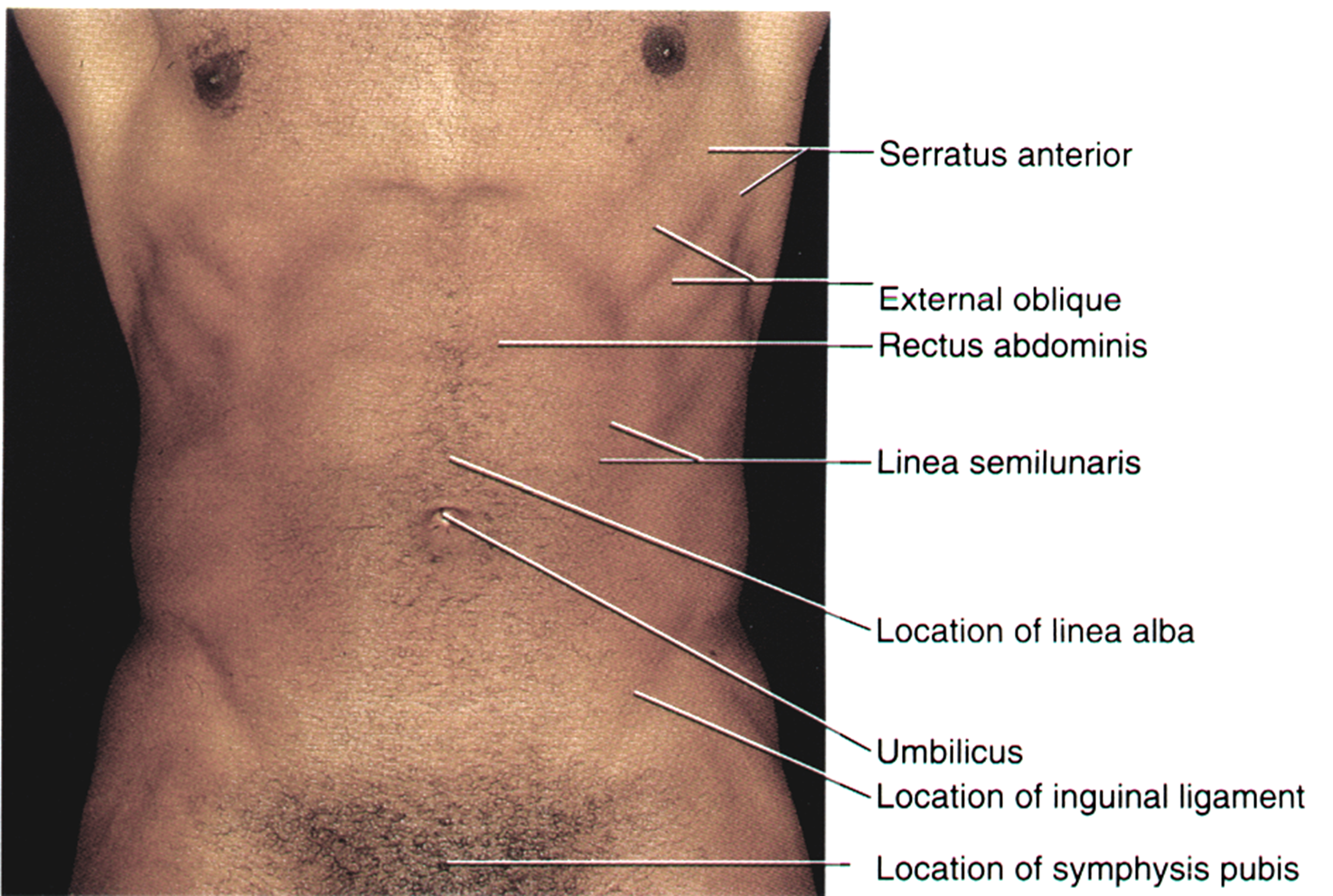
abdominal wall & inguinal canal
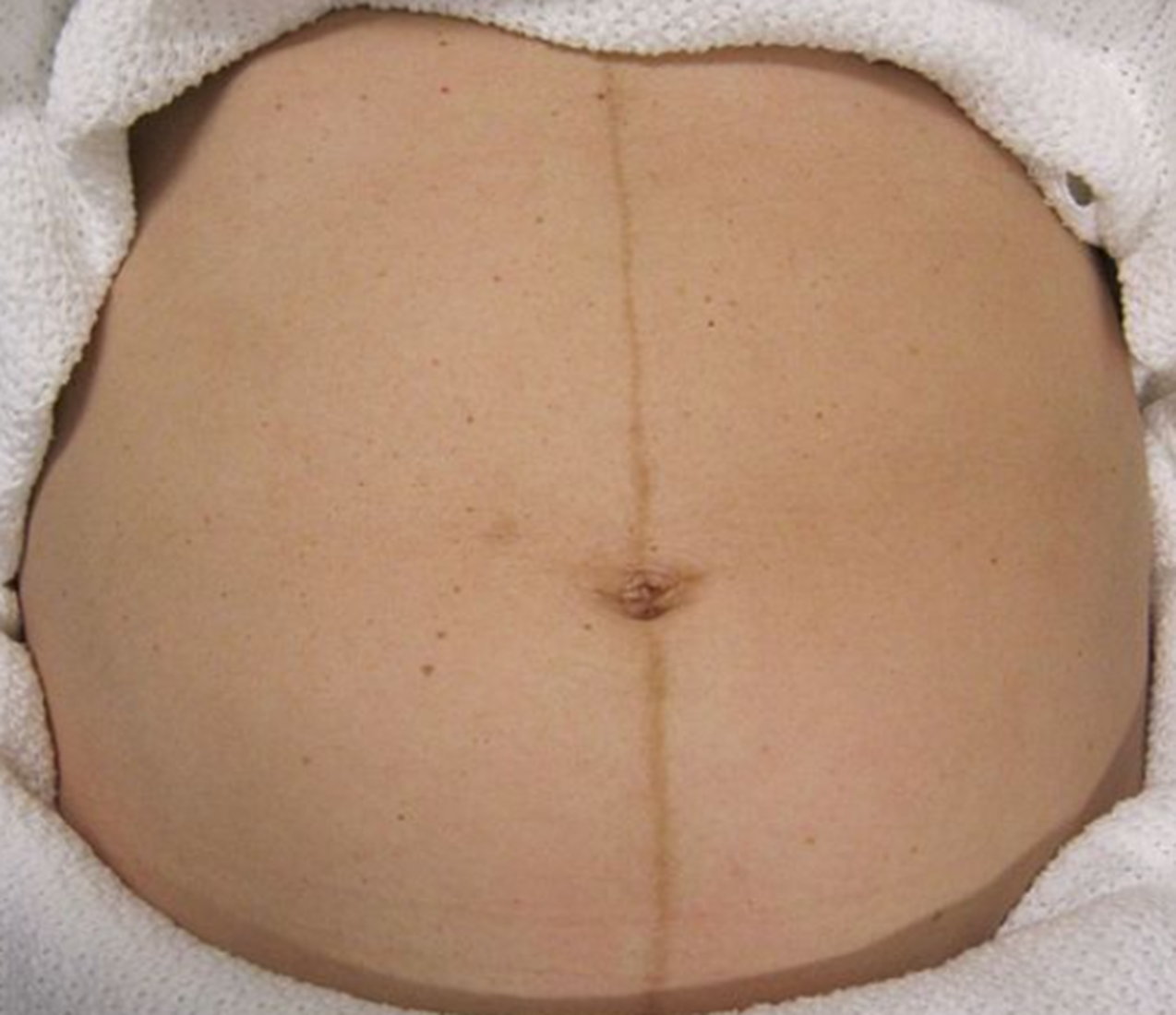
linea alba becomes pigmented in pregnancy becomes the linea nigra
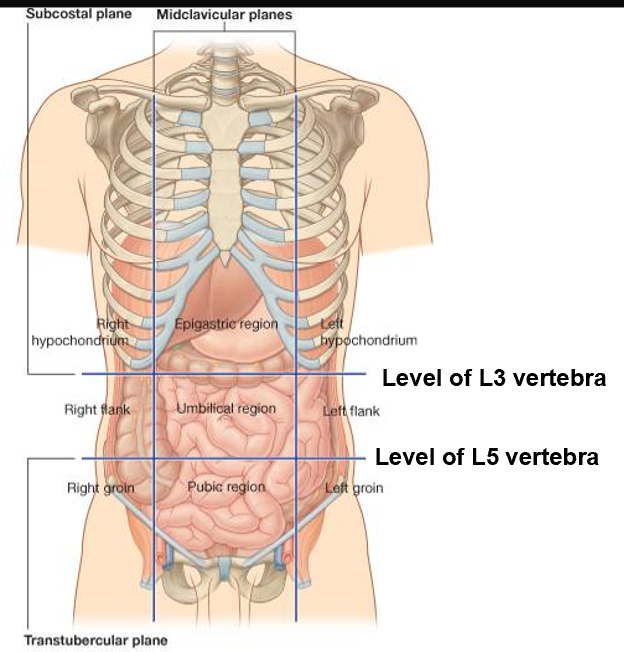
transverse (axial) planes
4 important transverse or axial planes that are used clinically to describe the abdomen and its contents.
Transpyloric at L1: Superior mesenteric artery
Subcostal at L3: Inferior mesenteric artery
Supracristal at L4: Bifurcation of aorta
Transtubercular at L5: Formation of inf. vena cava
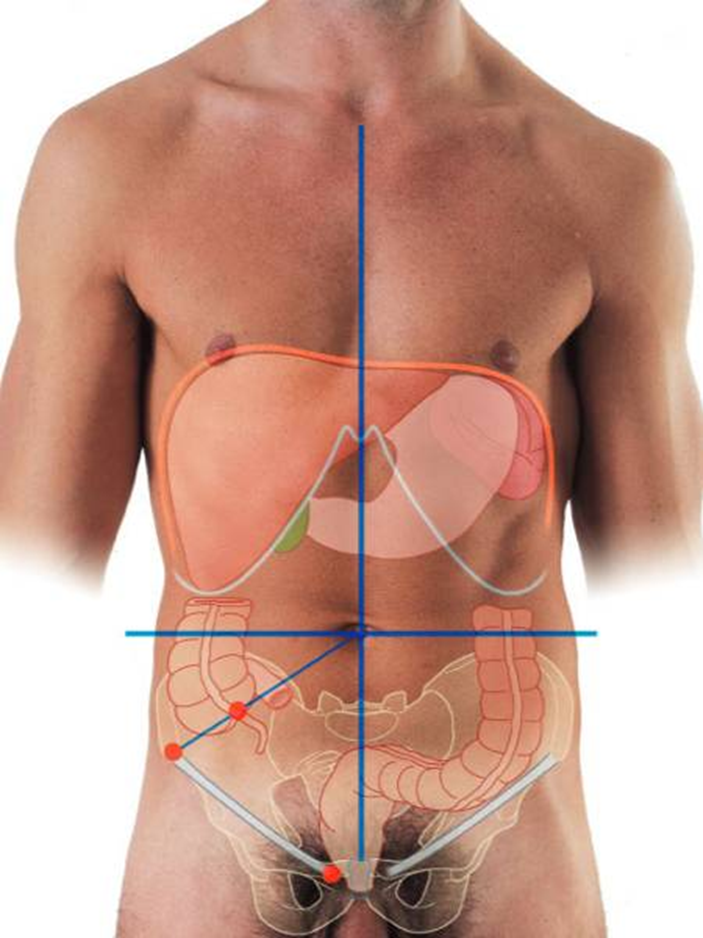
mcburney’s point
1/3rd of the way up along a line from the right anterior superior iliac spine to the umbilicus.
Pressure here will cause maximum tenderness in a patient with acute appendicitis.
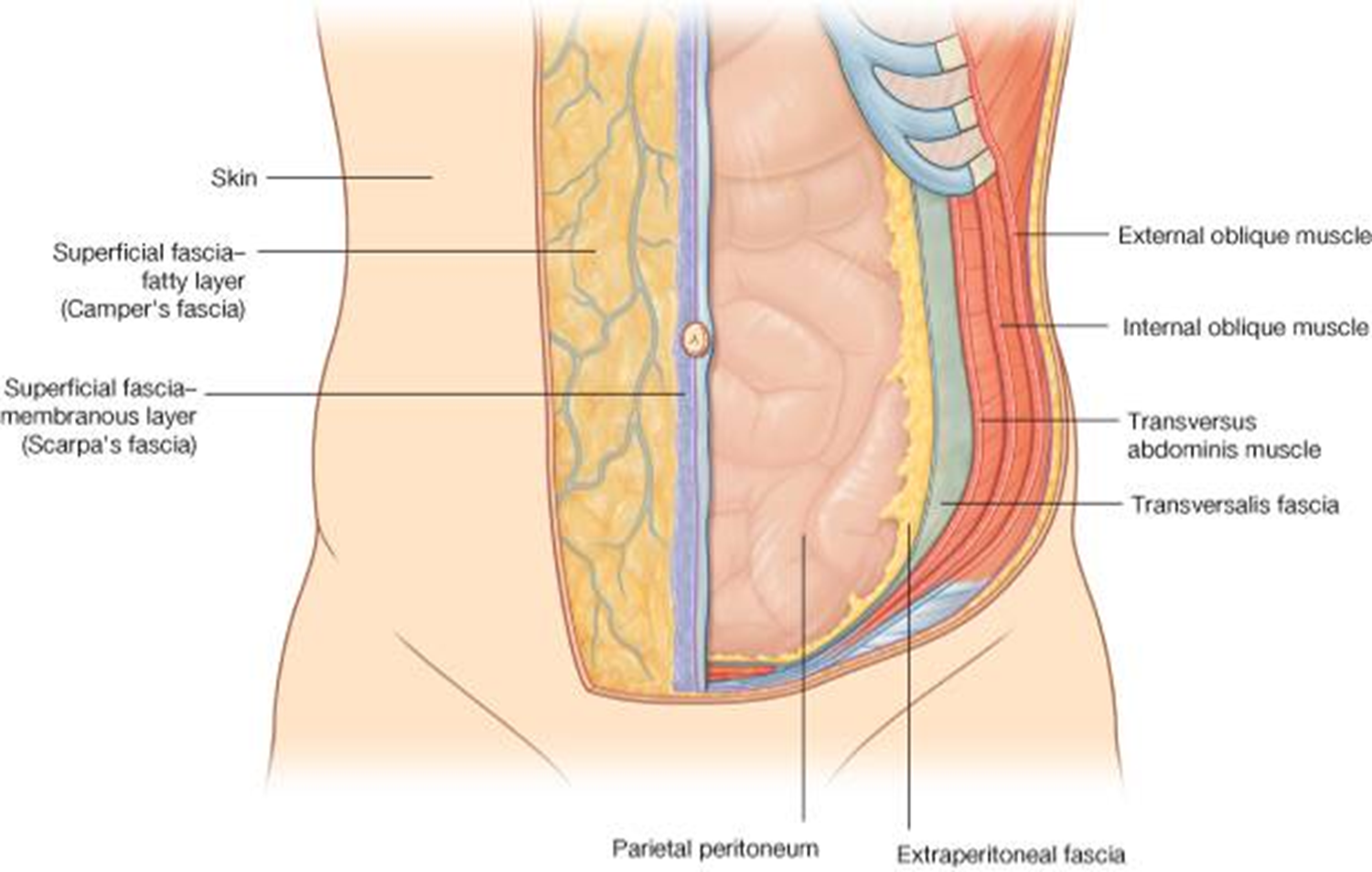
subdivisions of abdominal wall
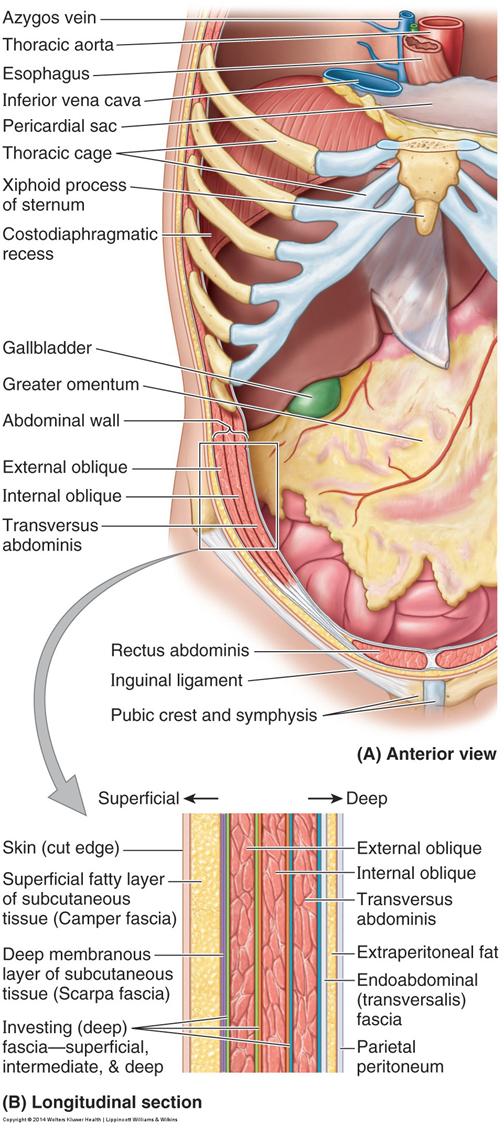
layers
Skin
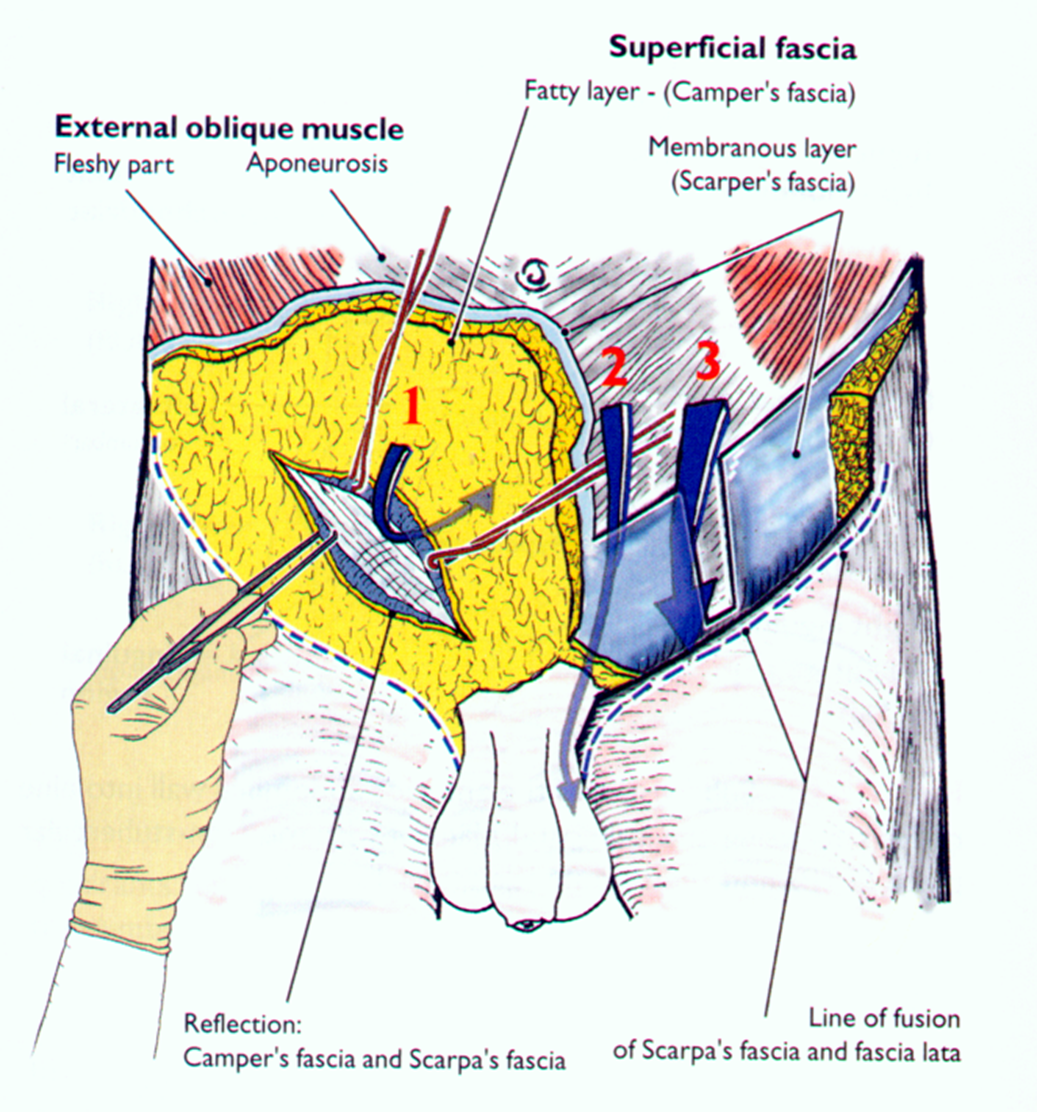
Superficial fascia has two layers
(fatty layer) – Camper’s fascia
(membranous layer) – Scarpa’s fascia
Flat muscles
External oblique
Internal oblique
Tranversus abdominis
Transversalis fascia
Extraperitoneal fascia
Peritoneum (parietal) – serous membrane that lines the peritoneal cavity
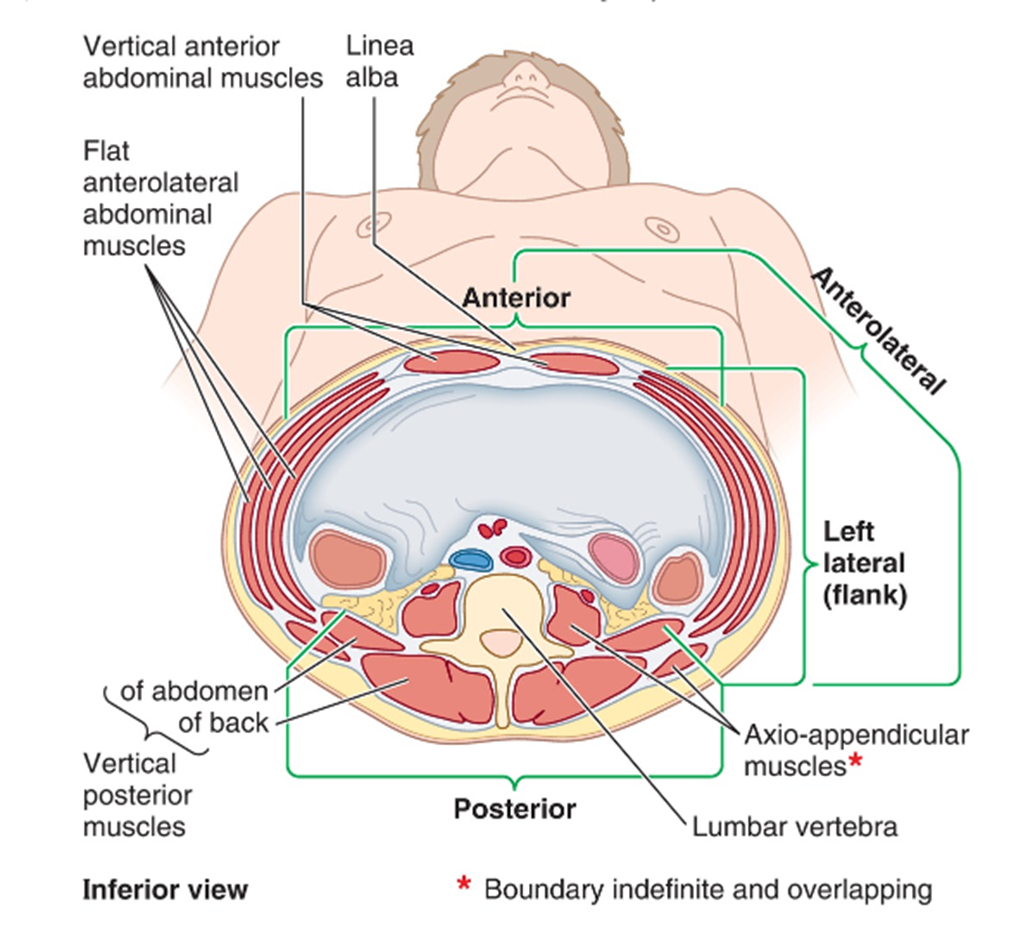
layers of anterolateral abdominal wall
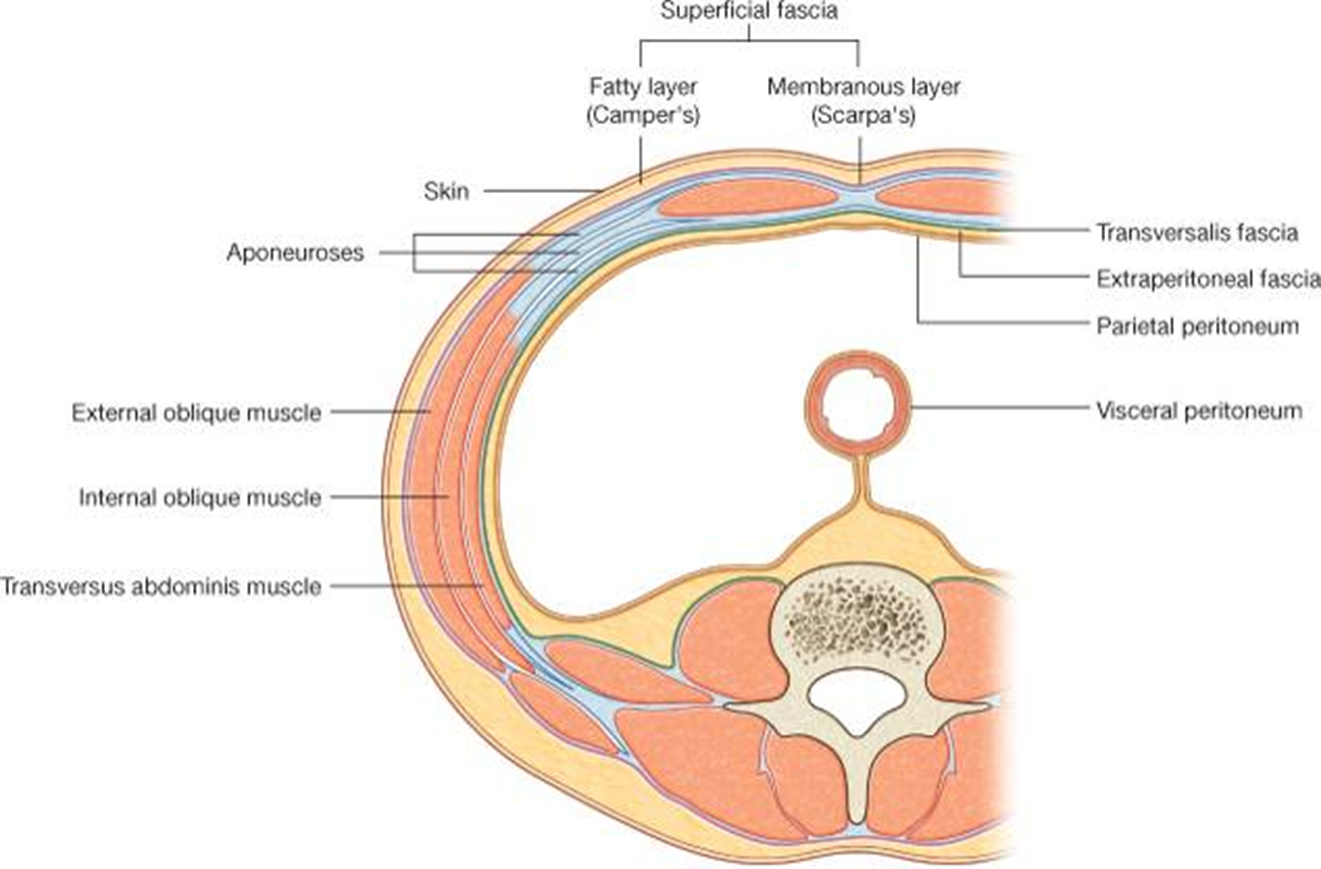
