Nerve and Skeletal Muscle
Nerve and Skeletal Muscle
Nerve Objectives
Key Differences to Understand:
Axonal degeneration vs. Wallerian degeneration.
Most common cause of acute peripheral neuropathy.
Characteristic histopathologic findings in CMT I disease.
Clinical features of Guillain-Barre syndrome.
Formation of traumatic neuroma.
Treatment options for diabetic neuropathy.
Pre-lecture Questions
Neuropathy Presentation: Organophosphates, pesticides, and industrial solvents have a common clinical presentation referred to as neuropathy.
Common Cause of Acute Peripheral Neuropathy: Identify the most common cause.
Nerve Conduction Studies: Useful for distinguishing between demyelinating neuropathy and axonal neuropathy.
Axon Composition: True or false: a single axon contains both myelinated and unmyelinated fibers.
Myelin Production: Myelin is produced by Schwann cells in the peripheral nervous system.
Diabetic Neuropathy Treatment: Best treatment options need to be identified.
Muscular Dystrophy Characteristic: Identify which muscular dystrophy is characterized by the inability to “let go” of a handshake.
Duchenne Muscular Dystrophy: Absent structural protein needs to be pinpointed.
Corticosteroid Response: Inclusion body myositis response to corticosteroids needs verification (True/False).
Staining for Muscle Fibers: Identify the histochemical stain used to distinguish between slow (Type I) and fast (Type II) twitch muscle fibers.
Myasthenia Gravis Diagnosis: Name the test used for diagnosing Myasthenia Gravis.
Peripheral Nerves
Normal Structure
Normal peripheral nerves consist of bundles of axons, including both myelinated and unmyelinated fibers.
Myelin Production: Produced by Schwann cells.
Neuron Cell Components
Parts of a neuron:
Neuron cell body
Dendrites
Myelin sheath
Nodes of Ranvier
Neuron nucleus
Schwann cell
Axon
Motor Units
Types of motor units:
Normal
Segmental demyelination
Axonal degeneration
Reinnervation
Myopathy
Tests for Neuropathies
Nerve Conduction Studies:
Distinguish between demyelinating neuropathy (DN) characterized by slowing of conduction velocity or conduction block, versus axonal neuropathy (AN) which is associated with low-action potential amplitudes.
Other Tests:
CSF analysis, EMG (Distinguishes between denervation atrophy vs. primary muscle disease), Muscle or Nerve biopsy.
Segmental Demyelination
Characteristics
The axon remains intact, the neuron cell body remains, but myelin is lost (can sometimes be recovered).
Results in conduction block.
Clinical Examples:
Acute: Guillain-Barre syndrome
Chronic: Charcot-Marie-Tooth disease.
Guillain-Barre Syndrome
Epidemiology:
Most common acute peripheral neuropathy.
Leading cause for acute flaccid paralysis.
Primarily affects motor pathways; variants can be motor and sensory.
Involves nerve roots and peripheral nerves.
Preceding Illness:
Approximately 2/3 of cases are preceded by an influenza-like illness.
Pathogenesis:
An autoimmune demyelination syndrome is suspected to be the cause,
Characterized by inflammation of the peripheral nerve with perivenular and endoneurial infiltration of lymphocytes, macrophages, and few plasma cells.
Causes included infections from Mycoplasma pneumoniae, Campylobacter jejuni, and viral infections (HIV, EBV, CMV, influenza).
Symptoms:
Rapidly progressive ascending paralysis beginning with proximal muscles and can spread, leading to respiratory muscle paralysis and potential death.
May experience decreased or absent deep tendon reflexes.
Laboratory Testing in Guillain-Barre Syndrome
Findings:
Oligoclonal bands on high-resolution electrophoresis.
CSF indicates elevated protein, normal glucose, and little or no pleocytosis.
Mortality and Recovery:
Improvements in mortality due to better supportive measures including mechanical ventilation and treatments like IV immunoglobulin or plasmapheresis.
95% survival with most patients experiencing no lasting defects. Continuance of symptoms three weeks post onset correlates with lower chances of complete recovery.
Charcot-Marie-Tooth Disease
Description:
Most common hereditary neuropathy, incidence ~1 in 2500.
Inheritance pattern: Autosomal dominant; typically affects young adults.
Pathology and Clinical Features:
Peroneal nerve neuropathy leading to weakness and atrophy of calf muscles, presenting with an “inverted champagne bottle” appearance in the lower legs.
Other findings include abnormal gait and hammer toes.
Treatment: Supportive including orthotics and physical therapy.
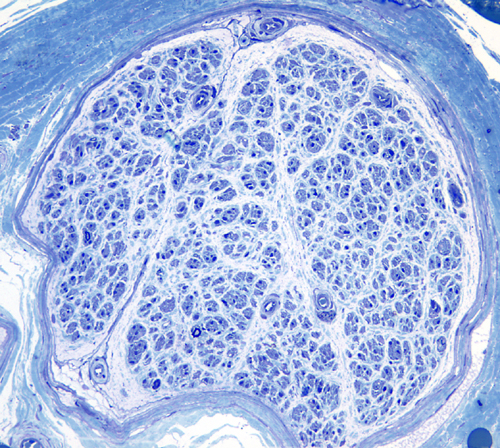
Pathologic Findings:
Degeneration of the posterior column, demyelination, remyelination(Presenting as thin myelin sheaths), axonal loss, onion bulb formation.
Wallerian Degeneration
Mechanism:
Occurs when the axon connection to the neuronal cell body is lost, typically due to trauma or degeneration.
Clinical Examples:
Often seen in traumatic scenarios.
Sequence of Events:
Image illustrating biology of Wallerian degeneration demonstrates axon degeneration, repair processes by Schwann cells, and associated debris clearance.
End Results:
We observe axonal sprouts among the Schwann cells undergoing mitosis, with growth cones directed toward regeneration.
Traumatic Neuroma
Occurs post injury either from:
Poor approximation and repair of the injury resulting in a tangled mass of regenerating nerve fibers that fail to connect with the distal end.
Presents as a painful mass.
Pathologic Features:
Characterized by a disordered mix of nerve fibers (axons), fibroblasts, Schwann cells, and scar tissue.
Distal Axonopathy
Definition: A condition where degeneration affects the distal part of the axon and its myelin first,
Results in a characteristic distal