27. Saliva chewing and gastric secretions
Page 2: Learning Objectives
List the contents of saliva and gastric juice.
List the functions of saliva and gastric juice.
Describe the secretion of saliva and its control.
Describe the chewing reflex.
Describe the three main phases of swallowing: oral, pharyngeal, and oesophageal.
Describe the secretion of gastric acid.
Describe the phases of gastric secretion.
Explain the importance of gastric intrinsic factor for vitamin B12 absorption.
Describe the role and function of gastrointestinal hormones.
Page 3: Introduction to Digestion
The Gastrointestinal Tract (GIT) is a continuous tube extending from the mouth to the anus, including the oesophagus, stomach, duodenum (upper GI tract), and the small and large intestines (lower GI tract). Its primary functions include:
Motility (movement of food),
Secretion (enzymes, acids, etc.),
Digestion,
Absorption of nutrients, water, electrolytes, vitamins, and other essential substances from food and drink.
Key Points:
Absorption: Most digestion and nutrient absorption occur in the small intestine, though some absorption happens in the stomach (e.g., medium-chain fatty acids, some drugs).
Digestive Secretions: The stomach, salivary glands, gall bladder, pancreas, and liver secrete substances that aid digestion.
Specialized Cells: Enterocytes in the small intestine absorb digested nutrients into the portal circulation or lymphatic system.
Control Mechanisms:
Food Processing & Timing: The mixing and propulsion of food at each stage of the GIT are regulated by nervous and hormonal mechanisms to optimize nutrient absorption. (neurohormonal control)
GI Hormones: Released from the mucosa of the stomach and small intestine, these hormones are triggered by nervous activity, food intake, and distension.
Endocrine Functions: The GIT is the largest endocrine organ in the body and is controlled by the autonomic nervous system (ANS), which includes:
Sympathetic Nervous System (SNS)
Parasympathetic Nervous System (PSNS)
Enteric Nervous System (ENS), which operates autonomously but can be modulated by SNS and PSNS.
Enteric Nervous System (ENS):
Known as the "mini brain," the ENS has as many neurons as the entire spinal cord.
Neural Reflexes: GI functions are regulated by neural circuits involving mechanoreceptors or chemoreceptors in the mucosa, stimulating neurons in the myenteric and submucosal plexuses, which regulate endocrine or secretory cells.
Plexus Locations:
Myenteric plexus: Located between circular and longitudinal muscle layers throughout the GIT.
Submucosal plexus: Found in the small and large intestine.
The GIT is a highly complex system, integrating neural and hormonal control for efficient processing and absorption of nutrients.
Page 6: Saliva Composition
Summary of Saliva
Daily Secretion:
Saliva is produced at a rate of 800–1500 mL/day by the parotid, submandibular, sublingual, and tiny buccal glands.Properties:
Hypotonic overall (~200 mmol/L) and alkaline - pH 6 to 7
Large volume relative to gland mass.
Low osmolality but high potassium concentration (2–30x plasma levels, depending on secretion rate).
Major Constituents:
Water
Electrolytes:
Sodium (Na⁺) and chloride (Cl⁻) → hypotonic
Potassium (K⁺) and bicarbonate (HCO₃⁻) → hypertonic at higher secretion rates
Proteins:
Mucin: Lubricant
Ptyalin (α-amylase): Begins starch digestion
Ribonuclease: Degrades RNA
R Protein: Protects vitamin B12 during digestion
Lipase: Aids in lipid digestion
Lysozyme and IgA, IgG, IgM, thiocyanate : Provide antibacterial protection
Epidermal Growth Factor (EGF): Protects gastroduodenal mucosa, prevents ulcers, and promotes healing
Functions:
Lubrication:
Mucus binds to food, aiding swallowing.
Protection:
Alkaline pH buffers dietary acid, protecting against dental caries.
IgA and lysozyme defend against bacteria.
Digestion:
Salivary amylase: Begins starch and glycogen digestion.
Lingual lipase: Initiates dietary lipid hydrolysis.
Summary of Saliva Secretion
Control Mechanism:
Primarily controlled by neural influences from the salivatory nuclei in the brainstem.
Parasympathetic Nervous System (PSNS) plays the main role via acetylcholine acting on muscarinic receptors. - > increase saliva secretion
The Sympathetic Nervous System (SNS) has a minor influence.