superficial fascia
In the lower abdomen, two distinct layers
Superficial fatty
Camper’s fascia
contains superficial veins
Deep membranous
Distinct below the umbilicus
Scarpa’s fascia
Gives rise to fundiform ligament of penis
Can be sutured
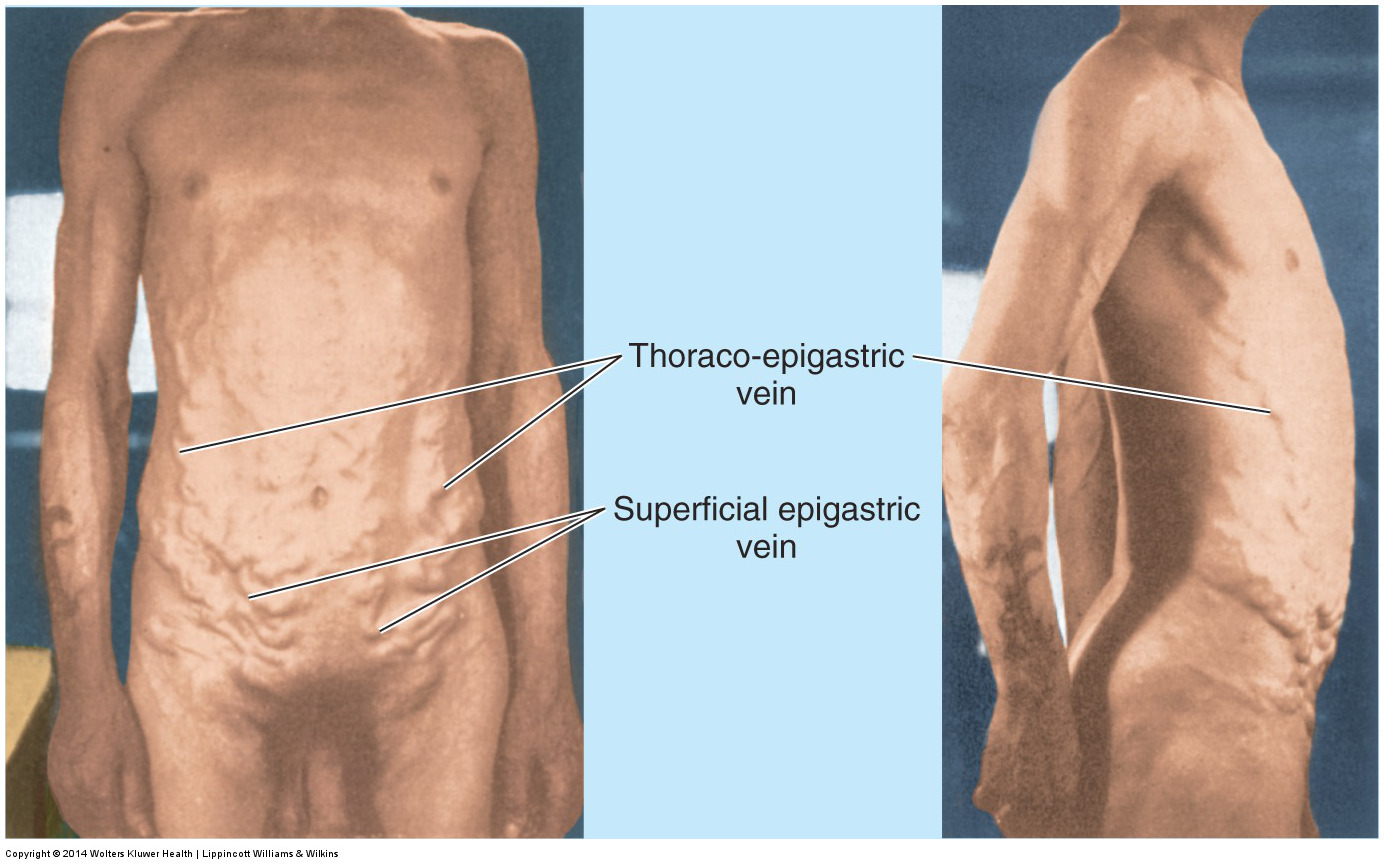
veins of anterolateral abdominal wall
cutaneous veins around the umbilicus anastomose with paraumbilical veins, which are small tributaries of the portal vein, which run along the round ligament of the liver.
They run along the obliterated umbilical vein, which in the adult forms the round ligament of the liver.
The thoraco-epigastric vein (circled in red) can allow blood to return to the heart from the lower limb if the inferior vena cava is blocked.
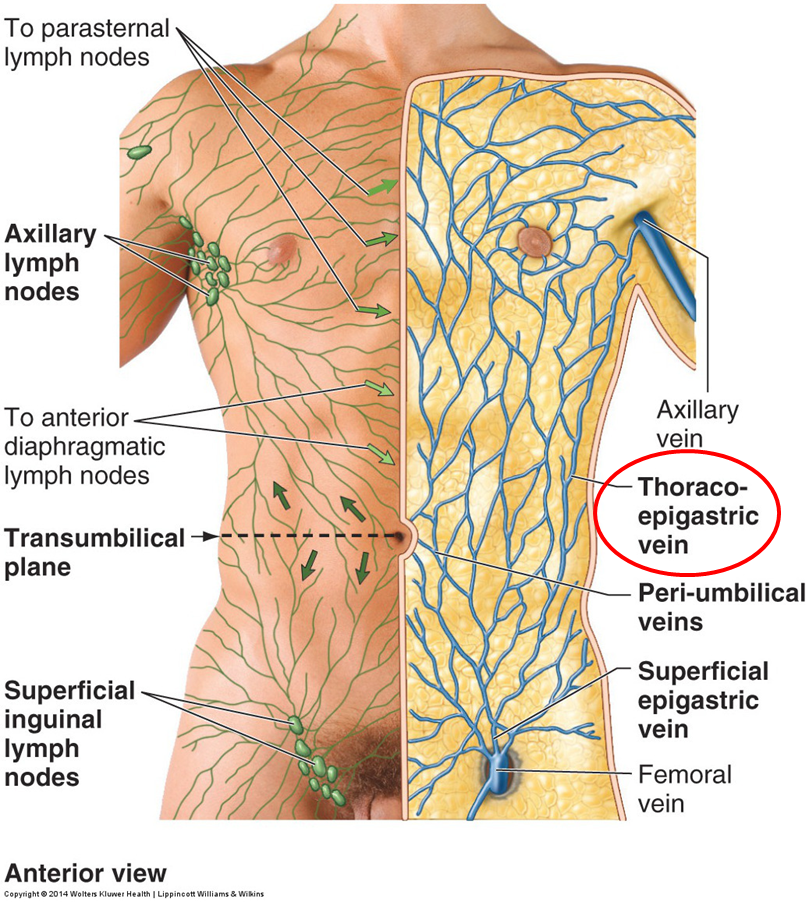
clinical note: caput medusae
Blockage of portal drainage, as in portal hypertension caused by end-stage liver disease, causes distension of the paraumbilical veins.
Can also occur with blockage of inferior vena cava.

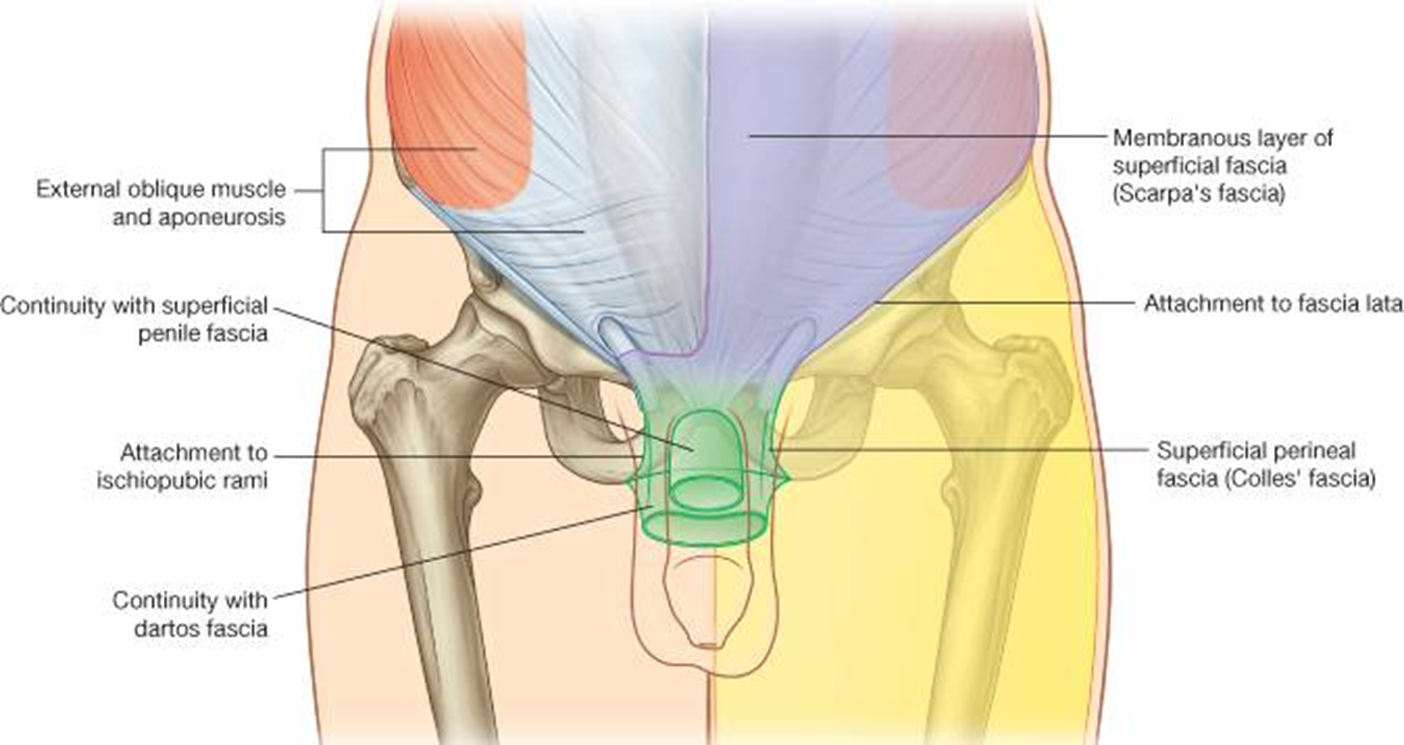
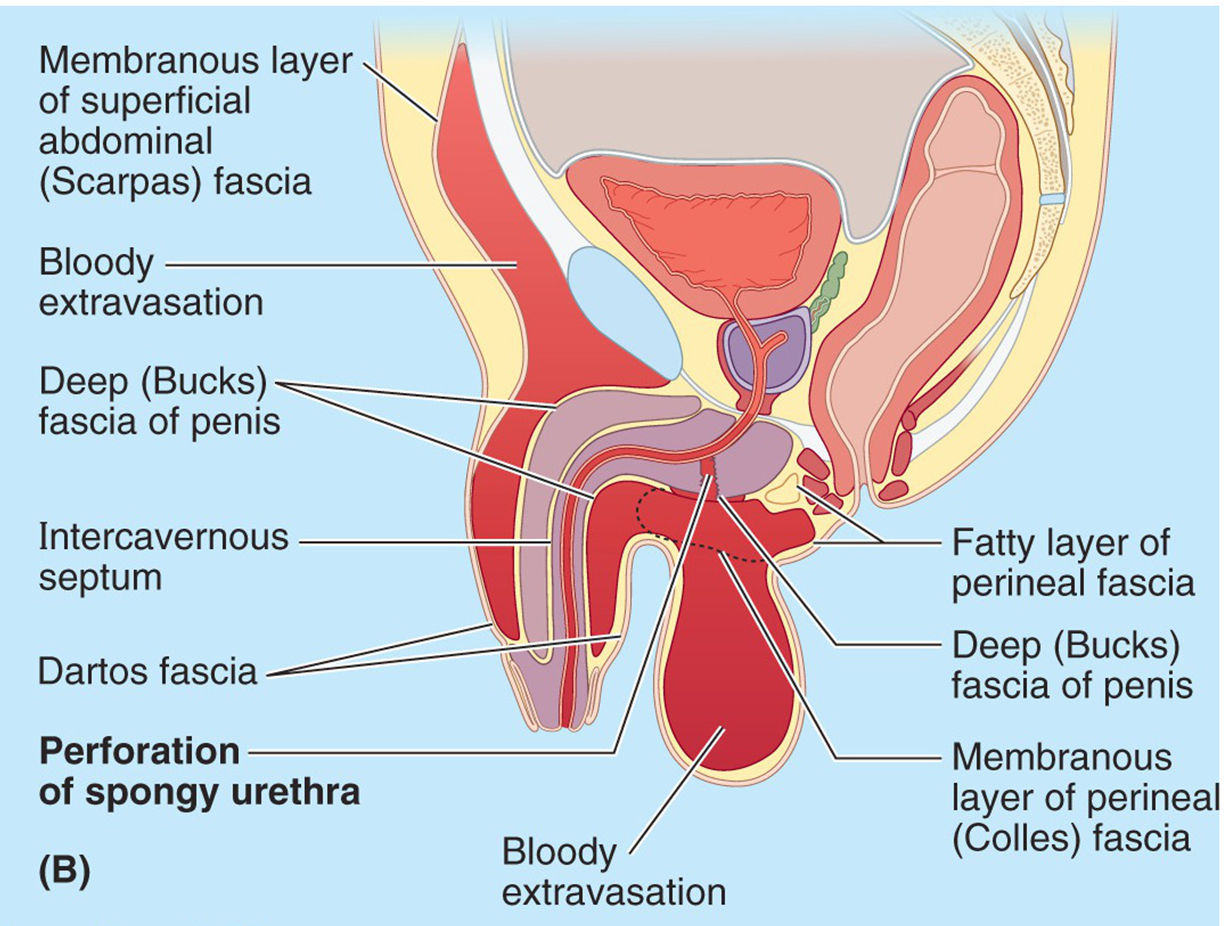
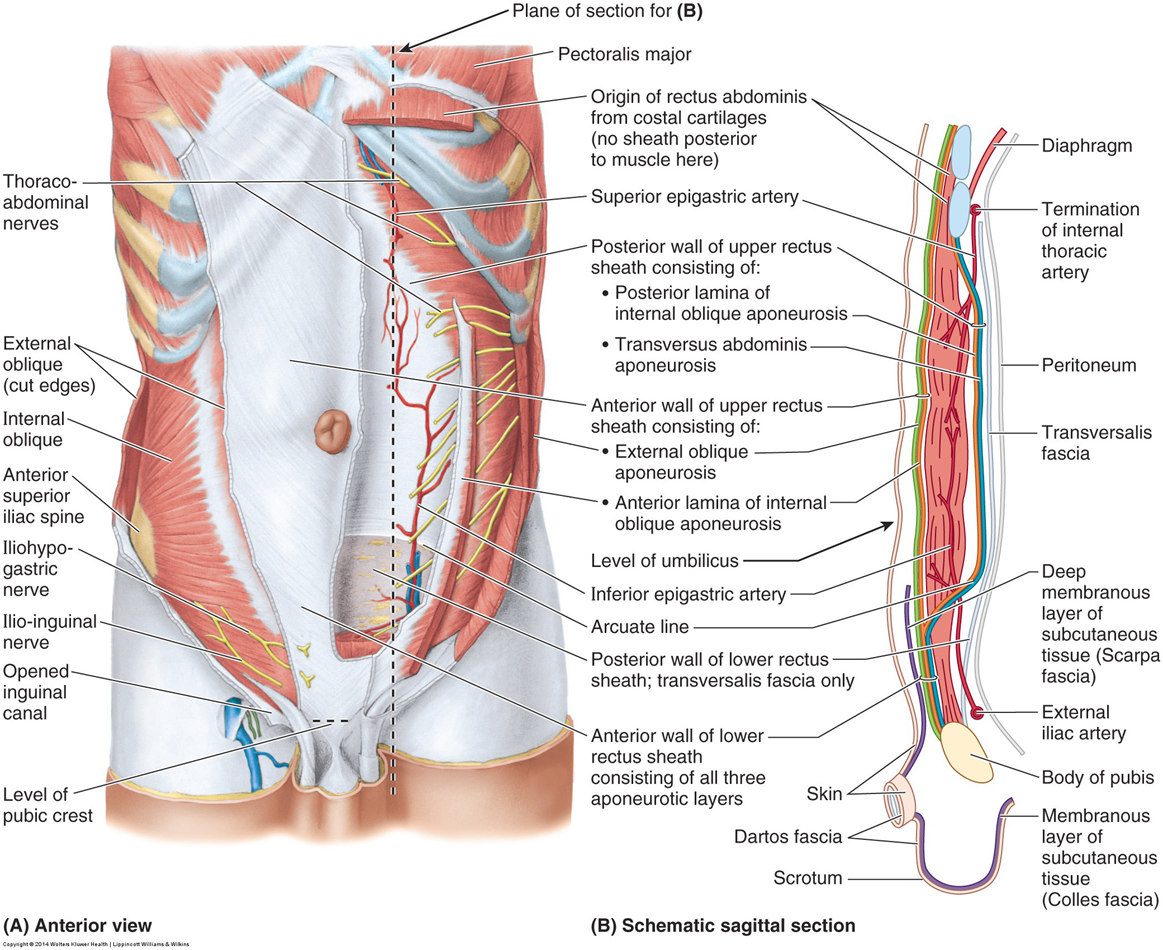
membranous layer of superficial fascia
membranous layer of the superficial fascia is continuous with Colles fascia in the perineum, the tunica Dartos of the scrotum and the superficial penile fascia.
