NURS 4581: Strokes
Cerebrovascular Disorder Overview
Definition: A cerebrovascular disorder indicates a functional abnormality of the central nervous system (CNS) due to disrupted blood supply to the brain.
Stroke in the U.S.: Leading cerebrovascular disorder and a major cause of serious long-term disability.
Statistics: Stroke has decreased to the 5th leading cause of death.
Types of Stroke
Categories:
Ischemic Stroke: 87% of strokes, caused by blockage of blood vessels leading to significant hypoperfusion.
Types of Ischemic Stroke:
Large artery thrombotic strokes (20%)
Small penetrating artery thrombotic strokes (25%)
Cardiogenic embolic strokes (20%)
Cryptogenic strokes (30%)
Others (5%)
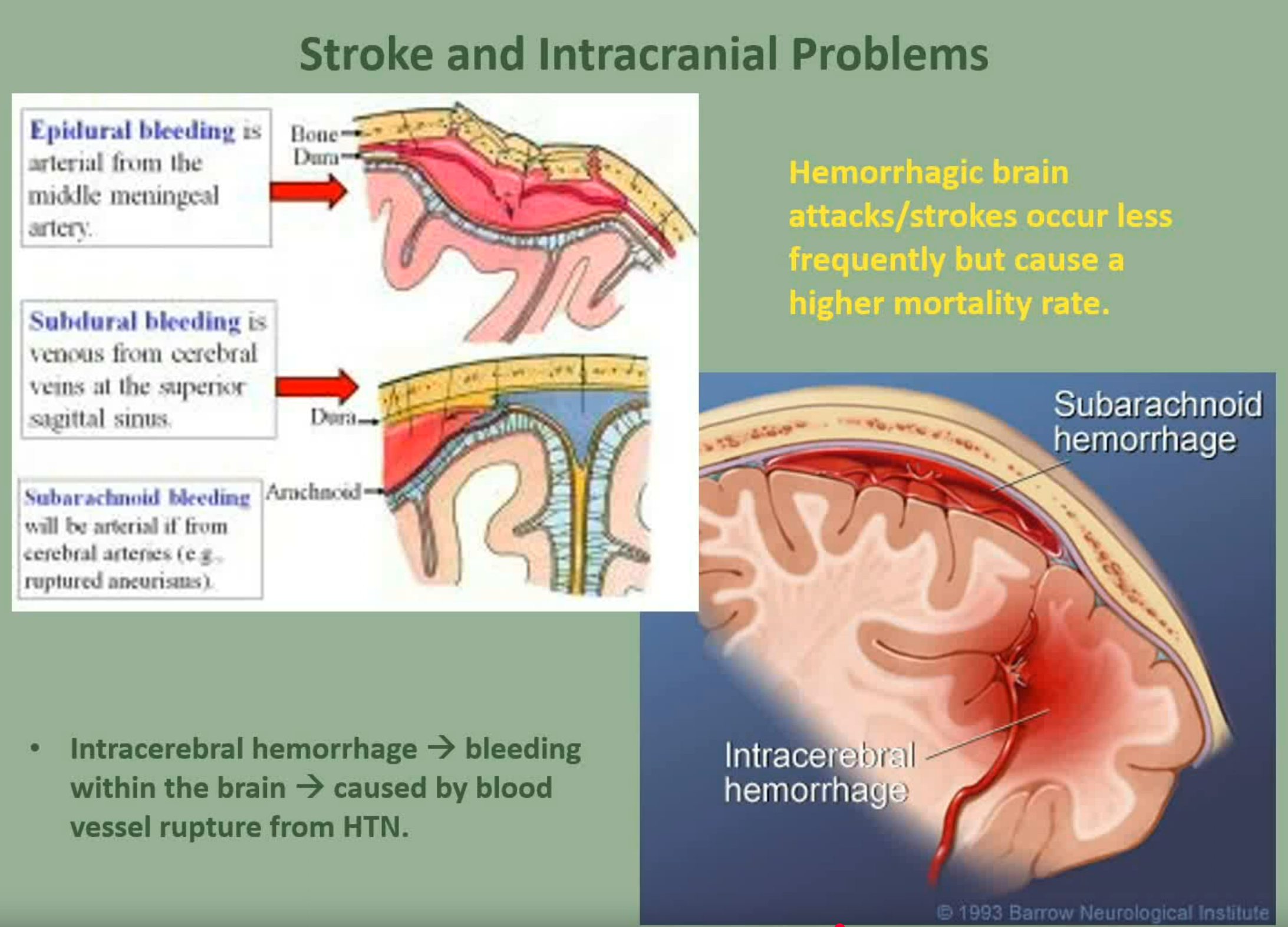
Hemorrhagic Stroke: 13% of strokes, involves blood extravasation into brain tissue or subarachnoid space.
