abdominal viscera
key to understanding abdominal viscera
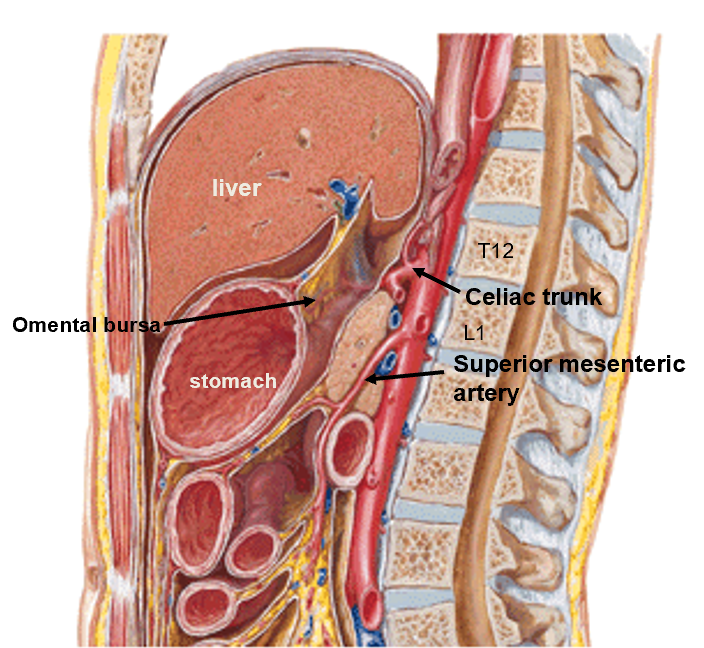
There are three unpaired arteries that arise from the abdominal aorta
These three arteries supply derivatives of the foregut, midgut, and hindgut
Celiac trunk – Foregut : Arises at the level of the T12/L1
Superior mesenteric - Midgut : Arises at the level of the lower border of L1
Inferior mesenteric – Hindgut: Arises at the level of L3
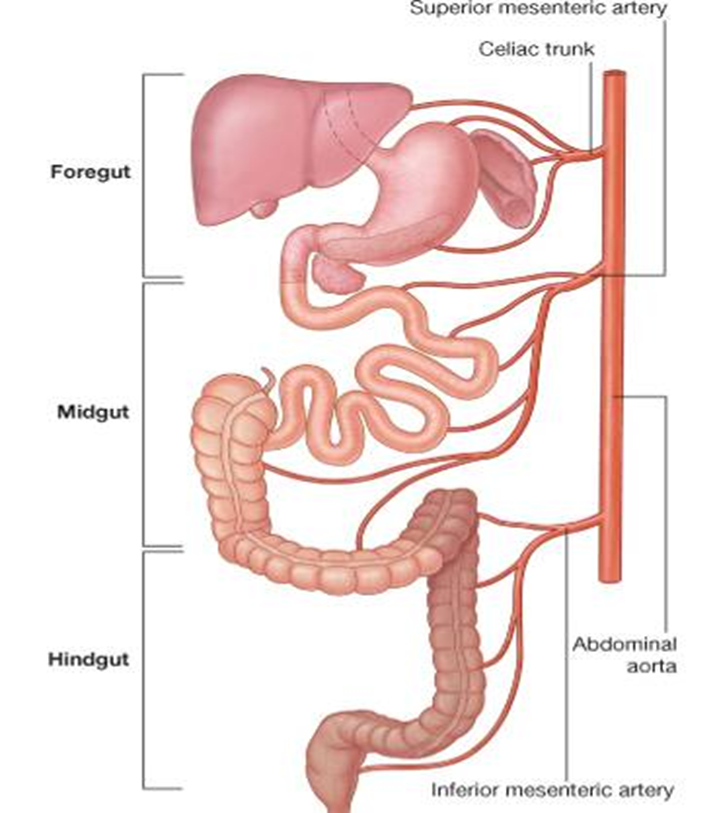
foregut derivatives are supplied by branches of celiac trunk
Lower esophagus
Stomach
Proximal duodenum
Pancreas
Liver
Gallbladder
esophagus
25 cm long muscular tube
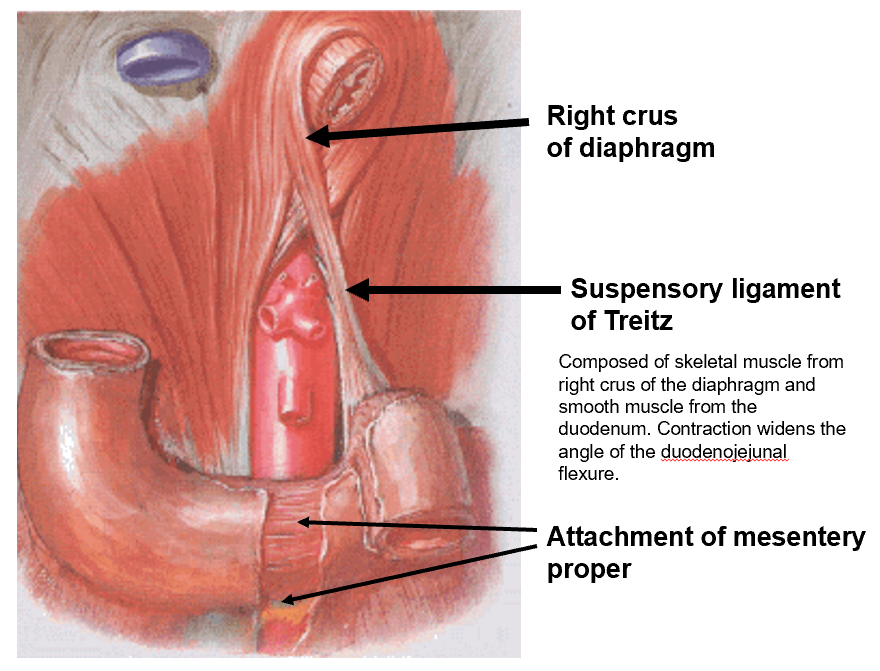
Passes through the diaphragm at level of T10 vertebra
Esophageal hiatus is within the right crus of the diaphragm
Terminates at cardiac orifice at level of T11
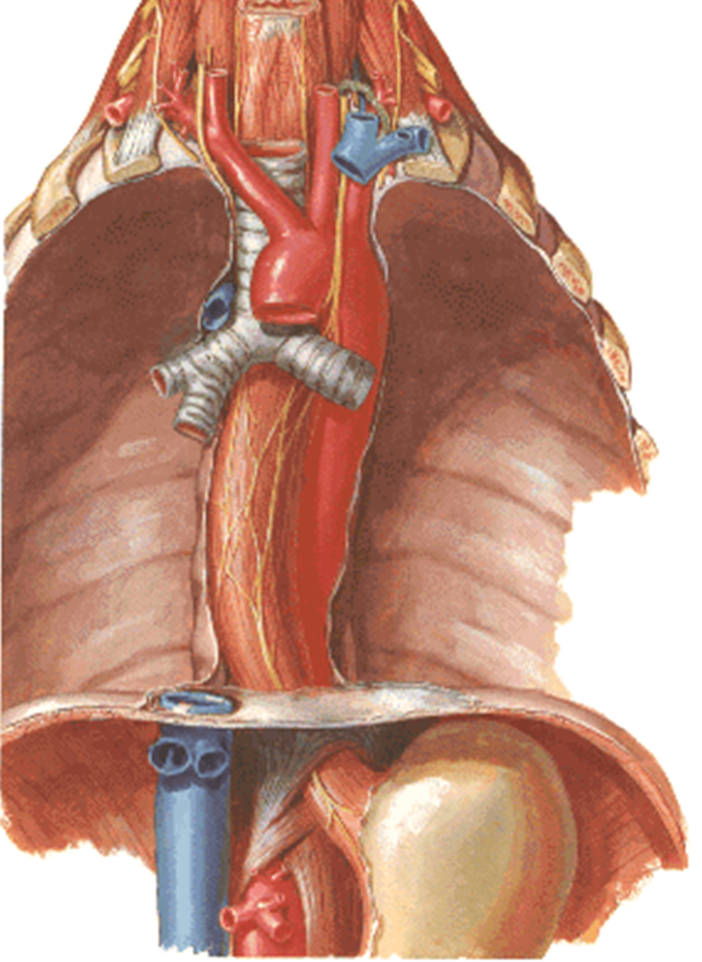
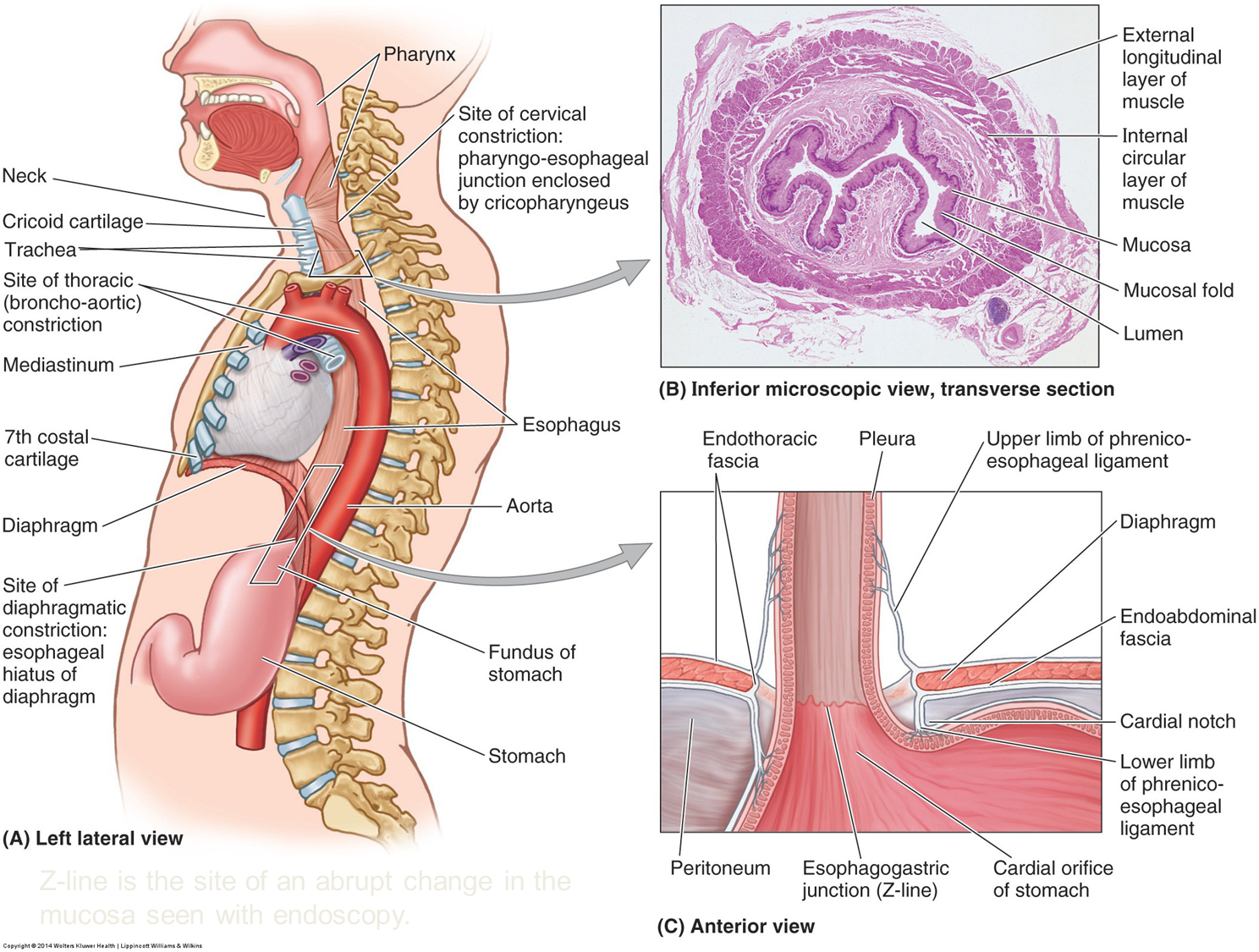
