Oral biology and tooth morphology Final
Orofacial development
first thing that happens during the Orofacial development is the embryo develops into three types of tissues, called the germ layers:
1- Ectoderm: forms the outer covering and the nervous system
2- Mesoderm: gives rise to muscle, internal organs, and connective tissues such as blood and cartilage.
3- Endoderm: produces the lining of the digestive tract or gut, along with some of the associated organs.
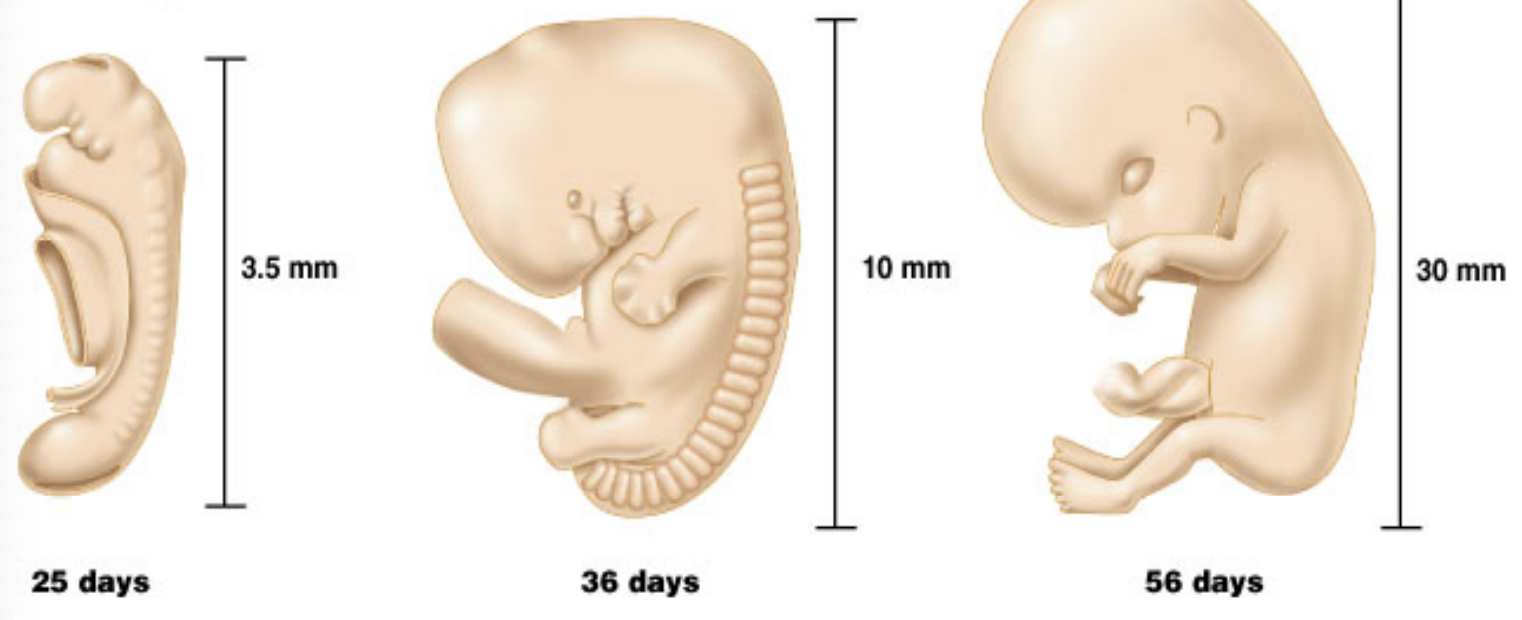
Embryonic period: first 8 weeks after conception during which all major organs and structures are formed, laying the groundwork for the subsequent stages of development.
29 day embryo or about 4 weeks or 1 month: Heart starts pumping, size is ½ cm
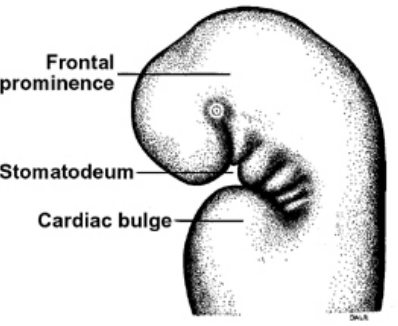
Development of primitive oral cavity and head fold:
The head folding results in the formation of the primitive oral cavity = stomatodeum.
Initially, the stomatodeum is separated from the developing gut by the buccopharyngeal membrane. In the fifth week of development, this membrane ruptures, connecting the oral cavity to the foregut and forming the oropharynx. This connection is essential for the subsequent development of the digestive and respiratory systems.
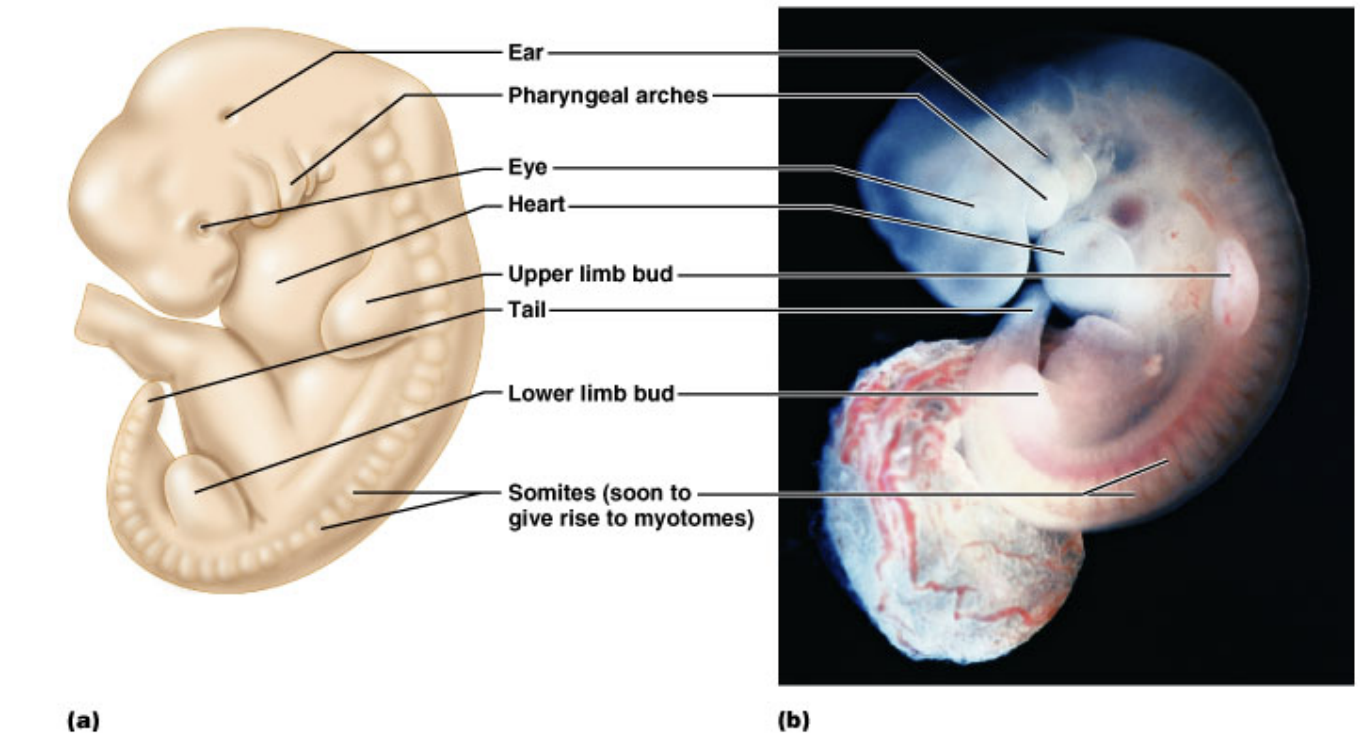
Branchial arches/ pharyngeal arches/ branchial apparatus
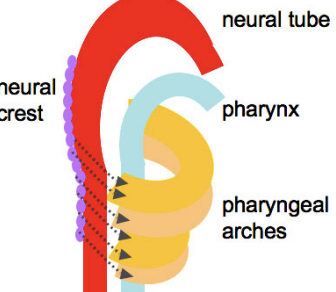
The pharyngeal arches are named like this because they bend around the sides of the pharynx as bars of tissue, each arch is separated by vertical grooves on the lateral sides of the neck at the fifth week
Medially they are seperated by pharyngeal pouches.
They are 6 pairs - U Shaped
Core of the mesenchymal tissue is formed from neural crest cells that migrate in to form the arches
They are covered externally by ectoderm and lined internally by endoderm
Each have their own developing cartilage, nerve, vascular and muscular components
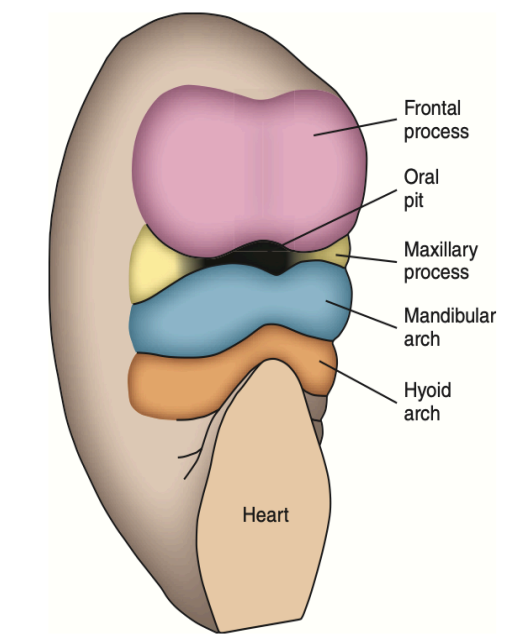
These arches separate the stomatodeum from the developing heart.
The first arch (mandibular arch) - forms the mandibular and maxillary processes, associated muscles of mastication, nerves, and blood supply.
The second arch (hyoid arch) - forms the hyoid bone, and part of the temporal bone (VII)
Cartilage = Reichert’s cartilage- form the muscles of facial expression, the middle ear muscles
Third arch - forms the tongue (ix nerve)
Fourth arch - forms the tongue, most of the laryngeal cartilages (IX and X nerves)
Fifth arch - Incorporates into the fourth
Sixth arch - Forms most of the laryngeal cartilages (IX and X nerves)
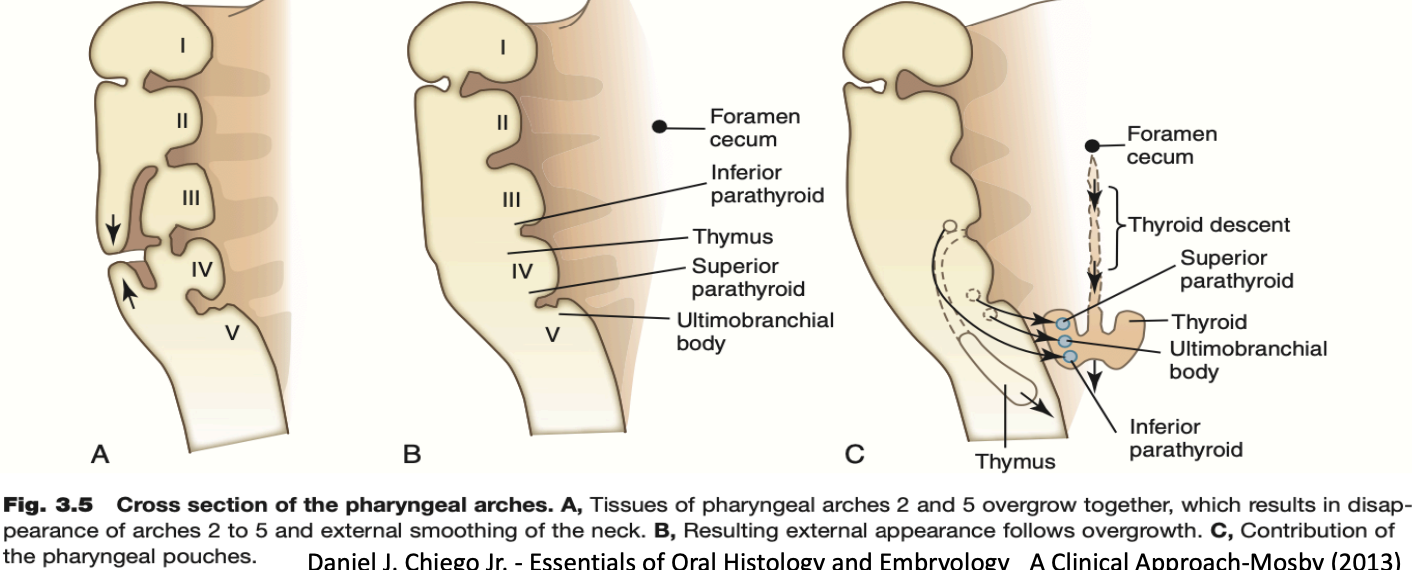
Pharyngeal pouches:
They are four well-defined pairs of pharyngeal pouches that develop from the lateral walls of the pharynx.
The first pouch (between the 1st and 2nd arches) gives rise to the external acoustic meatus, tympanic membrane, and eustachian tube
The second pouch forms the palatine tonsils.
The third pouch forms the thyroid and parathyroid glands
The fourth pouch forms the parathyroid gland
The fifth pouch becomes incorporated with the fourth
Development of the face
Starts from the fusion of five face-primordia (or bulges or processes) that were formed during 4th week of IUL
• One Frontonasal prominence from frontal lobe
• Two Maxillary prominences from first branchial arch
• Two Mandibular prominences from first branchial arch
• The fusion occurs during the 5th to 8th week of IUL.
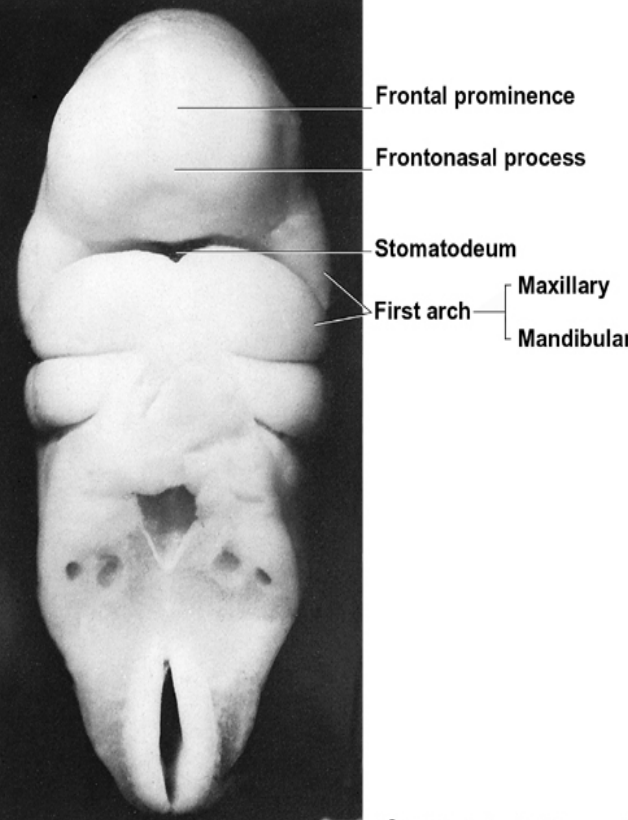
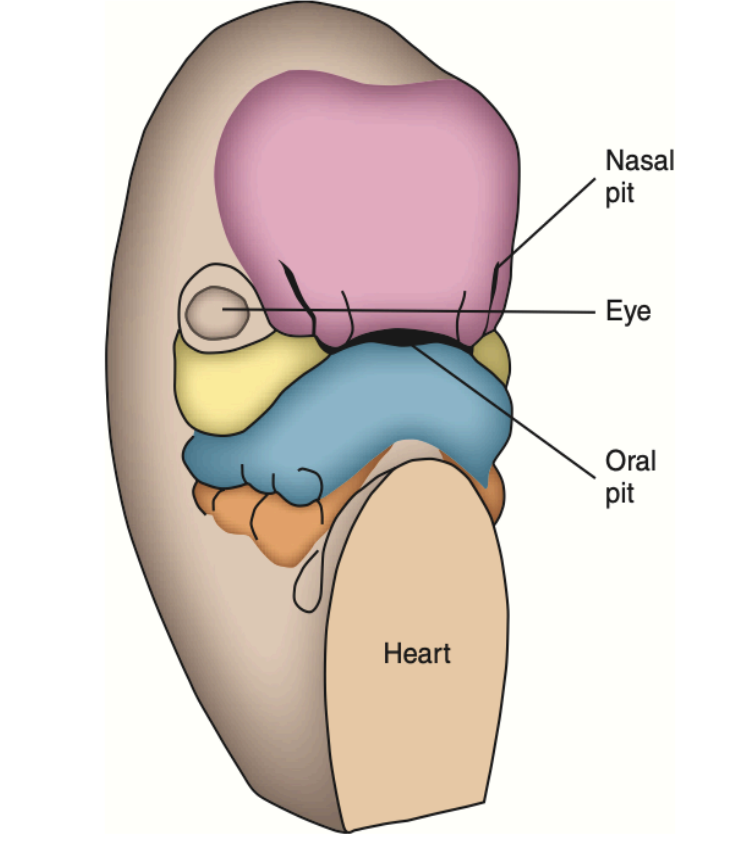
During the 4th week of IUL, the centrally located oral pits are grouped at the frontal and maxillary processes and the mandibular arch. Although it appears unrelated at this time, during this period these processes and the first arch form the human face.