Stimuli for Secretion:
Taste and tactile stimulation:
Chewing and taste stimuli (especially spicy and sour foods, smooth) → increase saliva secretion.
Rough objects or unpleasant tastes → reduce salivation.
Conditioned reflexes:
Thought, smell, or sight of food can trigger or inhibit saliva production through the appetite area in the hypothalamus, which receives signals from the cerebral cortex and amygdala.
Gastrointestinal reflexes:
Irritating foods or gastrointestinal abnormalities (e.g., nausea) trigger excess saliva production to dilute or neutralize irritants.
Saliva Secretion – Simplified Breakdown
1. Initial Secretion (by Acini):
Acini (secretory cells in salivary glands) produce a fluid:
Has an electrolyte concentration similar to extracellular fluid (ECF)
Contains enzymes and proteins like:
Ptyalin (amylase) – digest starch
Mucin – lubrication
2. As the Fluid Moves Through the Ducts:
Sodium (Na⁺) is reabsorbed (taken back into the body)
Potassium (K⁺) is secreted into the duct (swapped with Na⁺)
This creates a negative electrochemical gradient → pulls Chloride (Cl⁻) back in passively
Bicarbonate (HCO₃⁻) is secreted into the duct fluid:
Passively
Actively, in exchange for Cl⁻
3. Saliva Composition at Rest:
Na⁺ and Cl⁻ levels are lower than in plasma
HCO₃⁻ K+ levels are higher than in plasma
4. During Maximal Salivation:
Acini can increase secretion rate by up to 20 times
Fluid moves too fast through the ducts for full reabsorption → not enough time to reabsorb Na⁺ and Cl⁻ or secrete much K⁺).
Therefore, saliva becomes more similar to plasma, but still slightly hypotonic.
higher Na⁺
lower K⁺
5. Hormonal Influence (ADH & Aldosterone):
ADH and aldosterone affect duct cells
Decrease Na⁺ in saliva (more reabsorbed)
Increase K⁺ in saliva (more secreted)
but minimal effect
Function of Saliva in Oral Hygiene & Clinical Significance
Role in Oral Hygiene:
Cleansing action:
Saliva washes away bacteria and food particles that promote bacterial growth.
Antibacterial properties:
Contains igA, thiocyanate ions and lysozyme, which destroy bacteria.
Also contains protein antibodies that help fight infections.
Protective effect:
Prevents ulceration and infection of oral tissues.
Reduces the risk of dental caries by neutralizing acids and removing debris.
akaline pH
Clinical Significance:
Saliva deficiency can lead to: xerostomia
Ulceration and infection of oral tissues.
Increased risk of dental caries
oral candidiasis
Summary of Chewing (Mastication)
Tooth Function:
Incisors: Cutting action.
Canines: Tearing and piercing.
Molars & Premolars: Grinding and crushing.
Chewing Reflex: - voluntary and reflex
Food in mouth → reflex inhibition of jaw muscles → lower jaw drops.
Stretch reflex activates → rebound contraction → jaw raises and teeth close.
Bolus compression → inhibits jaw muscles again → jaw drops.
The process repeats
Importance of Chewing:
Prevents choking by breaking large food lumps. - prevents airway obstruction
Mixes food with saliva and mucus for lubrication and digestion.
Increases surface area of food for more effective digestion by GI secretions.
Summary of Swallowing
Swallowing consists of three stages: OPO
Oral Phase (Voluntary):
The tongue pushes the food bolus backward.
Pressure on the pharyngeal wall triggers the swallowing reflex, which is involuntary from this point onward.
Controlled by the swallowing center in the medulla oblongata.
Pharyngeal Phase (Involuntary):
Soft palate lifts → seals off the nasal passages.
Larynx is pulled upward.
Glottis closes and the epiglottis deflects food away from the trachea → prevents food from entering the airway.
Oesophageal Phase (Involuntary):
Peristaltic waves drive food through the oesophagus to the stomach.
If the primary wave fails to clear the food, secondary waves are initiated until all food reaches the stomach.
Controlled by:
Somatic nerves (glossopharyngeal) → innervate striated muscle in the upper GI tract.
Parasympathetic nerves (vagus) → innervate smooth muscle in the lower oesophagus.
These nerves stimulate muscle contraction and relaxation of the oesophageal sphincters.