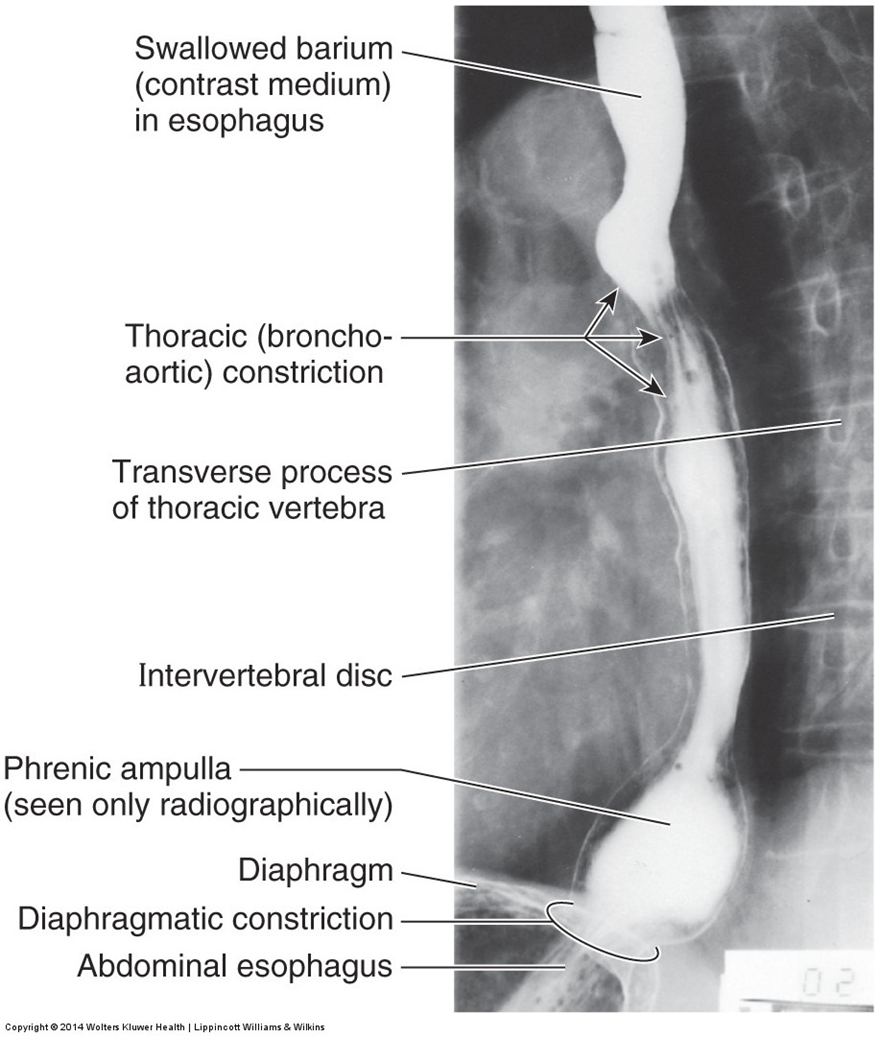
normal (anatomic) constrictions of esophagus
Three constrictions:
Cervical caused by the cricopharyngeus muscle. (not shown)
Broncho-aortic is a compound constriction caused by the aorta and then, left main bronchus.
Diaphragmatic at the esophageal hiatus.
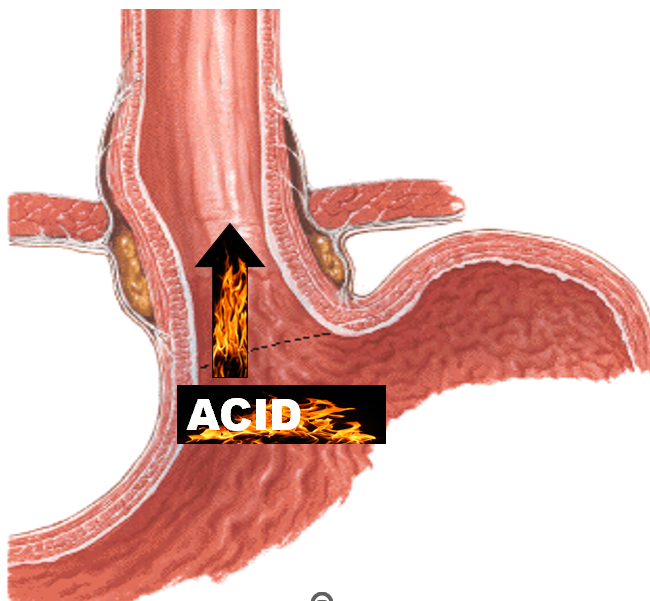
clinical note: pyrosis & GERD
GERD
Gastroesophageal reflux disorder is when an incompetent esophageal valve allows acid to rise into the esophagus causing pyrosis (heartburn).
In chronic cases, the lining of the esophagus can change or worse, become eroded.
clinical note: barret esophagus
Barrett esophagus is a metaplastic change of the esophageal epithelium from stratified squamous to simple columnar epithelium, like that of the intestines, secondary to gastroesophageal reflux.
The majority of people with Barrett esophagus are smokers and drinkers.