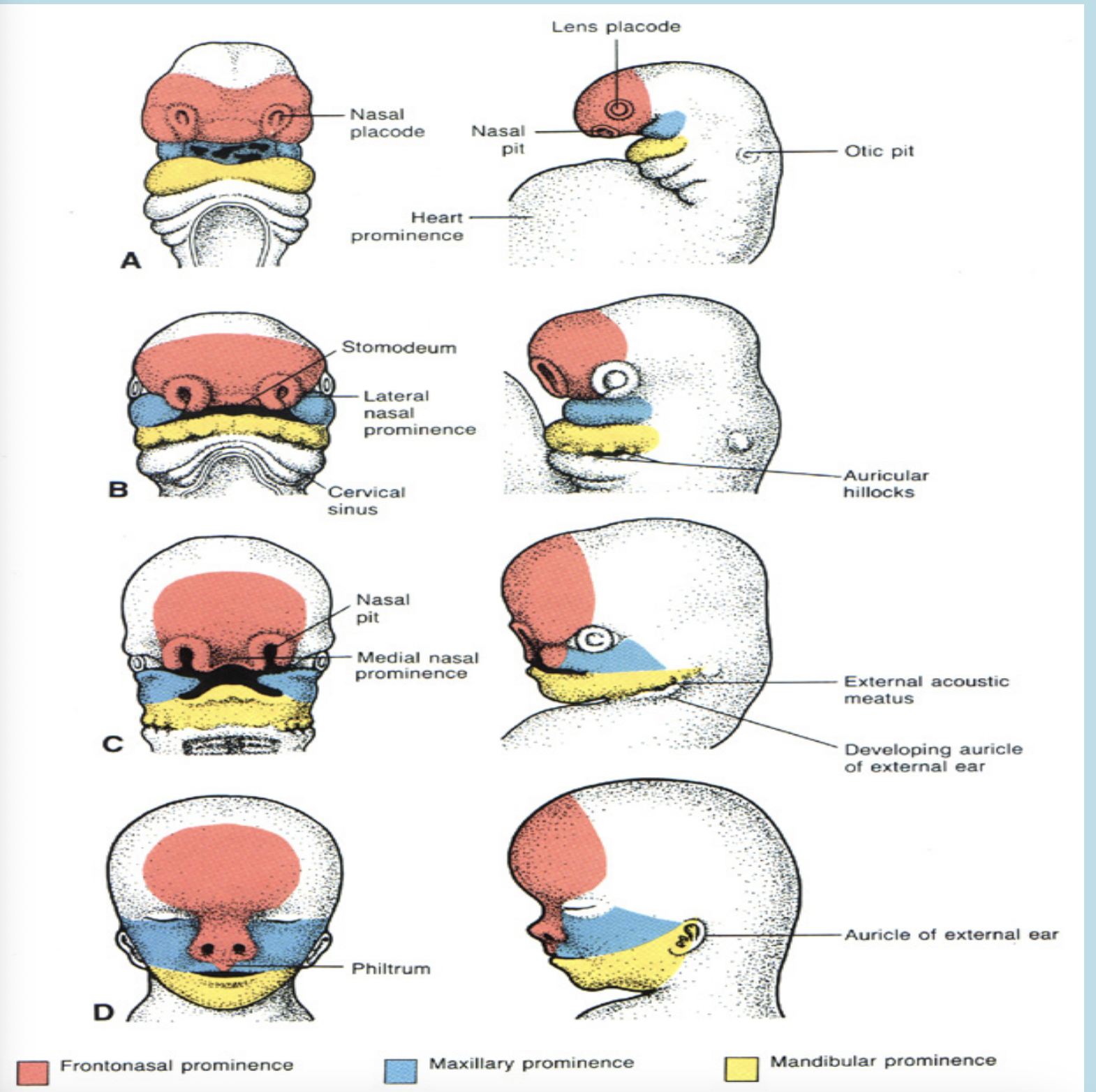
During the 5th week of IUL the nasal pits develop and now appear on the sides of the face. The frontal processes now become the frontonasal process.
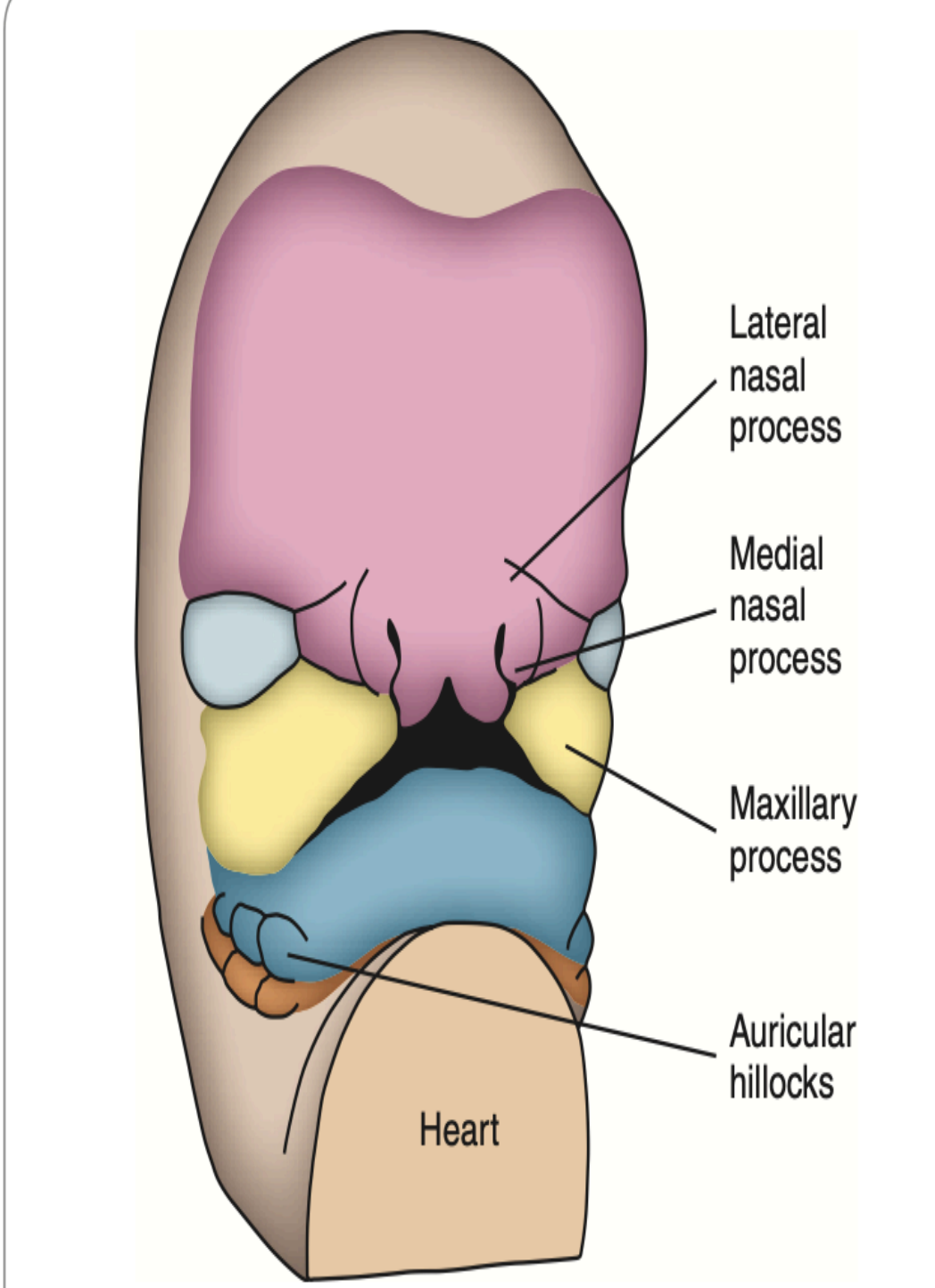
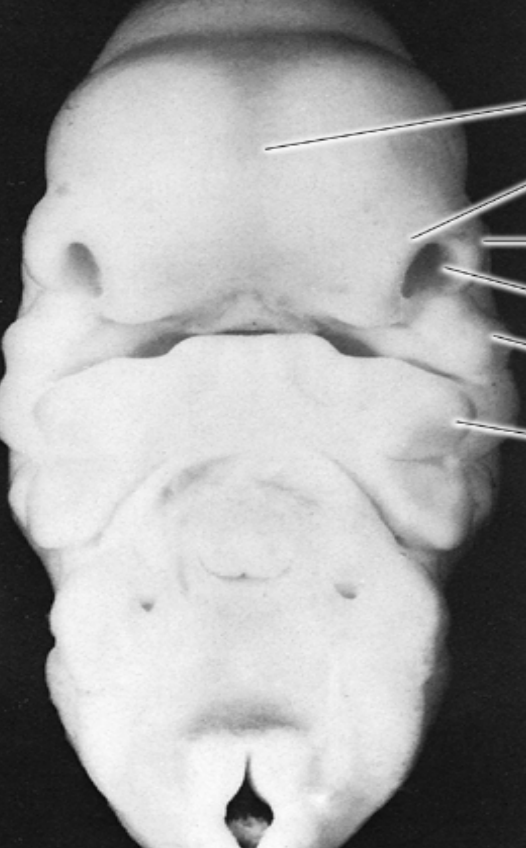
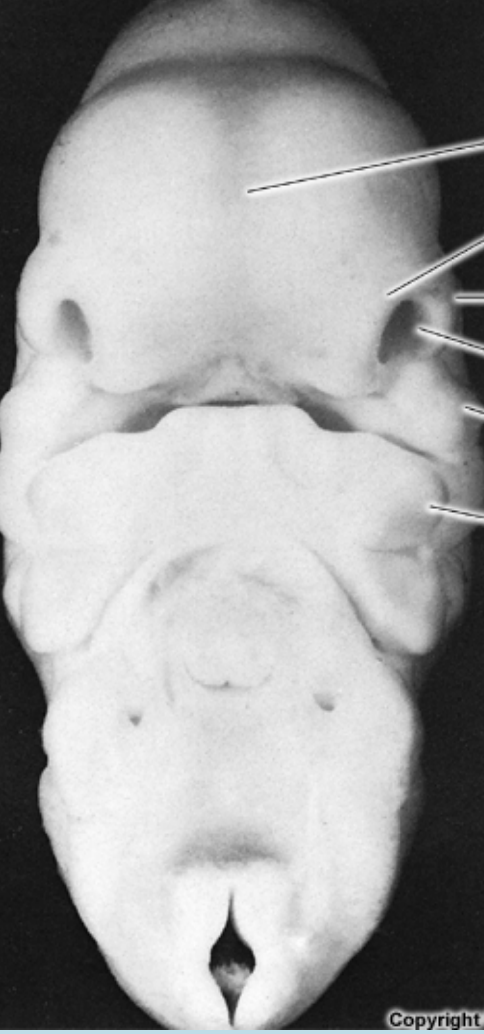
During the 6th week of IUL, the lateral parts of the face begin to expand which broadens the face. the nasal processes are limited to the middle of the upper lip, which make the face appear more human like
The upper lip is composed of a medial process and two lateral maxillary segments
The medual nasal process is called the philtrum
A ridge of tissue surrounds each nasal pit
The tissue lateral to the pits is the lateral nasal process
The tissue medial to the pits is the medial nasal process
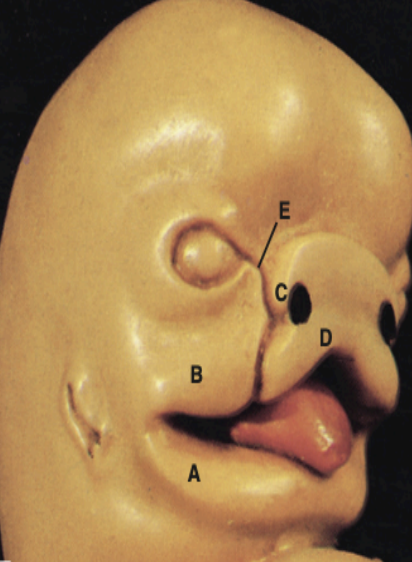
A- Mandibular process
B- Maxillary process
C- Lateral nasal process
D- Medial nasal process
E- Naso-optic furrow
The development of the upper face is from the tissues surrounding the oral pit.
Day 24: The frontal process develops (it covers the forebrain) Which result in the start of the maxillary and mandibular processes from the 1st branchial arch, and a well-defined boundaries of the stomatodeum.
Day 26: The maxillary and mandibular processes become well-formed
Day 27: The nasal placode and the odontogenic epithelium appear
Day 28: Localized thickenings develop within the frontal prominence which are the olfactory placodes.
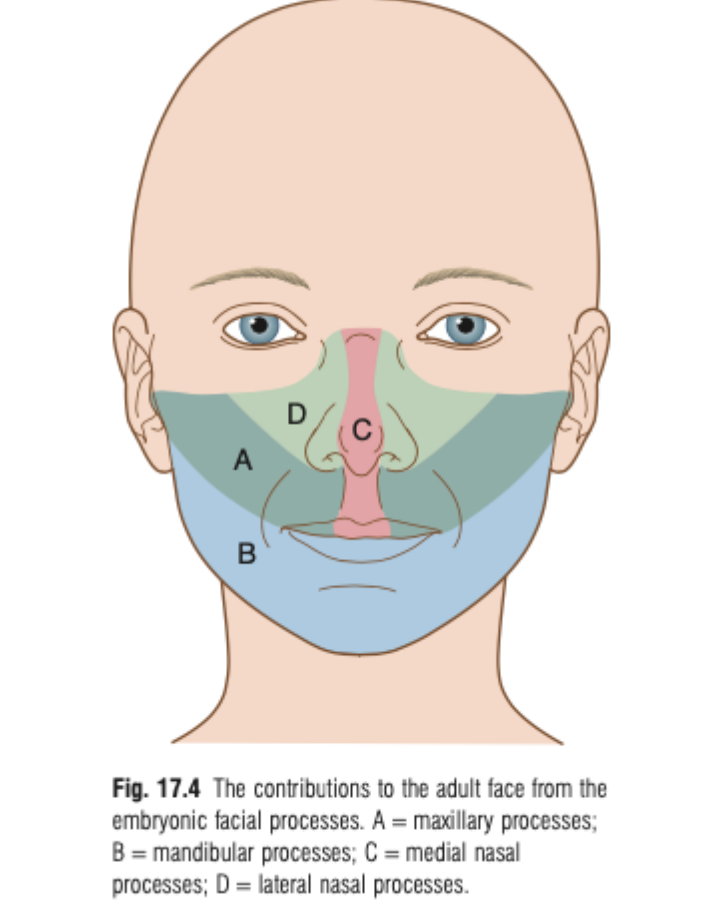
The contributions to the adult face from the embryonic facial process:
Maxillary processes: Contribute to the upper lip, cheeks, and part of the palate.
Mandibular processes: Form the lower lip and mandible.
Medial nasal processes: Forms the bridge of the nose, the tip of the nose, and the nasal septum, as well as the midline of the upper lip.
Lateral nasal process: Forms the lateral aspects of the nose and contributes to the alae of the nostrils.
Development of naso-maxillary complex:
By the 4th to 5th week of development, nasal placodes (thickened areas of epithelium) form, which become the olfactory epithelium.
Ectomesenchyme cells proliferate and migrate around these placodes, forming medial and lateral nasal processes surrounding the nasal pits.
The medial nasal processes fuse at the midline, forming the intermaxillary (premaxillary) process, which contributes to the premaxillary segment.
Development of naso-maxillary complex:
The frontal lobe proliferates between the medial nasal processes to form the frontonasal prominence, which contributes to the forehead and parts of the nose.
The medial nasal processes (from both sides) and the frontonasal prominence together form the middle portion of the nose, upper lip, anterior maxilla, and the primary palate.
The upper face develops faster than the lower face during this period.
Early facial development is driven by tissue proliferation and migration forming the primitive nasal cavities.
The naso-maxillary complex forms early in development through tissue growth and movement.
Around day 28, olfactory placodes (thickened ectoderm) appear and form nasal pits as the tissue beneath (mesenchyme) grows.
These pits split into:
Medial nasal processes (inner side)
Lateral nasal processes (outer side)
The frontonasal prominence (from the forehead area) and the medial nasal processes join to form the:
Middle nose
Upper lip
Front part of the upper jaw (anterior maxilla)
Primary palate
During this time, the upper face grows faster than the lower face.
Paranasal Sinuses & Nasal Cavity Development
Some paranasal sinuses begin developing in late fetal life.
Frontal and sphenoid sinuses are not present at birth.
By age 2, the anterior ethmoid sinuses grow into the frontal bone (visible on X-rays by age 7).
Posterior ethmoid sinuses grow into the sphenoid bone.
Sinuses influence facial size/shape in infancy and voice resonance.
Remaining sinuses develop after birth.
They form as outgrowths from the nasal cavity wall.
These outgrowths become air-filled extensions in adjacent bones.
The original openings remain as the adult sinus orifices.
Maxilla Development
The maxillary process arises from the first branchial arch.
Ossification centers form in the maxillary processes and extend into the palatine process to form the hard palate.
The maxillary process gives rise to the cheek, maxilla, and zygomatic bone.
It fuses with the lateral nasal process (LNP), creating the naso-optic furrow.
Fusion of facial processes at the center creates a bulge from the medial nasal process (MNP) called the premaxillary/globular process.
This forms the primary palate and four incisor teeth.
Maxillary tooth development begins as epithelial thickenings in the arch at their future positions.
Development of palate involves the formation of:
Primary palate
Forms from the premaxillary process (fusion of medial nasal processes)
Secondary palate
Forms from the two lateral palatine shelves or processes
Develop as internal projections of the maxillary prominences
Fusion of their processes
Fusion of the median nasal processes gives rise to the median palatine process and form the primary palate.