Functions of Stomach and Gastic Juice
The stomach has several essential functions, including storage, mixing, and controlled emptying of food into the small intestine for digestion and absorption. These functions are vital for the initiation of the digestive process.
Key Functions of the Stomach:
Storage: The stomach stores food until it can be processed. As food enters, the stomach stretches, triggering a vagovagal reflex to relax the stomach muscles and accommodate more food.
Mixing: The stomach mixes food with gastric secretions to form a semi-fluid mixture called chyme. This mixing is controlled by the myenteric plexus, with regular peristaltic waves (3-4/min) progressing from the body to the antrum, becoming more intense. MIX WITH HCL
Slow Emptying: The chyme is gradually emptied into the small intestine at a controlled rate. Gastric emptying is influenced by the strength of antral contractions and pyloric resistance, which are regulated by hormones released from receptors in the duodenum and jejunum.
Major Components of Gastric Juqice:
Pepsinogen: Secreted by chief cells, it is an inactive form of pepsin. It is converted into pepsin in acidic conditions (pH < 5), which starts protein digestion.
Pepsin: An enzyme that digests proteins and can activate more pepsin from pepsinogen.
Hydrochloric Acid (HCl): Secreted by parietal cells, it sterilizes food, starts hydrolysis of macromolecules, and creates the acidic environment needed to convert pepsinogen to pepsin.
Mucus: Secreted by mucous cells, it provides a protective, lubrication, alkaline layer on the stomach lining and aids in the smooth passage of food.
Intrinsic Factor: Also secreted by parietal cells, for the absorption of vitamin B12.
These functions and components of gastric juice work together to initiate digestion and prepare the food for absorption in the small intestine.
Gastric Secretion
The stomach secretes various substances to aid in digestion, with key contributions from different types of glands and cells:
Mucous Cells: These line the entire surface of the stomach and secrete mucus, providing protection for the stomach lining.
Oxyntic (parietal) Glands: Located in the body and fundus of the stomach, they secrete hydrochloric acid (HCl), pepsinogen, intrinsic factor, and mucus.
Pyloric Glands: Located in the antral portion of the stomach, these glands primarily secrete mucus and the hormone gastrin.
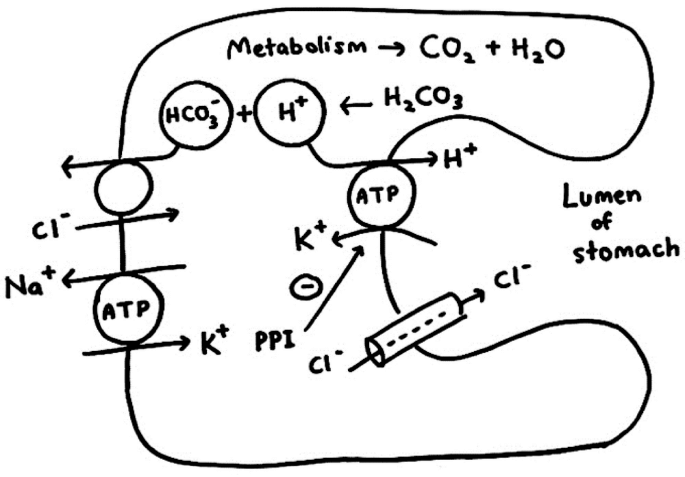
Hydrochloric Acid (HCl) Secretion:
Parietal cells secrete an extremely acidic solution of hydrochloric acid (with a pH around 0.8), which is isotonic with body fluids but highly acidic.
This process is energy-dependent, requiring significant energy (1500 calories per liter of gastric juice).
Hydrogen-Potassium Pump (H+-K+ ATPase): The main mechanism for HCl secretion:
Water dissociates into H+ and OH- within the parietal cell.
H+ is secreted into the canaliculus (lumen) in exchange for K+ through the H+-K+ ATPase pump.
K+ leaks back into the lumen but is recycled back into the parietal cell.
OH- combines with CO2 to form HCO3-, which is exchanged for Cl-, and then Cl- is secreted into the canaliculus.
The H+ and Cl- combine to form HCl, which is secreted into the lumen of the gland.
Water moves into the canaliculus by osmosis, resulting in the secretion of H2O, HCl, KCl, and NaCl, with a final pH of 1-2.