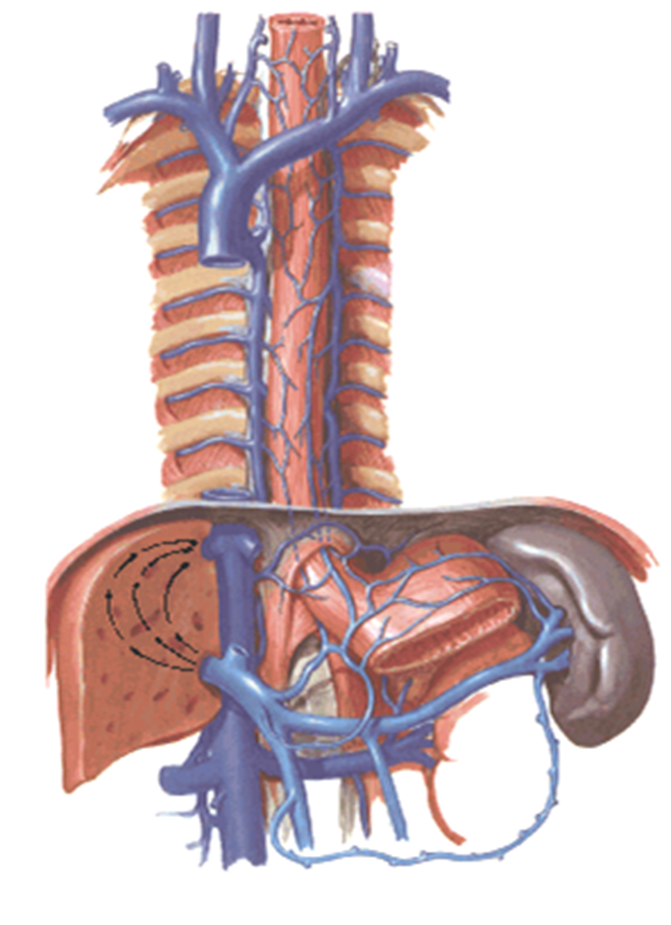
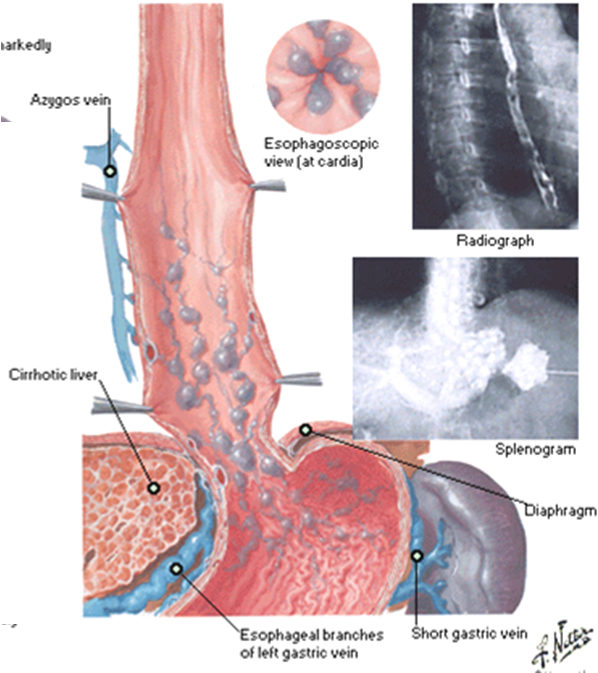
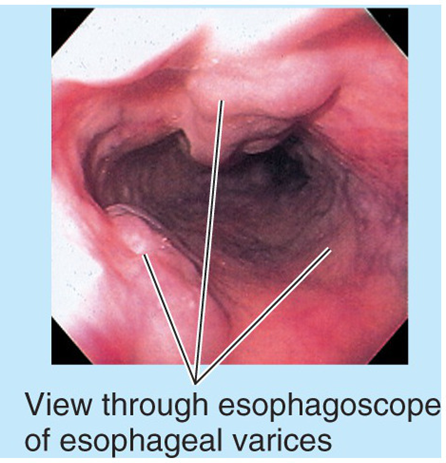
clinical note: esophageal varices
The esophageal veins are a site where the caval venous
drainage anastomoses with the portal venous drainage.
Portal hypertension cause dilation of the esophageal veins. These
dilated and weakened varices are prone to hemorrhage and is a
common cause of death in persons with portal hypertension.
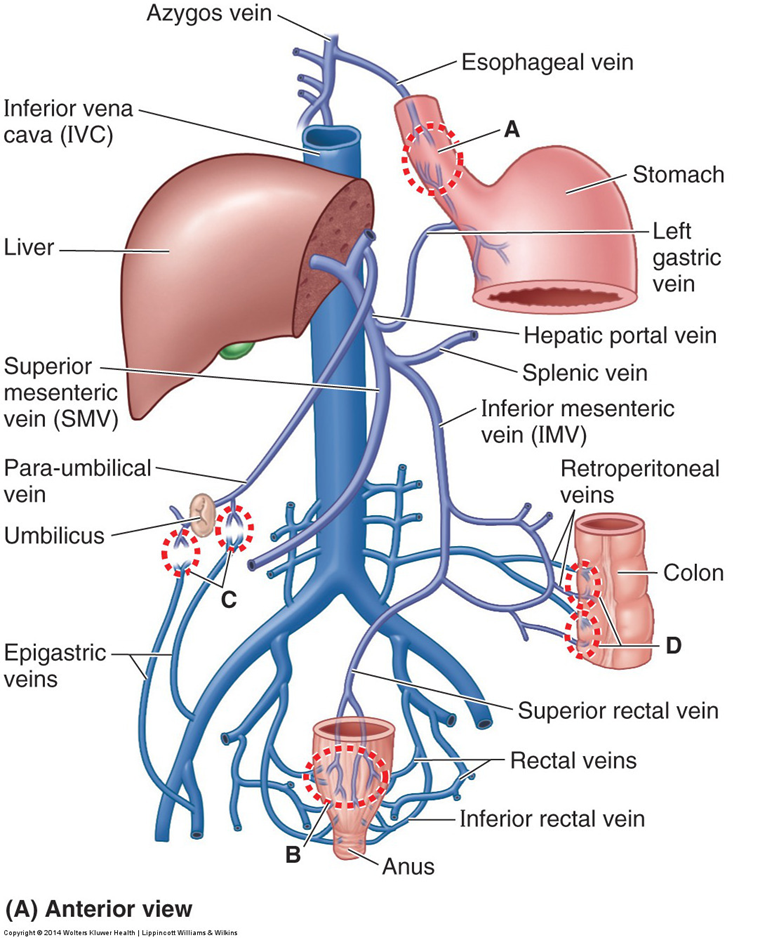
The esophageal veins are a site where the caval venous drainage, azygos vein, anastomoses with the portal venous drainage, left gastric vein.
Portal hypertension cause dilation of the esophageal veins. These dilated and weakened varices are prone to hemorrhage and are a common cause of death in persons with portal hypertension.
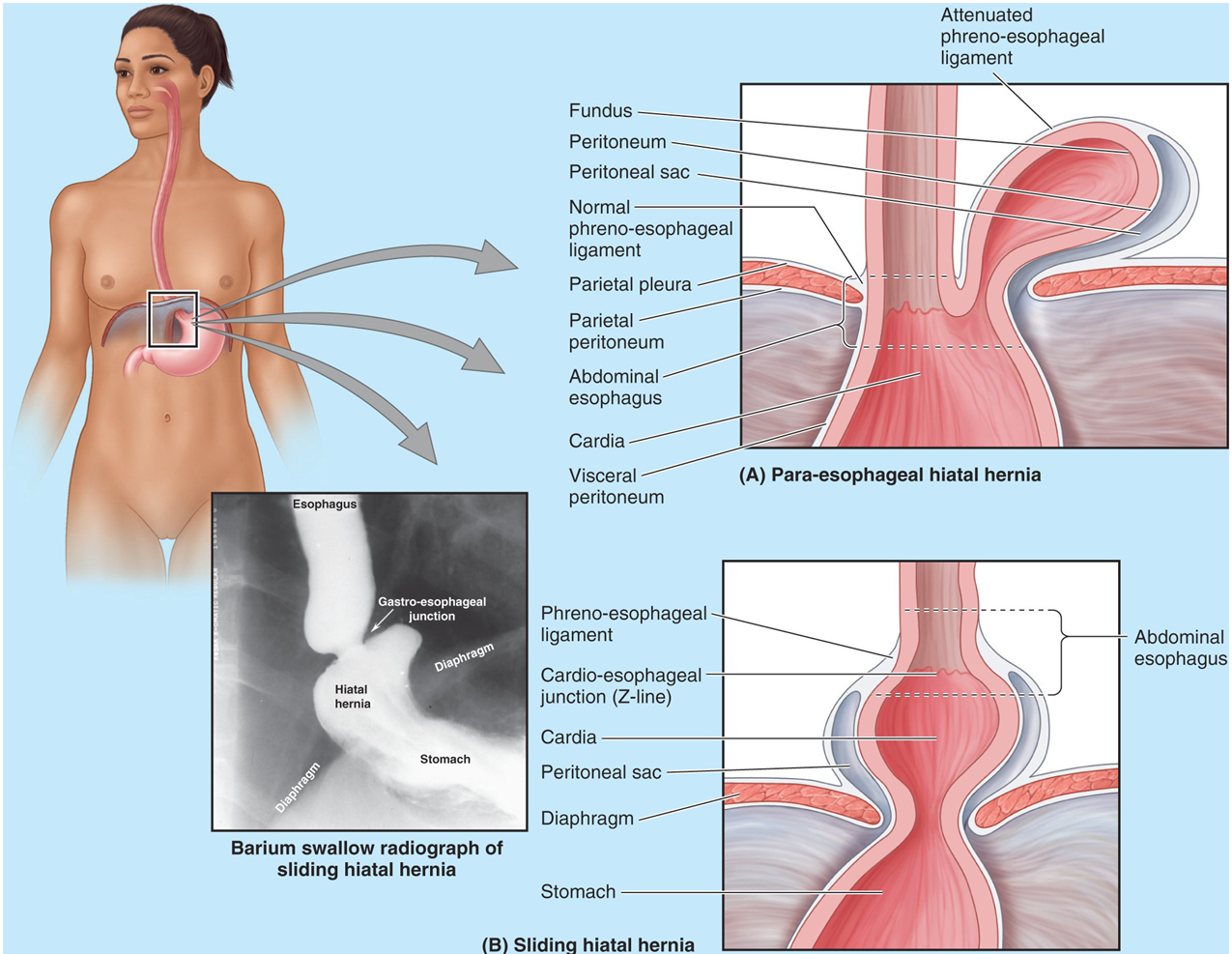
clinical note: hiatal hernia
more common in women over 50.
