KNPE 335 Wk 4 - Psychological and Mental Healthy Aging
Learning Objectives:
define they psychological dimensions of aging
understand the difference between mental health and mental illness
understand what effects mental health for older adults and aging
describe the common mental health conditions and their characteristics for older adults
explore interventions to improve mental health for older adults and healthy aging
Psychological Definitions
Mental Health:
cognitive function:
changes in memory, attention, and processing speed
mental disorders:
depression, anxiety, cognitive impairments, etc
Wellbeing:
coping mechanisms:
strategies used to manage stress and life changes
resilience:
ability to adapt positively to adversity or significant life events
QoL
life satisfaction:
overall contentment and fulfilment with life experiences
purpose and meaning:
a sense of contribution and meaningful engagement in daily activities and relationships
Social Connections:
social support:
relationships with family, friends, communities
social isolation:
the degree to which an individual lacks a sense of engagement with others
Life Transitions:
retirement:
adjusting to a new phase of life with changes to one’s routine, responsibilities, and identity
bereavement:
coping with loss and the associated grief process
Self Identity and Autonomy:
self esteem:
maintaining a positive self image and self worth
Autonomy:
maintaining independence and control over life decisions
What is Mental Illness?
“characterized by alteration in thinking, mood, or behaviour - or any combination thereof - associated with some significant distress and impaired functioning”
mental illness takes many forms including mood disorders, schizophrenia, anxiety disorders, personality disorders, eating disorders, and addictions such as substance dependance and gambling
Mental Illness vs Mental Health

Mental Health and Aging
the prevalence of mental health problems in adults over the age of 65 ranges from 20-30%
depression and anxiety are the most common mental health conditions among older adults
sub clinical depression and anxiety raises estimates of mental health issues to 40% for older adults
globally, ~27.2% of deaths from suicide are among people aged 60 or over
What Affects Mental Health?
housing
transportation and mobility
income
services
health
housing
dental
vision
food services
hearing
recreation
physical factors
exercise
nutrition
sleep
illness/disability
emotional factors
self esteem
self knowledge
coping skills, etc
spiritual factors
religious beliefs
nature and meaning of one’s life
social factors
personal relationships
meaningful activity
Neurotransmitters and Healthy Aging
dopamine
reward-motivation system
motor control, decision making, teaching, motivation, pleasure
serotonin
boost when you feel significant and important
mood, memory, sleep, cognition