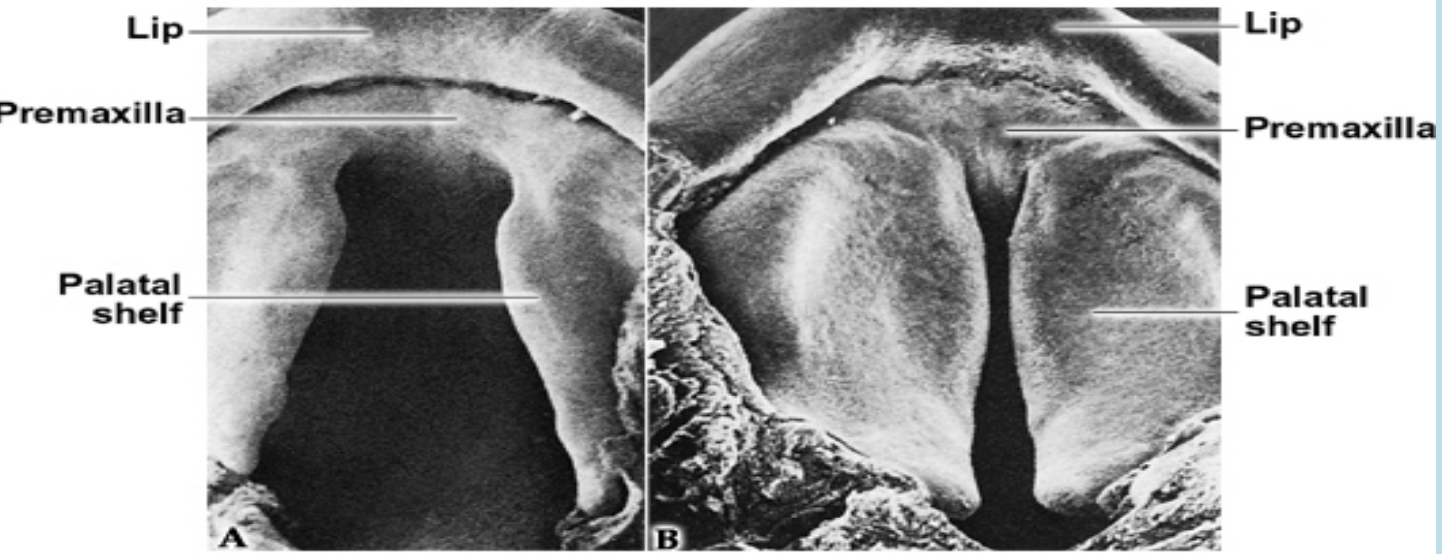
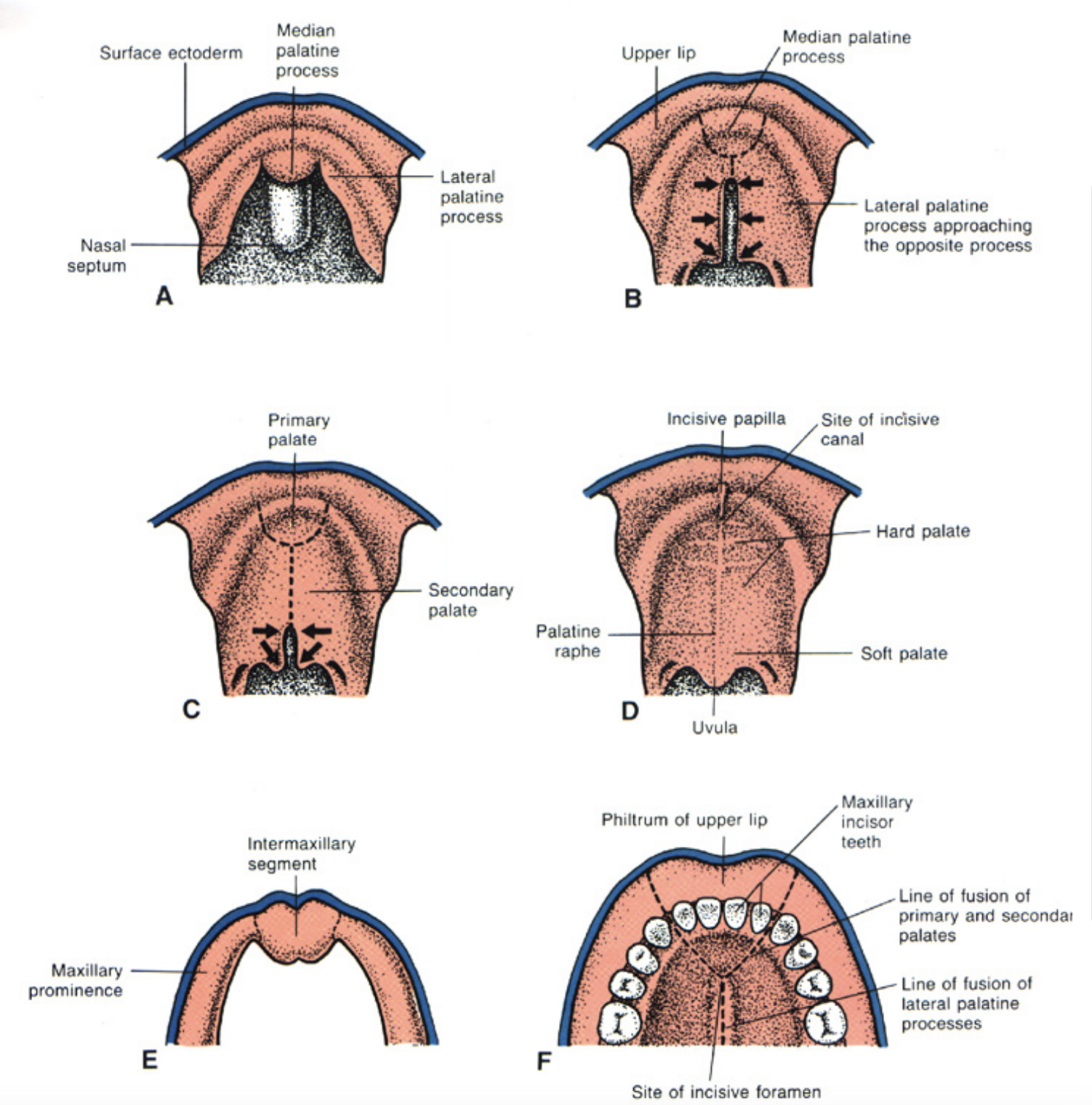
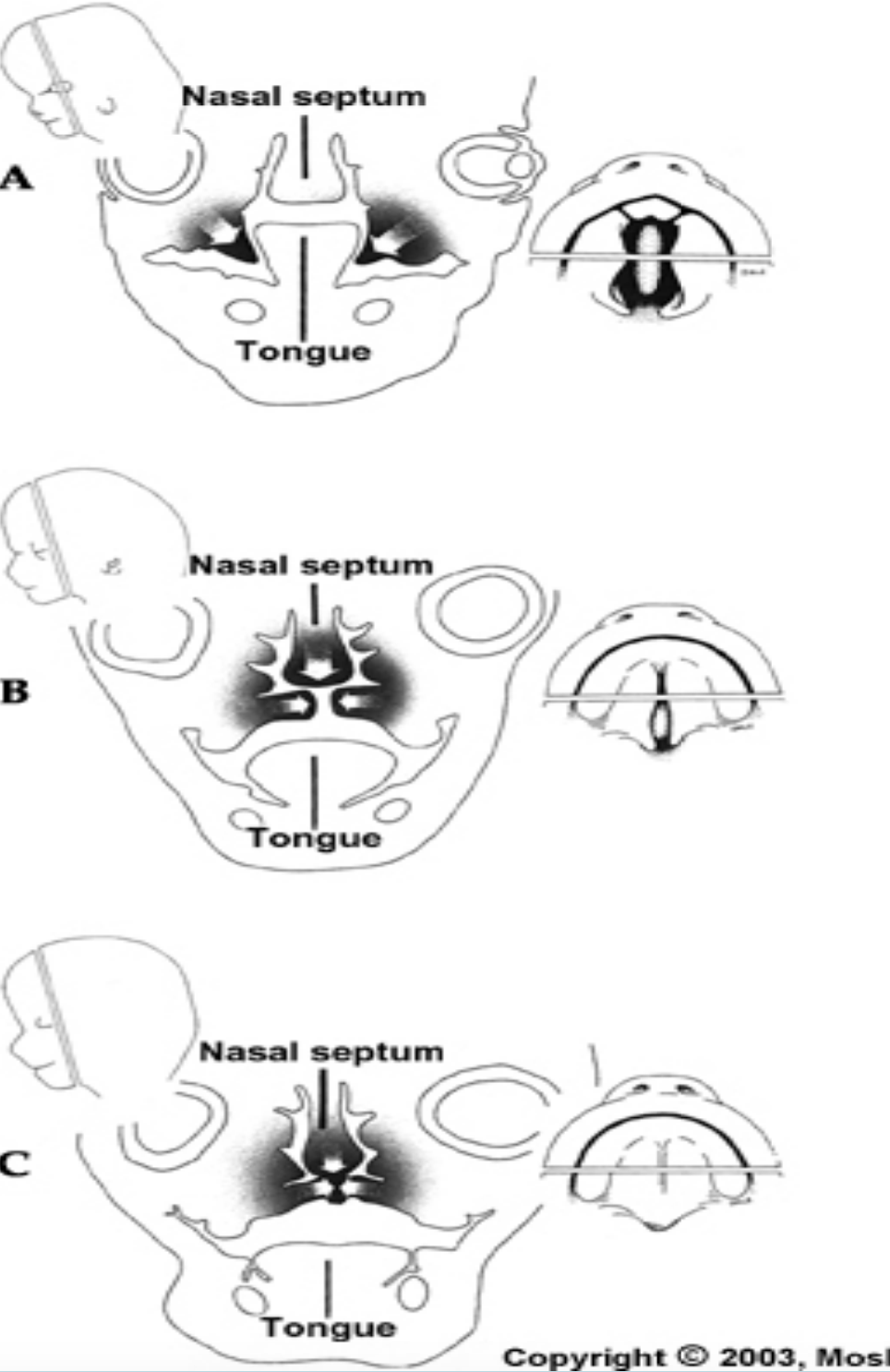
Primary and secondary palate:
The common oronasal cavity is bounded anteriorly by the primary palate and occupied by the developing tongue
Only after the development of the secondary palate, the oral and nasal cavities can be distinguished.
Three outgrowths appear in the oral cavity:
Nasal septum: Grows downwards through the oral cavity and it encounters the primary and secondary palates
2 palatine shelves
The closure of the secondary palate involve the hardening of the palatine shelves along with the downward movement of the tongue.
During the fourth week of development:
The maxillary processes fuse with the medial nasal processes, forming the lateral parts of the upper lip, while the medial nasal processes form the central part of the upper lip.
The maxillary processes also fuse with the lateral nasal processes, creating the nasolacrimal groove (from the inner eye corner to the nasal cavity).
The entire lower lip develops from the mandibular process.
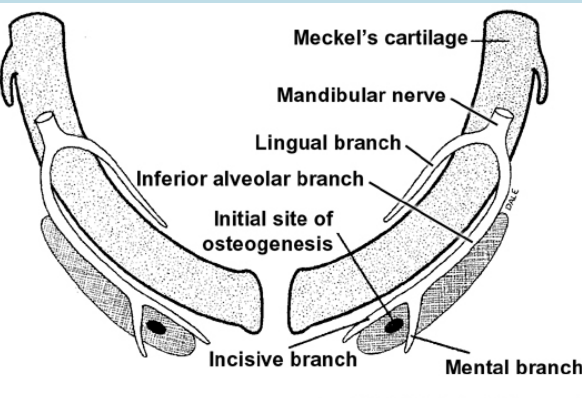
Mandible development begins with Meckel’s cartilage (from the first branchial arch) around 6 weeks, forming a rod surrounded by a fibrocellular capsule. The two cartilages are separated at the midline by the mandibular symphysis.
Mesenchymal condensation occurs near the symphysis.
At 7 weeks, intramembranous ossification begins in this mesenchyme, spreading forward and backward to form the mandible.
The mandible bones grow toward the midline but do not fuse immediately—the mandibular symphysis, derived from Meckel’s cartilage, fuses shortly after birth.
The ramus forms through rapid posterior ossification into the first arch mesenchyme.
Growth of the mandible until birth is influences by the appearance of three secondary (growth) cartilages
condylar – 12th week, developing ramus by endochondral ossification, a thick layer persists at birth at the condylar head (mechanism for post-natal growth of the ramus = endochondral)
coronoid – 4 months, disappears before birth
symphyseal – appears in the connective tissue at the ends of the Meckel’s cartilage, but disappear after 1 year after birth
Development of the tongue begins in about 4 weeks of embryonic development.
The oral part (anterior two-thirds) of the tongue develops from the fusion of two lateral lingual swellings and a median tuberculum impar.
The pharyngeal part or root of the tongue (posterior one-third) develops from the copula and the hypobranchial eminence (forms from the 2nd, 3rd and 4th branchial
arches)
Muscles of the tongue arise from occipital somites which migrate into the tongue area
The tongue develops from the endoderm of the first four bronchial arches.
During the fourth week of IUL, pairs of swellings called lingual swellings from the first arch and a single swelling called tuberculum impar originates, with ectoderm covering outside. The lingual swellings give rise to anterior 2/3 of the tongue.
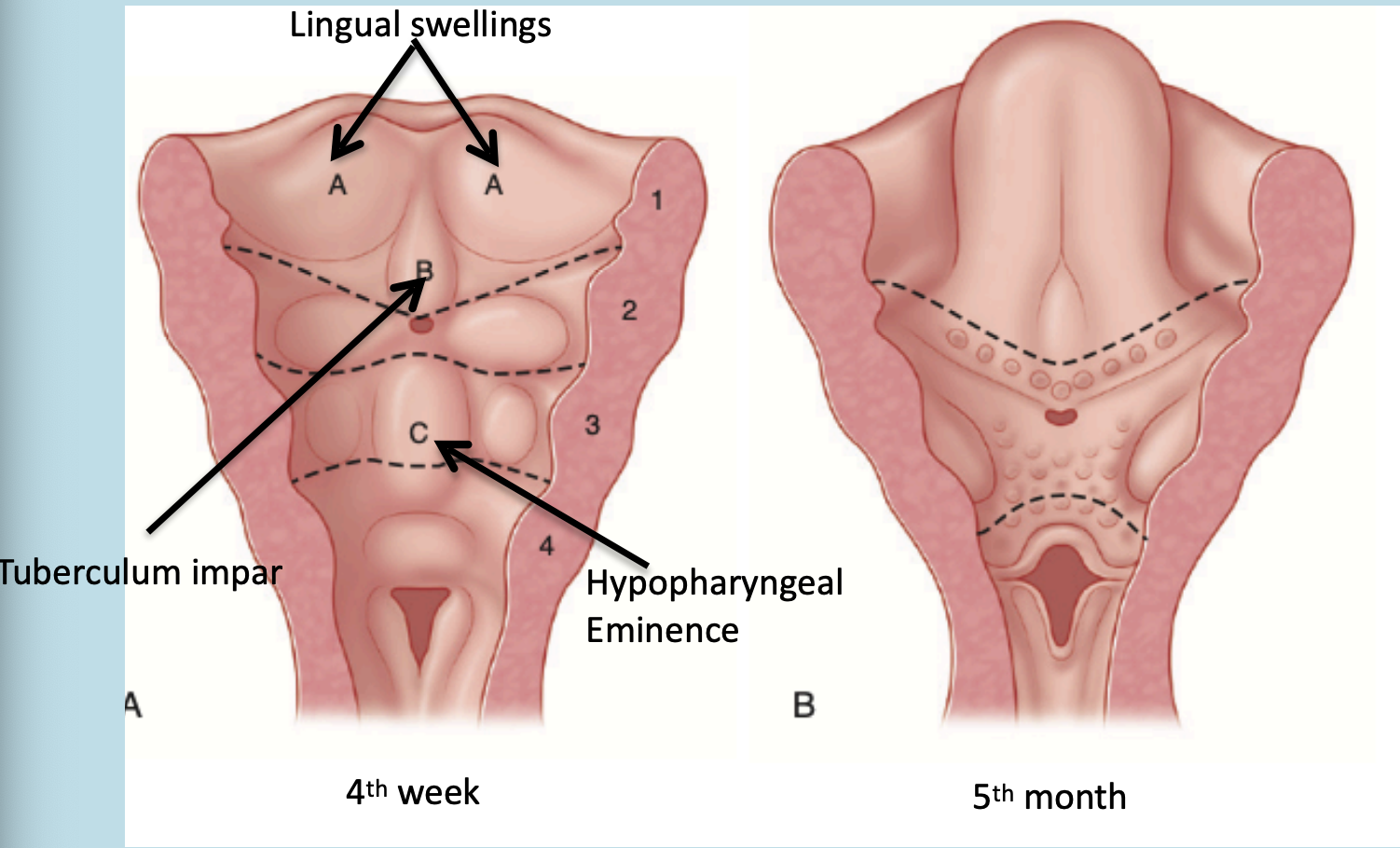
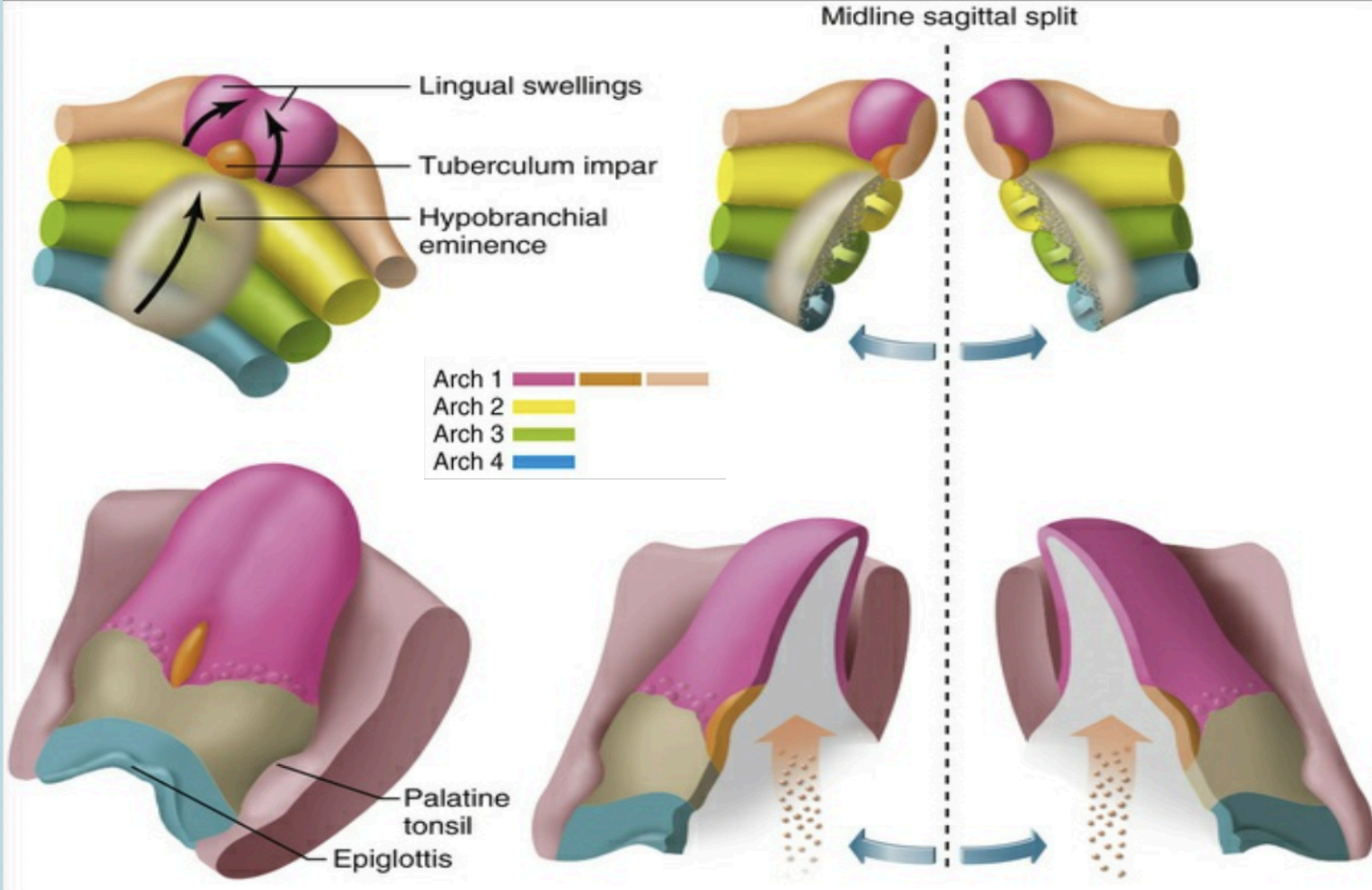
The lingual swellings, together with the tuberculum impar, which arise from the first arch, will form the anterior two thirds of the tongue. The hypobranchial eminence overgrows the second arch. Final disposition of the tongue and the relative contributions of the first to fourth arch. The arrow depicts the route of incoming occipital myotomes that form the tongue muscle.