Protection Mechanisms:
To prevent back leakage of acid into the stomach mucosa, there is a gastric barrier consisting of alkaline mucus and tight junctions between cells. If this barrier is damaged, acid can leak into the mucosa, leading to ulceration.
Summary of Gastric Acid Secretion and Related Processes
Stimulation of Gastric Acid Secretion: stimulate parietal cell
Endocrine and Nervous Control: Gastric acid secretion by parietal cells is regulated by both nervous and endocrine mechanisms.
Acetylcholine: Released by the parasympathetic nervous system (specifically the enteric nervous system), acetylcholine stimulates gastric acid release in response to vagovagal reflexes.
ECL Cells and Histamine: Enterochromaffin-like (ECL) cells release histamine which directly stimulates parietal cells. ECL cells are activated by gastrin, a hormone released by G cells in response to the presence of protein-rich food in the stomach.
Gastrin: Released by G cells in the pyloric region of the stomach, gastrin stimulates ECL cells to release histamine, which in turn activates parietal cells to secrete hydrochloric acid (HCl).
Stimulation and Activation of Pepsinogen:
Pepsinogen Release: by peptic/cheif cells of oxyntic mucosa. Stimulated by acetylcholine (released by the vagus nerve) the inactive precursor of the enzyme pepsin.
Activation to Pepsin: Pepsinogen is activated to pepsin by HCL or pepsin itself. Pepsin is a proteolytic enzyme that breaks down proteins.
Intrinsic Factor:
glycoprotein
Function: Secreted by parietal cells of the oxyntic glands, intrinsic factor is crucial for the absorption of vitamin B12 in the ileum.
Absorption Process: Intrinsic factor binds with vitamin B12 - form intrinsic factor vitB complex in the stomach, protecting it from digestion as it moves into the small intestine. In the terminal ileum, the complex binds to receptors, allowing vitamin B12 to be absorbed through the membrane via pinocytosis.
Vitamin B12 Transport: After absorption, vitamin B12 enters the bloodstream and is transported to the liver for storage and later use in red blood cell production. Lack of intrinsic factor impairs vitamin B12 absorption, leading to pernicious anemia, a condition with impaired red blood cell production.
Gastric Secretions: Phases, Control, Contents, and Function
Gastric secretion occurs in three phases: CGI
Cephalic Phase:
stimulated by sight, smell, taste → CNS
Function - to prepare stomach for arriving of food, short duration
Occurs before food enters the stomach, triggered by taste, smell, chewing, swallowing, and even the thought of food.
Receptors in the tongue, buccal, and nasal cavities are stimulated.
Signals from the cerebral cortex, medulla oblongata, and hypothalamus travel via the vagus nerve to the stomach, promoting secretion.
increase Gastric secretions released:
Mucus (from mucous cells)
Pepsinogen (from chief cells)
Hydrochloric acid (HCl) (from parietal cells)
Gastrin (from G cells)
Gastric Phase:
Occurs once food enters the stomach.
Vagovagal reflexes, local enteric reflexes, and gastrin secretion are triggered.
Distention of the stomach and mixing of food with gastric juices raise the pH, stimulating gastrin release.
Gastrin promotes:
Increased gastric juice production
Enhanced gastric motility (mixing waves)
Intestinal Phase:
Begins when chyme enters the duodenum.
Chyme stimulates intestinal gastrin release, which promotes continued gastric secretion.
As more chyme enters, sympathetic reflexes (reverse enterogastric reflex) are triggered due to stretch receptors and the presence of acids, fats, and protein breakdown products.
Hormones released:
Secretin, GIP, CCK, and somatostatin.
Purpose:
Inhibit gastric secretion and motility.
Slow gastric emptying to allow proper digestion and absorption in the small intestine.
Protect the duodenal mucosa from damage caused by acidic chyme.
Enterogastrones (intestinal hormones) inhibit gastric acid secretion and gastric emptying to regulate the flow of chyme, ensuring optimal digestion and absorption.
GIP: gastric Inhibitory peptide. stumulate by glucose in chyme. stimulates release of insulin
Somatostatin: Inhibits gastric secretions.
Secretin: increase bile secretion. stimuates by acidic chyme
CCK: stimulate production of pancreatic enzymes. stimulated by lipids and proteins of chyme
Gastrin - stimulate production of HCL and enzyme, increase motility