may mimic heart pain
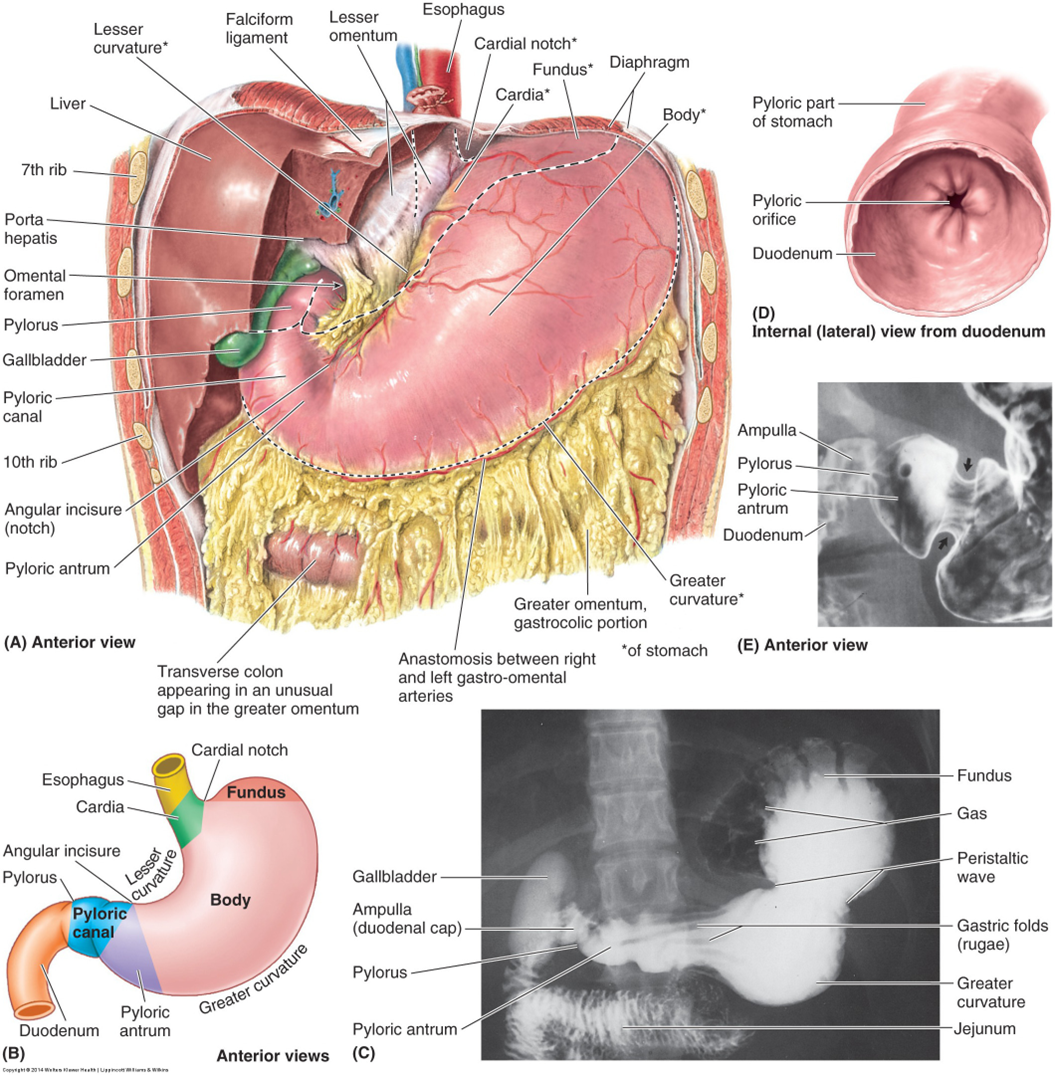
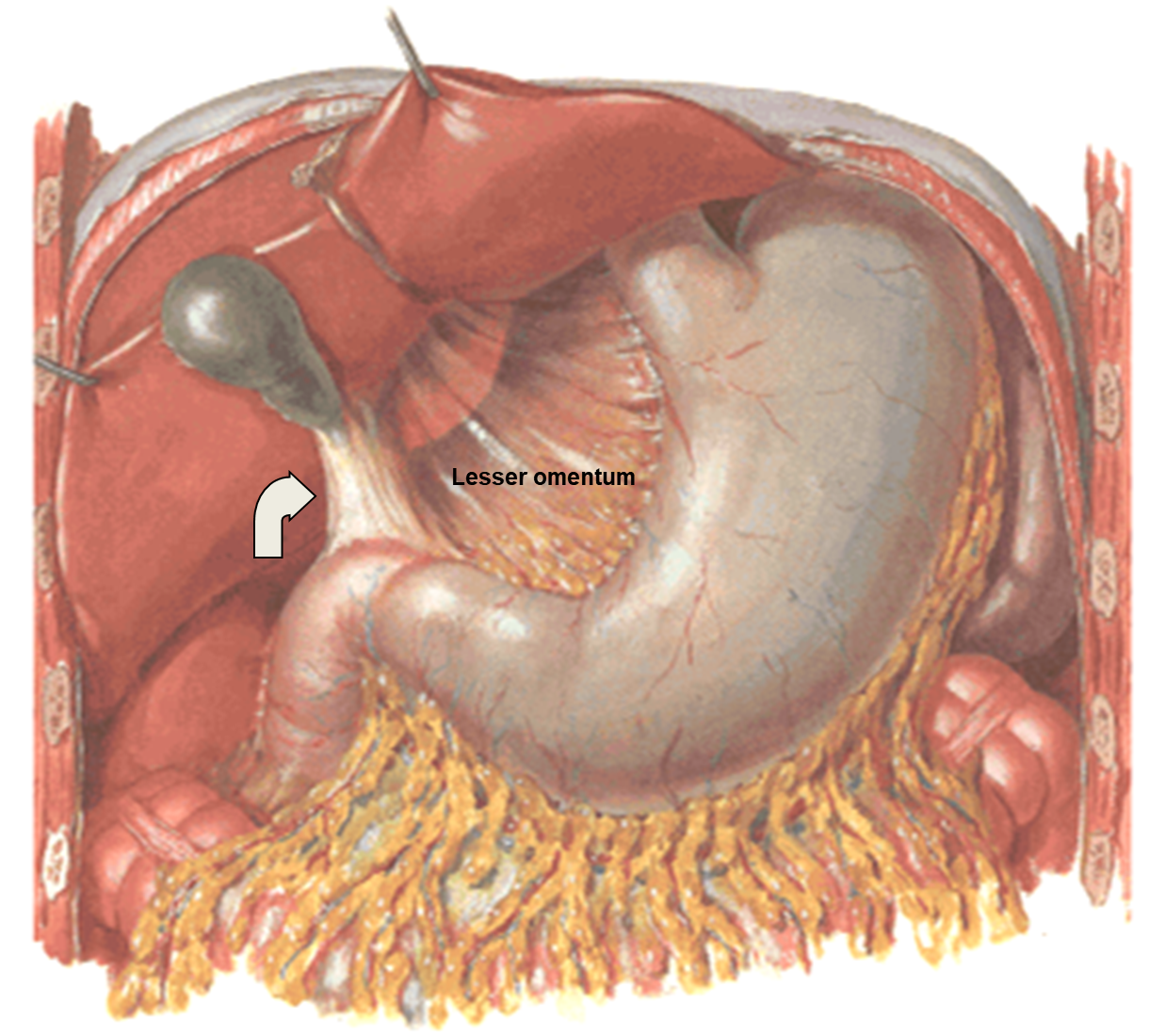
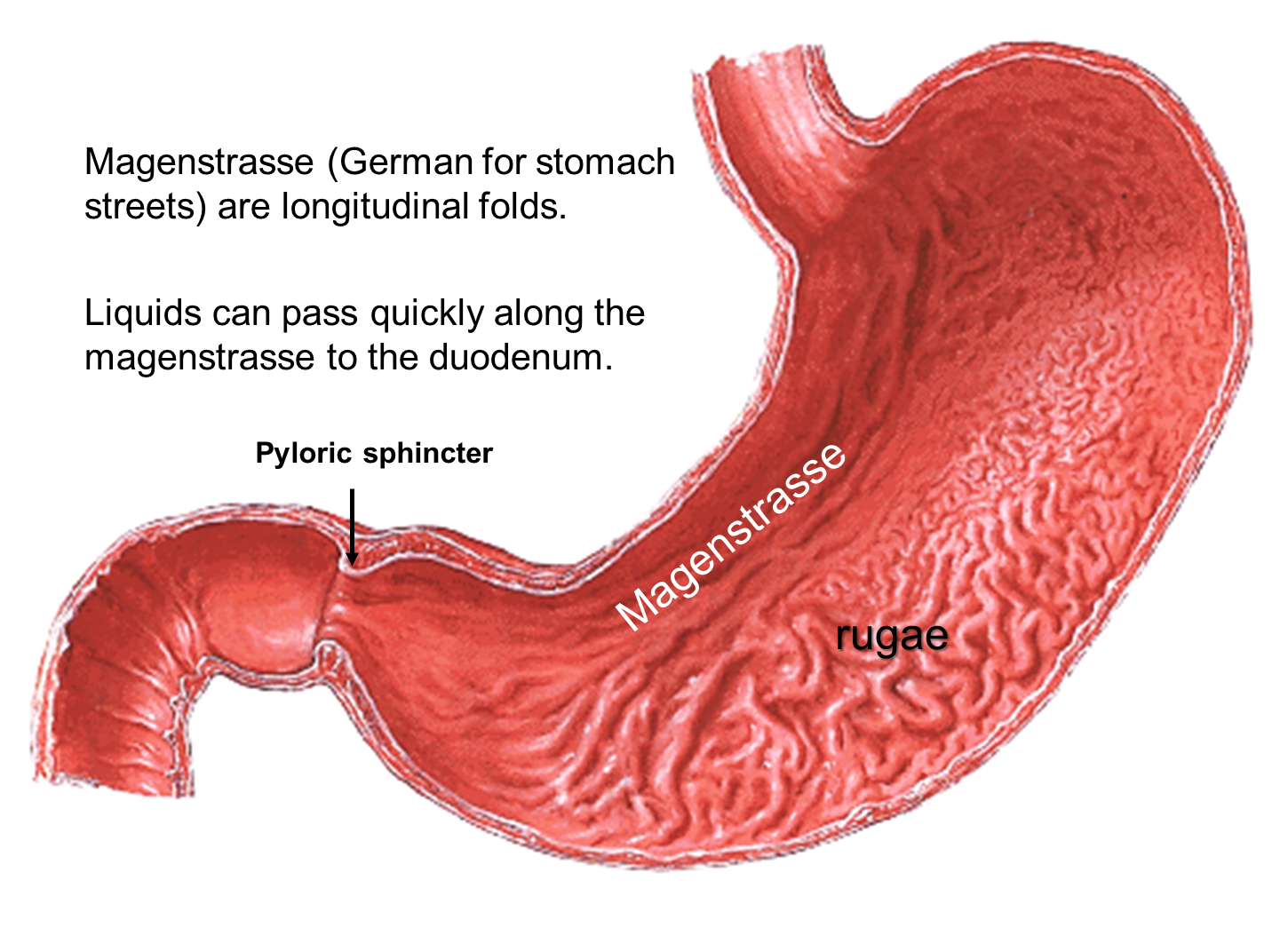
stomach
duodenum
Name duodenum derived from Latin, duodenum digitorum, meaning 12 finger breadths.