It is tightly adherent to the fascia lata below the inguinal ligament.
There is a potential space between the membranous layer of the superficial
(Scarpa’s) fascia and the deep fascia over the external oblique muscle.
Exudate (blood) can flow into this space.
clinical note: urinary extravasion
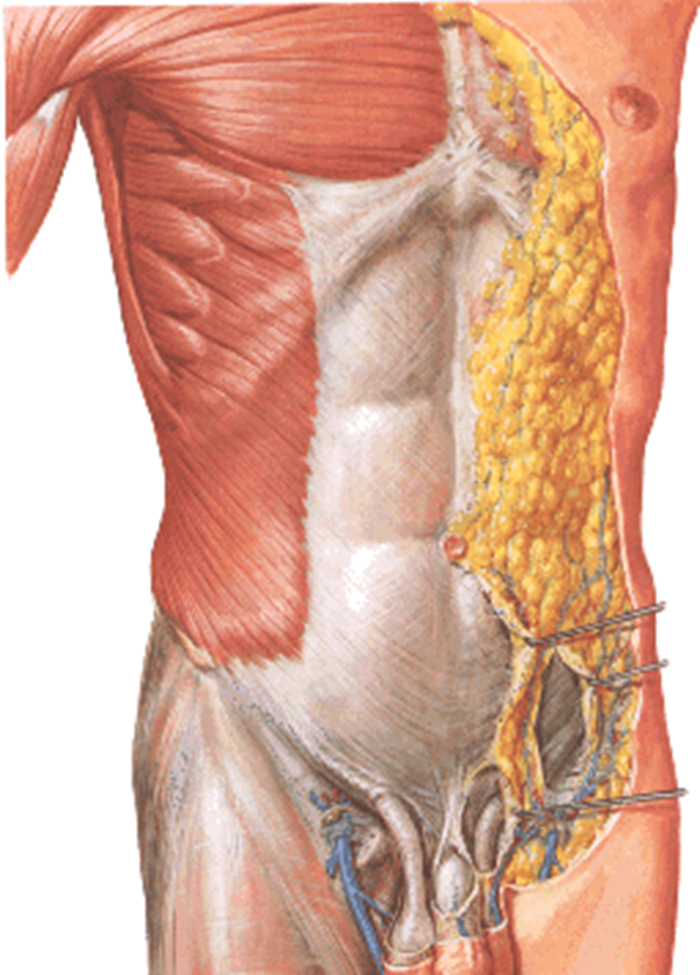
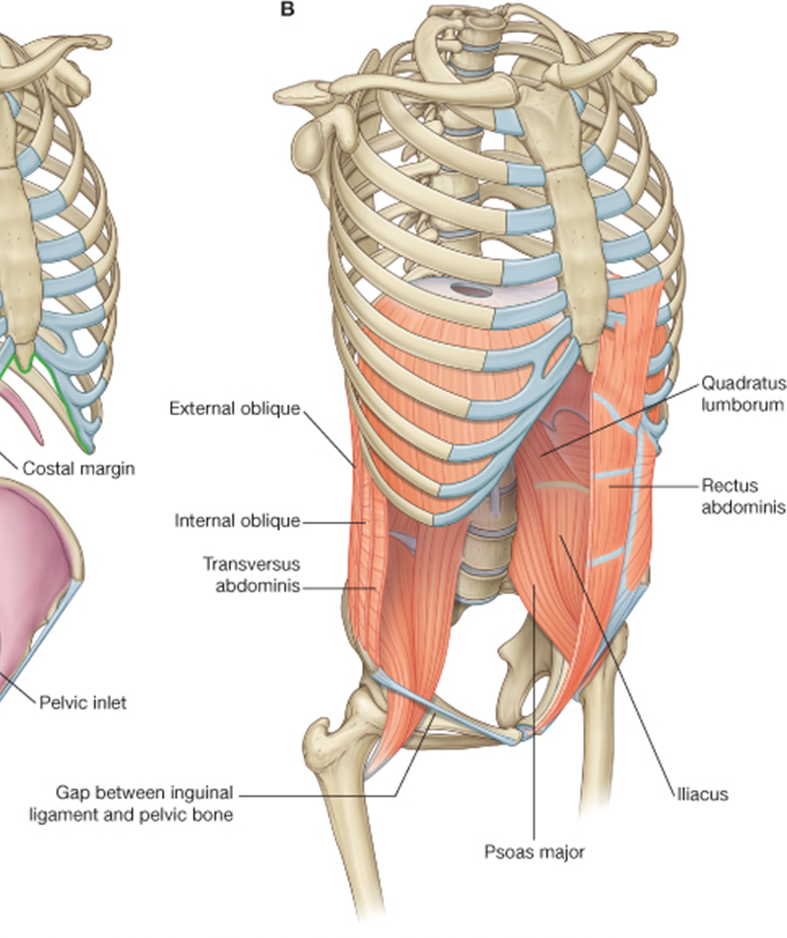
muscles of abdominal wall
Posteriorly
Quadratus lumborum
Psoas major
Iliacus
Anterolaterally
Transversus abdominis
Internal oblique
External oblique
Rectus abdominis
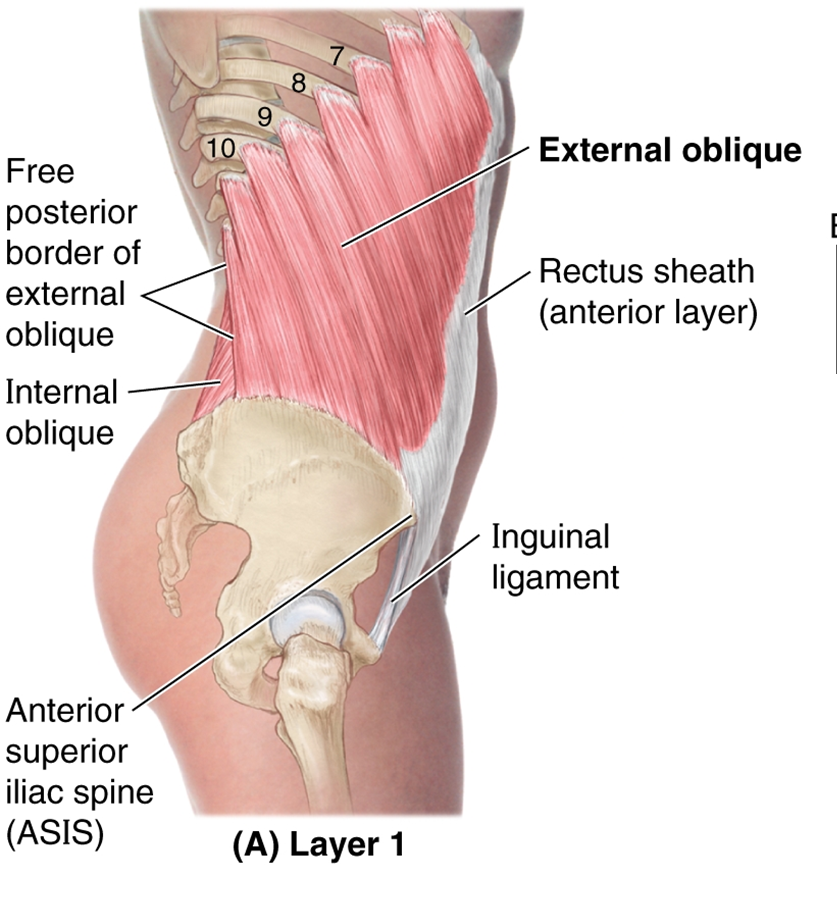
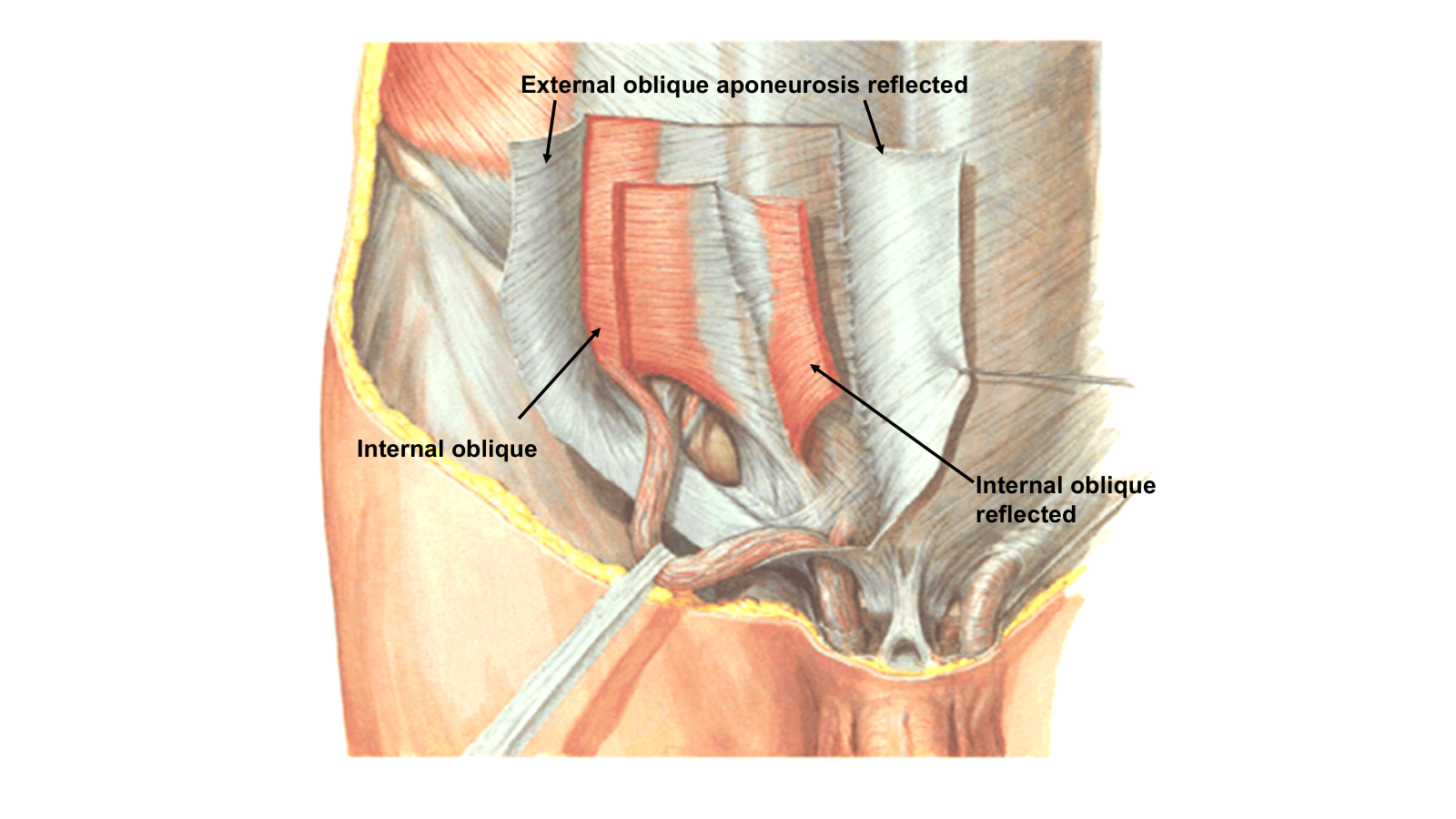
external oblique muscle
Origin: Outer surface of ribs 6-12
Insertion
Linea alba
Pubic tubercle
Anterior ½ of iliac crest
Free margin forms inguinal ligament
Aponeurotic fibers form external spermatic fascia
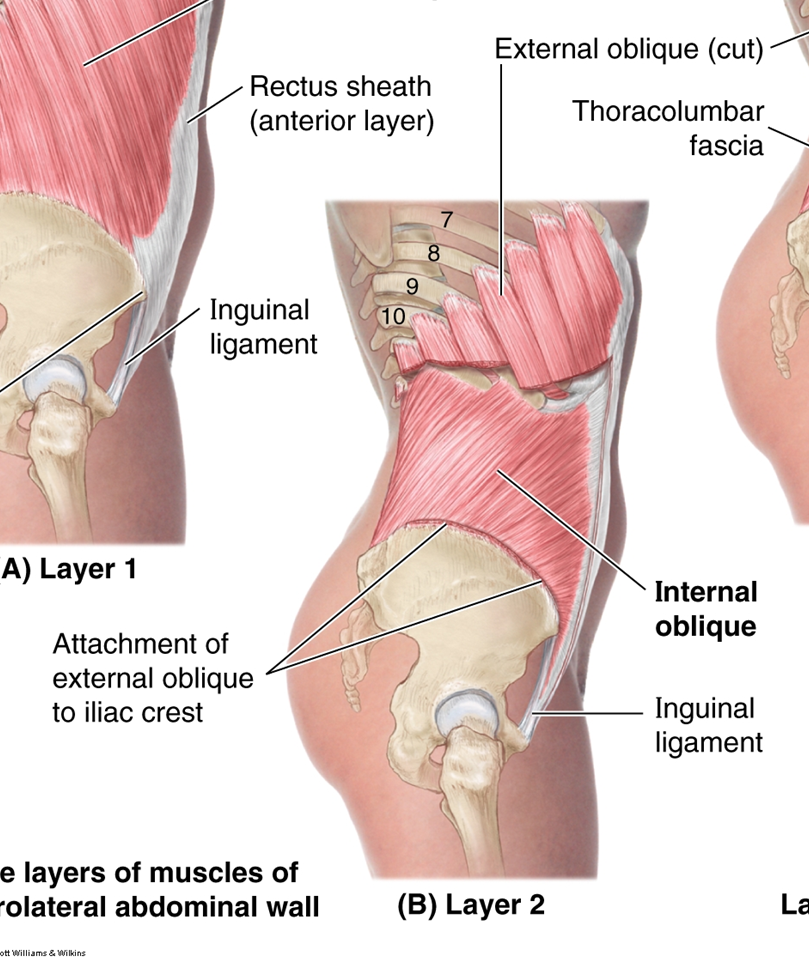
internal oblique muscle
Origin
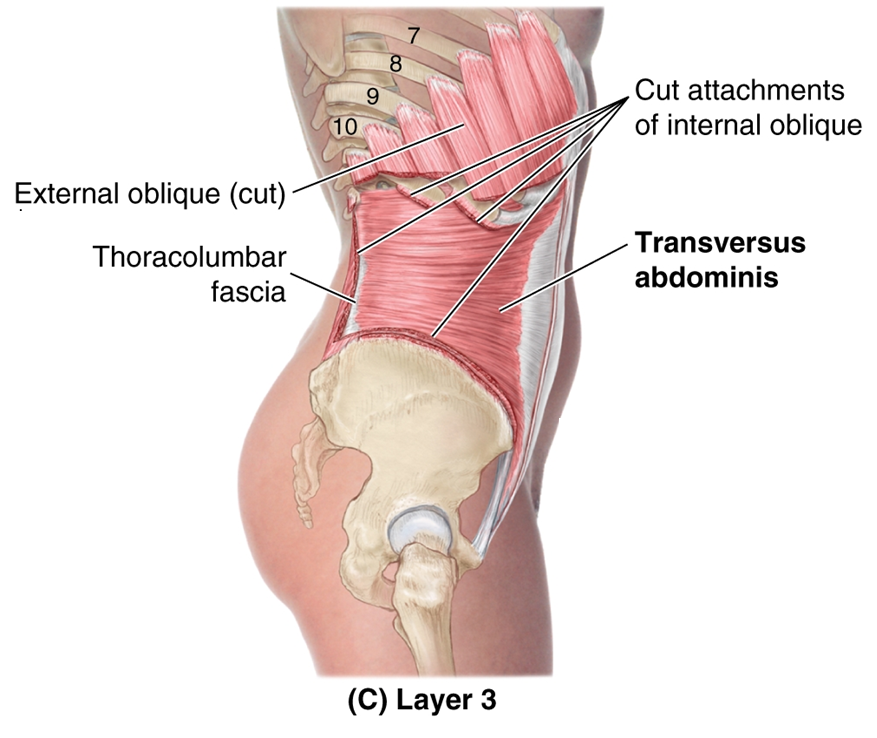
Thoracolumbar fascia
Anterior 2/3 of iliac crest
Lateral ½ of inguinal ligament
Insertion
Inferior borders 10-12th ribs
Linea alba
Pecten pubis via conjoint tendon
Gives rise to cremaster muscle
transversus abdominis muscle
origin
Inner surfaces of 7th-12th costal cartilages
Thoracolumbar fascia
Iliac crest
Lateral 1/3rd of inguinal ligament
insertion
Linea alba