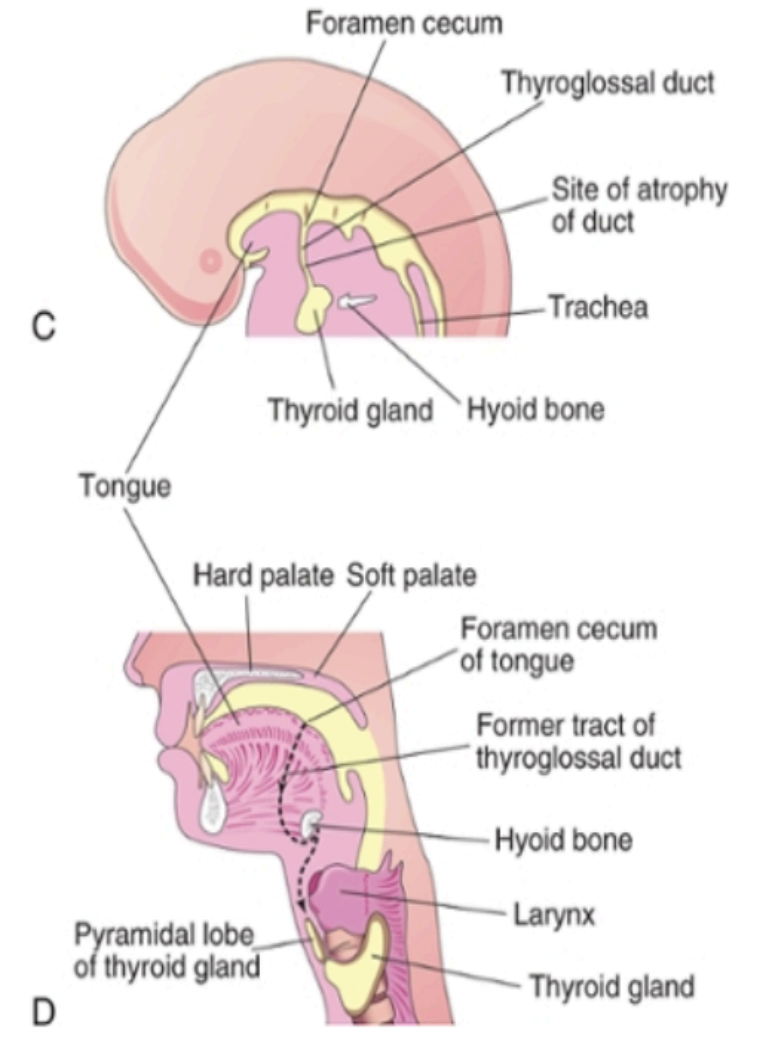
Development of the thyroid:
The thyroid gland is the first of the body’s endocrine glands to develop, on approximately the 24th day of gestation from the primative oral cavity.
The thyroid originates from two structures: The primative phaarynx and neural crest
It begins at the foramen cecum, located between the tuberculum impar and copula (tongue-forming structures).
A thyroid diverticulum (tube-like outgrowth) forms from the foramen cecum and elongates downward as the thyroglossal duct, passing in front of the hyoid and thyroid cartilage.
By the 5th week, the duct bifurcates to form the two lateral lobes of the thyroid and the isthmus.
During migration, the thyroid remains temporarily connected to the tongue by the thyroglossal duct.
Neural crest cells
The band of cells at the outer most edges on neural plate. They present on the dorsal aspect of the neural tube. They migrate from the ectoderm to mesoderm to form the connective tissue called the ectomesenchymal cells.
They give rise to:
Connective tissue of the craniofacial structures including bone, cartilage, ligament
Connective tissue of lacrimal and salivary glands
Dental structures (enamel is from the surface ectoderm but the signal for the stimulation is from the ectomesenchyme )
Connective tissue of thyroid, parathyroid and thymus
Tunica media of the outflow tract of the heart and the great vessels
Dental nomenclature and notation
Anatomic parts of the tooth include the apical foramen, cementum, pulp, dentin, and enamel
There are 2 types of dentition that exist in humans:
Primary dentition
2 Incisors - 1 canine - 2 molars in each quadrant
20 deciduous teeth
Permanent dentition
2 incisors - 1 canine - 3 molars in each quadrant of the permanent dentition
32 permanent teeth.
There are four basic tooth types in permanent dentition:
Incisors (with a horizontal incisal edge)
Canines (with a single large pointed cusp)
Premolars (with two cusps of varying sizes)
Molars (with four or five cusps)
For anatomical position 5 components are required:
Position (maxillary or mandibular, upper or lower)
Side (right or left)
Relative position; (first, second, third or lateral, central), but this term is not used in case of canines!
Dentition (permanent or deciduous)
Tooth type (incisor, canine etc)
Example: lower right second permanent molar
Alpha numeric system:
The quadrants are denoted as UR, UL, LR, or LL
Tooth numbering system:
There are 3 tooth numbering systems:
Universal Numbering System
From 1 -32
Wildley used in the US
Palmer’s Notation (Zsigmondy cross)
Designated each tooth according to its location in the quadrant
Horizontal lines separates the maxilla from mandible and a vertical midline
Federation Dentaire internationale (FDI) /International Standard Organization/(ISO)
FDI/ISO system was introduced to provide a standard international system of coding teeth
Each quadrant is assigned a number
The teeth within each quadrant are then numbered 1-8.
The primary teeth are numbered 1-5
Tooth surface:
Each tooth has five surfaces according to its position in the arch:
Incisal /occlusal surface
Facial/vestibular (Labial/buccal) surface
Lingual /palatal surface
Mesial surface
Distal surface
Proximal
surfaces
Line and point angle
Point angle: junction of three surfaces
Line angle: Junction of two surfaces
Anatomical features of the teeth:
Cusp
A pointed elevation on the occlusal surface of a tooth
Mamelons
Small, rounded projection on the incisal edge
Cervical line
Also known as (CEJ). A demarcation separating the anatomical crown from root
Lobes
Centers of calcification during tooth development. All teeth develop from at least four lobes. Molars develop from 4 to 5 lobes
Ridge
A linear elevation on the surface of a tooth
Fissure or Groove
A long cleft between cusps or ridges
Cingulum
A bulbous convexity near the cervical region of a tooth
A pit
A small depression on the crown
Morphology of the pulp
Pulp cavity is divided:
Coronal
Pulp chamber - pulp cavity in the crown
Pulp horn
Radicular (pulp canal)
Pulp cavity
The pulp cavity is the inner portion of the tooth containing pulp, and connective tissue that is containing neuromuscular tissue. It is covered by dentin except at the apical foramen and is divided into pulp chamber in the crown and root canals in the root.
The pulp chambers in deciduous teeth are larger than the permanent.
Pulp space becomes smaller from the deposition of secondary reparative dentin which means that as a tooth ages, the pulp cavity decreases in size leading to a reduction in the overall volume of the pulp, which can affect tooth sensitivity and the ability to heal.
Pulp horn
A pulp horn is an accentuation of the pulp chamber directly under a cusp or a developmental lobe. Usually there is one pulp horn under each cusp and are closer to the outer surface.
The mesial pulp horns are usually higher than the distal horn
In younger people the pulp horns are wide but as they increase in age the pulp horns recede and pulp chamber becomes smaller
Pulp roof, floor, & canal orifice
Roof of pulp chamber
The roof of the dentin is covered by dentin occlusally or incisally
Floor of pulp chamber
The floor of the pulp chamber runs parallel to the roof near the cervical region of the tooth particularly in the dentin in the furcation area
Canal orifices
Canal orifices are openings in the floor of the pulp chamber leading into canal space
They are not separate structures but they continuations of the pulp space
Root canal
A straight root canal that extends the length of the root in uncommon
All canals are curved, but the degree of the curve is different. They can go from sharp curvatures, to gradual curvatures, or S shaped
Apical foramen
Apical foramen (major diameter) : Is the terminal region of the pulp which used to communicate with the peri-apical region
Apical constriction (minor diameter): The narrowest portion at the terminal end of pulp space
In young people the apical foramina is broader and the dentinal tubules are wider and regular
Lateral canals and accessory canals:
Lateral canals are located approximately right to the main canals, and they are usually in the body of the root rather than the base
The branch (es) from the main root are usually at the apical region from the root.
Delta formation:
Dela formation describes the process of when the primary or secondary canals are terminated (end) before reaching the apex so lateral canals start fanning out from that point to the end of the root surface
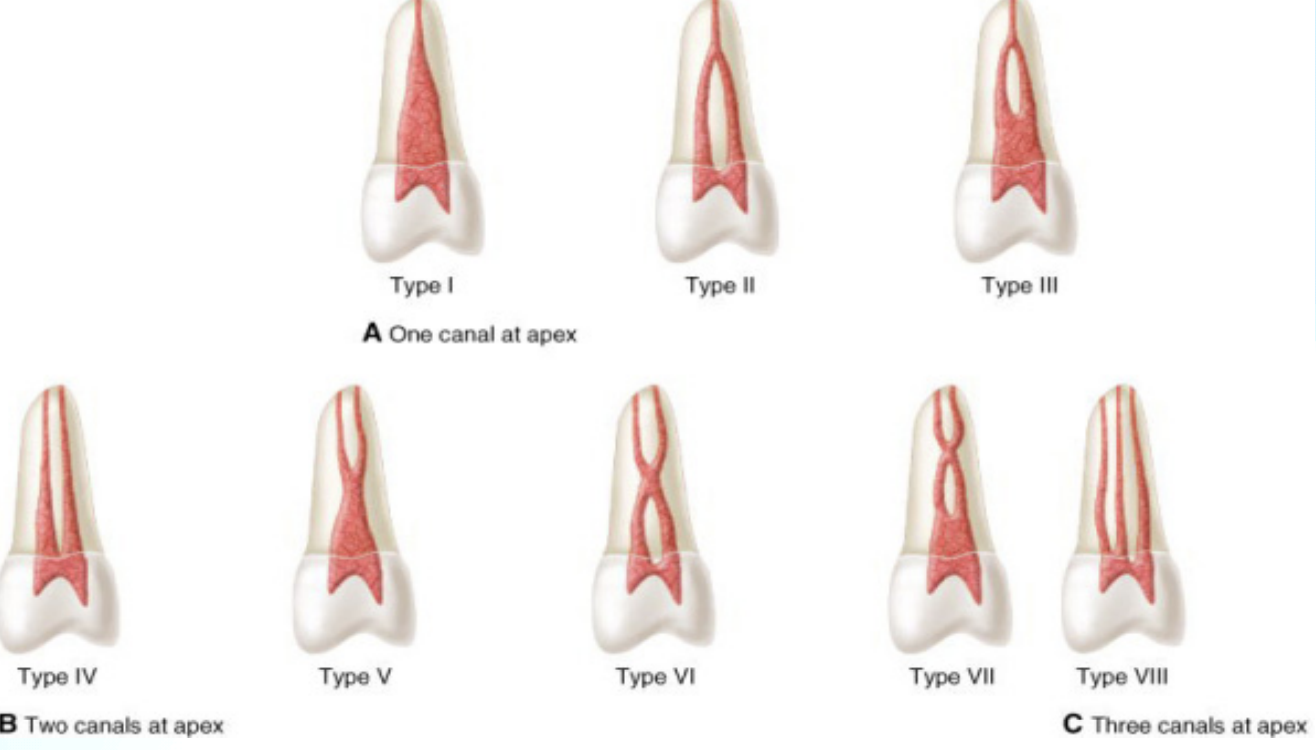
Classification of pulp cavity - vertucci’s classification
One canal at the Apex
Type 1: Single canal extending from pulp chamber to the apex
Type 2: Two canals leave the pulp chamber and join to form a single canal at the apex.
Type 3: One canal leaves the pulp chamber, divides into 2 canals, and then reconverts to form a single canal at the apex.
Two canals at the Apex
Type 4: Two separate canals leave the pulp chamber
Type 5: leaves pulp chamber as one, and then divides into 2 separate apical foramina
Type 6: Two separate canals leave the pulp, they merge as one in the middle body of the root but then re-divides short of the apex
Type 7: Single canal leaves the pulp chamber, divides into two, then rejoins in the middle, then finally re-divides into 2 canals short of the apex
Three canals at the Apex
3 separate and distinct canals extend from pulp chamber to the apex
Mandibular nerve
The mental foramen is usually found near the mandibular premolars and first molar:
33% of the time, it's between the first and second premolars
11% of the time, it's in line with the second premolar
56% of the time, it's behind the second premolar
Vertically, its position is:
22% of the time, it's above the root tips (apices)
15% of the time, it's at the level of the root tips
63% of the time, it's below the root tips
Occlusion
Occlusion is the contact relationship between the upper and lower teeth
Ideal occlusion is a complete, harmonious relationship of the teeth and all other structures, in an ideal occlusion, the teeth confirm to a specific pattern of occlusal contacts in the closure of the 32 permanent teeth. However the ideal relationship rarely exists
Centric occlusion and centric relation
Centric occlusion
Refers to the relationship between the mandibular and maxillary dentition during maximum occlusal contact
AKA maximum inter-cuspal position
Centric relation
Centric relation refers to the relationship of the mandible to the skull, more precisely the glenoid fossa.
It is less about the teeth contact but it is bone to bone relationship guided by the jaw muscles
Factors affecting development of occlusion
The factors affecting development of occlusion are branched out to general factors and localized factors:
General factors
Skeletal
Jaw relation to cranial bone
Alveolar bone to base
Muscle
Buccinators, tongue, lip posture, swallowing
Dental
Proximal contact
Etiology of crowding
Occlusal contact
Local factors
Presence of supernumerary teeth
Development of hypodontia
Labial frenum
Oral habits
What are the main factors involved in occlusion
Dental components
Upper & lower teeth, position, inclination, morphology
Temporomandibular joint components (TMJ)
Condyles, glenoid fossa, articular disc, tubercle
Neuromuscular system components
Muscle of mastication
Occlusion significantly changes from birth to adulthood
Dentition time periods:
No teeth (Edentulous):
from birth to 6 months old
There are no teeth visible in the mouth
Primary dentition only:
6 month to 2 years old is the eruption period
2 to 6 years old, all 20 primary teeth have erupted
Mixed dentition:
6 years to 12 years
Permanent and primary teeth are booth visible , leading to a transition period where children have both types of teeth present in their mouths.
Adult dentition:
12 Years onward
Development of occlusion
Age | Characteristic |
0-6 months | Gum pad contact |
3 years | primary dentition |
6 years | eruption of 1st permanent molars |
6-9 years | change of incisors |
9-12 years | change of canines and pre molars |
12 years | eruption of 2nd molars |
Development of occlusion
There are four stages
Pre-dental relationship - Gum stage
Birth to eruption of the first deciduous tooth
Usually primary mandibular central incisors at 6-10 months of age
Deciduous dentition stage
Time between the eruption of first primary tooth to eruption of the first permanent tooth
The arch and width is established by the 9th month
a localized spacing named as primate space is found between lateral incisor and canine in the upper arch and between lateral incisor and canine in the upper arch and between the canine and first premolar in the lower arch
Primary teeth are smaller overall and have a whiter enamel than the permanent teeth
There is spacing between them to allow for successor teeth to develop
These spaces are called primal spaces
The jaw to jaw relation is continuously changing during deciduous mention, this the occlusion
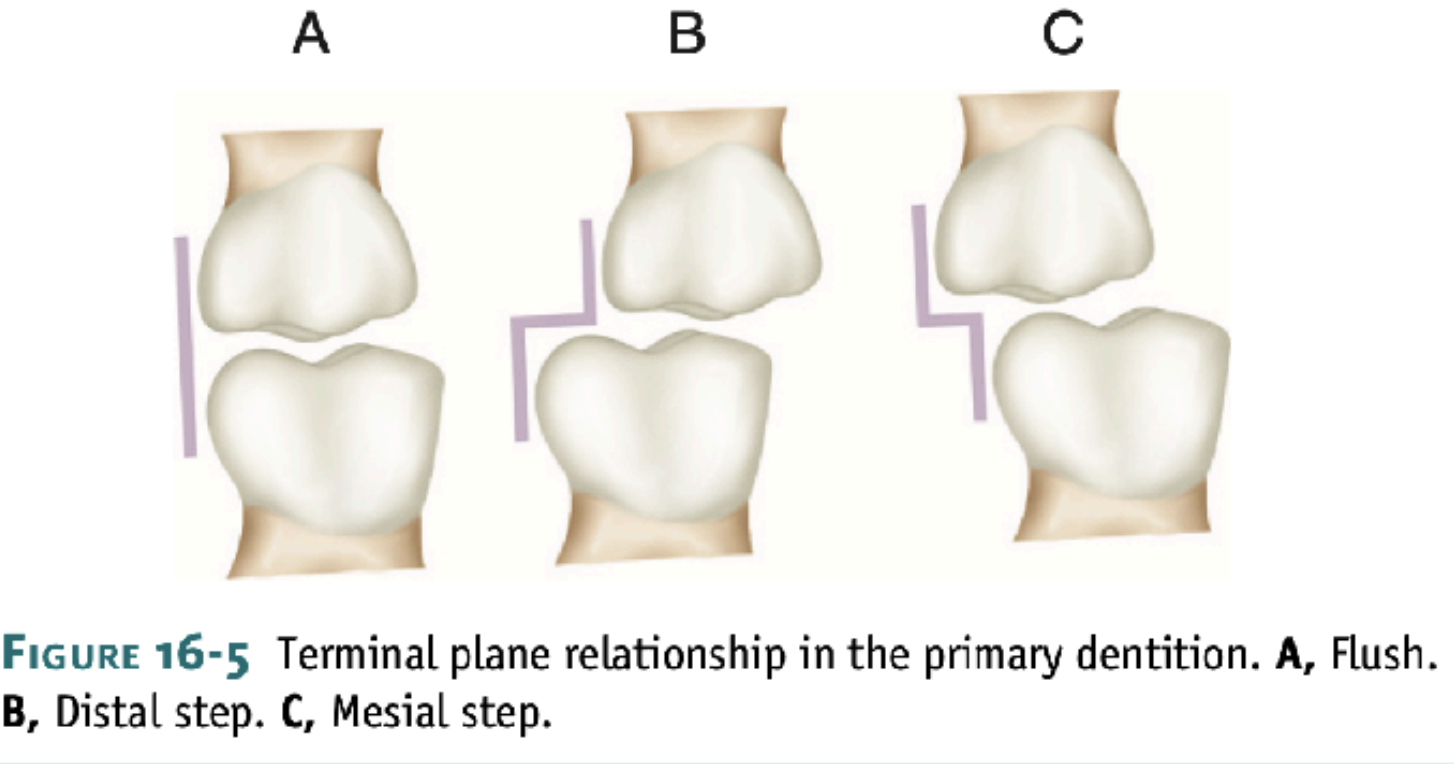
Primary molar relationship have been described as the: flush terminal plane, mesial step, and distal step.