norepinephrine
regulates blood pressure
memory formation and retrieval
stress and sleep regulation
Why are Mental Illnesses Missed?
in older adults, signs and symptoms often differ than those in younger people
older adults are less likely to self identify problems
mental illnesses can accompany or stem from serious physical illnesses and disorders
environmental social, and cultural factors can affect a person’s signs and symptoms of mental illness and willingness to seek treatment
caregiver stress about burnout
ageism
Older Adults, Dignity, and Mental Illness
causes of compromised dignity in older people with mental illness
ageism and elder abuse
loneliness
lack of policy provisions
increased frailty and dependence
lesser focus on functional recovery
neurocognitive disorders
institutionalization
healthcare inequalities
social stigma and discrimination
Common Mental Health Disorders in Older Adults
depression
suicide
anxiety disorders
dementia
loneliness and isolation
delusional disorders
delirium
paraphrenia (mental illness characterized by an organized system of delusions with or without hallucinations)
concurrent disorders (has both a mental illness and a substance use problem)
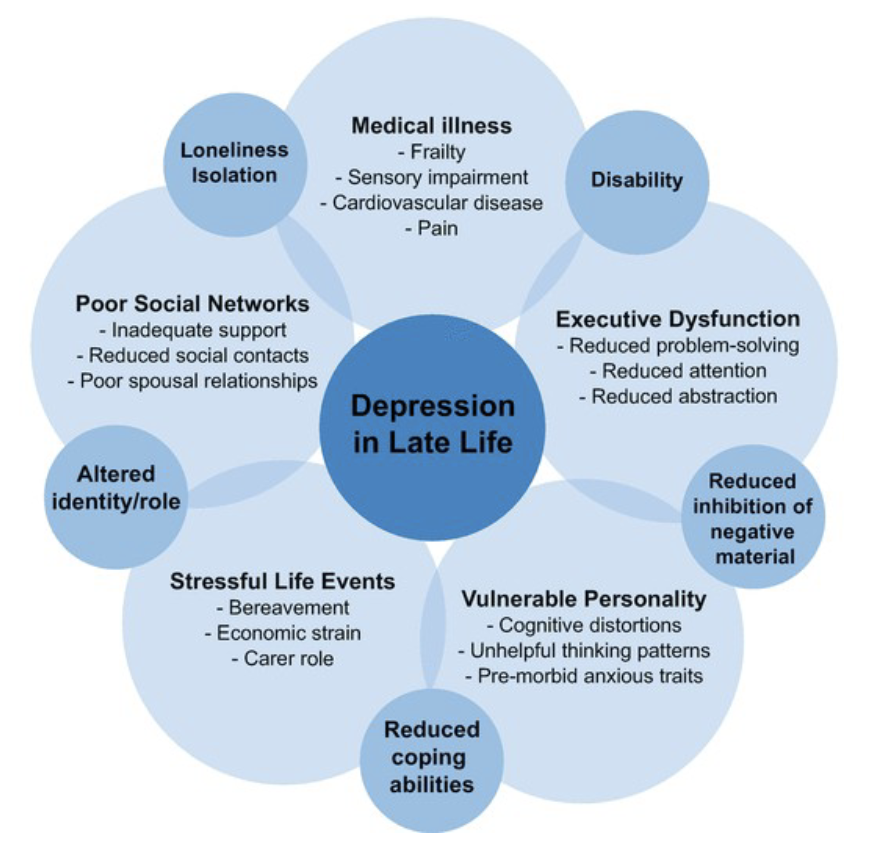
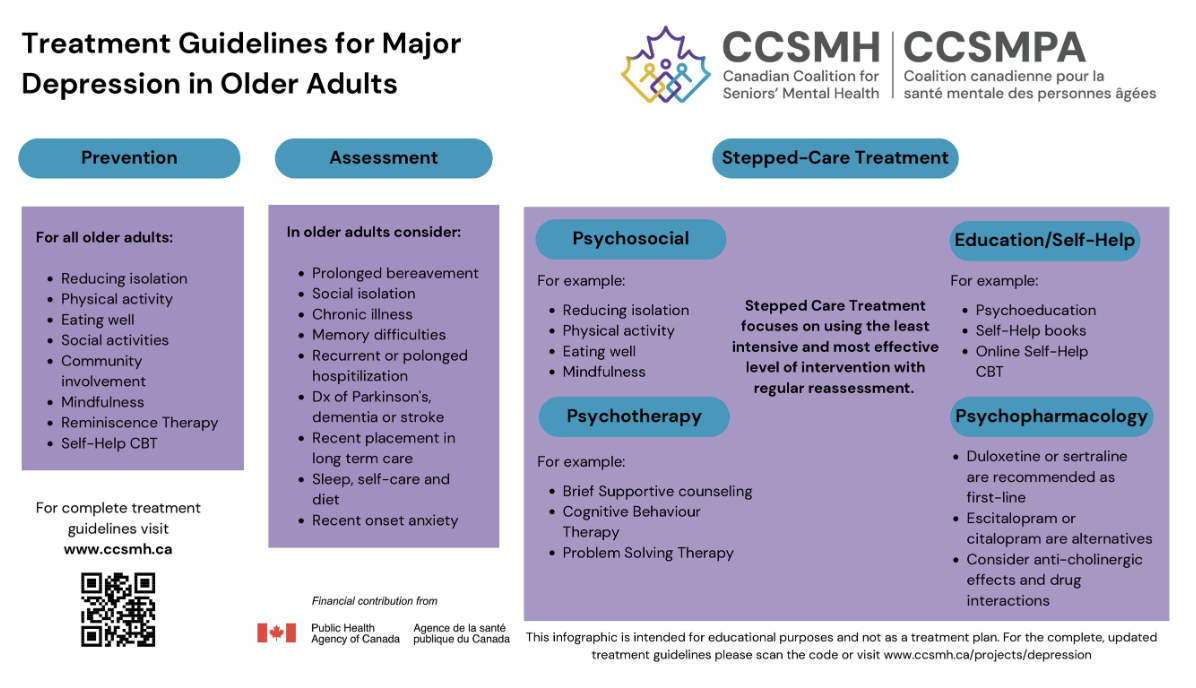
Depression and Aging
not a “normal” part of aging
there is a distinct type of depression in later life which may be reactive - such as long term care admission
late onset depression often has a cognitive component, some memory impairment, which may be related to decreased blood flows or TIAs
depressive symptoms are very similar to dementia, so the person is often labeled as having dementia
Symptoms of Depression in Older Adults
sleep
change in sleep patterns such as daytime napping, being unable to fall asleep. and/or being unable to stay asleep
feeling fatigued even with sleep
interest
lack of interest or pleasure in life’s daily activities, anhedonia
physical limitations and pain limiting activities that they once enjoyed
guilt
feeling like a burden, worthlessness, grief and loss, compounding life stressors, changes in roles and responsibilities, and feeling sad without a reason
concentration
fears about cognitive decline and memory loss, acute stress
medical conditions that may occur independent of depression or alongside depression that can contribute to issues with concentration and memory
energy
changes in energy (lethargy, fatigue)
increase in angry, aggressive, agitated, or irritable energy
appetite
changes in appetite, unintended weight gain or loss, increased or decreased sense of hunger and satiety, change in normal eating patterns or preferred foods, changes to perceptions about what foods are digestible or cause digestive issues
psychomotor
reduced activity, low energy, feeling that they have slowed down, sense of restlessness
suicide