Pubic crest
Pecten pubis via conjoint tendon
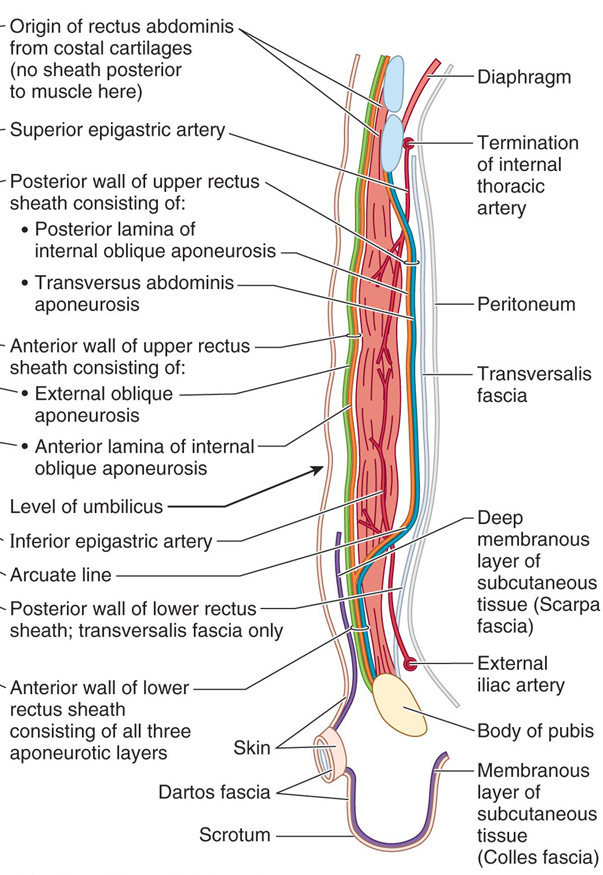
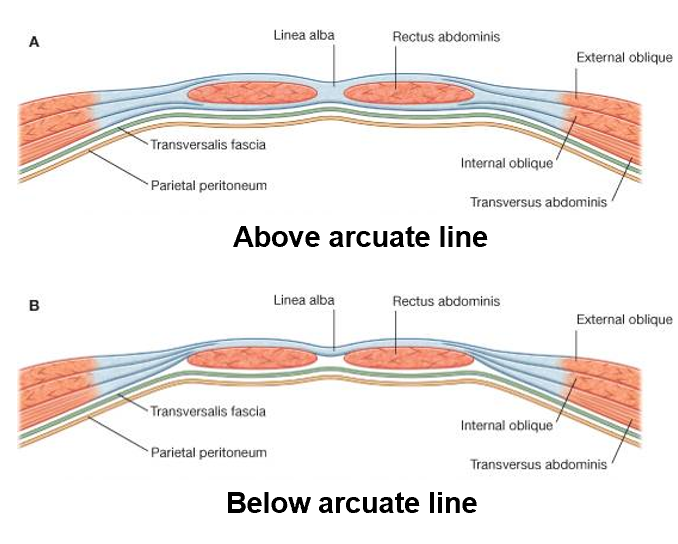
transversalis fascia
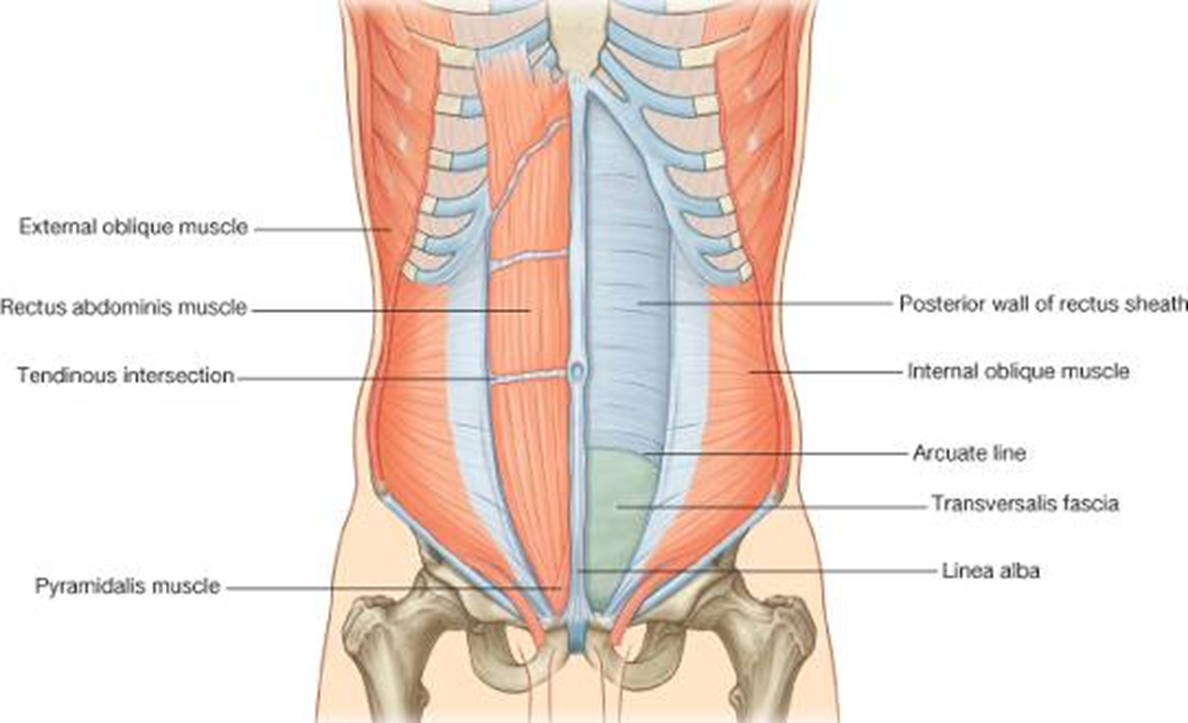
Helps form posterior wall of rectus sheath above arcuate line
Forms posterior wall of rectus sheath below arcuate line
Continues over spermatic cord as internal spermatic fascia
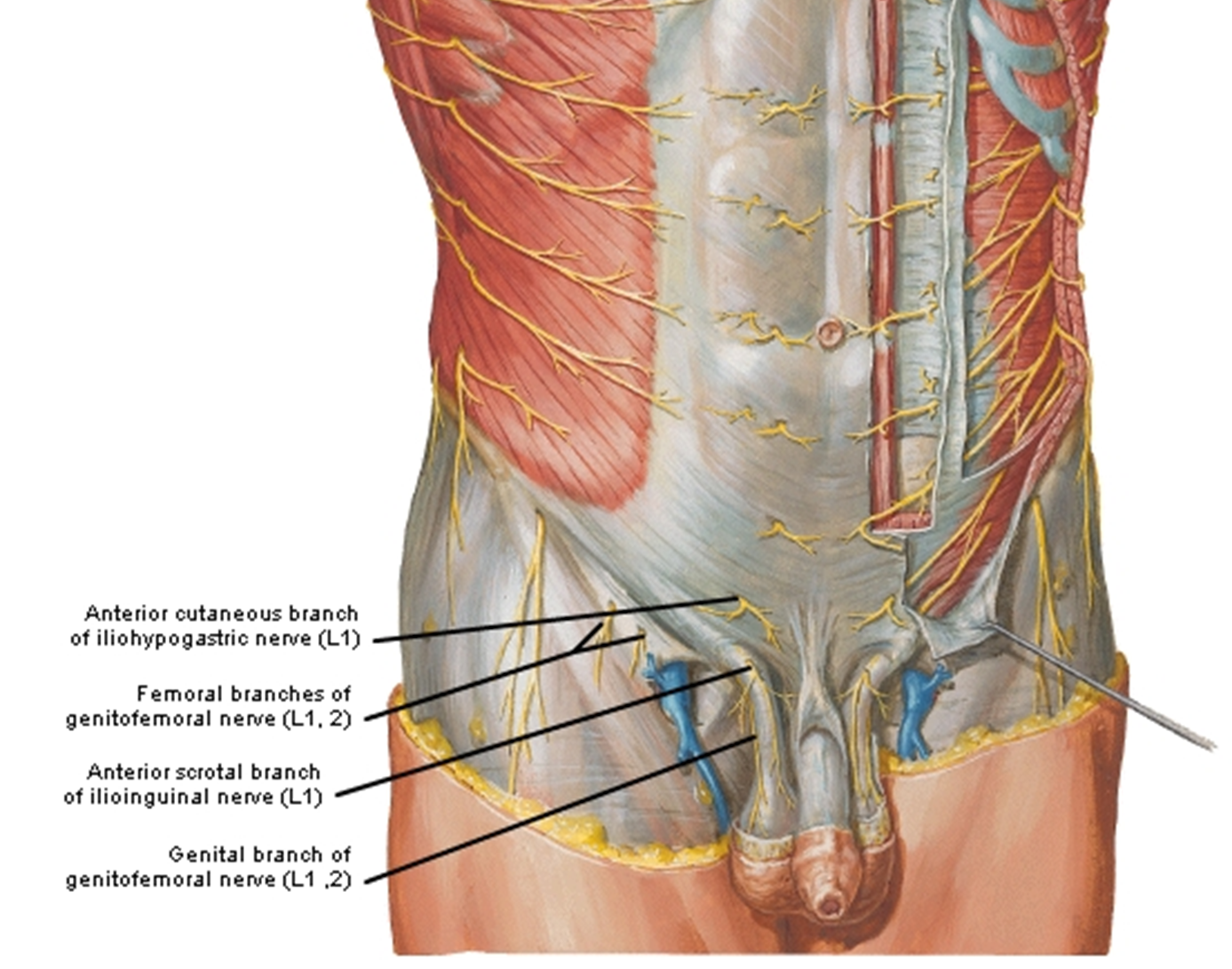
innervation
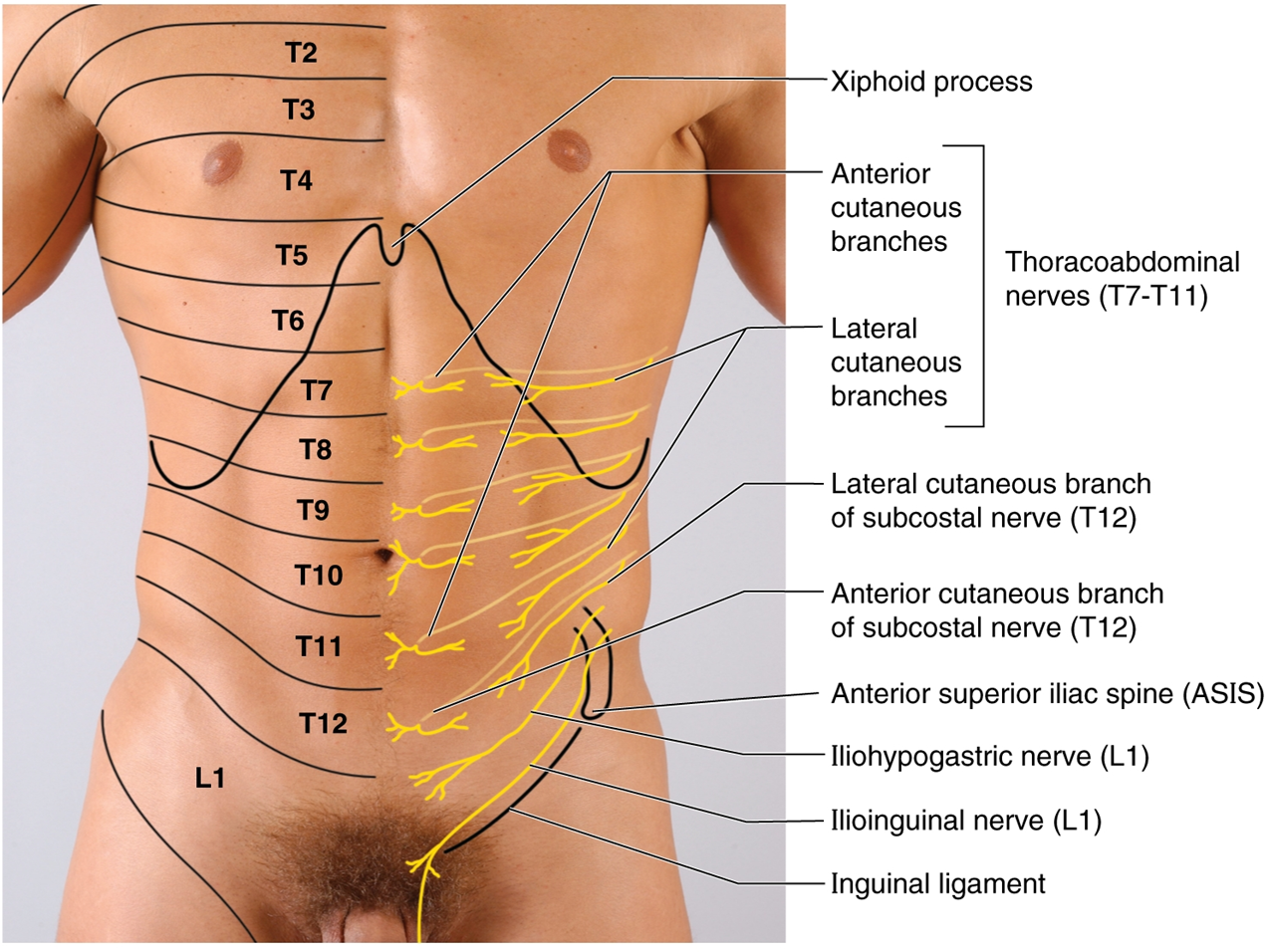
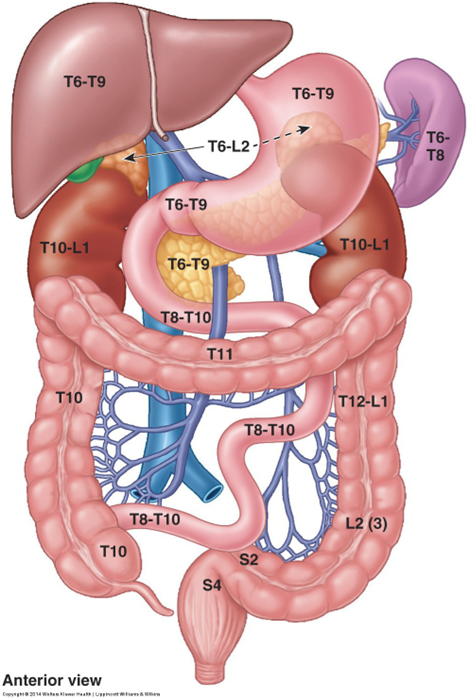
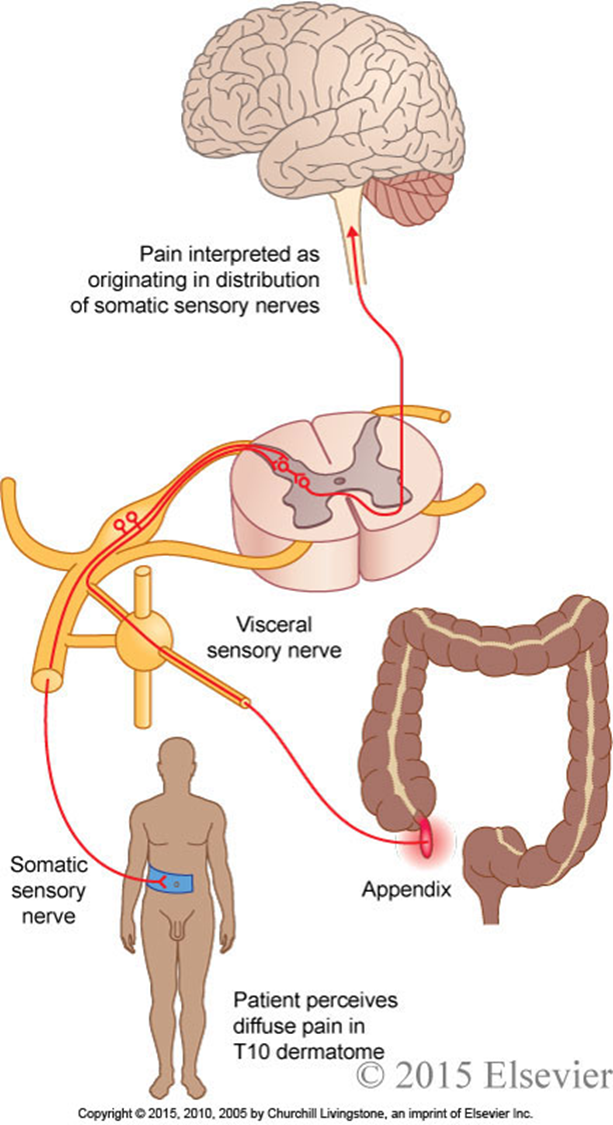
clinical note: referred pain
Pain associated with visceral disease and inflammation is referred to the abdominal wall.
This is because visceral afferents enter the spinal cord with somatic afferents.
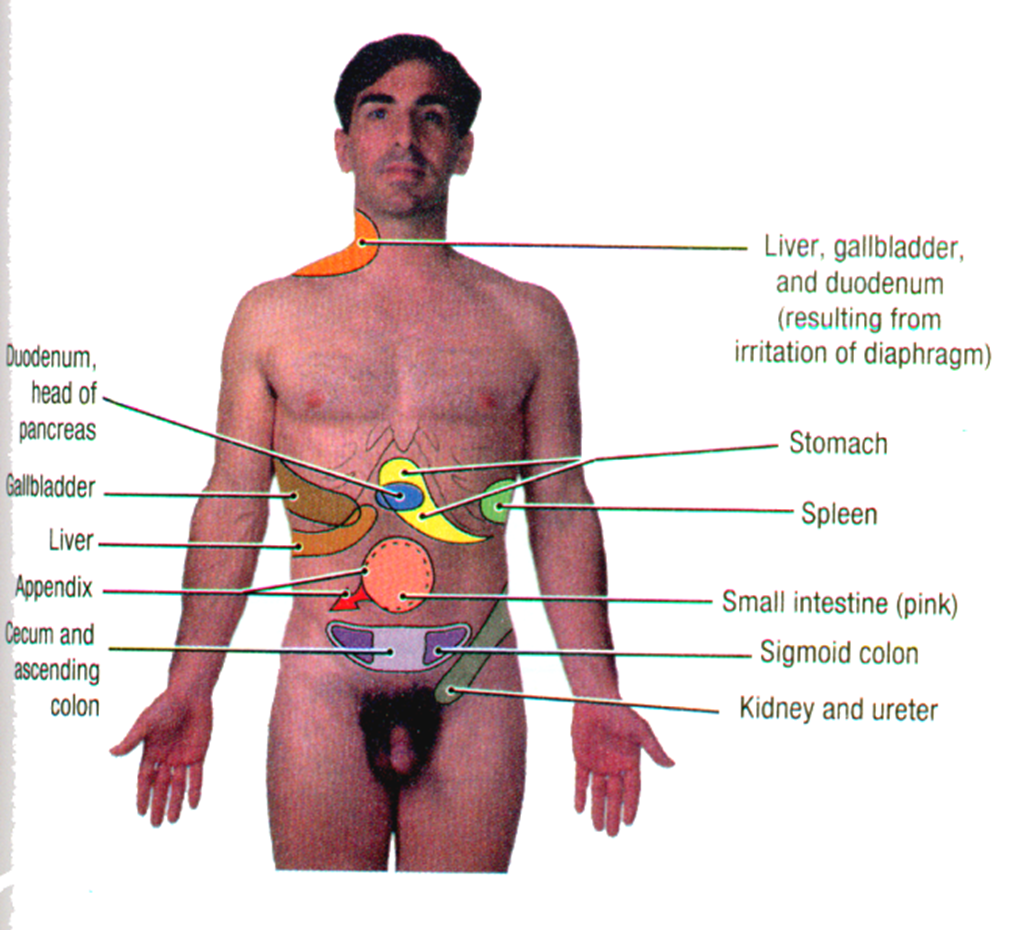
Pain associated with visceral disease and inflammation is often referred to the body wall.
The visceral nociceptive (pain) afferents enter the spinal cord with somatic afferents and synapse on the same second-order neurons.
All visceral pain fibers run with the sympathetic system (except below the pelvic pain line) and enter the spinal cord at the same segment that gives rise to the preganglionic efferents.
The example to the right is referred pain from the appendix, which is often referred to the T10 dermatome.