The distal step in the deciduous dentition proceeded to
develop into a Class II molar relationship in the
permanent dentition.
The flush terminal plane may progress into a Class I
molar relationship or a Class II molar relationship.
The mesial step indicates a greater probability for a
Class I molar relationship.
Mixed dentition stage
Begins from 6 years
Mandibular teeth erupt before maxillary
Ugly duckling stage during this stage, which is a transitional spacing between the maxillary incisors appear due to the eruption of canines
Permanent dentition stage
Dental Arch Relationships:
Maxillary arch is usually wider than the mandibular arch.
Functional (supporting) cusps:
Maxillary lingual cusps
Mandibular buccal cusps
Nonfunctional (guiding) cusps:
Maxillary buccal cusps
Mandibular lingual cusps
Forces on posterior teeth should be directed along the long axis of the teeth.
Maxillary buccal cusps normally sit buccal (outside) to mandibular teeth.
Ideal Contact Criteria:
Contact occurs at:
Lingual cusp tips of maxillary posteriors
Buccal cusp tips of mandibular posteriors
Central fossae or marginal ridges of opposing teeth
Incisal edges of mandibular anteriors
Lingual surfaces of maxillary anteriors
Functional cusps:
Mandibular buccal
Maxillary lingual
Leeway space:
The difference between the sum of the mesiodistal crown widths of the primary canines and molars and that of their successors, the permanent canines and premolars
In the maxillary arch = 0.9 on each side, total 1.8 mm
In mandibular arch _ 1.7 on each side, total to 3.4 mm
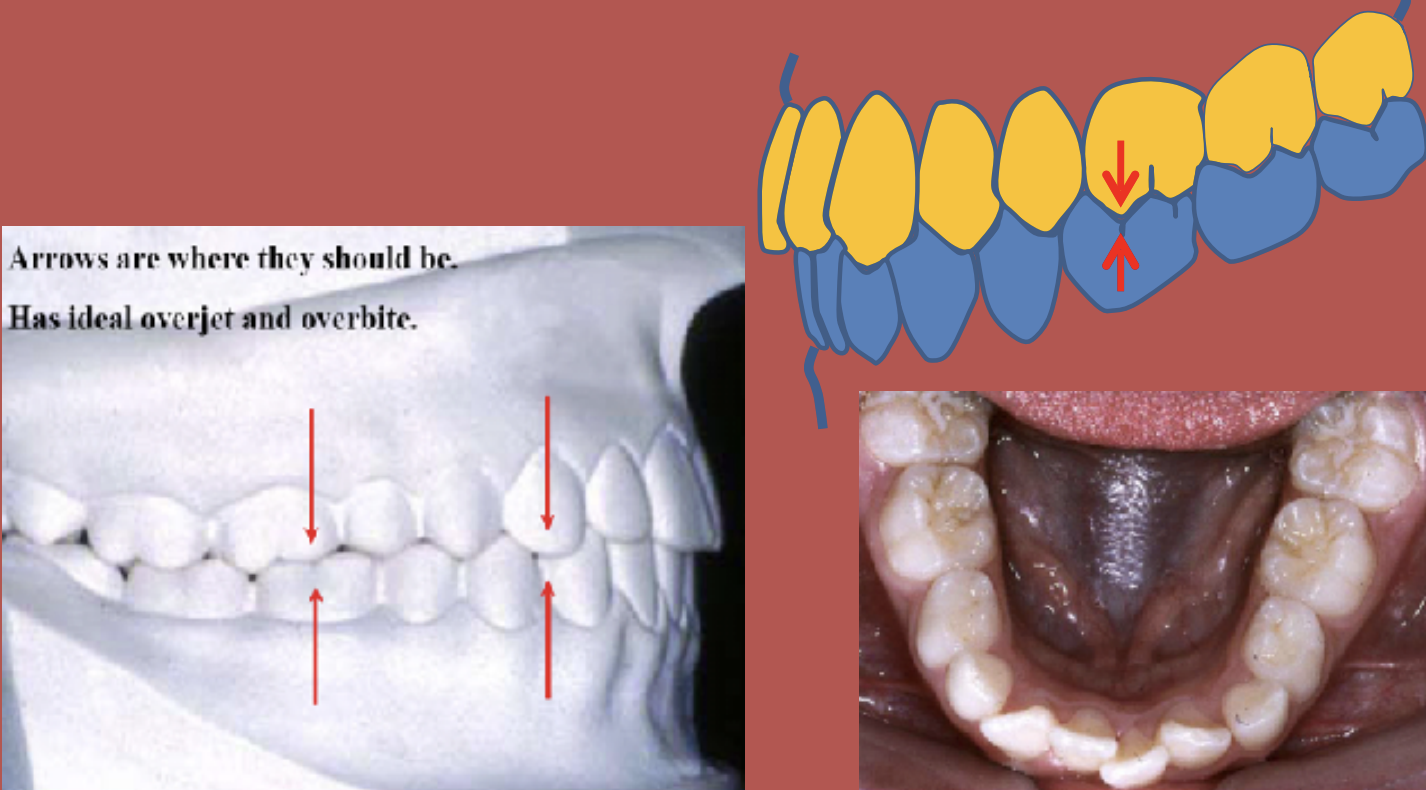
Overjet and Overbite
Overjet:
Horizontal measurement.
Distance between the lingual surface of maxillary incisors and the labial surface of mandibular incisors.
Measured when teeth are in centric occlusion.
Overbite:
Vertical measurement.
How far the maxillary incisors vertically overlap the mandibular incisors.
Normal range is about 2–3 mm in centric occlusion.
Terms related to Tooth - To - Tooth malocclusion
Angles classification:
By edward angle
Based on the relative position of the maxillary first molar
According to him the messiobuccal cusp of the upper first molar should rest on the mesiobuccal groove of the mandibular first molar.
Angles class-I malocclusion
a normal molar relationship exists but there is crowding, misalignment of teeth, cross bites, etc.
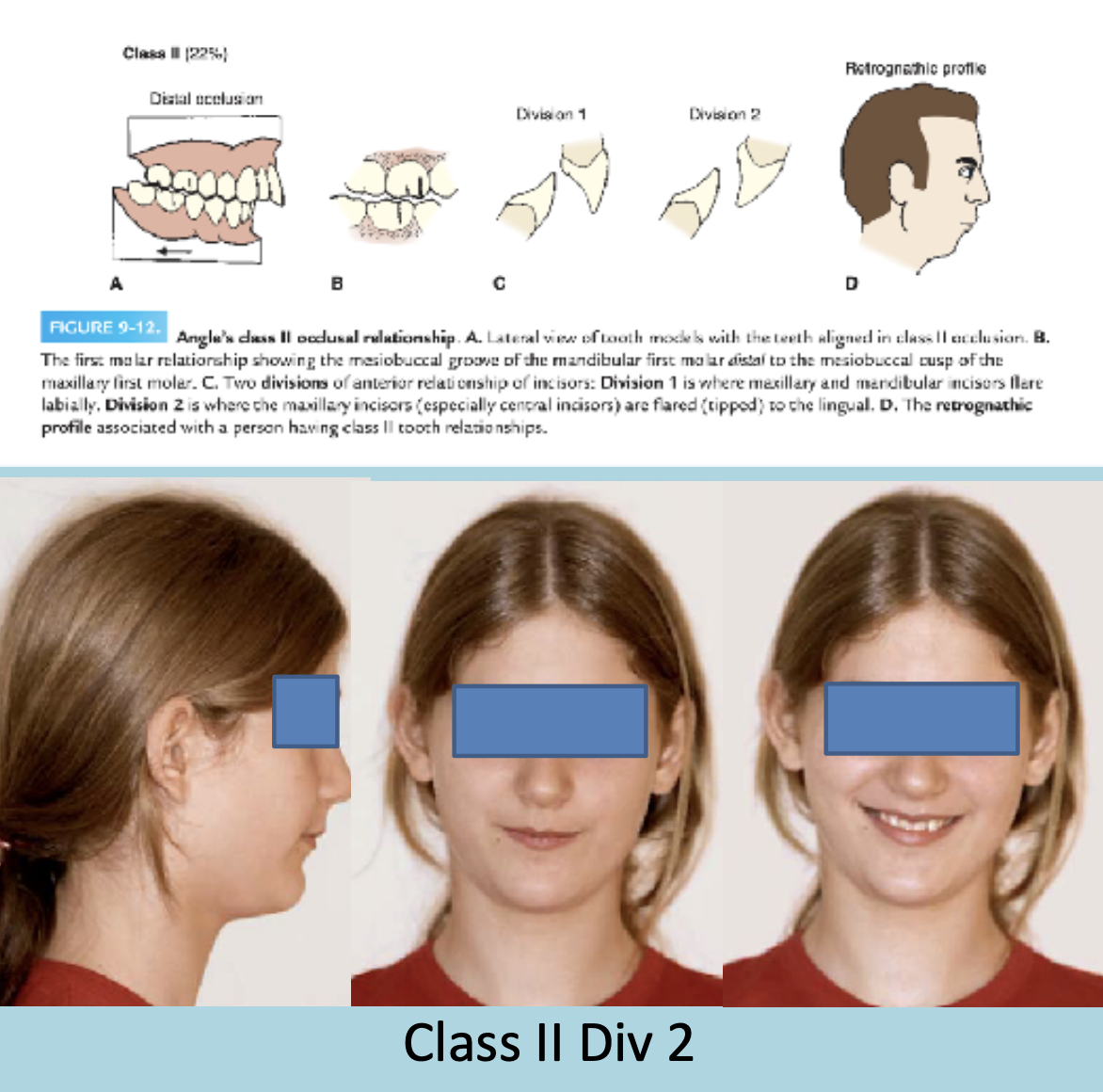
Angles class-II malocclusion
Class II is divided into two categories based on the position of the upper front teeth:
Class II Division 1:
The maxillary anterior teeth (front teeth) are proclined (tilted forward).
A large overjet is present (upper front teeth significantly ahead of lower front teeth).
Class II Division 2:
The maxillary anterior teeth are retroclined (tilted backward).
A deep overbite exists (upper front teeth excessively overlap the lower front teeth vertically).

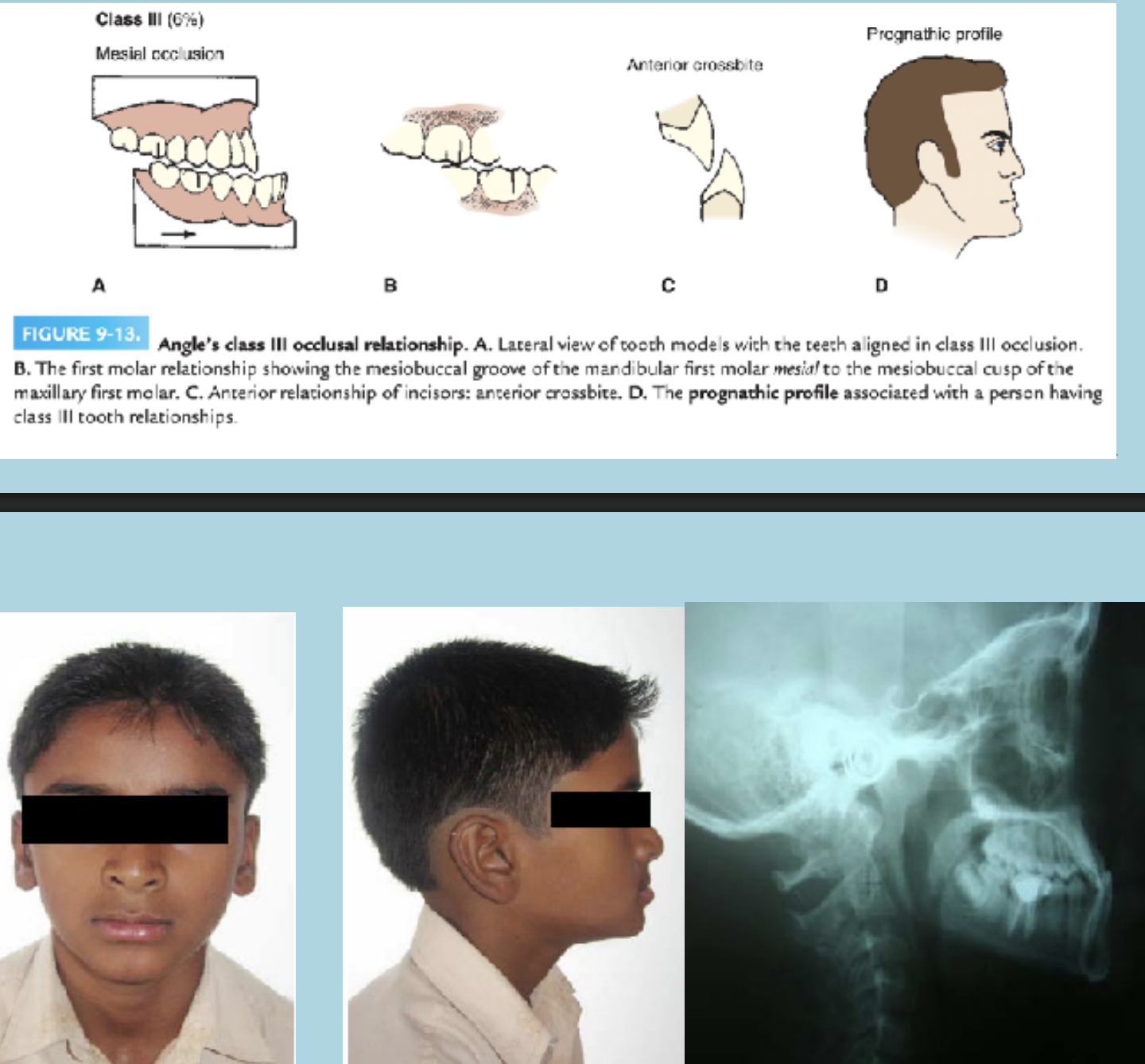
Angle’s class - III malocclusion
A malocclusion in which the buccal groove of the mandibular first molar is positioned mesially (toward the front) relative to the mesiobuccal cusp of the maxillary first molar when the teeth are in occlusion (bite).
This means the lower molars are ahead of where they should be in relation to the upper molars
TEMPOROMANDIULAR JOINT
The TMJ is a synovial bilatiral joint that permits the mandible to move as a unit with 2 functional joints (glinding and hinge movements) It is a ginglymoarthrodial joint since it is both a ginglymus (hinging joint) and an arthrodial (sliding/gliding) joint
The TMJ is the articulation of the temporal bones and the mandible
The temporal bone include the articular eminence and the articular fossa (AKA glenoid fossa)
Condyle of the mandible
Articular disc
Articular capsule
Histology of TMJ
Temporal bone:
It is a compact bone that is covered by the periosteum in the outer aspect , the articulating bony surface is covered by fibrocartilage
Mandible:
Mandible is formed by intramembranous ossification
Condyle of the mandible articulates with the temporal bone
condyle consists of compact bone, overlying cancellous bone and covered by periosteum
Fibrocartilage overlies the periosteum
The growth center is found at the head of each condyle
TMJ is a unique joint because the articulating surfaces are fibrocartilage instead of hyaline cartilage
Disc of the joint
Disc of the joint is located between the temporal bone and the condyle of the mandible
The disc appears cap shaped, and it divided the joint into two compartments
The two synovial compartments are:
Upper synovial cavity
Lower synovial cavity
The synovial membrane lines the capsule and produces synovial fluid that fills the 2 cavities
Disc attachments:
Posteriorly: to post - glenoid process (upper) and neck of condyle (lower)
Anteriorly: not to the temporal joint
Laterally and medially: to the condyle
Histologically the disc is composed of dense connective tissue, fibroblasts, and a few cells
The central part of the disc is avascular
With age the disc becomes thin
Joint Capsule:
Completely encloses the TMJ.
Surrounds articular eminence, fossa (superiorly), and condyle up to neck (inferiorly).
Two layers:
Outer: firm fibrous tissue with ligament support.
Inner: synovial membrane (thin connective tissue with nerves & blood vessels).
Synovial fluid: lubricates joint and nourishes avascular disc regions.