About 20-25cm long.
Mostly, secondarily retroperitoneal.
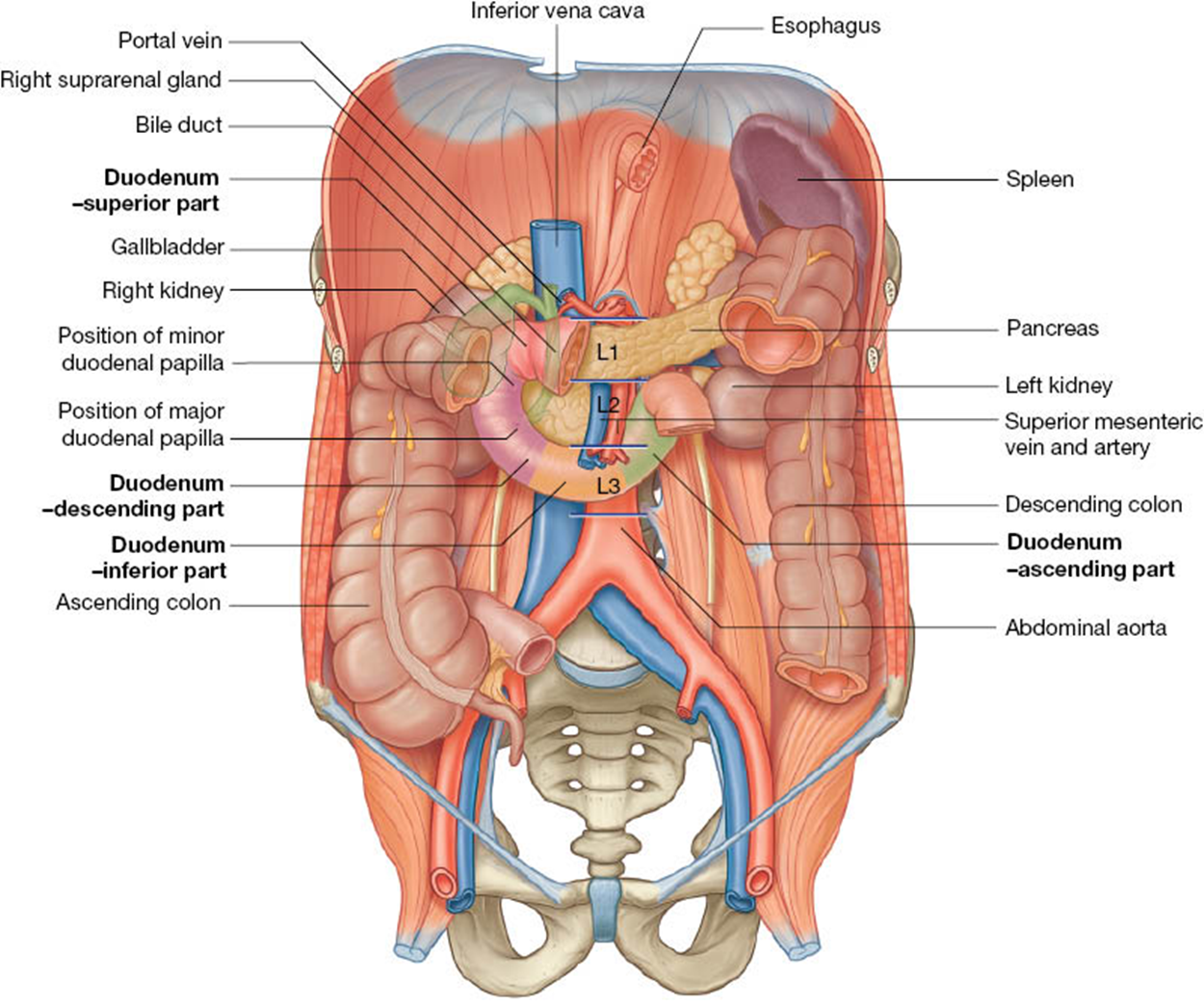
Has 4 parts:
From pylorus of stomach to neck of gallbladder at the level of the L1 vertebra.
Duodenal cap or ampulla is the site of duodenal ulcers.
Descending part, passes from the neck of the gallbladder inferiorly to the level of L3.
Lies over the hilum of the right kidney.
Crosses the IVC, aorta and the vertebral column.
The SMA, which arise at L1, and SMV pass anteriorly over the 3rd part.
Ascending part passes superiorly up to the level of L2 and joins the jejumum.
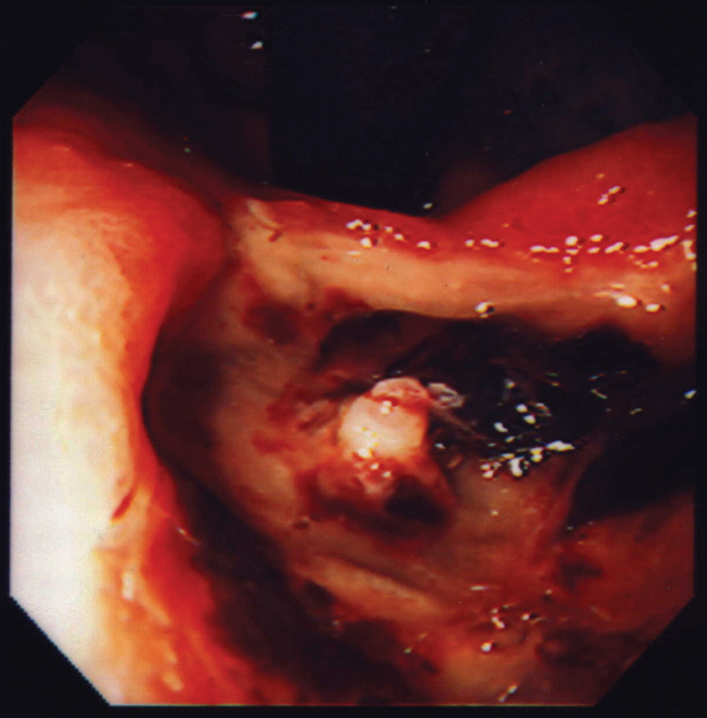
clinical note: duodenal ulcers
Usually occur in the superior part of the duodenum.
65% occur within the posterior wall within 3cm of the pylorus.
Most patients have impaired duodenal bicarbonate secretion.
Believed related to H pylori.
Posteriorly eroding ulcers can affect the gastroduodenal artery causing severe hemorrhage into the peritoneal cavity.
Image shows endoscopy of posterior erosion with an exposed branch of gastroduodenal artery.