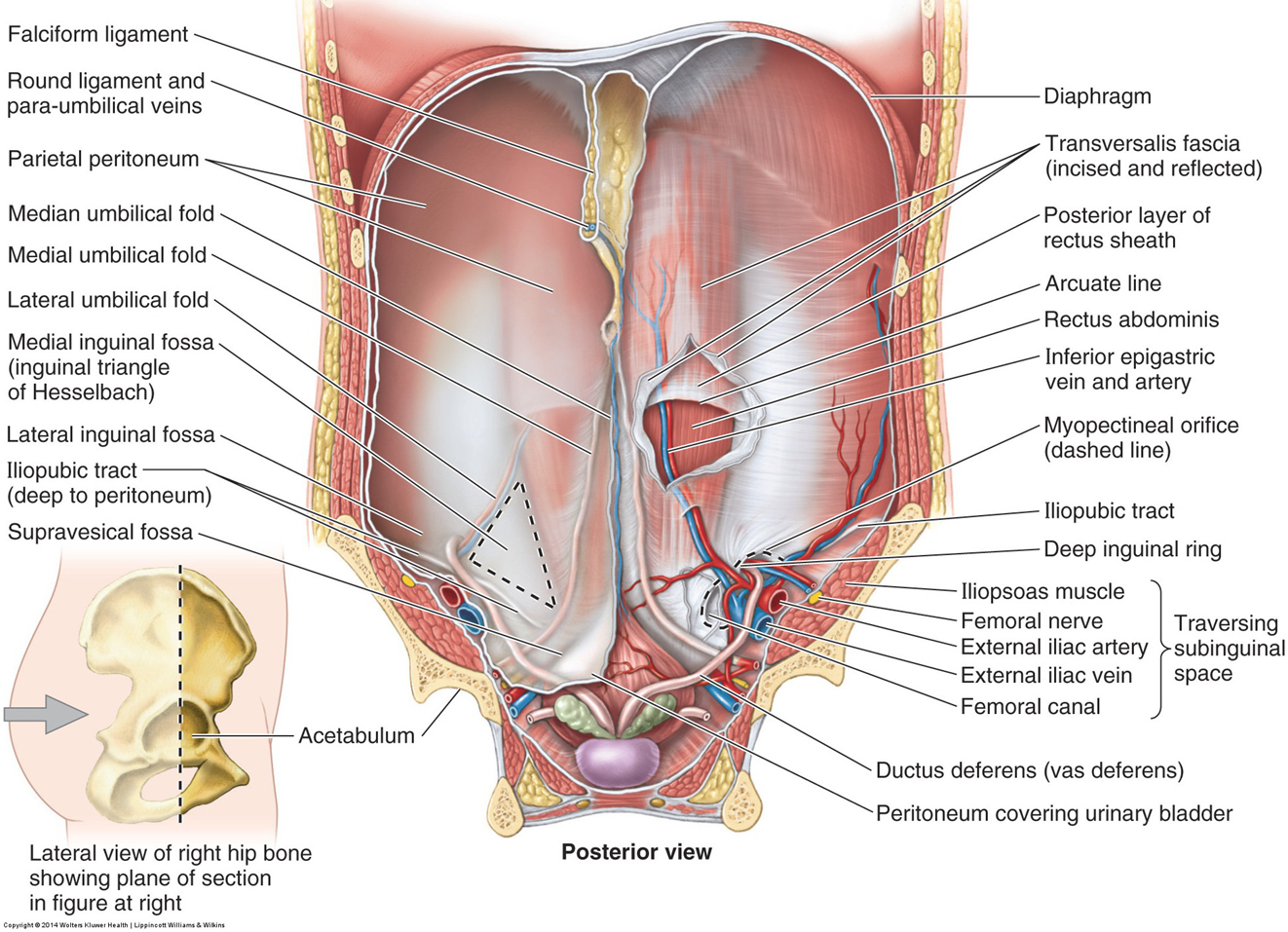
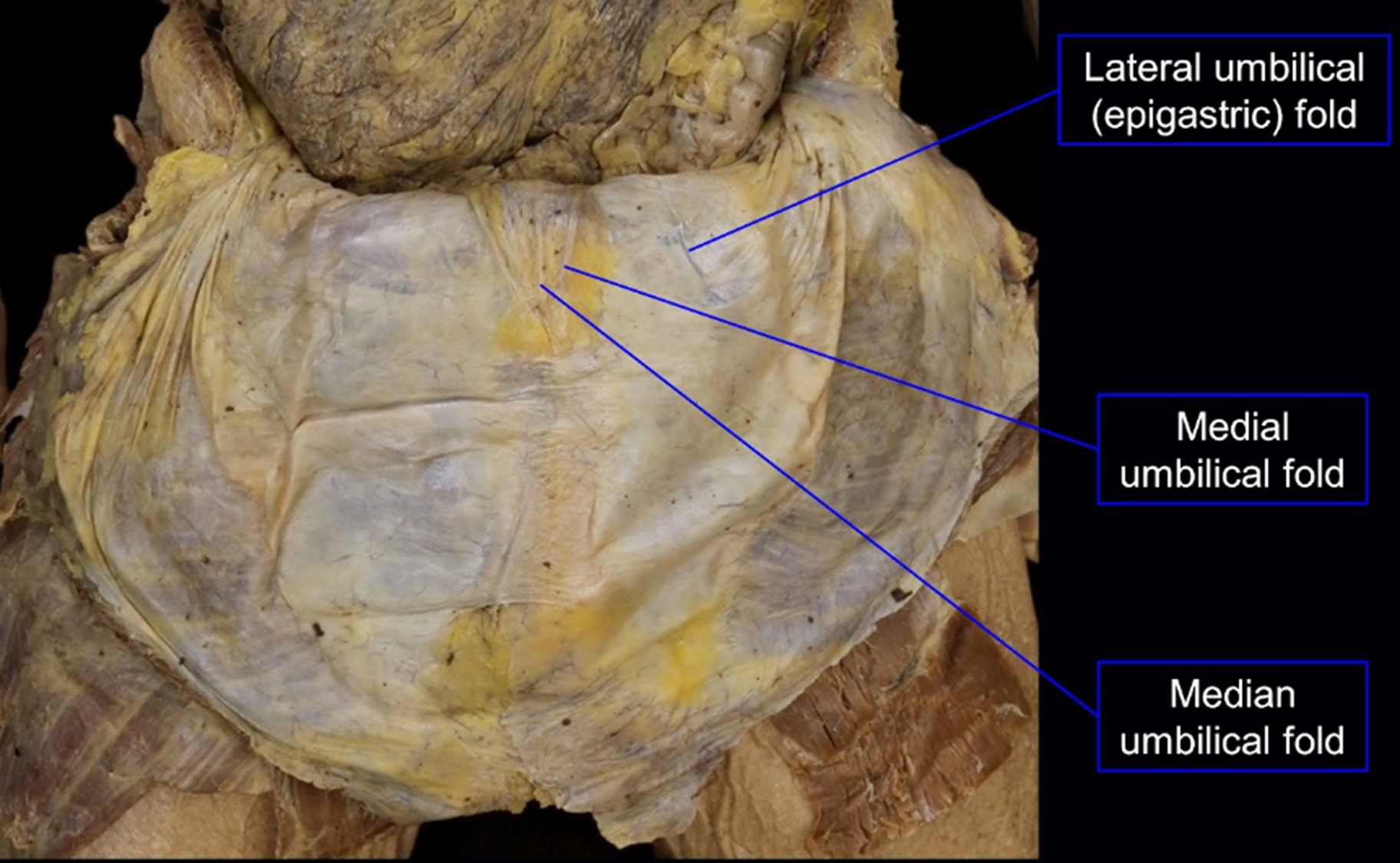
interior: anterolateral abdominal wall
Lateral fold
- Inferior epigastric vessels
Medial fold
- Obliterated umbilical artery
Median fold
- Urachus
rectus abdominis muscle & sheath
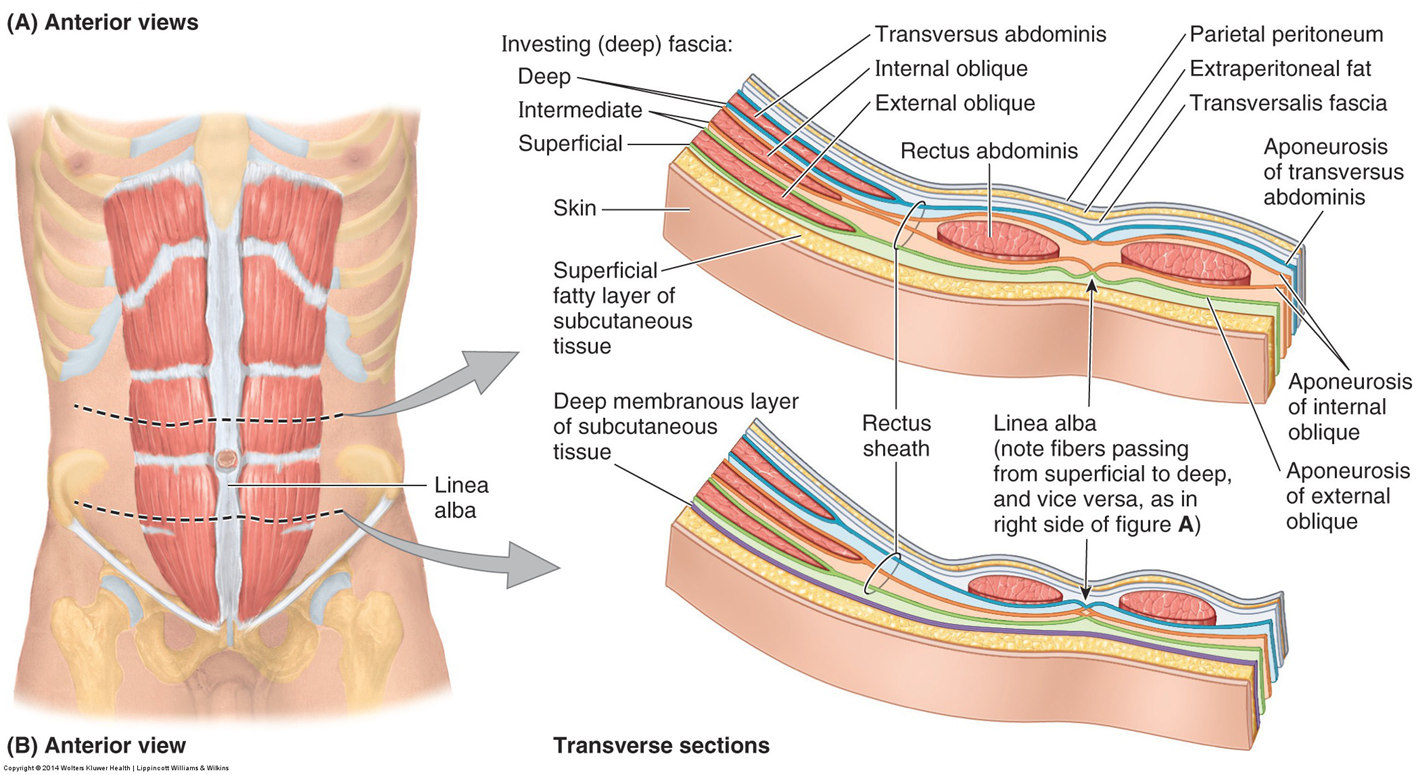
rectus sheath
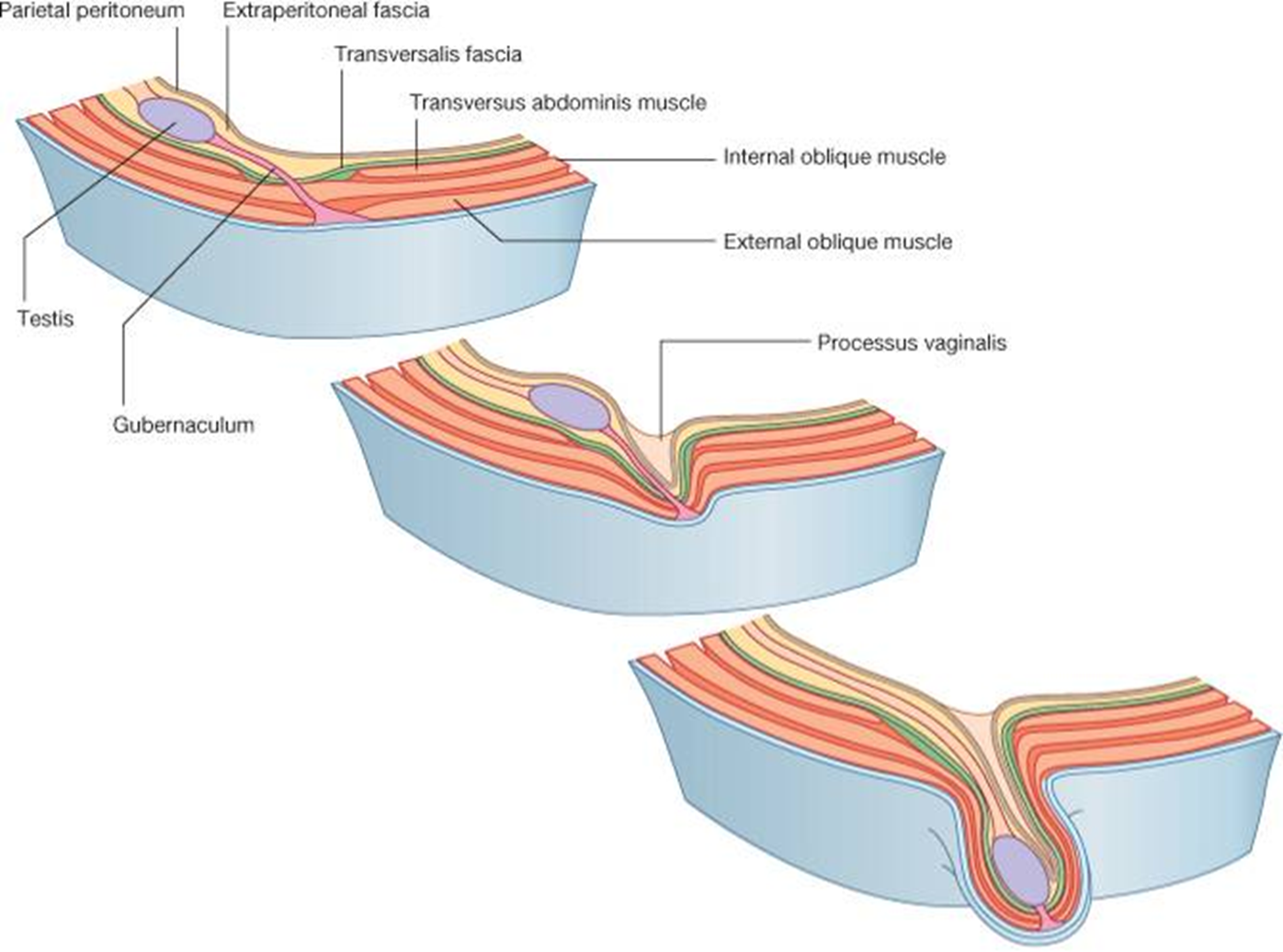
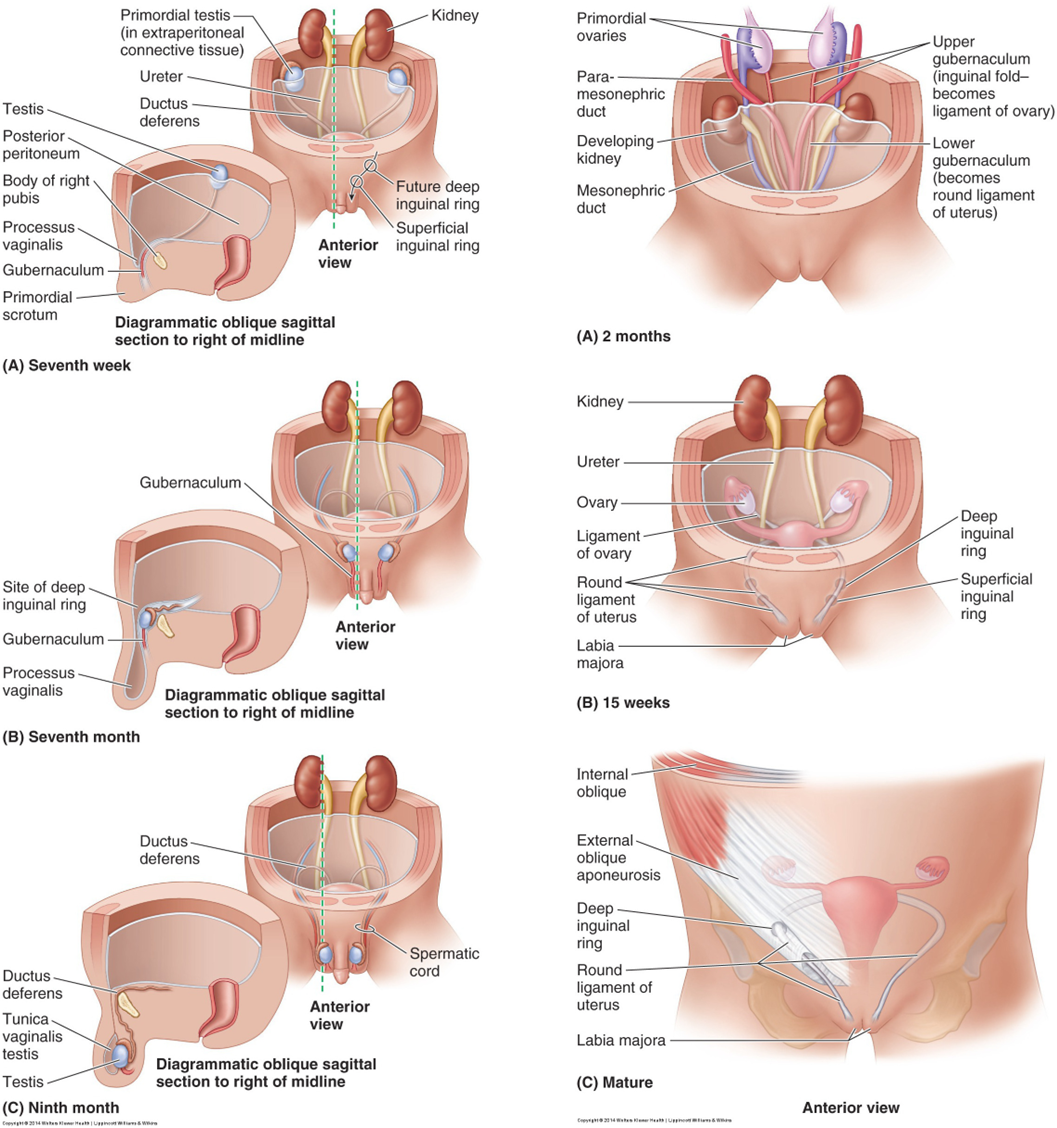
what is the scrotum & why do male mammals have one?
scrotum is an outgrowth of the anterior abdominal wall that occurs developmentally in the inguinal region.
Sperm production in post-pubertal males require the testis to be kept below body temperature (approximately 35-42 degrees Fahrenheit).
As the anterior abdominal wall evaginates, the testis descends behind the abdominal peritoneum to eventually lie behind the processus vaginalis, an extension of peritoneum into the scrotum.
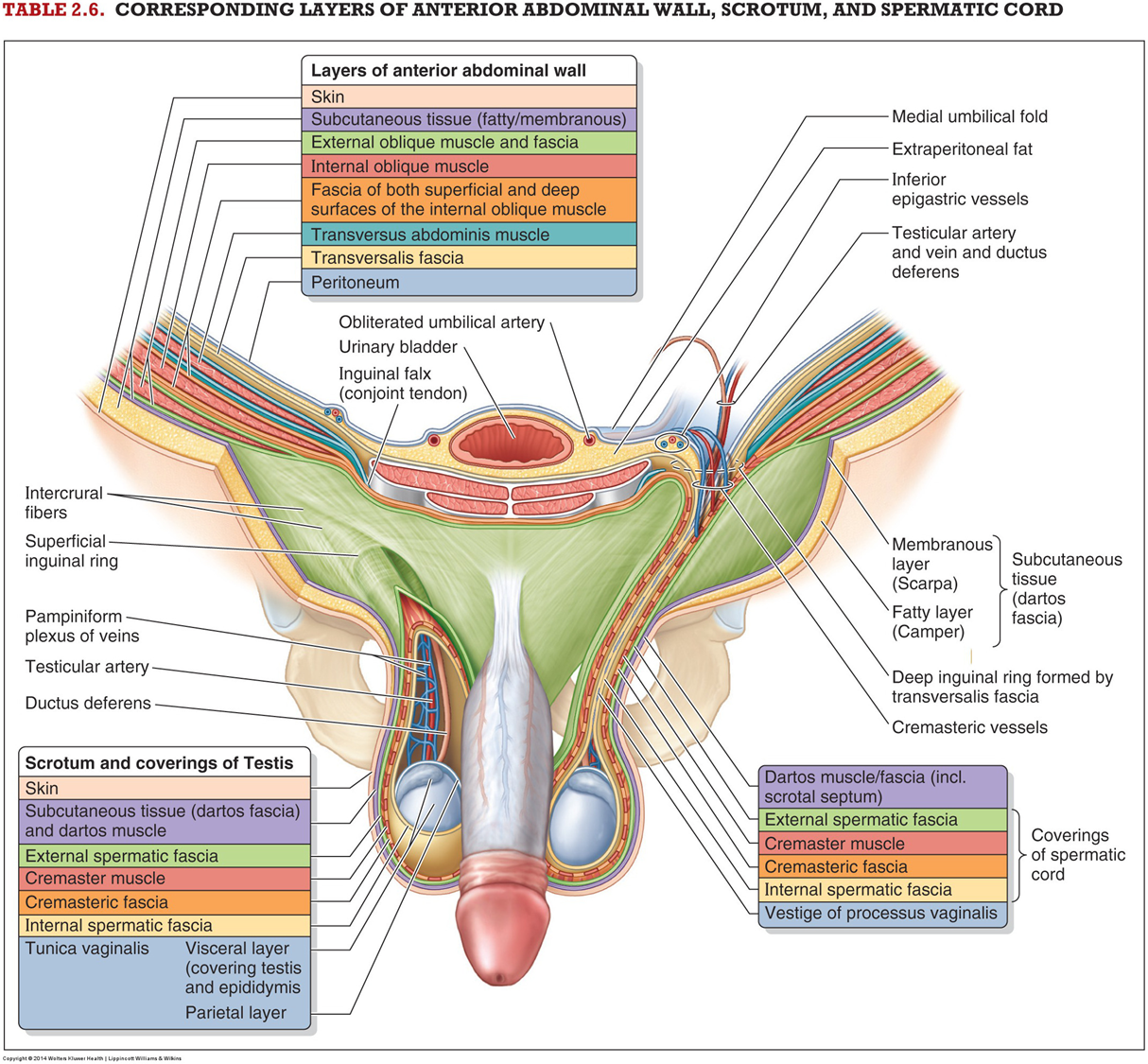
During testicular descent, the spermatic cord, which contains the ductus deferens, gonadal vessels, etc., takes on coverings derived from the layers of the abdominal wall.