Muscles of mastication:
There are four muscles of mastication:
Later pterygoid
Medial pterygoid
Masseter
Temporal
These muscles do not work alone but as group with the tongue and muscles that support the movements of the mandible
Muscle | Nerve supply |
Masseter | Masseteric nerve (Anterior division) CN V3 |
Temporalis | Deep temporal nerve (aanterior division) CN V3 |
Lateral pterygoid | Mandibular nerve (CN V3) via lateral pterygoid nerve (from anterior division of CN V3 |
Medial pterygoid | Mandibular nerve (CN V3) via medial pterygoid nerve (from anterior division of CN V3 |
Blood supply to the joint
Mainly from the branches of:
superficial temporal artery
deep auricular artery
anterior tympanic artery
Ascending pharyngeal artery
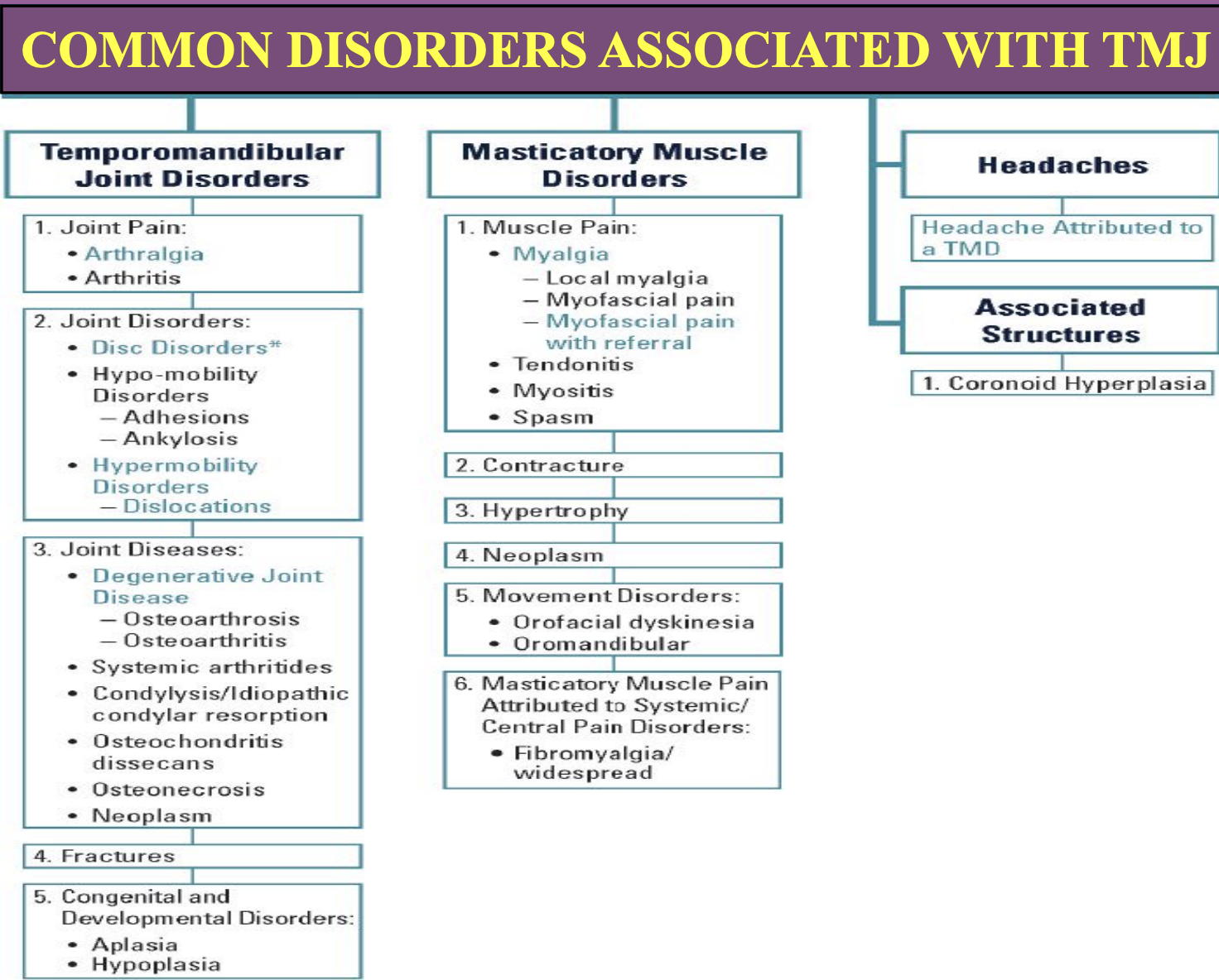
TMJ disorders:
Temporomandibular Dysfunction (TMD):
TMD occurs when there's a problem in the TMJ, muscles of mastication, or related nerves.
It causes chronic pain and reduced quality of life.
TMD is multifactorial, often involving multiple structures, making diagnosis and treatment challenging.
A psychological component is often present, requiring multidisciplinary care.
Treatment can be expensive, lengthy, and uncertain in outcome.
Four Major Primary Forces Affecting Tooth Position:
Intrinsic forces – from tongue and lips
Extrinsic forces – from habits (e.g., thumb sucking) and appliances
Occlusal forces – from contact between upper and lower teeth
Periodontal ligament forces – from supportive tissue around teeth
Equilibrium Theory:
Tooth position is maintained by a balance of intra-oral and extra-oral pressures.
Component | Intensity | Duration |
|---|---|---|
Occlusal forces | Very high | Very short |
Tongue/lip (swallow) | High | Short |
Tongue/lip (speech) | Low | Very short |
Tongue/lip (rest) | Low | Long |
Eruptive forces | Low | Long |
Jaw Movements – Working vs. Balancing Side:
Working Side (cheek side):
Mandible moves toward the cheek.
Condyle pivots in the socket.
Better supported and more stable.
Balancing Side (non-working side, tongue side):
Mandible moves toward the tongue.
Condyle moves downward and orbits.
Travels a greater distance, making it more prone to injury.
Curve of Spee (Anteroposterior Curve):
Begins at the tip of the lower canine, touches buccal cusps of mandibular posterior teeth, and extends to the anterior border of the ramus.
Ideally, the curve extends through the condyles.
Arc resembles part of a 4-inch radius circle.
Helps with normal protrusive movement of the mandible.
Curve of Wilson (Mediolateral Curve):
Connects buccal and lingual cusp tips of posterior teeth.
Mandibular arch: lingual cusps are lower due to inward tilt of lower teeth.
Maxillary arch: buccal cusps are higher due to outward tilt of upper teeth.
Supports chewing (mastication) by:
Allowing access to the occlusal table.
Preventing food from slipping off chewing surfaces (buccal cusps act as barriers).
Structure of Enamel, Dentin and pulp
Enamel:
enamel is highly mineralized tissue of ectodermal origin (96% mineral (calcium phosphate in the form of hydroxyapatite), 4% water)
It is very brittle but the underlying dentin provides some resilience, the physical, chemical and histological pattern on enamel allows it to withstand masticatory and other insults on the teeth.
Physical properties of enamel
Color: yellowish white to grayish white
Depends on translucency, degree of calcification, homogeneity
Yellowish enamel is more translucent, better calcified and homogenous, while, Grayish enamel is opaque, less calcified and less homogenous)
Thickness: It is thick at the incisal edge and cusp tip of molars and premolars (2-.25 mm) and it ends cervically as a knife
Hardness: It is the hardest calcified tissue in the human body because of the high calcification and crystal orientation.
It is greater at the outer surface and decreases at the DEJ.
It is greater at the cusp tip or incisal edge and decrease at the cervical line
Brittleness: Although it is very hard, enamel is very brittle especially when it looses the underlying elastic healthy dentin
Permeability: Enamel acts as a semi-permeable membrane for certain ions from: the saliva to the outer layer of enamel, the pulp to the inner layer of enamel across dentin
Enamel structure:
Rod and Interrod Structure: Enamel organized into rods (prisms) and interrods, each rod surrounded by a rod sheath.
Rod Dimensions: Average diameter of 4-5 µm; keyhole formation with distinct rod heads and tails.
Crystallography: Hydroxyapatite crystals predominantly oriented along the longitudinal axes of the rods, contributing to structural integrity.
Enamel structural organization:
Striae of retzius: Dark lines from DEJ to surface; result from weekly enamel production rhythms or successive enamel layer deposition.
Cross striation: fine lines at 4 μm intervals across enamel rods
Bands of Hunter and schreger: It is an optical effect from varying orientations of enamel rod groups
Gnarled enamel: twisted enamel rods near the DEJ, especially at the cusp tips
Neonatal line: prominent line that separates the enamel before birth and after birth
Surface enamel: Hard, unique outer-layer, often no prism
Enamel Tufts: Branched projections from the DEJ to the enamel. It has high organic content and abrupt rod direction changes
Enamel lamellae: Thin structures extending from enamel surface to the DEJ. Resulting into developmental disturbances
Perikymata: Surface manifestation of the incremental lines
DEJ (Dentinoenamel Junction): Scalloped line with concavities toward enamel; enhances resistance to chewing forces.
Enamel cuticle (Nasmyth membrane): Thin membrane covering newly erupted teeth; resembles ameloblast basal lamina.
Enamel spindles: Extensions of odontoblastic processes into enamel at DEJ during early development.
Enamel formation
Organic matrix formation:
Each enamel rod is formed by 4 ameloblasts, and each ameloblast contributes to 4 rods
Tomes process forms the rod head, interrod enamel is formed by the proximal part of this process.
Mineralization (2 - step process):
Initial stage: enamel becomes 30% mineralized
Second phase: Additional minerals added, organic material and water removed, reaching 96% mineralization. crystals grow in width and thickness
Ameloblasts:
Derived from Inner enamel epithelium (IEE)
Secretes matrix proteins that support mineral deposition
Undergo a distinct life cycle with specific stages known as amelogensis
Stages of Amelogenesis
Morphogenic phase:
IEE cells are cuboidal/low columnar; define the crown shape
Separated from the dental papilla by the basement membrane
Organizing/ Pre-secretory phase:
IEE differentiation into ameloblasts
Nuclei shift, Golgi & RER increase, Tomes process begins to form
Basement membrane disintegrates, allowing contact with odontoblasts
Early Secretion of enamel proteins begins before membrane breakdown
Secretory stage:
High protein synthesis activity
Enamel proteins are secreted via tomes processes directly into dentin
Little delay between secretion and mineralization
Ameloblasts move away from dentin as initial enamel forms
Maturation stage:
No new crystals; the existing hydroxyapatite crystals grow larger
Ameloblasts now called post - secretory cells
Includes:
Transitional phase: Ameloblasts shrink and prepare for maturation
Maturation proper phase:
Ameloblasts remove water and organic material
~50% undergo apoptosis (25% in each phase)
Cells alternate between ruffle-ended and smooth-ended forms
Secrete enzymes to degrade organic matrix and reabsorb it
Calcium ions support active crystal growth
Protective stage:
After calcification, ameloblasts become cuboidal, forming the Reduced enamel epithelium (REE)
REE protects the tooth until eruption
Desmolytic stage:
REE produces enzymes that break down overlyig connective tissue, allowing tooth eruption
Dentin
Dentin is first deposited as a layer of pre-dentin (unmineralized matrix), Which contains a layer of collagen and non-collagenous components (which is similar to osteiod)
Dentin has an elastic quality that is important to the functioning of the tooth.
Dentin physical and chemical properties:
Color: Yellow in color
Hard: Harder than bone and cementum but softer than enamel
Permeability: Tubular structure makes them permeable.
Comprehensive strength is more, but tensile strength is less when compared with enamel.
70% inorganic, 20% organic, and 10% water
Collagen: Type I collagen
Pattern of dentin formation
Begins at bell stage in the dental papillar near the Inner enamel epithelium (IEE)
Spreads from cusp tip down to cervical loop
Root dentin forms later requiring hertwigs epithelial root sheath
Deposition rates very between each tooth
Dentin is formed continuously throughout life, causing gradual pulp chamber reduction.
Dentinogenesis
Odontoblasts originate from the ectomesenchymal cells of the dental papilla
Differentiation is guided by signals from the IEE
Cells elongate, develop organelles and align opposite to pre-ameloblasts
One daughter cell (Exposed to IEE signals) becomes an odontoblast while the other becomes a sub-odontoblast.
Mantle Dentin Formation
Occurs first after odontoblast differentiation.
Odontoblasts secrete Von Korff’s fibers (collagen bundles) toward IEE.
Later, they produce type I collagen fibrils, aligned parallel to future DEJ.
Odontoblast processes project into the IEE (forming enamel spindles), and matrix vesicles are also released.
Capillaries are found beneath forming dentin and later migrate between odontoblasts to support exchange; capillary endothelium becomes fenestrated.
Control of Mineralization
Mineralization starts in matrix vesicles containing phospholipid-seeded crystals.
Crystals grow and fuse, forming clusters.
A layer of organic predentin lies between odontoblasts and mineralized dentin.
Dentin proteins regulate mineralization.
Calcium ions enter through channels in odontoblast membranes.
Mineralization patterns:
Globular – rapid, irregular deposition
Linear – slower, more uniform deposition
Formation of root dentin
Compositionally different that of the coronal dentin
The collagen fibers in the mantle dentin are arranged in a different orientation
The degree of root dentin is also less, and the rate of deposition is slower
Types of dentin
Primary dentin:
Forms the major bulk of the tooth
Surrounds the pulp chamber, also called cicrumpulpal dentin
The outermost layer is mantle dentin, which is mineralized differently
Secondary dentin:
Develops after root formation is complete
Formed by ongoing activity of odontoblasts
Less organized tubules than primary dentin; may be irregular or unevenly deposited, especially in molars
Leads to pulp recession, which is important in restorative dentistry - especially in older patients where pulp horns recede and are less likely to be exposed
Teriatary dentin:
AKA reactive or reparative dentin
Produced in responce to stimuli (ex. caries, wear, dental procedures)
Only affected odontoblasts contribute to its formation
Structure varies with stimulus intensity and duration; often irregular and rapidly deposited
odontoblasts may get trapped, distorting the tubular patter
Collagen production may be reduced during this process
Pulp
Pulp is a soft connective tissue that supports the dentin, It contains blood vessels, nerves, immune cells, and forms the dentin via odontoblasts.
Four zones of the pulp:
Odontoblastic zone:
At the pulp periphery; contains odontoblasts that line the chamber and extend processes into dentin
Cell-free zone (of weil)
Just below odontoblasts; has few cells, but nerve fibers from the plexus of raschkow pass through
Cell-rich zone
Contains fibroblasts, undifferentiated mesenchymal cells, immune cells, and fibers
Pulp core
Central region; rich in blood vessels, lymphatics, and nerves, along with ground substances like glycosaminoglycans
Odontoblasts
line the periphery; more columnar and active in the crown, cuboidal in the middle, and become flattened with age
Secretes dentin; the processes extend into dentinal tubules
connected via gap, tight junctions, and desmosomes
Golgi faces the dentin; nucleus has multiple nucleoli for protein synthesis
Processes contain microtubules, no major organelles; surrounded by dentinal fluid.
Pulp cells
Fibroblasts: Most numerous, active in young pulp, produces collagen and ground substance
Ectomesenchymal (Undifferentiated) cells: Can be become odontoblasts or fibroblasts in response to stimuli
Macrophages, lymphocytes, dendritic cells: Part of the immune defense
Vascular & Nerve Supply
Enter/exit via the apical foramen (also via smaller accessory foramina).
Arterioles occupy the center, branch toward the periphery, with capillary beds beneath odontoblasts.
Pericytes regulate blood flow.
Nerves follow arterioles and form the plexus of Raschkow in the cell-free zone (coronal pulp only).
Plexus includes myelinated and unmyelinated fibers, with sympathetic and sensory innervation.
No nerve plexus in root pulp.
Development of teeth (Odontogenesis)
Around the 6th week of development, the primitive oral cavity (AKA stomadeum) is lined with ectoderm.
This lining gives rise to primary epithelium bands, which are horseshoe-shaped bands that appear around the 37th day of development, they is one for each jaw.
The primary epithelium bands are separated into 2 subdivisions:
Dental lamina: Grows deep into the mesenchyme
Marks the spots where dental arches are.
Marks where the future deciduous teeth are going to grow in
Vestibular lamina: Cells grow large rapidly and then degenerate to form a cleft that will becomes the vestibule of the oral cavity.
The tissue below the ectoderm has specialized cells known as neural crest cells which help with guiding development.
The basement membrane seperates the the epithelium and the mesenchyme
Tooth development: stages
Bud stage
Epithelial ingrowth into ecto-mesenchyme
Cap stage
Further epithelium growth
Bell stage
Histo- and morpho- differentiation
Appositional stage (mineralization)
Formation of dentin and enamel of crown
Root formation
Formation of dentin and cementum of root
Eruption
Tooth development - Dentition and stages
Primary dentition: develops during prenatal period (20 teeth)
Permanent dentition: develops as the jaw grows and matures (32 teeth)
Mixed dentition: period between these 2
Bud stage:
The dental lamina grows and starts to push down into the mesenchyme which then creates tooth buds which are early shapes of future teeth.
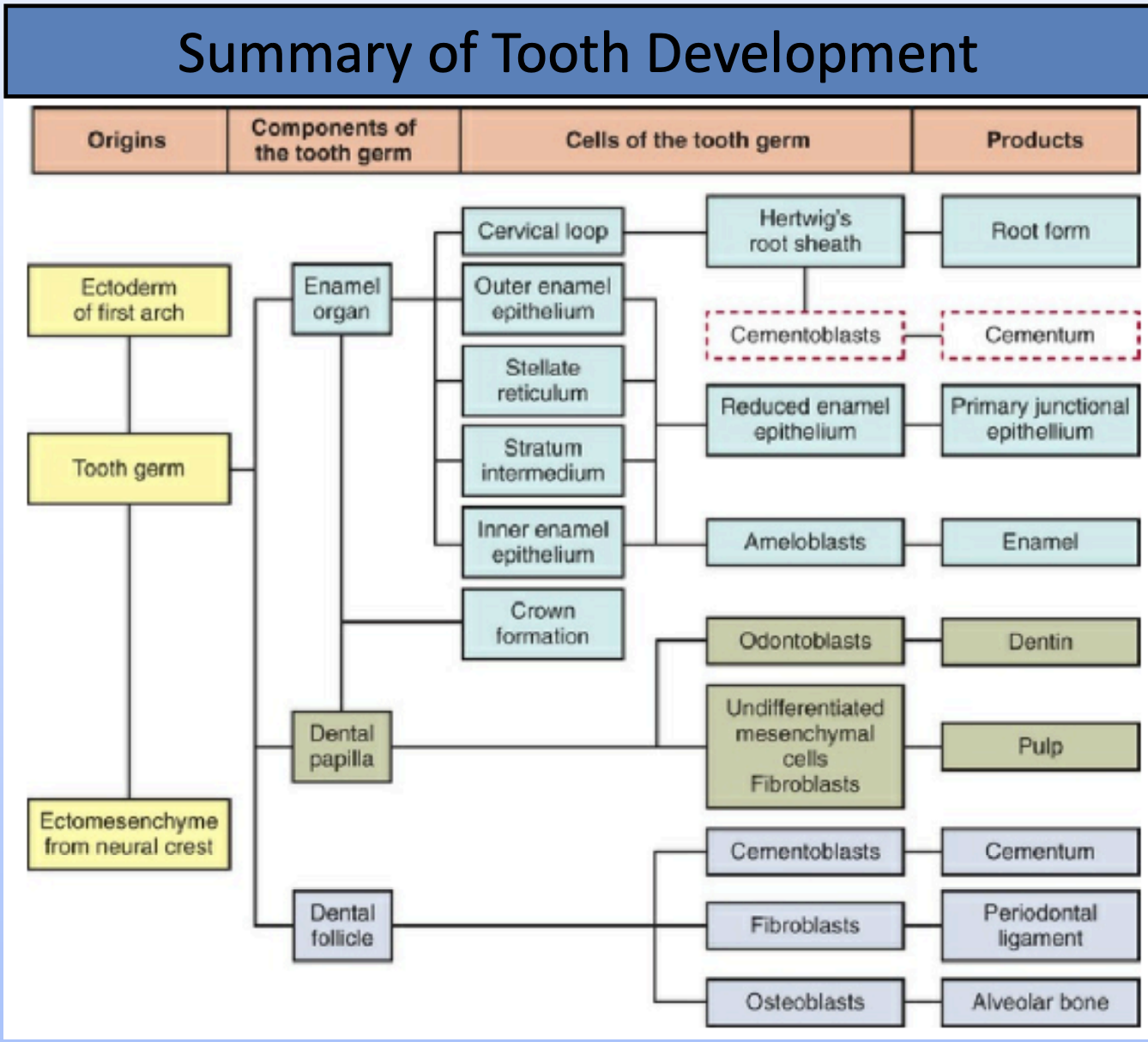
Each tooth bud becomes the enamel organ, and the tissue surrounding each tooth bud helps form; the dental papilla, and dental sac
Dental papilla (inside): forms the dentin and pulp
Dental sac (outside): Help form the supporting structures of the tooth like cementum, periodontal ligament, and alveolar bone.