feelings of hopelessness, helplessness, and sadness can lead individuals to consider suicide as a possible option
Late Life Depression
a depressive disorder developed at the beginning of old age
a serious and life threatening disorder which affects every 1 in 5 individuals in a lifetime
typically characterized by an atypical cluster of symptoms (ie. somatic symptoms, anxiety, and psychotic symptoms)
somatic (physical) symptoms are most common in late life depression compared to early
less likely to be characterized by sadness
under diagnosed and inadequately treated
becomes challenging to distinguish it from dementia (due to overlapping symptom profiles) especially when depression affects the cognition and is presented as ‘pseudodementia’
Delirium
delirium is an acute change in mental status causing shift in cognitive functioning, reduced environmental awareness, altered attention, and behaviour changes
Types of Delirium
hypoactive
withdrawn, reduced speech and activity, apathy, unawareness
hyperactivity
increased activity, irritability, restlessness, combativeness
mixed
fluctuations in psychomotor activity
Short Term Outcomes of Delirium
falls
pressure injuries
aspiration pneumonia
distress
prolonged hospital stay
long term care admission
increased risk of mortality
Long Term Outcomes of Delirium
functional and cognitive impairment
dementia
post traumatic stress syndrome
sleep disturbances
increased risk of mortality
Factors Reducing Risk of Delirium
cognitive reserve
the capacity of the mature adult brain can butter the effects of neurological disease or injury
social support and interactions
regular visits from care partners help to reduce the burden of cognitive impairment and provide comfort with frequent reorientation
environmental influences
exposure to natural daylight can support the promotion of regular circadian rhythms and healthy sleep cycles
pain management
appropriate and consistent pain assessments should be conducted to ensure pain is adequately controlled and severity is monitored, especially if communication becomes difficult with delirium
The Intersection of Delirium and Mental Health Conditions
unfortunately, some of the populations most vulnerable to delirium are older adults who have dementia, depression, and acute psychiatric syndrome
each of these syndromes can co-occur with delirium
when an individual develops delirium, it is called delirium superimposed on dementia
Loneliness
‘a state of solitude or being alone’
‘the perception of being alone and isolated that matters most’ and is a state of mind
typically thought to be a subjective, negative feeling related to the deficient social relations
reported to be more dangerous to health than smoking
High Degree of Loneliness Precipitates:
suicidal ideation
para-suicide
alzheimer’s disease
dementia
negative effects of immune system