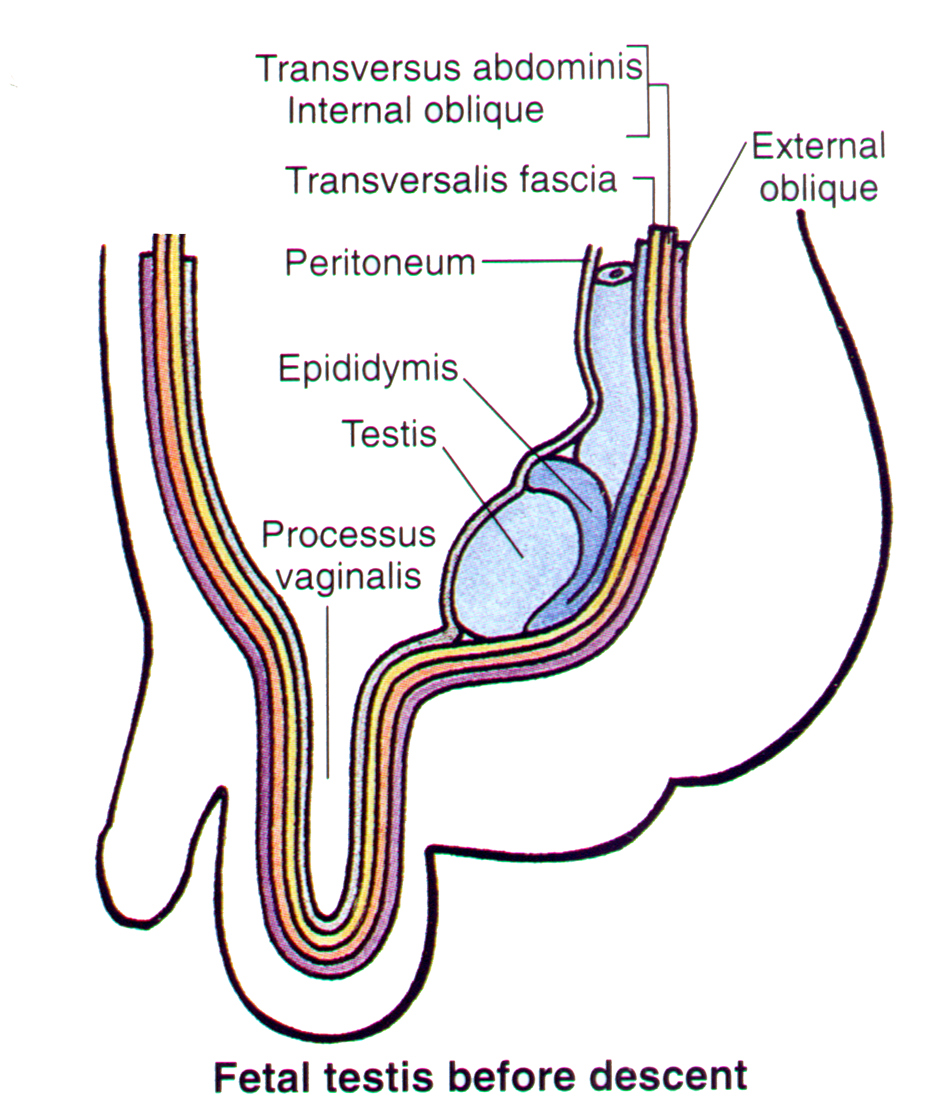
descent of testis occurs beneath or behind abdominal peritoneum
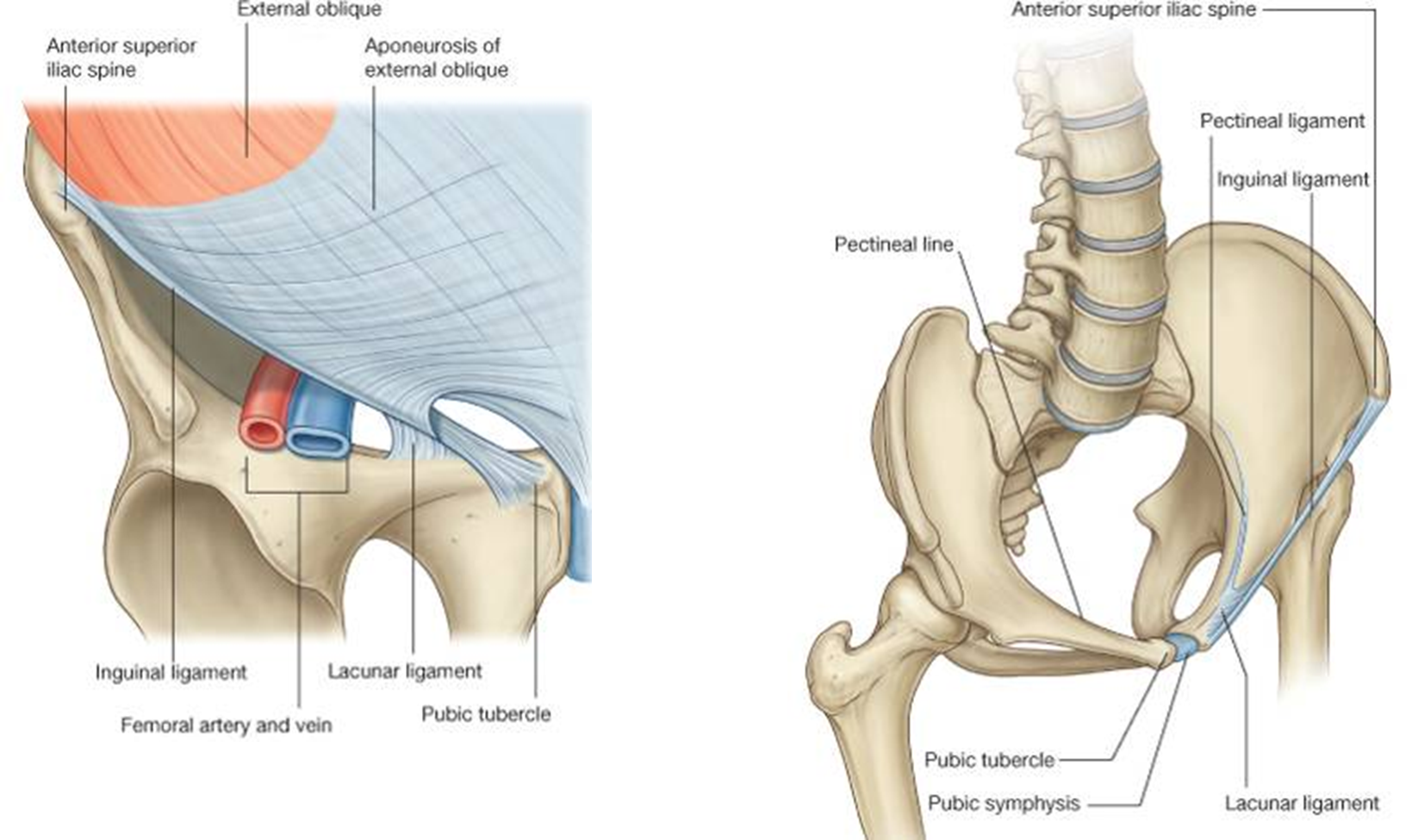
inguinal ligament
Conjoint tendon, AKA falx inguinalis, is formed by the joined insertions of the internal oblique and the traversus abdominis muscles into the pubic crest and the pectinate line. It forms the medial 1/3rd of the posterior wall of the inguinal canal.
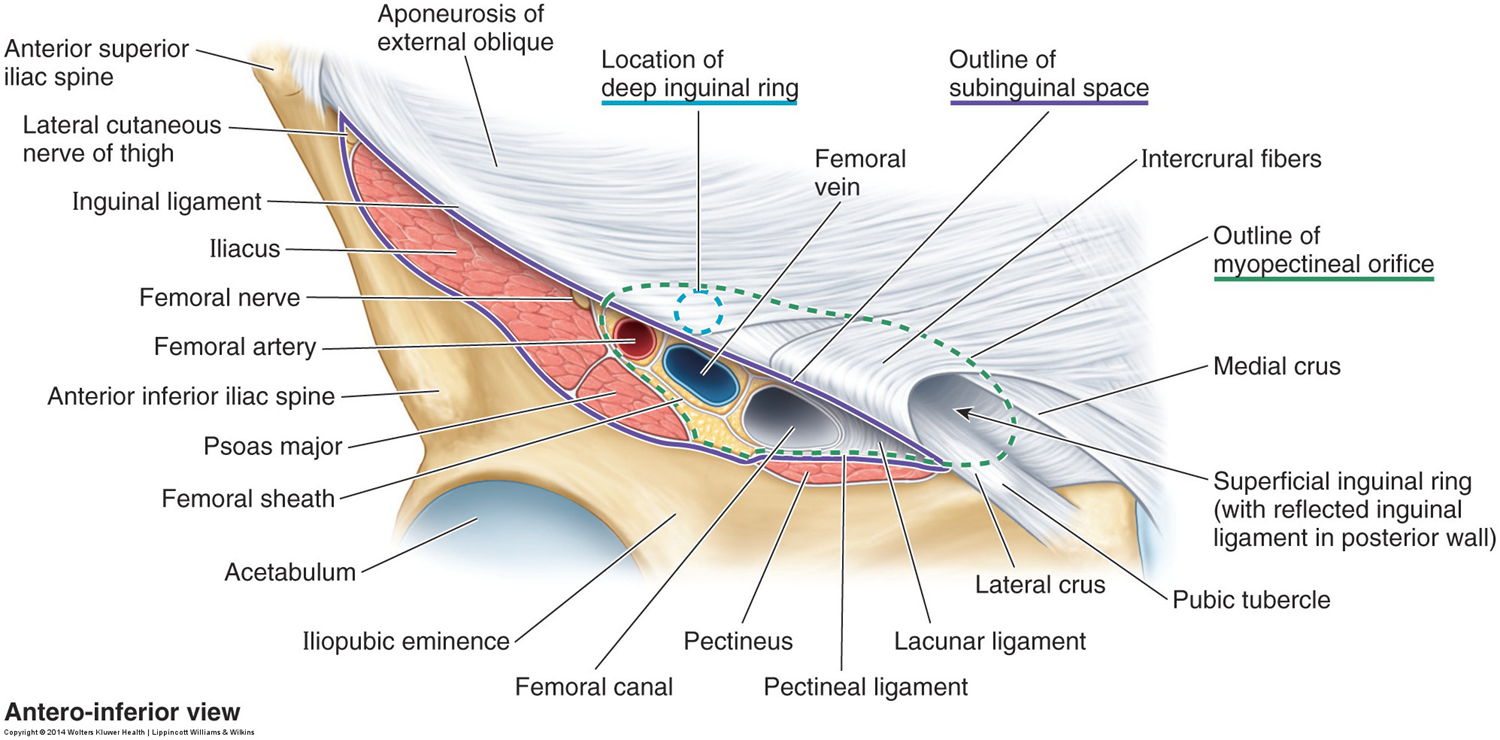
inguinal region (groin)
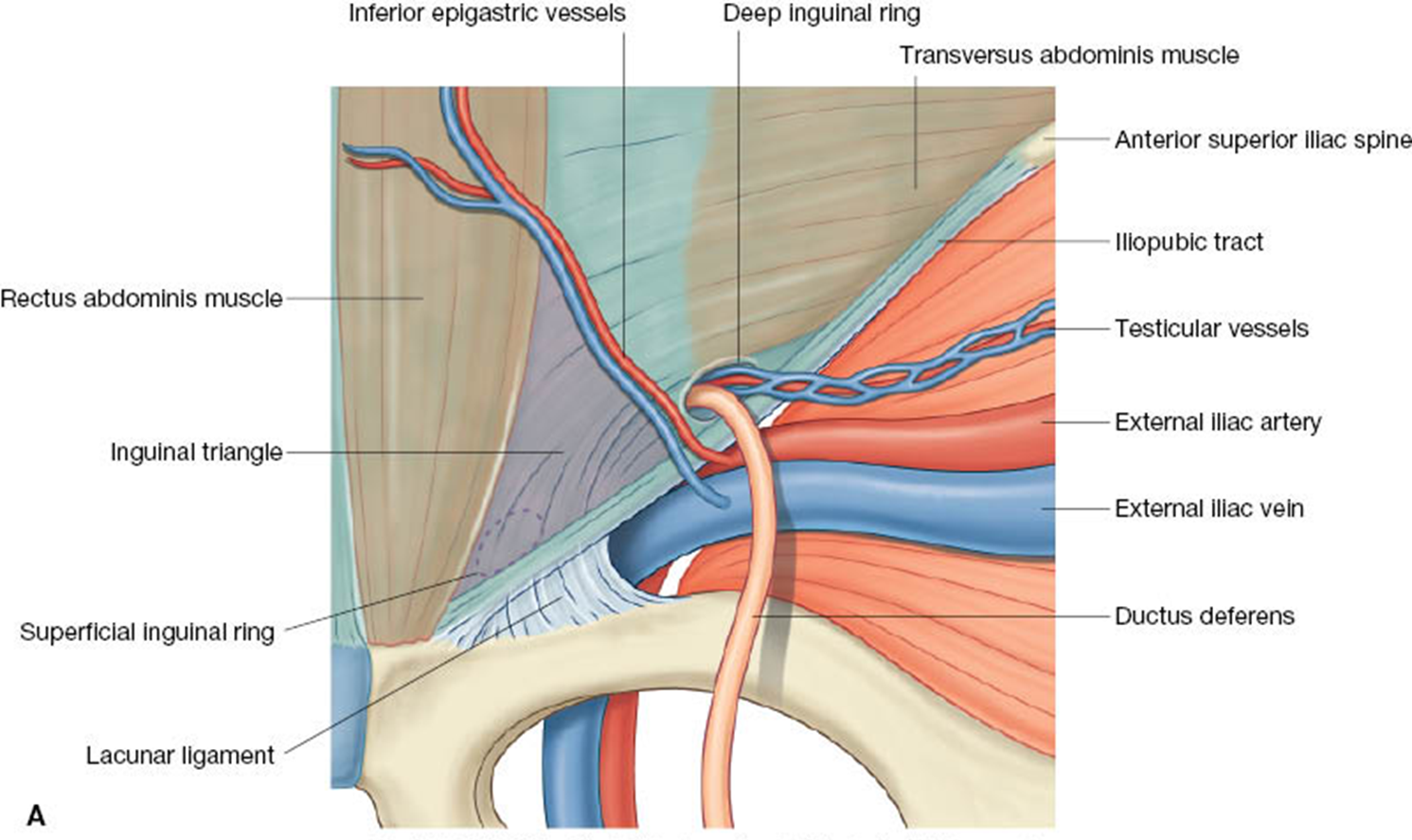
The deep ring lies superior to the inguinal ligament, medial to the femoral artery and lateral to the inferior epigastric vessels. The superficial ring lies just superior to the pubic tubercle.
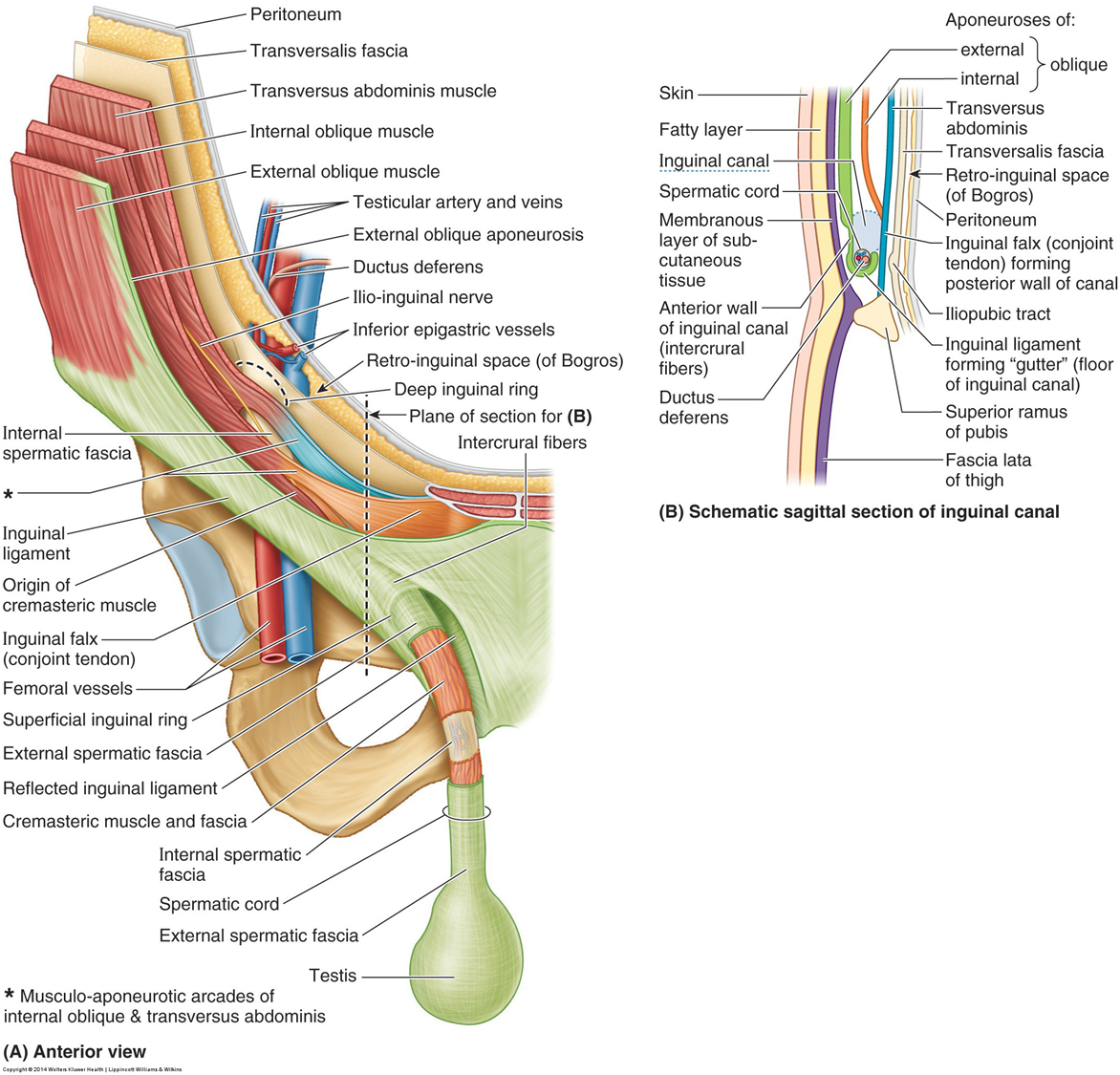
inguinal canal
The inguinal canal is a short (4cm), oblique, passage directed inferomedially through the inferior part of the anterolateral abdominal wall. It lies parallel and superior to the inguinal ligament. Passing through it, in the male, is the spermatic cord and, in the female, the round ligament of the uterus.