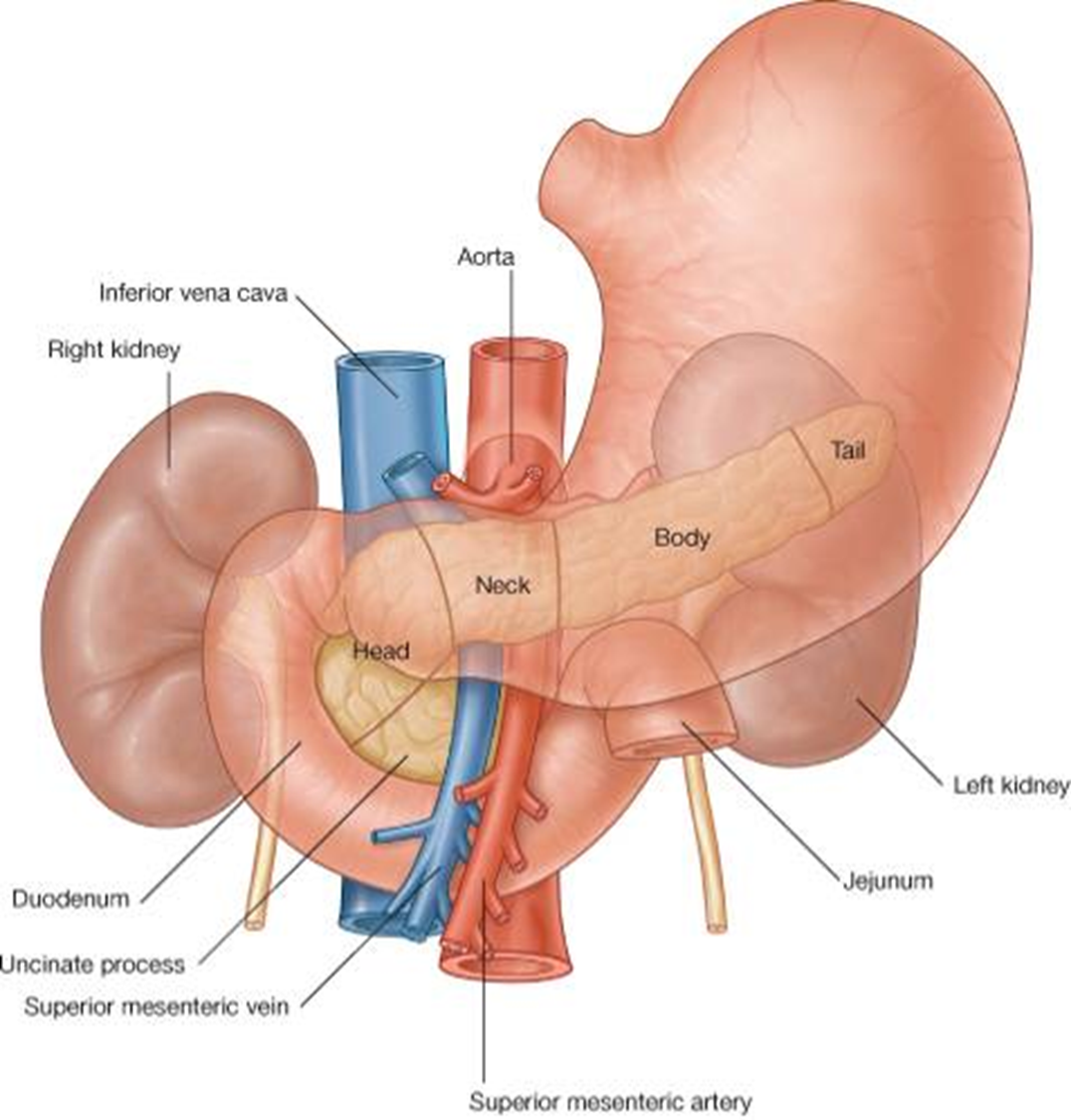
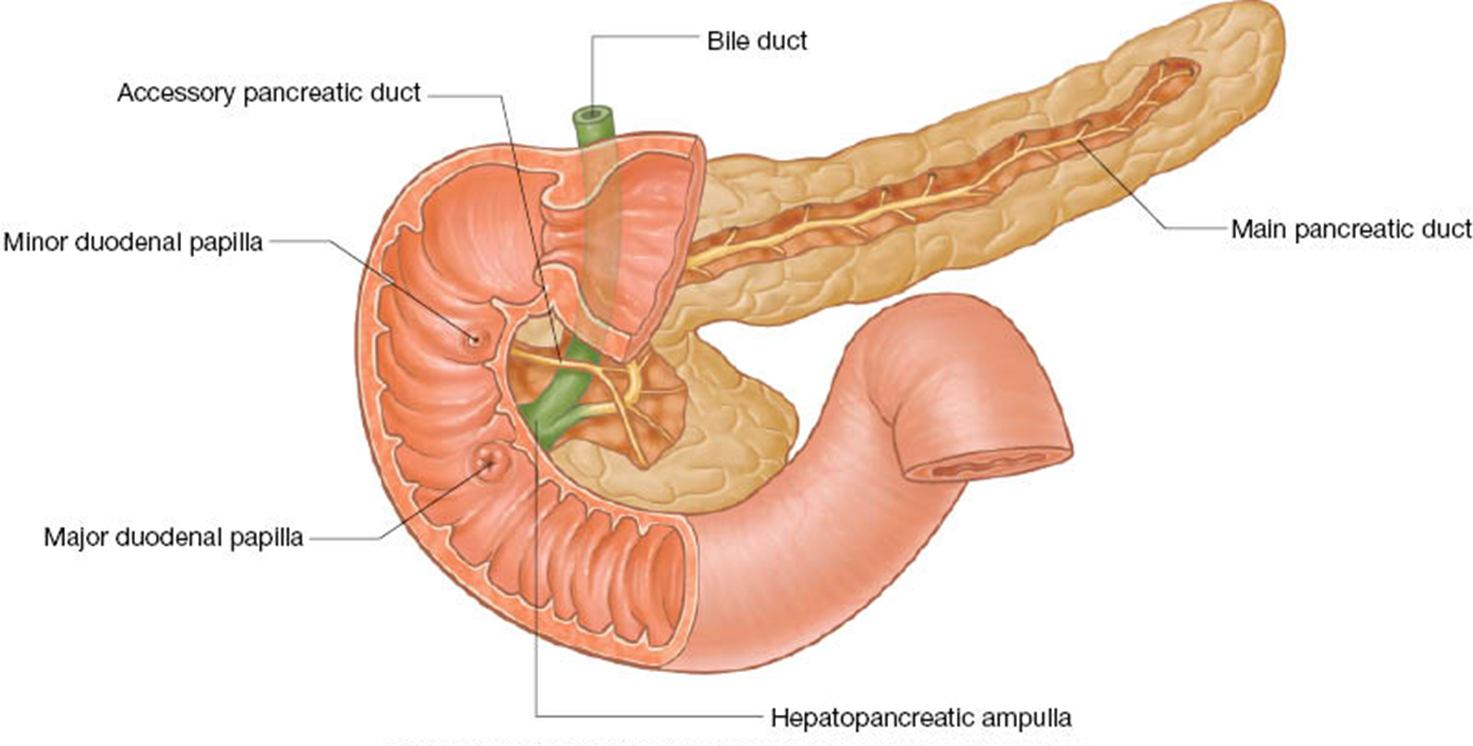
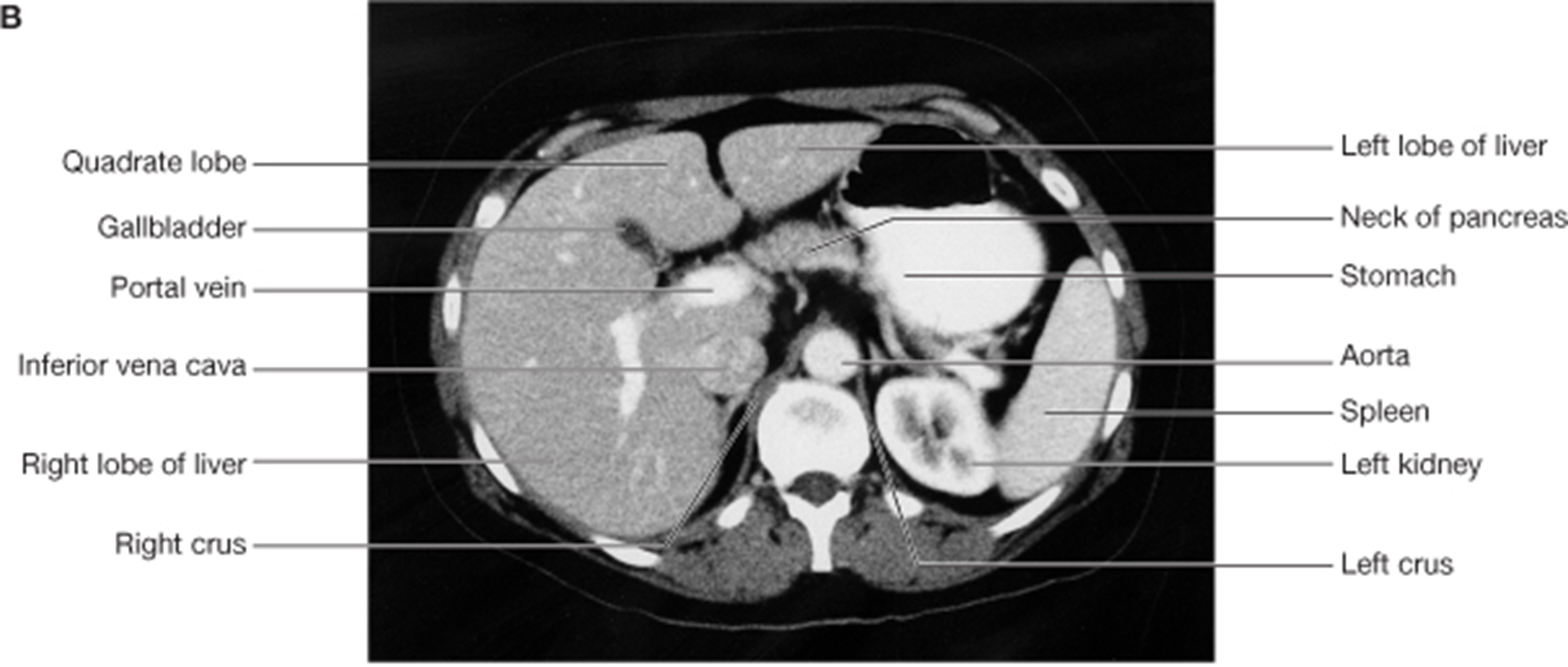
pancreas
mostly posterior to the stomach in the posterior wall of the omental bursa.