Cap stage:
The oral epithelium continues to grow into the mesenchyme.
The tooth bud grows unevenly and creates a cap-like shape which will then become the enamel organ — Which will produce the future enamel
A depression in the enamel organ will form, which will attract dense mesenchymal cells — this will form the dental papilla which will form the dentin and pulp (mesenchymal origin)
The basement membrane separating the enamel rogan and the dental papillae will become the future dentinoenamel junction (DEJ)
The surrounding mesenchyme condenses to form the dental sac (or follicle) which will help developing structures
The enamel organ, dental sac, and dental follicle all make up the tooth germ
Cap stage ends as the tooth starts morphodifferentiation (shape change) as it moves on to bell stage
Bell stage:
During bell stage histo-differentiation (cell specialization) and morpho-
differentiation (shape change) continue
The cap stage takes a bell like-shape and produces 4 types of cells within the enamel organ
Inner enamel epithelium
Becomes Ameloblasts that will produced enamel
Outer enamel epithelium
Provides protection
Stellate reticulum
Star shaped cells, that will support with enamel productio
Stratum intermedium
Flat / cuboidal cells that will support enamel production
The inner enamel epithelium and outer enamel epithelium are connected by a cervical loop or the curved rim of enamel organ
The dental papilla also undergoes differentiation and produces 2 types of cells:
Outer cells of dental papilla
Forms dentin-secreting cells
Central cells of the dental papilla
Forms pulp
Under the basement membrane there is an accelular zone where the first enamel proteins will be laid down
The dental sac (follicle), which covers everything, increases in collagen content and will later form the cementum, periodontal ligament, and the alveolar bone
The dental lamina breaks down into clusters and seperates the oral epithelium from the developing tooth.
The IEE folds, and the future shape of the crown can be seen
Cap and bell stages with permanent teeth
While primary teeth are in bell stage, permanent teeth have started forming, Their tooth buds appear as offshoots from the dental lamina—called the successional dental lamina.
The developing teeth are called as successor teeth
Appositional stage:
Enamel, dentin, and cemeuntum begin to form.
They first start as soft matrix
This matrix will be the framework for future calcification
Maturation stage
Calcification is completed
Ameloblasts
Form from IEE, which become more columnar
They differentiate into pre-ameloblasts
These pre-ameloblasts will signal to the dental papilla to differentiate into odontoblasts
Odontoblasts
Form from dental papilla mesenchyme after pre-AB appear
Start dentin formation (dentinogenesis)
Dentinoenamel Junction
After dentinogensis the basement membrane between the pre-ameoloblsts and odontoblasts break down
This allows for contact causing pre-ameloblasts to become mature ameloblasts, which starts enamel formation
When dentin and enamel meet the BM mineralizes making the Dentino-enamel junction
Mineralization is when enamel and dentin harden, they are distinct for each type of tissue
Tooth Development Timetable
Primary teeth: Begin forming at 6–8 weeks of embryonic life.
Successional permanent teeth: Start developing from 20 weeks in utero to 10 months after birth.
Permanent molars: Develop from 20 weeks in utero (first molars) to about 5 years old (third molars).
Root formation and root dentin
Root formation begins after the crown is fully formed
It starts in the cervical loop (where IEE and OEE meet)
The cervical loop grows into the dental sac and develops into Hertwigs Epithelial Root Sheath (HERS)
HERS shapes the root and signals outer dental papilla cells to become odontoblasts, which make root dentin.
HERS does not have stellate reticulum or stratum intermedium, so it cannot make enamel.
After dentin is laid down, HERS and the BM disintegrate.
The root is made of dentin and cementum.
Root formation in multirooted teeth:
All teeth start with a single root trunk
Posterior teeth (Molars and premolars) Divide into 2-3 roots
This division happens due to uneven growth of hertwigs epithelial root sheath (HERS)
Periodontal ligament
Mesenchyme from the dental sac condenses to form the PDL near the newly formed cementum
The PDL fibers attach to both cementum and alveolar bone
Remnants from the the disintegrated HERS becomes the new epithelial cells rests of malassez
They later may develop into radicular cysts
Cementum and radicular pulp formation
Cementogenisis begins after HERS breaks down, exposing root dentin and dental sac cells, these cells breaks down to form cementoblasts that lay down cementoid.
Once cementoid mineralizes it becomes cementum
The junction between cementum and dentin is called the dentinocemental junction (DCJ).
At the same time, central cells of the dental papilla form the pulp
Tooth Type Determination (Patterning of the Dentition)
This process decides what type of tooth (incisor, canine, molar) forms where in the jaw.
Some animals have teeth that are all the same shape (homodont), but most mammals have different types (heterodont).
Two Main Theories:
Field (Code) Model
This model suggests that specific genes (homeobox genes) are turned on in certain jaw areas, deciding tooth type.
Example:
Msx-1 and Msx-2 are active in regions where incisors and canines will develop.
Dlx-1 and Dlx-2 are active in areas where molars will form.
These gene patterns help "code" the location and shape of each type of tooth.
Maxillary sinuses
Paranasal sinuses
There are four pairs of paranasal sinuses: maxillary, frontal, ethmoid, and sphenoid
They are air filled, mucous lined spaces, located in the maxillofacial region and skull centered on
They communicated with the nasal cavity
Maxillary sinus
AKA antrum of highmore
It is a pneumatic space that is lodged inside the body of the maxilla
It communicates with the environment by medial nasal meatus and nasal vestibule
Maxillary sinus embryology
It is the only sizable paranasal sinus that is present at birth
First sinus to develop in the second month of IUL
it is located in between the oral cavity and orbital floor
Enlarges via pneumatization, reaching adult size by the eruption of first teeth
Enlarges due to facial growth, slows down during puberty but continues throughout life
Enlargement of the sinus is associated with overall enlargement of facial skeleton, including; jaws, which provide space in the jaw for growth & eruption of teeth.
The adult maxillary sinus is pyramidal in shape
Anatomy of maxillary sinus
Varies in shape, size, and position based on different individuals and sides
Pyramidal shape with:
Base: Lateral wall of nasal cavity
Apex: Points directly to zygomatic process of maxilla
Drainage: Via maxillary ostium into middle nasal meatus through semilunar hiatus
Walls:
Anterior wall: Facial wall of the maxilla
Posterior wall: Infraorbital surface of maxilla
Superior/Roof: Floor of the orbit
Inferior/Floor: Alveolar process of the maxilla
Functions of maxillary sinus
Lightens the skull
Adds resonance to voice
Regulates air pressure during respiration
Produces lysozomes for anti-bacterial protection
Innervation & blood supply
Arterial supply: Infraorbital branch of maxillary artery, sphenopalatine, greater palatine, and posterior alveolar artery
Innervation: branches of maxillary artery -anterior, posterior, middle. Superior alveolar nerve, greater palatine nerve
Lymph drainage: Submandibular lymph nodes.
Histology – Maxillary Sinus (Key Points):
Lined by Schneiderian membrane (bilaminar):
Ciliated pseudostratified columnar epithelium (facing sinus)
Subepithelial layer with periosteum
Contains basal cells, non-ciliated columnar cells, goblet cells (mucus), and immune cells (lymphocytes, mast cells)
Ciliary beating moves mucus toward nasal cavity
Mucus blanket is essential for ciliary function
Clinical consideration/pathology
Close the first molar root - poses a risk to dental sinus communication
Common issues:
Inflammatory diseases
Cysts, odontogenic infections
Tumors and neoplasia
Trauma
Congenital anomalies
Dental relevance:
Infections from premolars/molars can spread to sinus
Oroantral communication from traumatic tooth extraction
Root fragments may be displaced into sinus
Sinusitis can cause neuralgia (pain in posterior maxillary teeth due to nerve compression)
Implants near sinus require caution to avoid perforation
Eruption and shedding of teeth
Tooth eruption is the process from which the teeth move from the bone to functional positions in the oral cavity. Tooth eruption is a continuous process due to wear (Mostly occlusal) and jaw growth.
Functions begin after mastication
Phases of tooth eruption
Pre-eruptive phase:
Movement of tooth germs (crowns) from early development to crown completion
Ends with the start of root formation
Eruptive phase:
Begins with root formation
Moves to occlusal position in jaw
Has intra-osseous (within bone) and extra osseous (through soft tissue) stages
Post-eruptive phase:
tooth is functional
Maintains tooth position during jaw growth and occlusal wear
Pre-eruptive Tooth Movement:
Occurs within bony crypts before root formation.
Tooth germ enlarges, causing pressure → activates osteoclasts (resorption) and osteoblasts (bone formation), shifting the tooth.
Eccentric growth & remodeling guide direction of movement.
Teeth adjust position in response to changes in neighboring crowns and jaw growth.
Permanent teeth:
Develop lingual to primary incisors, later move apically.
Premolars form inside roots of primary molars and move outward.
Eruptive Tooth Movement:
Begins with root formation.
Moves the tooth occlusally/incisally toward the oral cavity.
Includes intraosseous (within bone) and extraosseous (soft tissue) phases.
Eruption rate: ~1–10 µm/day (intraosseous), ~75 µm/day (extraosseous)
It is a rhythmic, multifactorial process (genetic + environmental).
Stages of eruption
Root formation:
HERS proliferates
Root dentin and pulp form
Fibrous tissue increases
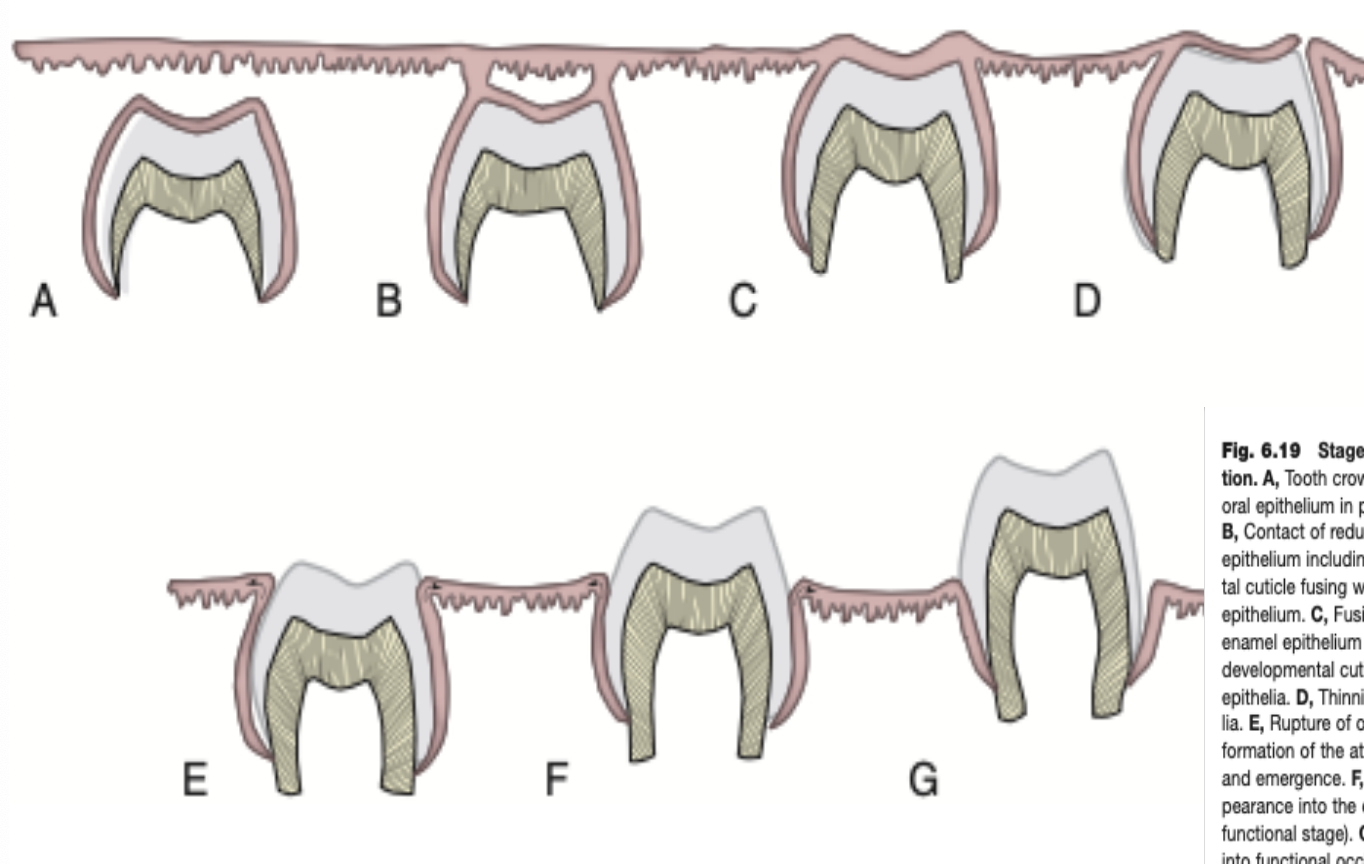
Movement:
Moves occlusally
REE fuses with oral epithelium
Penetration:
Crown tip breaks through epithelial layers
Enters oral cavity
Occlusal contact:
Eruption continues until tooth contact refuses crown
Marks functional position
Mechanisms or theories of Eruption
Root Formation Theory
Root growth pushes the crown occlusally.
Contradiction: Rootless teeth can still erupt; base fixation not always observed.
Bone Remodeling Theory
Similar to pre-eruptive movement: Pressure-tension changes cause bone resorption and formation, aiding eruption.
Vascular Pressure Theory
Pulsations in blood vessels may generate forces that help tooth movement.
Less widely supported.
Ligament Traction Theory (Most Accepted)
Periodontal ligament (PDL) or dental follicle traction pulls the tooth.
Dental follicle releases signals and chemoattractants for osteoclasts → bone remodeling aids eruption.
Supported by strong evidence: Defects in osteoclasts delay or prevent eruption.
✅ Most Accepted Theory: Ligament Traction due to its strong experimental and clinical support.
Histology During Eruption:
Tissue Degeneration: Nerves & blood vessels degenerate above erupting tooth.
Reduced enamel epithelium secretes enzymes (desmolysis) to clear eruption path.
Periodontal ligament (PDL): Becomes contractile, helps movement.
Myofibroblasts: Aid movement via contractile activity.
Macrophages: Break down tissues with enzymes.
Collagen fibers: Rapid turnover—attach, detach, and reattach as tooth erupts.
Gubernacular cord: Guides eruption of permanent (successional) teeth via gubernacular canal.
Post-Eruptive Tooth Movements:
Jaw Growth Adaptation (14–18 years): New bone forms at alveolar crest/base.
Occlusal Wear Compensation: Cementum is deposited at root apex (hypercementosis).
Mesial Drift: Teeth shift forward to maintain contact as interproximal wear occurs—guided by transeptal fibers.
Shedding of Teeth:
Definition: Natural loss of primary teeth for eruption of permanent ones.
Allows for stronger teeth and larger jaws to accommodate permanent dentition.
Factors Responsible for Tooth Resorption:
Bone Remodeling by Osteoclasts – Alveolar bone around the tooth reshaped.
Odontoclasts/Cementoclasts – Resorb dentin, cementum, and other dental hard tissues.
Macrophages – Resorb soft tissues around and inside resorbing tooth.
Pressure from Successional Teeth – Stimulates resorption in deciduous teeth.
Masticatory Forces – Contribute to early shedding by applying pressure.
Odontoclasts:
Function: Resorb hard dental tissues (like osteoclasts for bone).
Origin: Derived from TRAP-positive monocytes (from blood vessels).
Structure: Multinucleated, found in resorption bays.
Location: Seen on resorbing roots and crowns of deciduous teeth.
Teeth shed with intact pulp, despite external resorption.
Tooth eruption
Tooth resorption is mainly triggered by pressure from erupting permanent teeth.
Odontoclasts are activated at pressure sites to resorb hard tissues.
Cementum acts as a barrier—resorption starts when cementoblasts are damaged (by pressure, inflammation, or substances from reduced enamel epithelium).
Once damaged, odontoclasts attach via clear zone and begin resorbing.
Resorption is intermittent—can pause, and cementum may temporarily reform.
Ankylosis: Fusion of root cementum with alveolar bone prevents eruption (no PDL between them).
Salivary glands
Salivary glands are exocrine and merocrine glands of the oral cavity.
They are made up of glandular epithelial cells
Saliva aids in; digestion, mastication, speech, taste, and swallowing
Maintains oral health through antimicrobial action, cleansing, lubrication, tissue repair, and pH buffering.
The major salivary glands are:
parotid glands
Submandibular gland
Sublingual gland
The minor salivary glands are:
Von Ebner’s glands: Serous glands found beneath the sulci of circumvallate and foliate papillae on the tongue.
Glands of Blandin–Nuhn: Located on the ventral (underside) surface of the tongue.
Palatine and glossopalatine glands: Purely mucus-secreting.
Minor salivary glands are numerous and are located in the submucosa, they are not found within gingiva and anterior part of the hard palate
Salivary gland development
They develop between 4th-8th weeks of gestation
Parotid gland is the first to develop and the last to become encapsulated
All salivary glands follow similar pattern of development
There is an interaction between the epithelium and mesenchyme
Salivary gland development/embryology
Salivary glands develop from oral epithelium cell proliferation into the underlying mesenchyme
Stages:
Formation of small bud and long epithelial cord.
Mesenchymal cells condense around the bud forming glandular epithelium
Glandular morphogenesis begin which leads to full gland formation
Lumen forms within the branched structures
Cell differences:
Inner epithelial cells: become mucous of mucous secretory cells
Outer epithelial cells: differentiate into myo-epithelial cells
Structural development:
As parenchymal (glandular) components grow, connective tissue decreases.