development of inguinal canal M vs F
deep & superficial rings
deep inguinal ring
Beginning of inguinal canal
Located midway between the ASIS and the pubic symphysis
Beginning of a tubular evagination of the transversalis fascia (internal spermatic fascia)
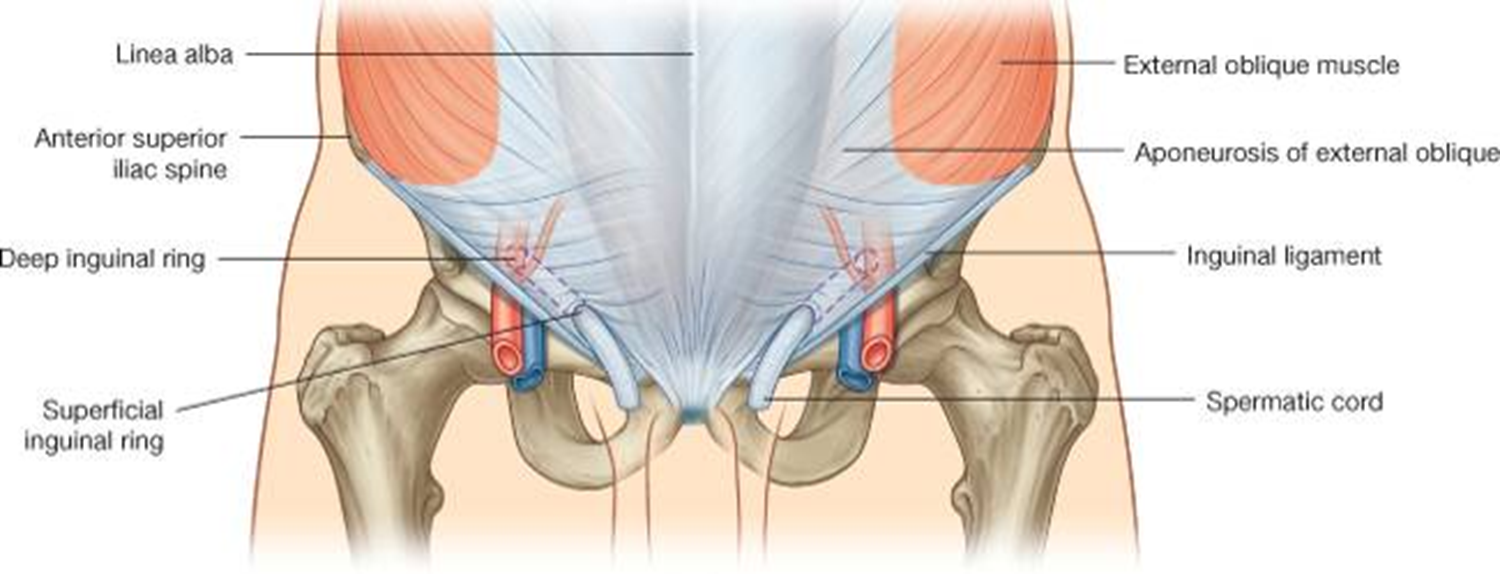
superifical inguinal ring
End of the inguinal canal
Superior to the pubic tubercle
Beginning of a tubular evagination of the aponeurosis of the external oblique muscle (external spermatic fascia)
Floor, Roof and Walls of the Inguinal Canal
Floor: medial ½ of the inguinal ligament and the lacunar ligament
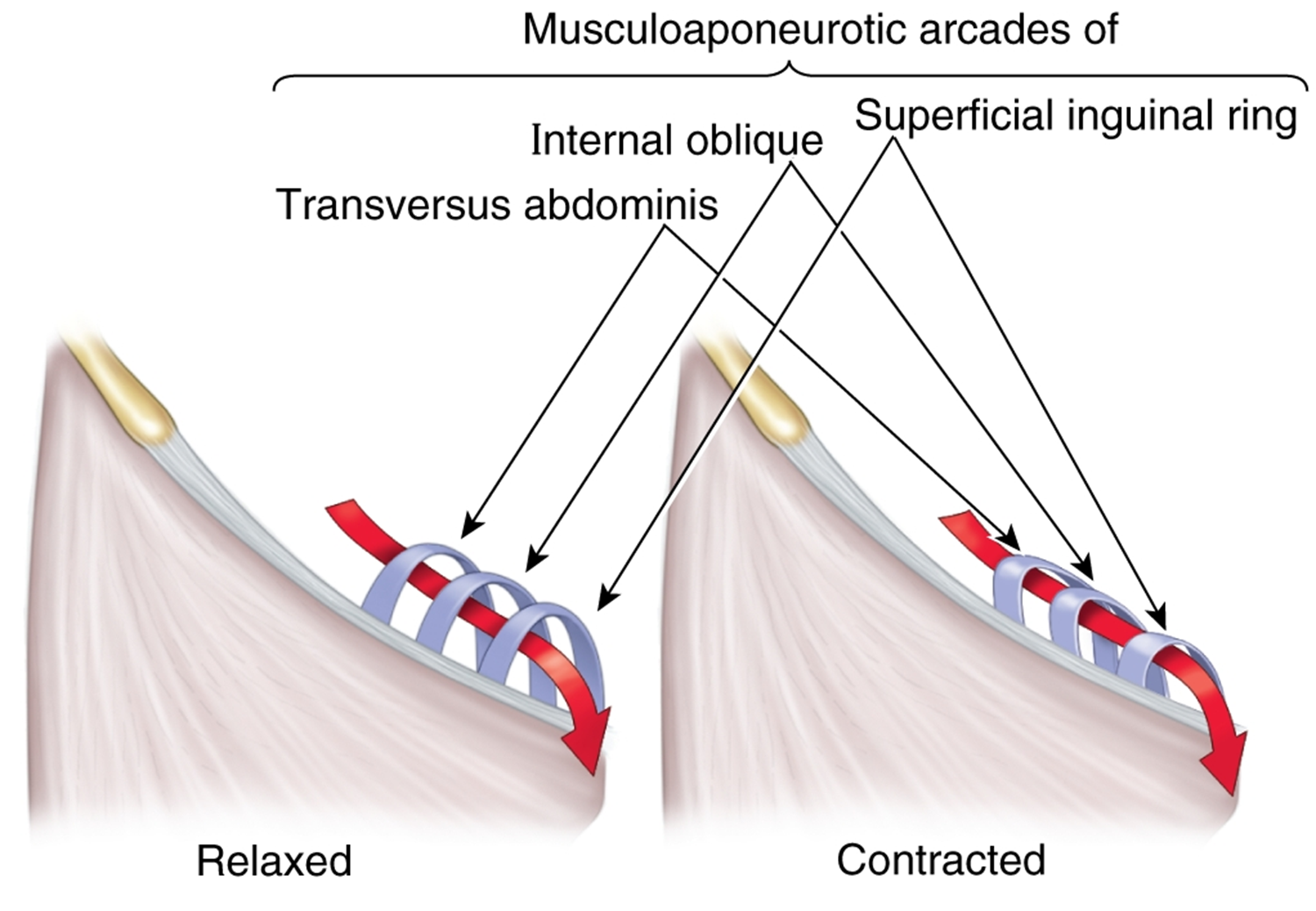
Roof
formed by the arching fibers of the transversus abdominis and internal oblique muscles on their way to form the conjoint tendon
Anterior wall
External oblique aponeurosis throughout the length of the canal and reinforced laterally by the internal oblique
Posterior wall
transversalis fascia which is reinforced medially by the conjoint tendon
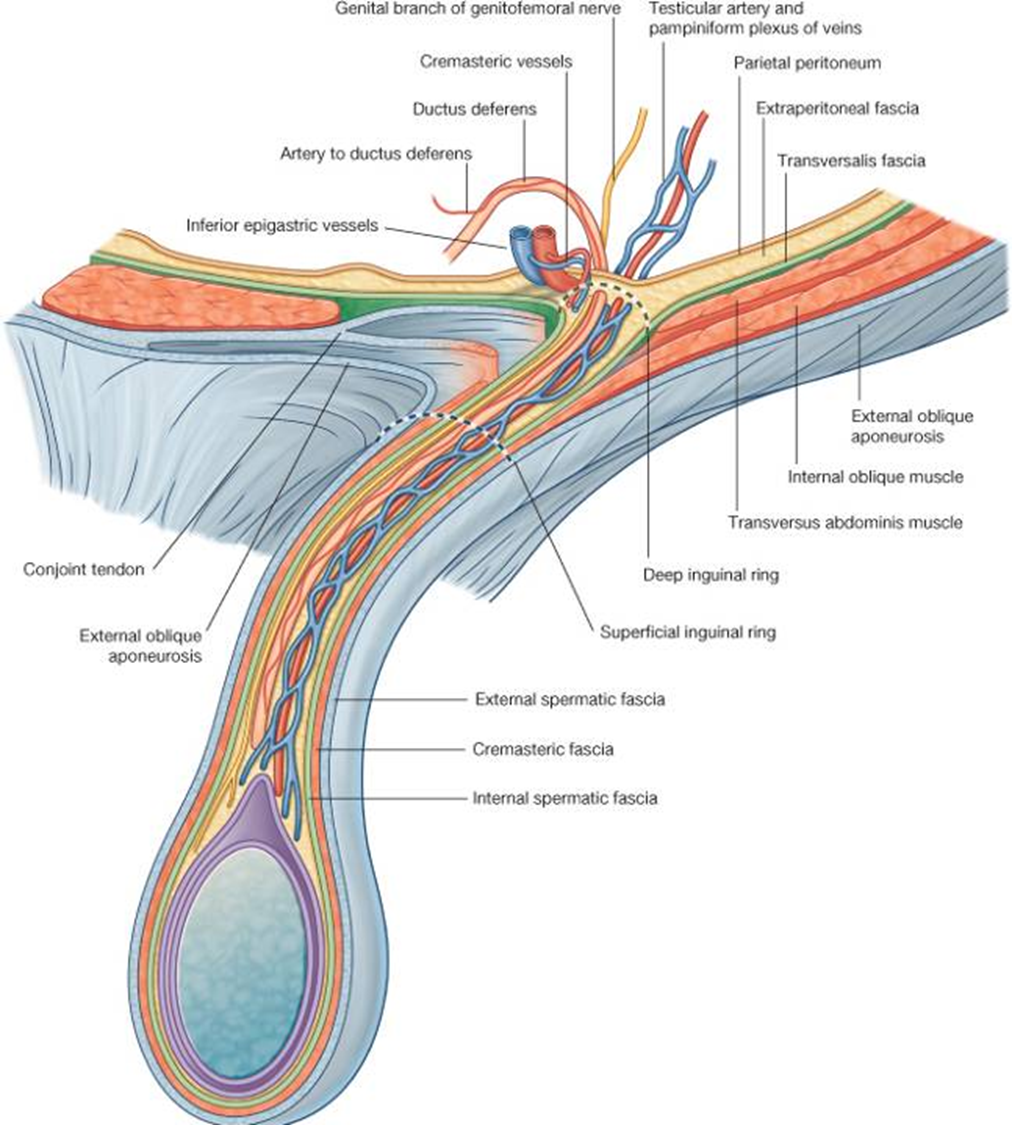
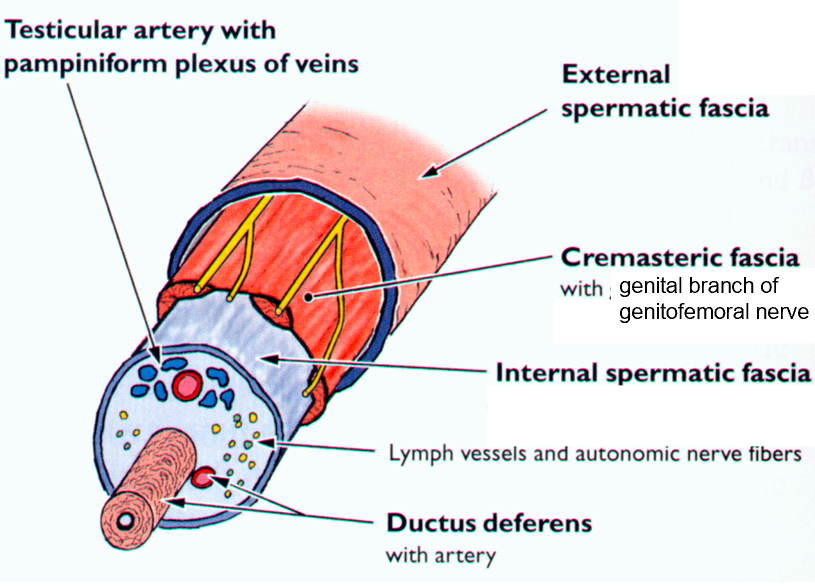
spermatic cord
Testis descends from upper lumbar region where it develops from intermediate mesoderm along with the kidney.
As the testis descends, posterior to the peritoneum, the spermatic cord forms.
spermatic cord takes on coverings or fasciae that are continuous with layers of the anterolateral abdominal wall.
As it passes through deep inguinal ring, it takes on the internal spermatic fascia, which is derived from the transversalis fascia.
As it passes beneath the conjoint tendon, it takes on a layer from the internal oblique, the cremasteric fascia, which contains skeletal muscle.
As it passes through the superficial ring, it takes on a layer from the aponeurosis of the external oblique muscle, the external spermatic fascia.
cremasteric reflex
Cremasteric fascia is the middle covering of the spermatic cord.
Derived from the internal oblique muscle.
Innervated by the genital branch of the genitofemoral nerve (L1/L2).
Stroke upper medial thigh, which is innervated the ilioinguinal nerve (L1) and a reflex arc causes the cremasteric muscle to contract.
More active in children.
Can be used to test integrity of L1 spinal level.
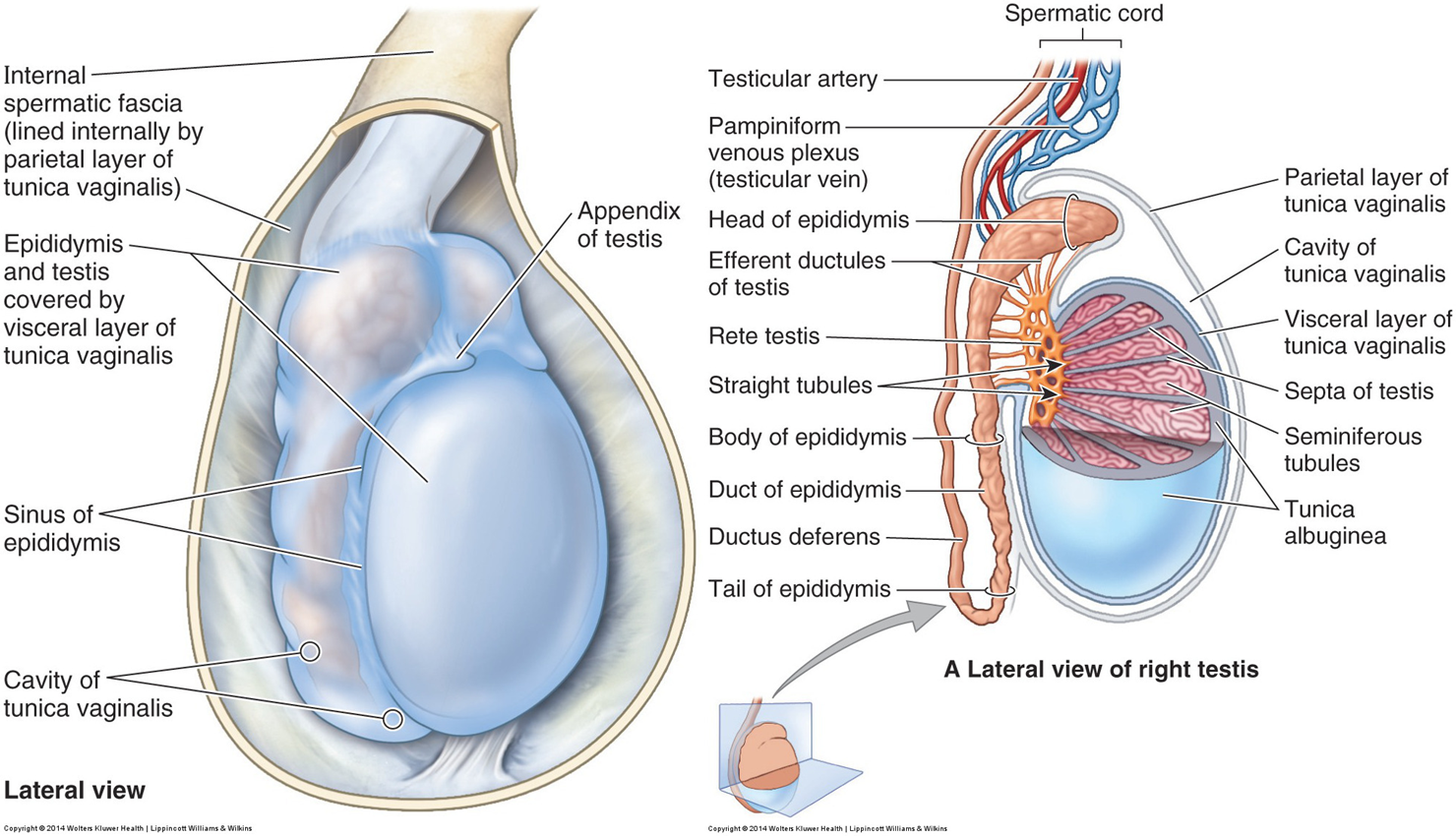
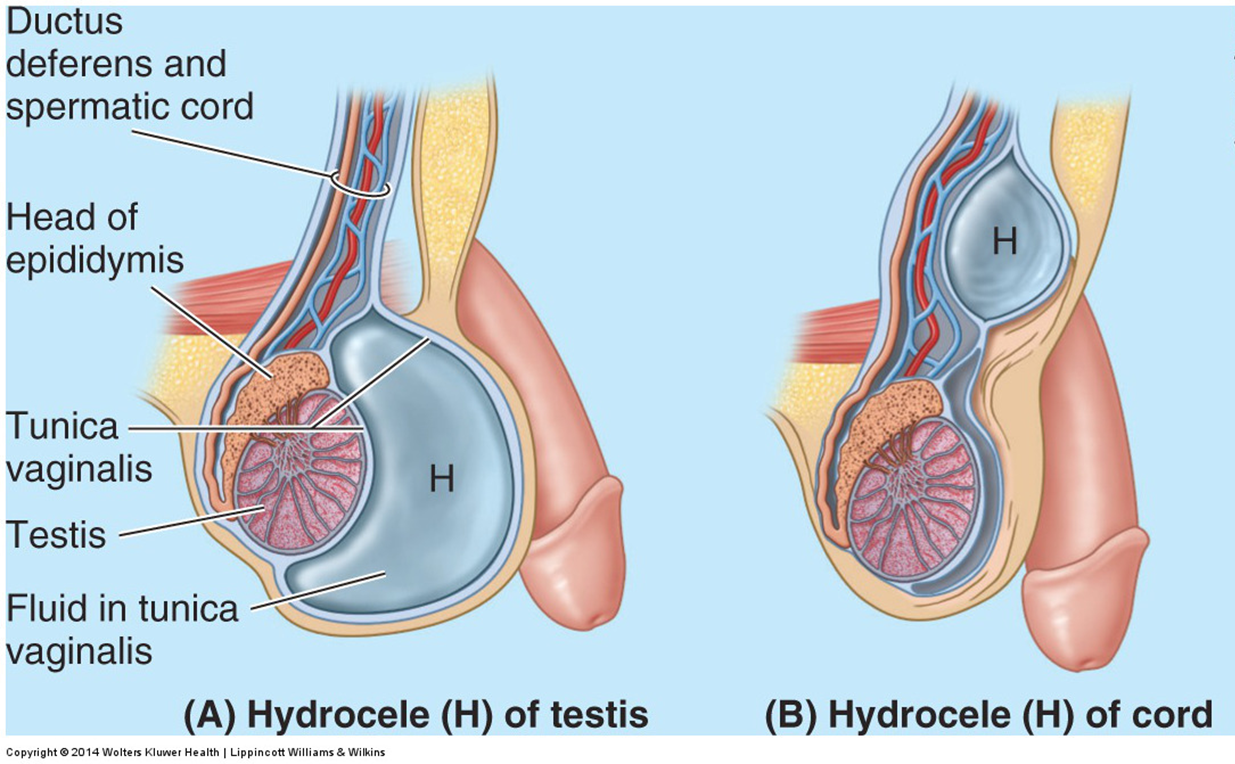
Note: The tunica vaginalis is a remnant of the processus vaginalis. It has a visceral layer, which covers the testis except where the testis is attached to the epididymis and spermatic cord. Parietal layer is adjacent to spermatic fascia.
innervation & lymphatics of genitalia
Testicular innervation is vagal para-sympathetics and visceral afferents and sympathetics from T10-T11 spinal cord segment.