negative effects of cardiovascular system
increased risk of hospitalization
increased risk of LTC facility placement
Types of Loneliness
developmental loneliness
lack of balance between individualism and innate desire to relate to others
internal loneliness
the perception of being alone. associated with low self esteem and self worth
situational loneliness
socio-economic and cultural milieu. effected by the environment
Interventions for Loneliness
activity involvement
volunteer roles
developing and keeping quality relationships
pharmacological management of physical ailments
staying in contact with family and friends
Social Isolation
“a state in which the individual lacks a sense of belonging socially, lacks engagement with others, has a minimal number of social contacts and they are deficient in fulfilling and quality relationships”
social isolation is a major and prevalent health problem among community-dwelling older adults, leading to detrimental health conditions
prevalence of social isolation in community-dwelling older adults indicate that it is as high as 43%
Impacts of Social Isolation
health behavioural
behaviour habits
encouragement to adhere to medical treatment
refrain from negative or risky behaviours
psychological
less participation in social activities
increased risk of cognitive decline
increased risk of suicide or depression
physiological
predictor of mortality from heart disease or stroke
decreased infection resistance
other outcomes
all cause mortality
risk of falls
rehospitalization and institutionalization
Interventions for Social Isolation
Fakoya et al., (2020)
no one size fits all approach
tailor programs to individual needs, specific population, degree of loneliness
Paquet et al., (2023)
social prescribing programs can enable primary care providers to refer patients to a range of local nonmedical services
group based social activities, support groups, recreational activities, training or use of technology are most effective
Manjunath et al., (2021)
patient centred approach is essential for any effective intervention ie. social facilitation, exercise, psychological therapies, health and social services, animal therapy, befriending, and leisure and skill development
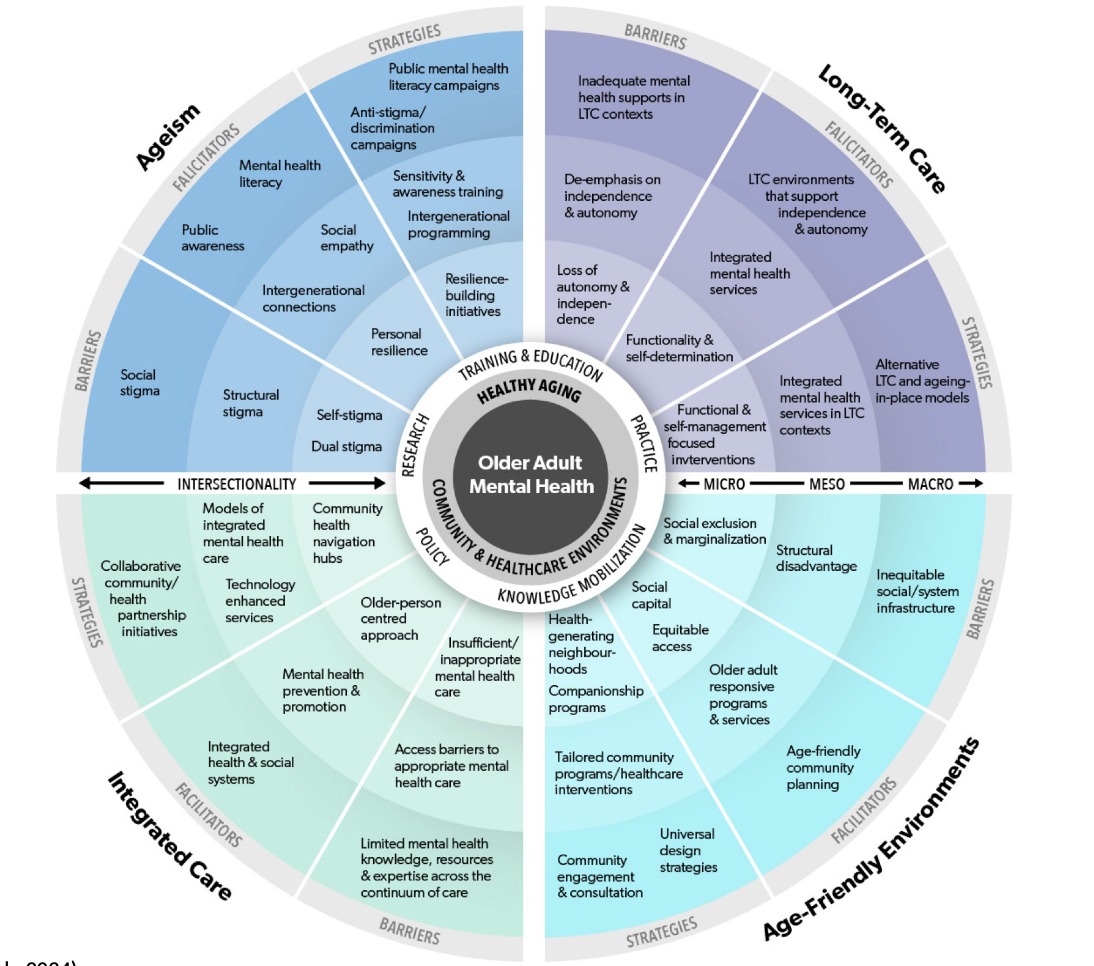
Mental Health Interventions
mental health promotion and prevention strategies for older adults focus on supporting healthy aging including:
measures to reduce financial insecurity and income inequality
programs to ensure safe and accessible housing, public buildings, and transport
social support for older adults in their carers
support for healthy behaviours, especially to eat a balanced diet, be physically active, refrain from tobacco and reduce alcohol use
health and social programs targeted at vulnerable groups such as those who live alone or in remote areas and those living with a chronic health condition