Ischemic Stroke
Definition: Sudden loss of brain function due to disruption of blood supply, also called a "brain attack."
Treatment Window: The FDA-approved thrombolytic therapy (t-PA) must be administered within 3 hours after stroke onset; can be extended to 4.5 hours.
Ischemic Cascade:
Initiation: Decreased cerebral blood flow leads neurons to switch from aerobic to anaerobic respiration, causing a lactic acid buildup, diminished ATP production, and cellular dysfunction.
Penumbra Region: Surrounding area of low cerebral blood flow which may be salvaged if treated quickly.
Pathophysiological Events: Increase in intracellular calcium, release of glutamate, vasoconstriction, production of free radicals leading to cellular destruction.
Clinical Manifestations of Ischemic Stroke
General Symptoms:
Numbness/weakness on one side of the body (face, arm, leg)
Confusion, changes in mental status
Speech issues (dysarthria, dysphasia, aphasia)
Visual disturbances
Loss of balance or coordination
Severe headache
Motor Function: Loss of voluntary control; common dysfunction includes hemiplegia and hemiparesis.
Communication and Cognitive Function Impact
Language:
Aphasia (expressive, receptive, global), apraxia (difficulty in performing tasks), and dysarthria (difficulty speaking).
Perceptual Disturbances:
Visual-perceptual dysfunction affecting the ability to interpret sensations leading to conditions like agnosia.
Cognitive Function: Damage to the frontal lobe may lead to impaired learning and memory.
Assessment and Diagnostics
Initial Assessment: Focus on airway, cardiovascular status, functional deficits. Rapid history-taking is crucial.
Transient Ischemic Attack (TIA): Symptoms resolving within 24 hours but indicates risk for stroke.
Diagnostic Tools:
Non-contrast CT scans are preferred at presentation.
Further evaluations may include MRI, CT angiography, and ECGs.
Prevention of Stroke
Primary Prevention: Managing modifiable risk factors is key, including:
Controlling hypertension and diabetes
Healthy diet (DASH and Mediterranean diets recommended)
Regular physical activity, maintaining healthy weight, avoiding smoking.
Medication: Low-dose aspirin may reduce the risk of first stroke for those at risk.
Medical Management of Post-Stroke
Medications:
Anticoagulants for TIA or stroke patients.
Platelet inhibitors and dual antiplatelet therapy (aspirin + clopidogrel).
Statins recommended for long-term stroke prevention.
Thrombolytic Therapy (t-PA) Protocol
Administration:
Dosage: 0.9 mg/kg maximum 90 mg; 10% as IV bolus, remaining as infusion over 1 hour.
Intensive monitoring is crucial.
Goals: Rapid diagnosis and treatment can significantly improve outcomes.
Hemorrhagic Stroke
Definition: Caused mainly by intracerebral hemorrhage; high mortality rate (up to 50%).
Causes: Include hypertension, cerebral aneurysms, arteriovenous malformations (AVMs).
Clinical Presentation: Symptoms similar to ischemic stroke with severe headaches, nausea, decreased consciousness.
Management: Focus on controlling blood pressure, surgical interventions may be required.
Complications of Stroke Management
Increased Intracranial Pressure (ICP): Monitor for deterioration in neurological status.
Preventative Measures: Bed rest, medication for blood pressure management, seizure precautions, monitoring for signs of hydrocephalus and cerebral vasospasm.
Surgery: Carotid endarterectomy (CEA) and stenting procedures are essential for certain patients.
Conclusion
Holistic Approach: Comprehensive assessment and timely intervention are vital for effective stroke management and rehabilitation.