures. Observe the cornea and lens. Assess the iris and pupil, particularly noting their size, shape, and equality; the pupillary light reflex; and accommodation.
Finally, inspect the ocular fundus, or the internal surface of the retina, using an ophthalmoscope.
Observe the optic disc, noting its color, shape, and margins.
Estimate the cup-disc ratio.
Inspect the retinal vessels, assessing their number, color, caliber, and arteriovenous crossings. Estimate the artery-vein ratio, and check for tortuosity and pulsations.
Evaluate the color and integrity of the general background.
Inspect the macula last because it may cause watering, discomfort, and pupil constriction.
Adapt your examination techniques based on the patient’s developmental status. For example, use age-appropriate tools to assess visual acuity, such as a picture chart or Snellen E chart for a child, and color vision. Also adjust your expected findings based on the patient’s age.
The older adult’s central acuity and peripheral vision may be diminished. Vision impairment in the elderly is a leading cause of falls.
• When assessing the eyes, incorporate health promotion concepts. Keep in mind, for instance, that glaucoma is the leading cause of preventable blindness in the United States. Encourage early screenings for glaucoma
Class Notes
External Anatomy
Bony orbital cavity surrounded by cushion of fat protects eye
Palpebral fissure: opening between eyelids
Limbus: forms border between sclera and cornea
Canthus: upper and lower lids meet in corner of the eye.
Lateral and medial
Medial canthus holds the caruncle which is the fleshy part in corner of eye that moisturizes eyes and protects from bacteria
Tarsal plates
Meibomian glands
Conjunctiva: covers sclera and underside of upper and lower eyelids. Lubricants eye, secretes mucous and tears, protective barrier.
Cornea
Lacrima apparatus: lacrimal glands excrete tears
Extraocular muscles are innervated by cranial nerves III, IV, and VI. They hold eyes symmetrical and help eyes move at same time
Superior rectus (III)
Inferior rectus (III)
Lateral rectus (VI)
Medial rectus (III)
Superior Oblique (IV)
Inferior oblique (III)
Internal Anatomy
Eyes: Sphere of three concentric coats
Outer fibrous sclera
Sclera: Very limited blood vessels. Maintain shape of eye. Protects from external trauma.
Cornea: Protective. Allows lights in, focuses retina. Bends light to focus objects on inner retina. Must remain clear. Contains nociceptive cells (pain)
Middle Vascular Choroid:
Choroid: provide nourishment, very vascular
Iris: Color tissue. Use muscles to change size of pupil
Pupil: Determines how much light comes through. Opening at center of iris. Round, equal, black, very reactive to light. Normally 3-5 cm in size.
Lens: Size changes with focus. Behind iris. Clear. Refract light onto pupil. Elastic. Bulges to focus near and flattens when looking far.
Chambers act as boundaries
Anterior: Aqueous humor. Space between cornea and iris. Thin fluid contains vitamins and proteins. Aids in eye shape and light refraction. Small amount of fluid enters and exits constantly.
Posterior
Vitreous: Largest chamber, gel like vitreous humor, shock receptor maintains shape.
Inner Nervous Retina
Retina
Optic Disc: Circular area inside the back of the eye. Entry point for major blood vessels. Edema is papilledema (due to increased cranial pressure from CSF)
Optic Nerve: Responsible for carrying visual images to the brain
Macula: Center of retina. Central vision.
Fovea Centralis: Area of sharpest vision
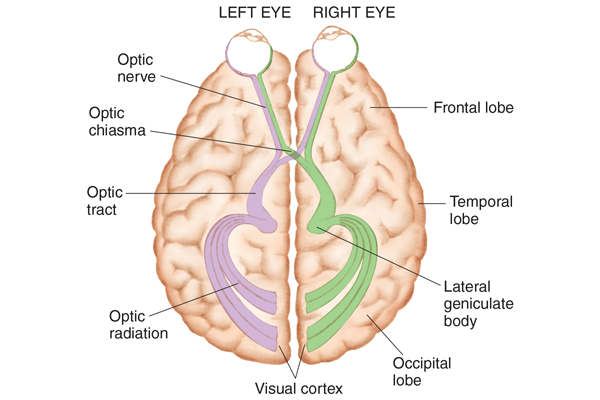
Visual Pathways and Visual Fields: Pathway connects eyes to brain
Crossing of fibers at optic chiasm:
Left vision: Everything on the left.
Right Vision: Everything on the right
Optic Chiasm: Some visual signals will pass to other side. If there is damage before optic chiasm, you lose vision in one eye. If there is damage after the optic chiasms, vision is lost in both eyes.
Visual Reflexes:
Pupillary Light Reflexes: No conscious control.
Direct: When one eye is exposed to bright light and it constricts
Consensual: When light is shined in one eye, both eyes constrict
Fixation Reflex: Maintaining fixed visual gaze on an object. Foiba centralis. Extra ocular muscle helps maintain fixation. Can be impacted by external effects
Accommodation Reflex:
Convergence: Happens automatically (Like looking at far object and changed to near object)
Developmental Considerations:
Infants and Children:
Peripheral Vision: Intact but lens is spherical
Macula: Absent but matures at 8 months
Binocular Vision: 3-4 months old and can fixate Reaches adult size at 8 years
Aging Adult: Loss of skin elasticity. Lose fat tissue around orbit, muscles atrophy, pupil size changes, lens change and thickens, more rigid, and can’t accommodate for near vision. Presbyopia after age 40. Visual acuity decreases at 50. Difficulty adapting to the dark which impairs night driving and increases risk of falls.