Head is cradled by the C-shaped duodenum.
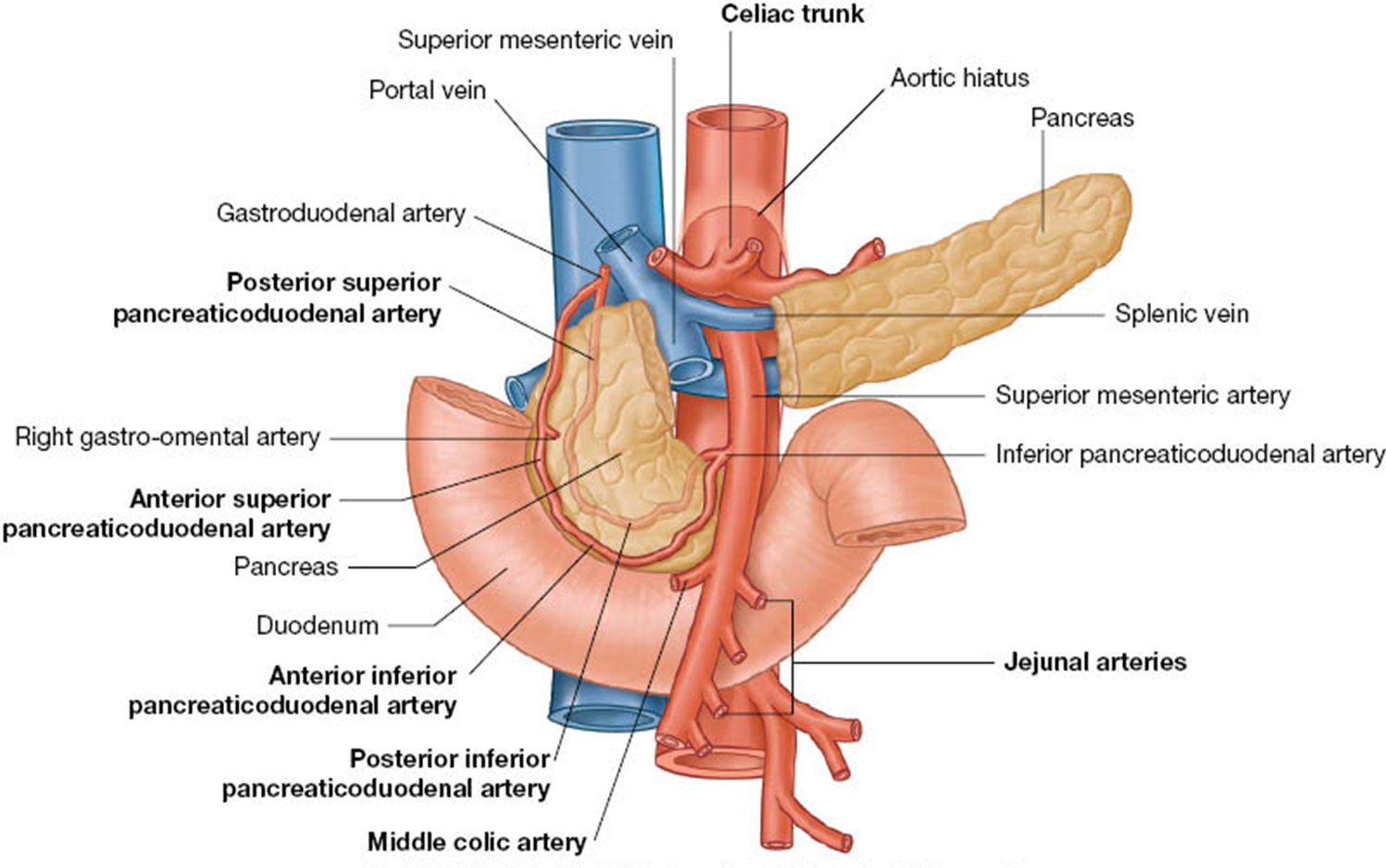
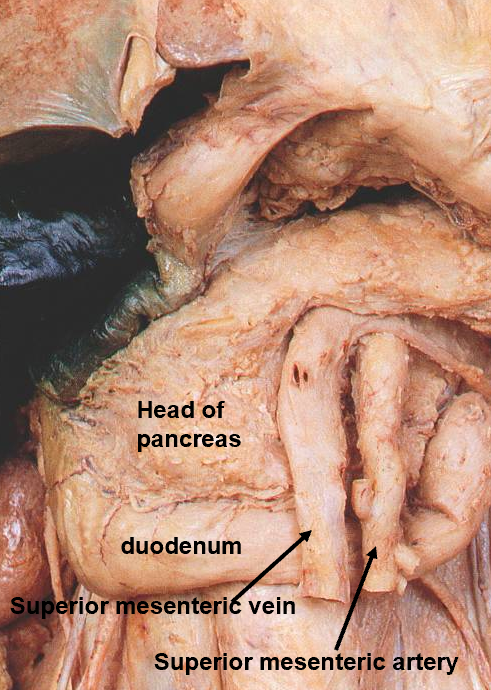
Neck lies anterior to the SMV and SMA.
Body is elongated.
Tail passes between the layer of the lienorenal (splenorenal) ligament to the hilum of spleen.
Uncinate process lies posterior to SMV and SMA.
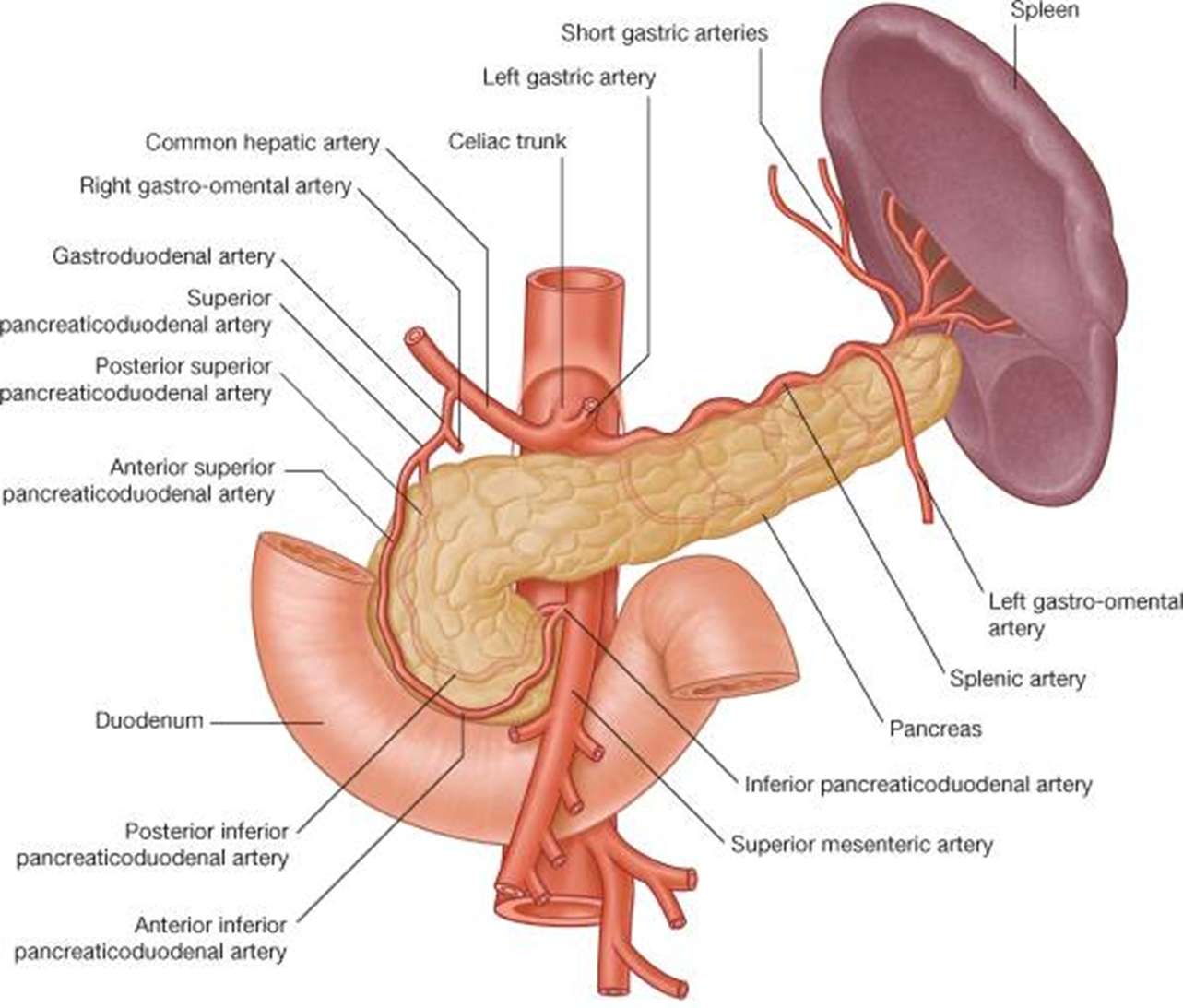
blood supply to pancreas
Note anterior and posterior pancreaticoduodenal arcades. These vessels provide anastomoses between the celiac trunk via the gastroduodenal artery and the SMA.