Formation of fibrous tissue septa, connected to the capsule.
Blood vessels and nerves pass through these septa.
Key Signaling Molecules:
FGF (Fibroblast Growth Factor)
TGF (Transforming Growth Factor)
Sonic Hedgehog (Shh)
Structure of salivary glands:
The functional unit of salivary gland is acini, there are three types:
Serous
Mucous
Seromucous (mixed)
The salivary flow pathway:
Acini produce saliva.
Saliva flows into intercalated ducts.
Then into striated ducts (within lobules).
Finally, it reaches excretory (collecting) ducts, located between lobules (interlobular ducts).
Duct System (Branched Ducts)
Intercalated ducts → receive saliva from acini.
Striated ducts → modify and transport saliva within lobules.
Excretory ducts → carry saliva to the oral cavity; found between lobules.
Secretory cells - serous cells
Serous cells are one of two secretory cells
Serous cells:
8-12 cells surrounding central lumen
Pyramidal with broad base
Spherical nuclei
Has zymogen granules
Cell membrane is folder (to increase surface area of cell)
The cells are joined by tight g2ap junctions in addition to desmosomes and hemidesmosomes, these junctions allow passage of molecules and coordinate cells activate
Secretory cells - Mucous cells
Mucous cells secrete mucous
Mucous cells:
Have tubular configuration
Mucous cells are larger than the serous
Nucleus is flattened and compressed against the basal surface
Less prominent rough endoplasmic reticulum and mitochondria
Accumulate large amounts of mucus in the apical cytoplasm.
Have a large Golgi apparatus.
Organelles concentrated at the base of the cell.
Connected by intercellular junctions.
Lack intercellular canaliculi.
Myoepithelial cells
Myoepithelial cells are contractile epithelial cells, they forcibly express the content of glands.
1–3 cells surround each secretory unit and intercalated duct.
Have 4–8 actin- and myosin-rich processes.
Connected to secretory cells via desmosomes.
Myofilaments
Myofilaments form dark bodies along cell processes.
In intercalated ducts, cells are spindle-shaped with fewer processes.
Ultrastructure resembles smooth muscle cells.
Functions:
Support secretory cells.
Contract to help widen intercalated ducts.
Aid in rupture of acinar cells (to release secretion).
Intercalated ducts
They are small in diameter, and lined by small cuboidal cells
Nucleus located in the center
Well developed rough endoplasmic reticulum (RER), golgi apparatus and occasionally secretory granules
Myoepithelial cells present
They are prominent in salivary glands having a watery secretion (parotid)
Striated Ducts
Columnar cells
Centrally located nucleus
Eosinophilic cytoplasm
Prominenty striations
Some RER and some golgi, short microvilli
Modify the secretion
Hypotonic solution = low sodium and chloride and high potassium
Exceratory Ducts
Located in connective tissue septa between lobules of the gland
Larger than striated ducts
Lined by pseudo-stratified epithelium, that transistion to stratified epithelium the closer it gets to the oral muscosa
Goblet cells are present
Other cells include dendritic cells and nerve endings.
Connective tissue:
Capsule:
Encloses the gland and separates it from surrounding structures
Septa:
Extends inward from the capsule
Divides the gland into lobes and lobules
Carries blood vessels, excretory ducts and nerves
Connective tissue is composed of:
Cells: Fibroblasts, dendrititc cells, mast cells, macrophages etc…
Matrix: Proteoglycans, glycoproteins, collagen fibers and elastic fibers
Plasma cells: They are found near secretory units and ducts; produce IgA (sIgA) for saliva immunity.
Nerve supply of connective tissue:
Supplied by postganglionic nerve fibers of the Autonomic nervous system:
Parasympathetic: Preganaglionic fibers via facial nerve (VII CN) and glossopharyngeal nerve (IX CN) synapse in the submandibular and otic ganglia, that send their axons to the glands through lingual and auriculotemporal nerves.
Sympathetic: Preganglionic sympathetic fibers synapse in the superior cervical ganglion. Postganglionic fibers travel with arterial blood supply to reach the glands.
Inside gland lobules, nerve branches form plexuses of unmyelinated fibers near:
Arterioles
Ducts
Secretory end pieces
Neurotransmitters:
Sympathetic: Norepinephrine
Parasympathetic: Acetylcholine
Blood Supply of saliva
90% of saliva is water, requiring rich blood supply.
Arteries → arterioles → capillaries surround secretory units and ducts.
Capillary plexus exists around excretory ducts.
During max secretion, blood flow increases up to 15 times to support fluid filtration.
Saliva Formation
Primary Saliva:
Produced by secretory end pieces and intercalated ducts.
Isotonic, contains water and organic components.
Final Saliva:
Modified in striated ducts by electrolyte reabsorption/secretion.
Becomes hypotonic.
Macromolecular Component (Protein Synthesis)
Rough ER & Golgi abundant in secretory cells.
Process: Ribosomes → RER (protein synthesis & modification) → Golgi → secretory granules.
Exocytosis releases proteins (triggered by norepinephrine).
Endocytosis handles granule membrane recycling/degradation.
Age changes in salivary glands include :
fibrosis and fatty degenerative changes
presence of oncocytes (eosinophilic cells containing many mitochondria)
Oral physiology I
Introduction:
Calcium and phosphate are essential for bone and tooth formation in the body, with a (phosphate) 2:1 ratio in the body
Calcium phosphate forms the hard matrix of bones in the body, magnesium strengthens it
Both are absorbed by the duodenum, Calcium is excreted by feces and urine, Phosphate primarily urine
High calcium levels absorb phosphate to maintain balance
Function of calcium and phosphate:
Calcium: muscle contraction, blood clotting, building bone and teeth
Phosphate: Building bone and teeth, ATP and nucleic acid formation, fat/carbohydrate metabolism
Serum levels of Calcium and phosphate:
Calcium:
Normal serum levels: 9 to 10.5 mg/dL
Normal Ionized calcium: 4.5 - 5.6 mg/dL
Phosphate:
Children: 4-7 mg/dL
Adults: 3-4.5 mg/dL
Calcium and phophate levels and dietary requirements:
Calcium:
Adults: 500-800 mg
Pregnant women: 1500 mg
Lactating women: 2000 mg
Infants: 360 mg
Children: 800 mg
Dietary requirements: Milk, Milk products, Eggs, fish, vegetables, fruits, nuts
Phosphate:
Adults: 800 mg
Pregnant women: 1200 mg
Infants and children: 240 mg
Dietary requirements: Same as calcium, found in cereals and pulses
Calcium in bone and teeth
A bulk quantity of calcium is used for bone and teeth formation. They are the reservoir of calcium in the body .
Osteoblasts induce bone deposition and osteoclasts produce demineralization
Factors affecting calcium absorption
Inhibiting
High pH
Dietary fiber
Free fatty acid
Dietary phosphate
Promoting
Vitamin D
Parathyroid hormone
Low pH
Lactose
Amino acid
Regulating Factor | Target Cells/Tissue | Effect |
|---|---|---|
Parathyroid Hormone | Kidney and bone | Stimulates 1,25 Vitamin D formation and osteoclastic activity; increases circulating calcium concentrations |
Calcitonin | Osteoclasts | Inhibits osteoclast activity; lowers circulating calcium concentrations |
Vitamin D (1,25D) | Osteoblasts | Stimulates collagen, osteopontin, and osteocalcin synthesis; promotes differentiation; increases circulating calcium |
Bone (osteoclasts) | Stimulates osteoclast activity | |
Kidney | Stimulates calcium retention | |
Intestine | Stimulates calcium absorption |
Calcium Balance
Calcium balance is regulated by hormones—Parathyroid Hormone (PTH), Calcitonin, and Vitamin D—acting on three main sites: intestine, bone, and kidney.
These hormones help maintain plasma calcium levels by regulating calcium absorption, excretion, and mobilization.
If dietary calcium is low or in cases of malabsorption, calcium is drawn from bone to maintain blood levels.
Concept of Calcium Balance
Type of Balance | Description |
|---|---|
Positive Balance | Occurs in growing children (up to ~10 years); helps build skeletal mass. |
Zero Balance | Found in healthy adults; calcium intake equals loss. |
Negative Balance | Seen in elderly, especially in women with osteoporosis; calcium loss exceeds intake. |
Peak skeletal mass is reached between 25–30 years of age.
Aging causes mild calcium loss, but osteoporosis leads to significant bone calcium depletion.
Hypercalcemia
Definition: Plasma calcium level >11mg/dL
Causes:
Primary Hyperthyroidism
Hyperthyroidism
Sarcoidosis
Thyrodtoxicosis
Vitamin D poisining
Hypocalcemia
Definition: Serum calcium level < 8.8 mg/dL
< 8.5 mg/dL = Mild tremors
< 7.5 mg/dL = Tetany (life-threatening condition)
Causes:
Vitamin D deficiency
Hypoparathyroidism (primary, secondary)
Increased calcitonin
Calcium and Oral health
Pre-eruptive Effects:
Tooth mineralization begins at 4 months in utero and continues till 6–13 years.
Calcium deficiency during gestation and childhood affects tooth development.
Role in Periodontal Disease:
Adequate calcium improves healing and tooth stability in gingivitis.
Low calcium intake leads to worse periodontal and gingival disease.
Effect on Alveolar Ridge Resorption:
1g calcium daily for 12 months increased mandibular bone density by 12.5%.
Phosphate Homeostasis & Metabolism
Key Regulators:
FGF23, Vitamin D, and Parathyroid Hormone (PTH)
Mechanisms:
Regulation through intestinal absorption, bone storage/release, and renal reabsorption.
FGF23 (Fibroblast Growth Factor-23):
Produced by bone and connective tissue
Inhibits phosphate reabsorption in kidneys → causes phosphaturia
Reduces calcitriol (1,25-vitamin D) → lowers phosphate absorption from the gut
Phosphate Metabolism Response:
Condition | Response |
|---|---|
↓ Serum Phosphate | ↓ FGF23 → ↑ Renal phosphate reabsorption + ↑ Calcitriol → ↑ Gut absorption |
↑ Serum Phosphate | ↑ FGF23 → ↓ Renal phosphate reabsorption + ↓ Calcitriol → ↓ Gut absorption |
Hydroxyapatite
Composition: Ca₁₀(PO₄)₆(OH)₂ – a naturally occurring mineral form of calcium apatite.
Found in: Enamel, Dentin, Cementum, and bone
Makes up: ~50% of bone weight
Known for its osteoconductive and osteointegrative properties.
Enamel Characteristics
Hardest substance in the human body.
Composed of large HA crystals:
Thickness: ~25 nm
Width: 40–120 nm
Length: 160–1,000 nm
Mineralization Process
A lifelong process involving precipitation of minerals onto an organic matrix.
Collagen fibrils serve as a scaffold for calcium phosphate crystal organization.
Alkaline phosphatase enzyme aids this process.
Nucleation (formation of crystal centers):
Homogeneous: High local mineral concentration
Heterogeneous: Occurs with nucleating substances at lower concentrations
Theory | Key Idea |
|---|---|
Booster/Robinson's Theory | Alkaline phosphatase promotes mineralization |
Collagen-seeding Theory | Collagen initiates and organizes mineral deposition |
Matrix Vesicle Theory | First crystals form inside vesicles, grow, and burst to continue mineralization |
Tissue | Mechanism |
|---|---|
Bone & Dentin | Combination of matrix vesicle and heterogeneous mineralization |
Enamel | Heterogeneous mineralization only |
Demineralization: Loss of mineral ions from HA crystals.
Remineralization: Re-deposition of lost minerals into HA structure.
Permeability in dentin
Dentin permeabitlity refers to its ability to allow bacterial or chemical substances to diffuse across to the pulp.
Function: It plays a protective role for the pulp by regulating substance movement.
Aspect | Detail |
|---|---|
Variation in Permeability | Lowest at the Enamel-Dentin Junction (EDJ), highest near the pulp. |
Age-related Change | Permeability decreases with age due to physiological dentin sclerosis. |
Impact of Enamel/Cementum Loss | Exposed dentinal tubules act as pathways for irritants to reach the pulp. |
Increased permeability puts teeth at risk for:
Pulpal inflammation
Tooth sensitivity
Periradicular tissue irritation
Mechanism | Effect |
|---|---|
a. Appositional growth of intratubular dentin | Natural blockage of tubules |
b. Deposition of calcium phosphate crystals (e.g. Whitlockite) | Forms "caries crystals" ahead of demineralized zones |
c. Coagulation of plasma proteins (fibrin) | Blocks tubules beneath freshly cut cavities |
d. Pathological precipitations (minerals, collagen, bacteria) | Leads to tubule occlusion |
e. Smear layer formation during cavity prep | Blocks surface tubules temporarily |
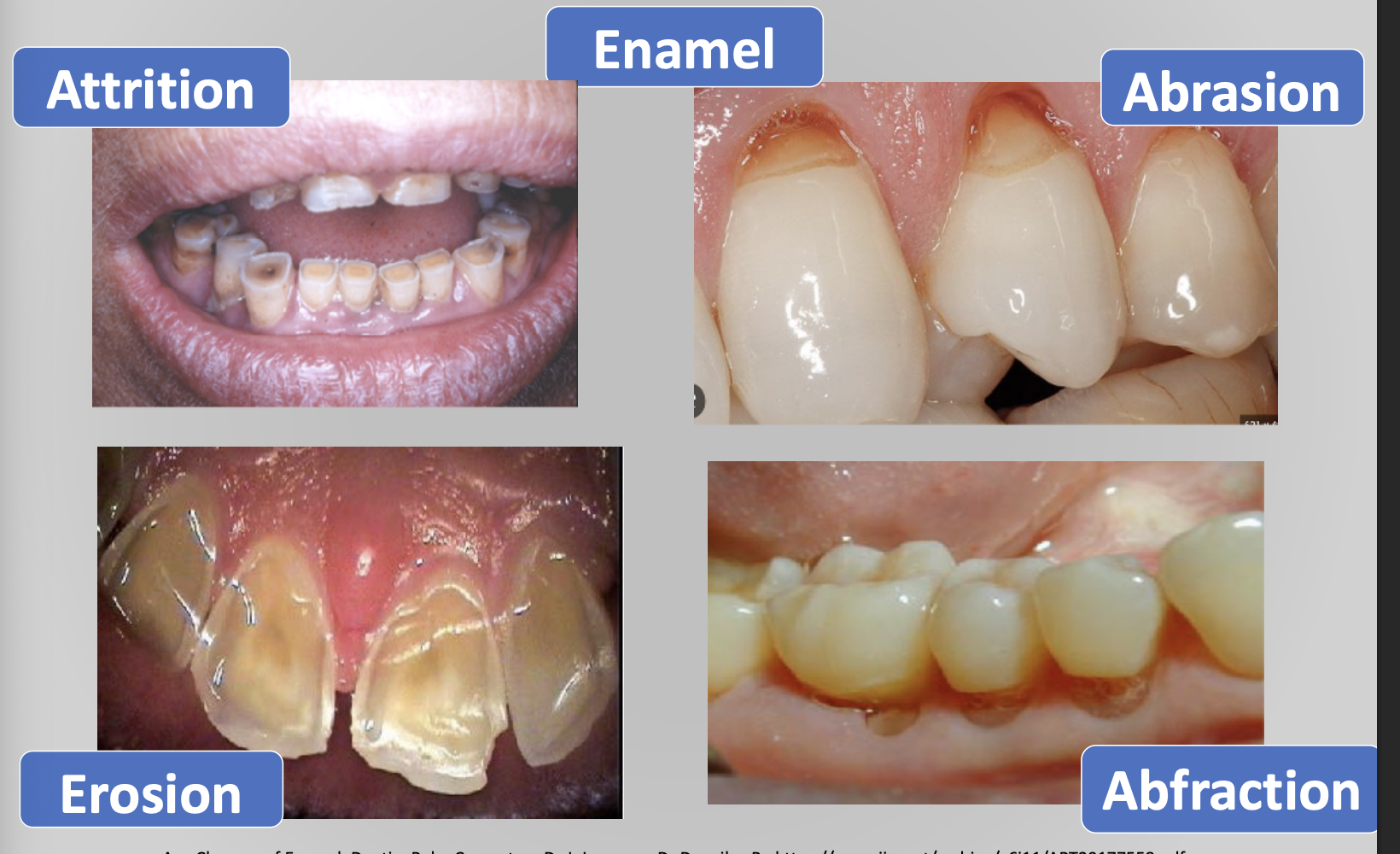
Age changes in enamel:
Attrition: Most notable age change in enamel, it is basically when there is wear of the occlusal surfaces and proximal contact points as a result of mastication. It is evidenced by a loss of vertical dimension of the crown and flattening of the proximal contour
Abrasion: pathological loss due to mechanical forces
Abrafaction: Biomechanical bending of teeth due to abnormal occlusal forces
Erosion: chemical insult to teeth without bacterial process
Age changes in dentin:
Reparative dentin: Formed in response to severe injury (abrasion, erosion, caries, or operative procedures) odontoblasts may die or survive depending on the severity of injury
Transparent or sclerotic dentin: Mostly in elderly people, especially in the roots. it reduces the permeability of the dentin
Age changes in Cementum:
Hypercementosis = Too much cementum
Cementum hypertrophy → Helpful overgrowth (makes teeth stronger)
Cementum hyperplasia →Useless overgrowth (not helpful)
Cementicles → Tiny hard lumps (calcium deposits) that form when tissue near the root breaks down
Permeability ↓ with age → Cementum becomes less porous, so fewer harmful things can enter
Nutrition & Oral Health – Key Points
Nutrition and oral health are closely connected.
Healthy oral tissues, saliva, and sense of taste all depend on proper nutrient intake.
At the same time, your oral health affects what foods you can eat — and that influences your overall nutrition.
Postnatal Growth of face and skull
Post-natal period:
Begin from birth to the end of adolescence
It is divided into:
Neonatal (birth - month 1)
Infancy (1 month - 1 year)
Childhood (1 up to 12 years)
Adolescence stage (13 -19 years age)
General Concepts of Growth and Development
Growth and development refer to sequential anatomical and physiological changes from prenatal life to old age.
Defined as a measurable change in shape, size, or structure (morphologic parameters).
The craniofacial skeleton grows through interactions of internal factors (like hormones and genes) and external stimuli (like soft tissue growth, dental changes, and mechanical forces).
Growth involves changes in:
Size
Shape
Position — to maintain correct alignment and function.
Facial growth is closely connected among tissues — each part influences and is influenced by the others.
No part of the face grows independently.