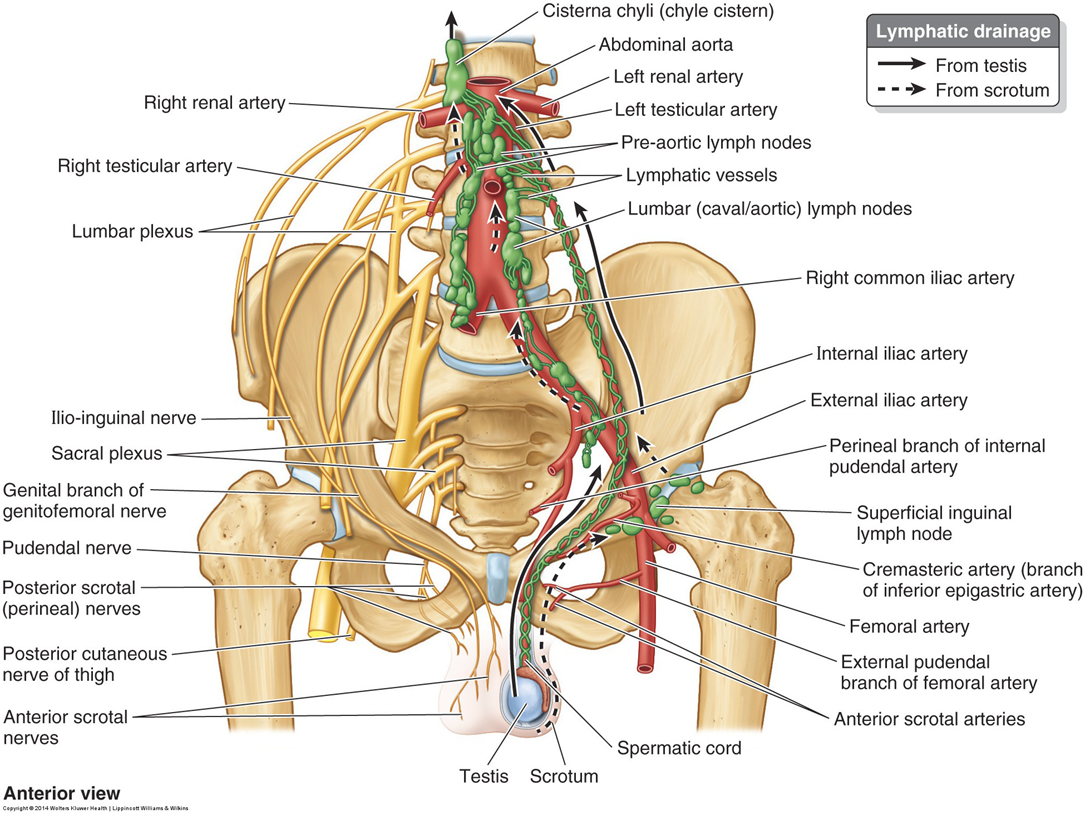
clinical note: testicular vs scrotal cancer
Testicular cancer travels to lumbar nodes.
Scrotal cancer travels to superficial inguinal nodes.
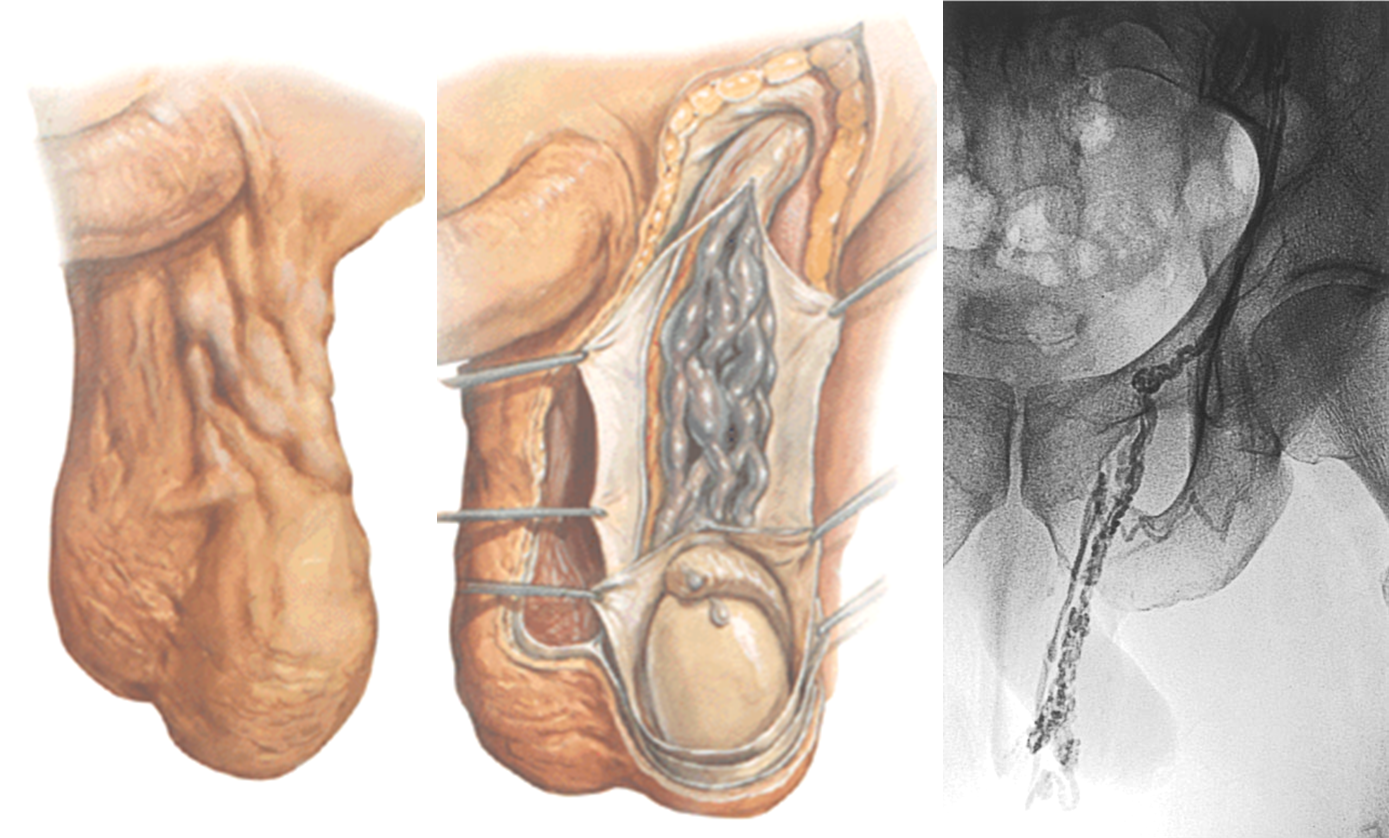
clinical note; hydrocele
clinical note: varicocele
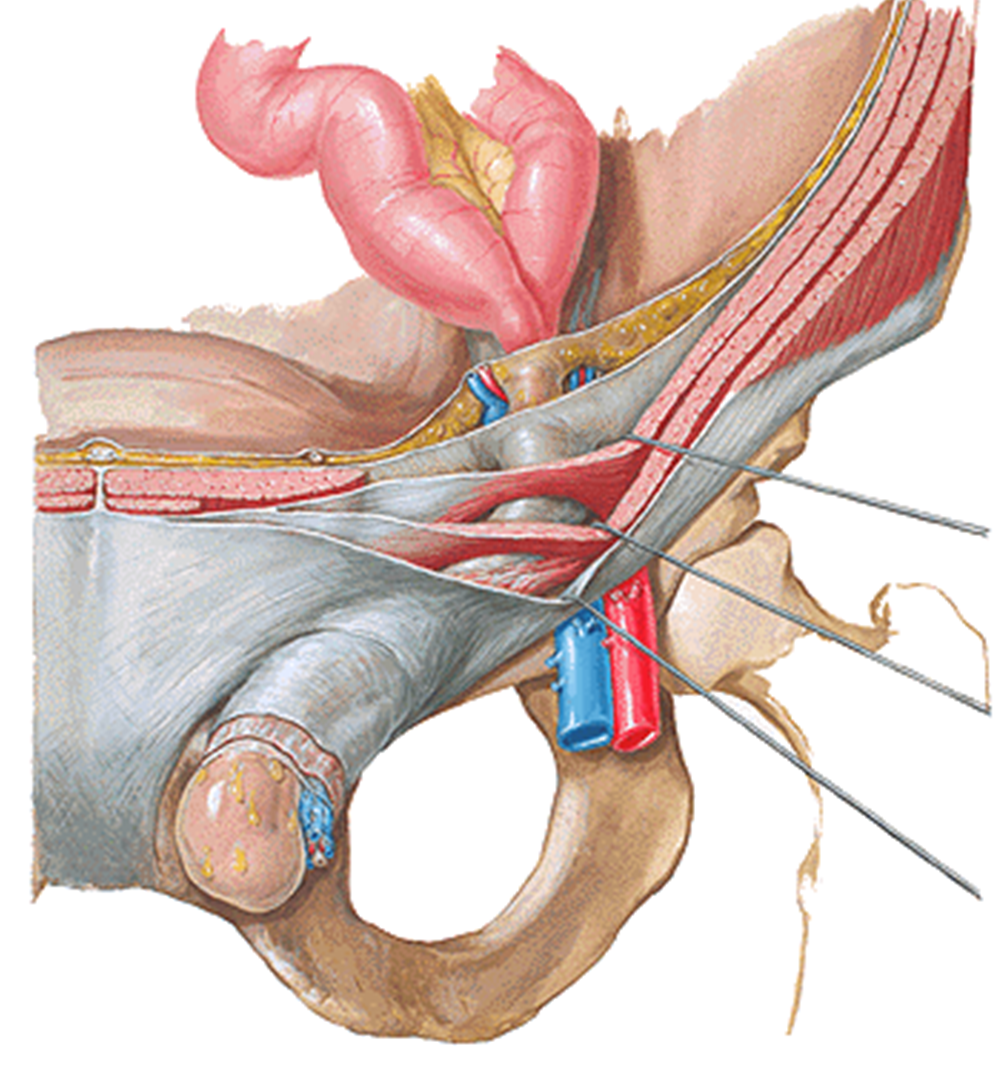
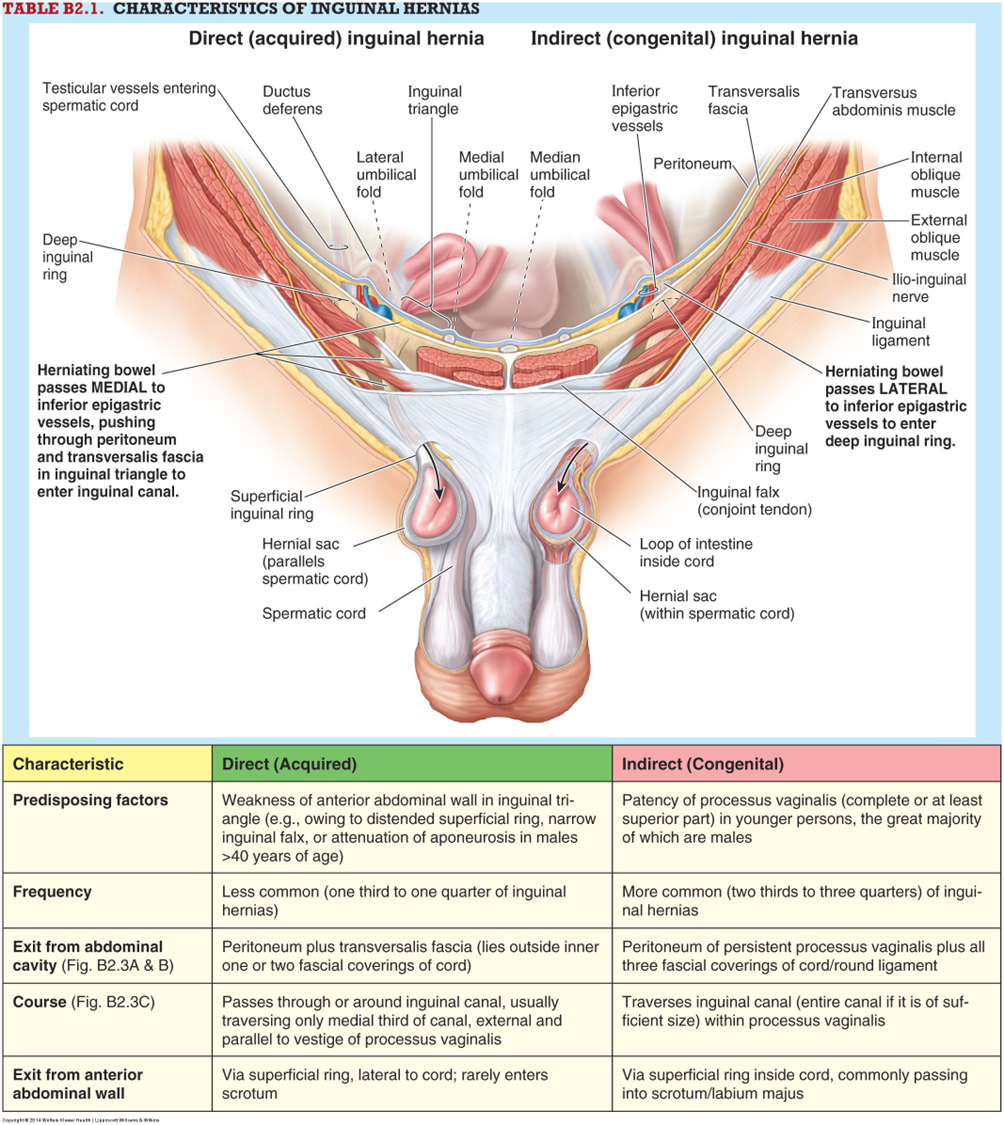
inguinal hernia
25% of males and 2% of females will have an inguinal hernia in their lifetime
Male:female ratio is 12:1
Two types of inguinal hernias
Direct (AKA acquired)
Usually occur in older patients
One-third of all inguinal hernias
Occurs medial to inferior epigastric vessels
Weak abdominal wall
Indirect
Most common
Two-thirds of all inguinal hernias
Right side predominance
Occurs lateral to inferior epigastric vessels
Congenital condition

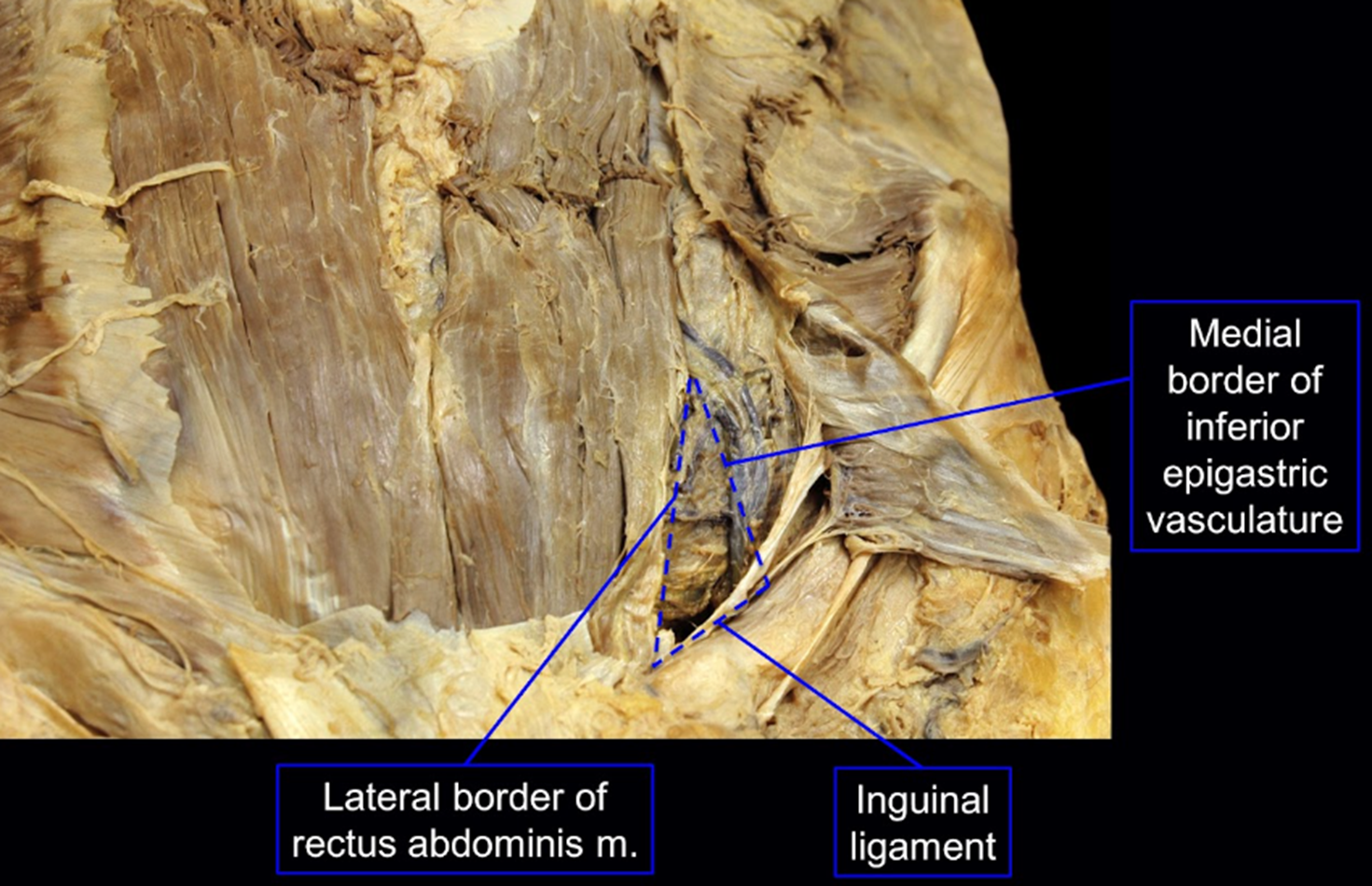
inguinal (hesselbach’s) triangle
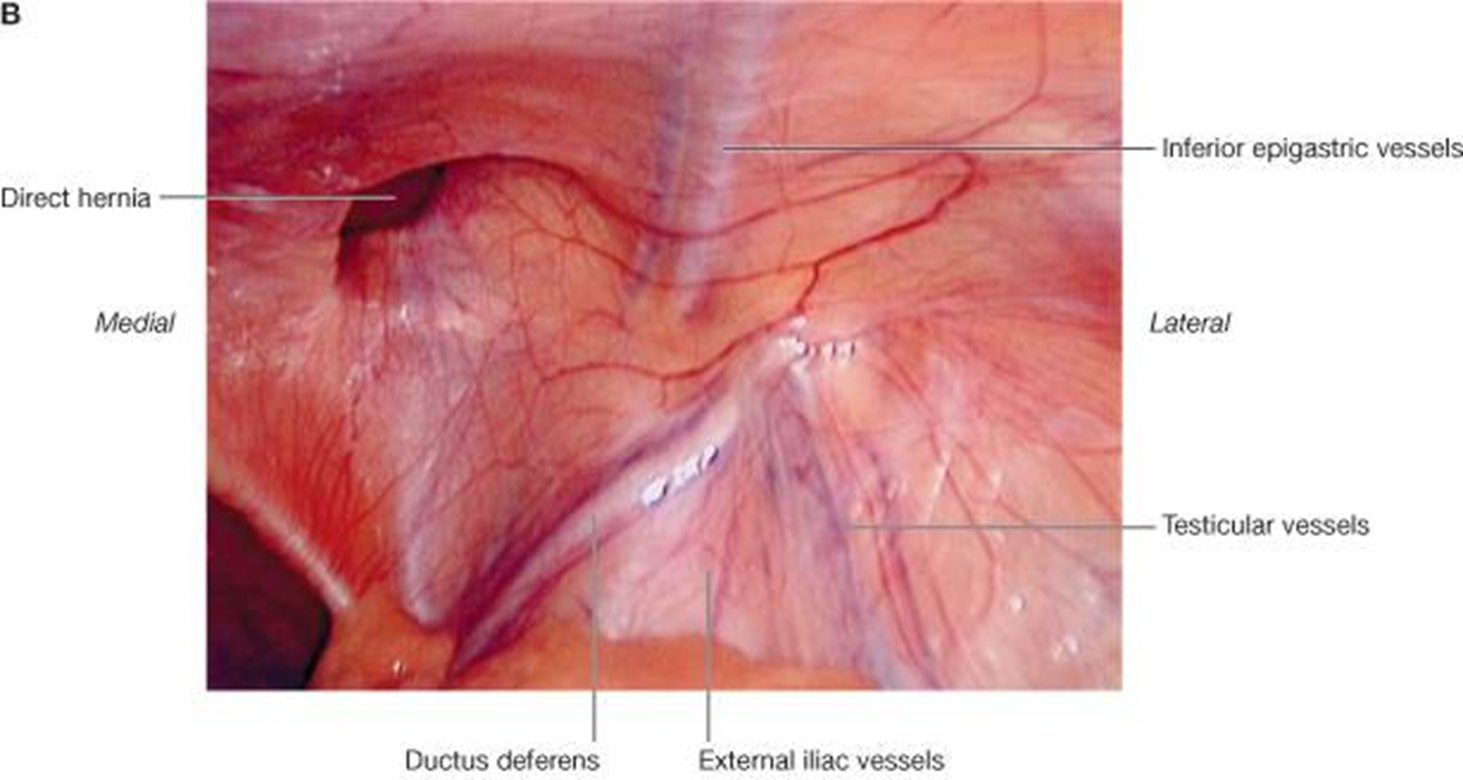
An indirect hernia has peritoneum and the coverings of the spermatic cord over it
While a direct hernia iscovered by peritoneum alone. This is because the viscera herniate along the path of testicular descent in the case of an indirect hernia.