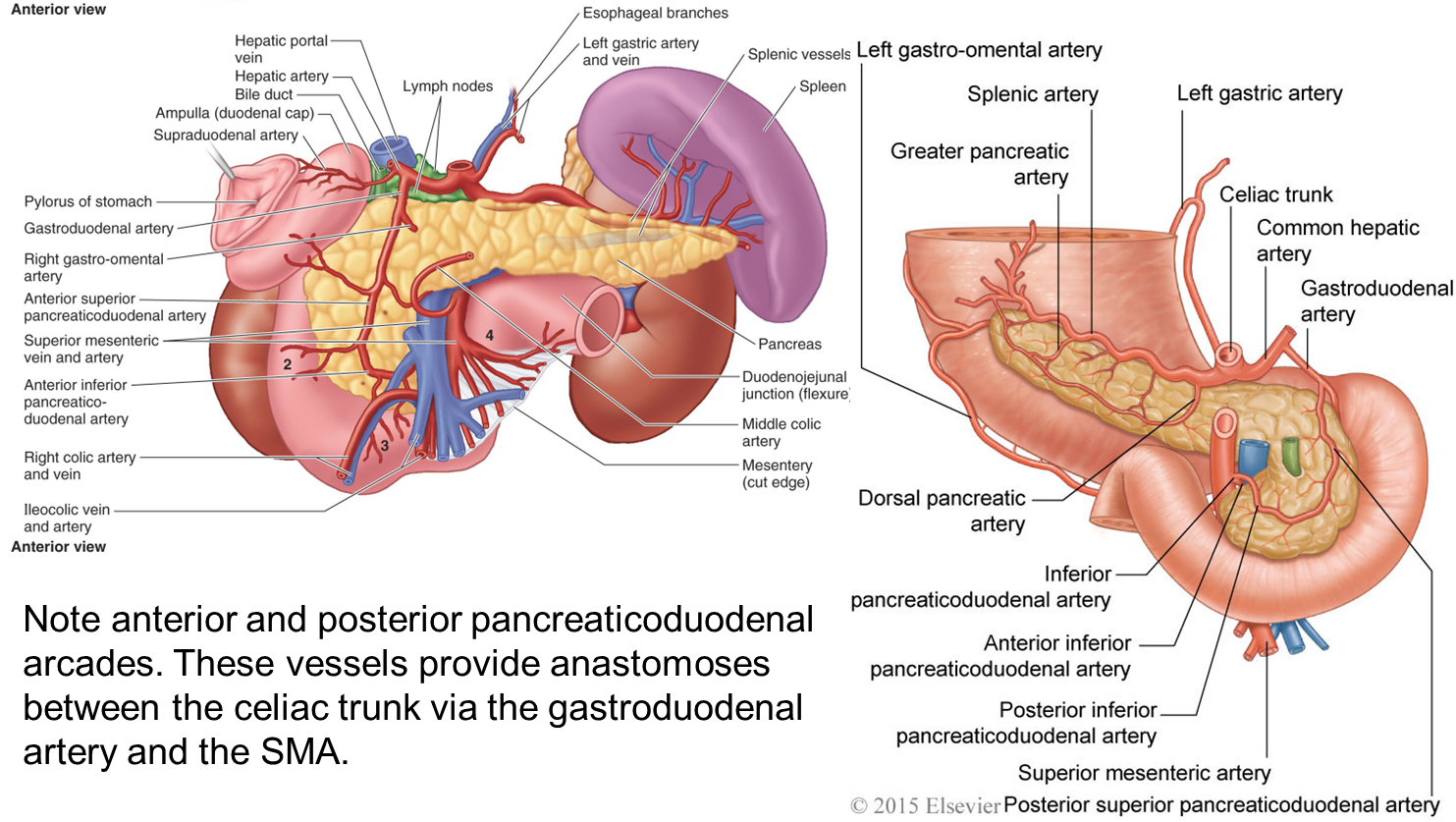
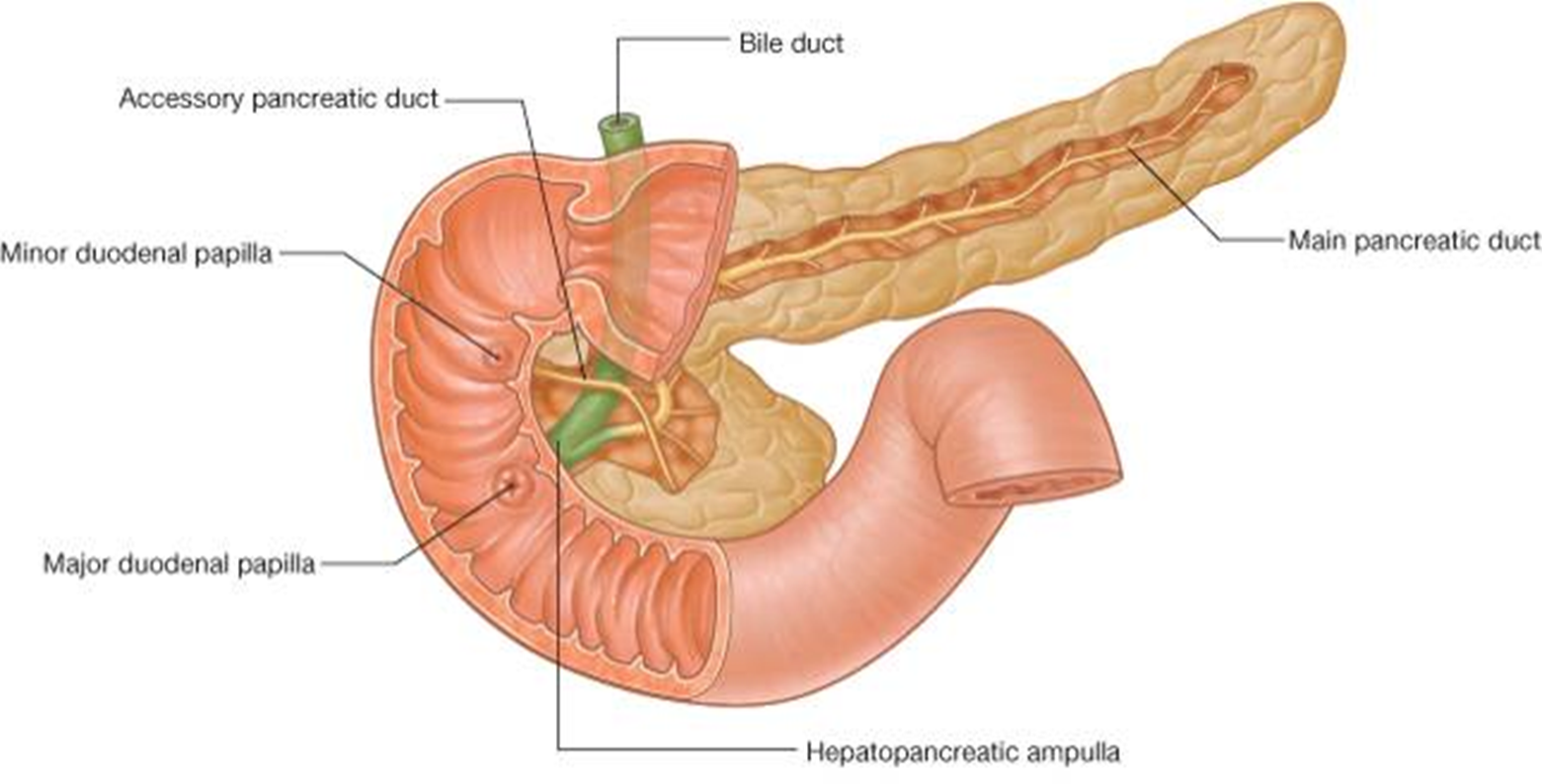
The major duodenal papilla marks the junction between foregut and midgut derived structures.
clinical note: Obstructive Jaundice Due to Pancreatic Carcinoma
Jaundice results from retention of bile.
Bile pigments stain tissues such as the sclera (whites) of the eyes (icterus)
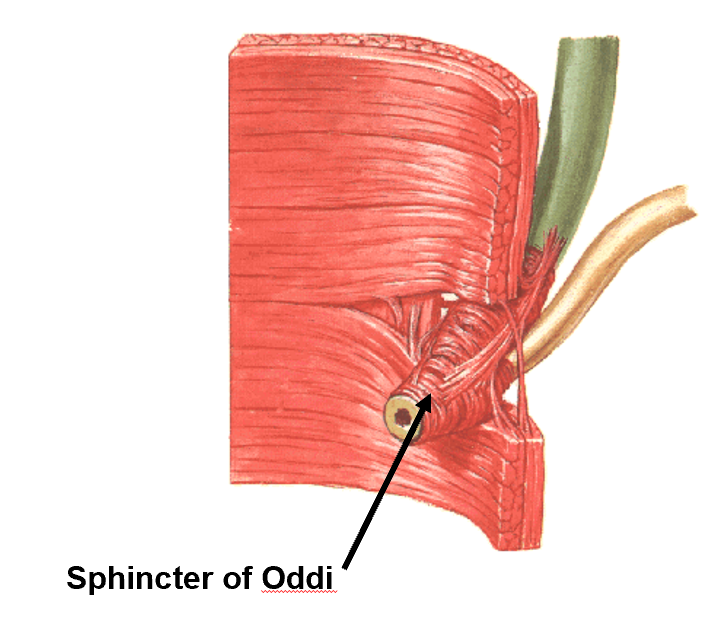
Cancer of the head of the pancreas can often compress the bile duct or the hepatopancreatic ampulla (ampulla of Vater).
Associated with severe back pain.
Large gallstone can also cause obstructive jaundice and so one must consider this as a possibility in the differential.
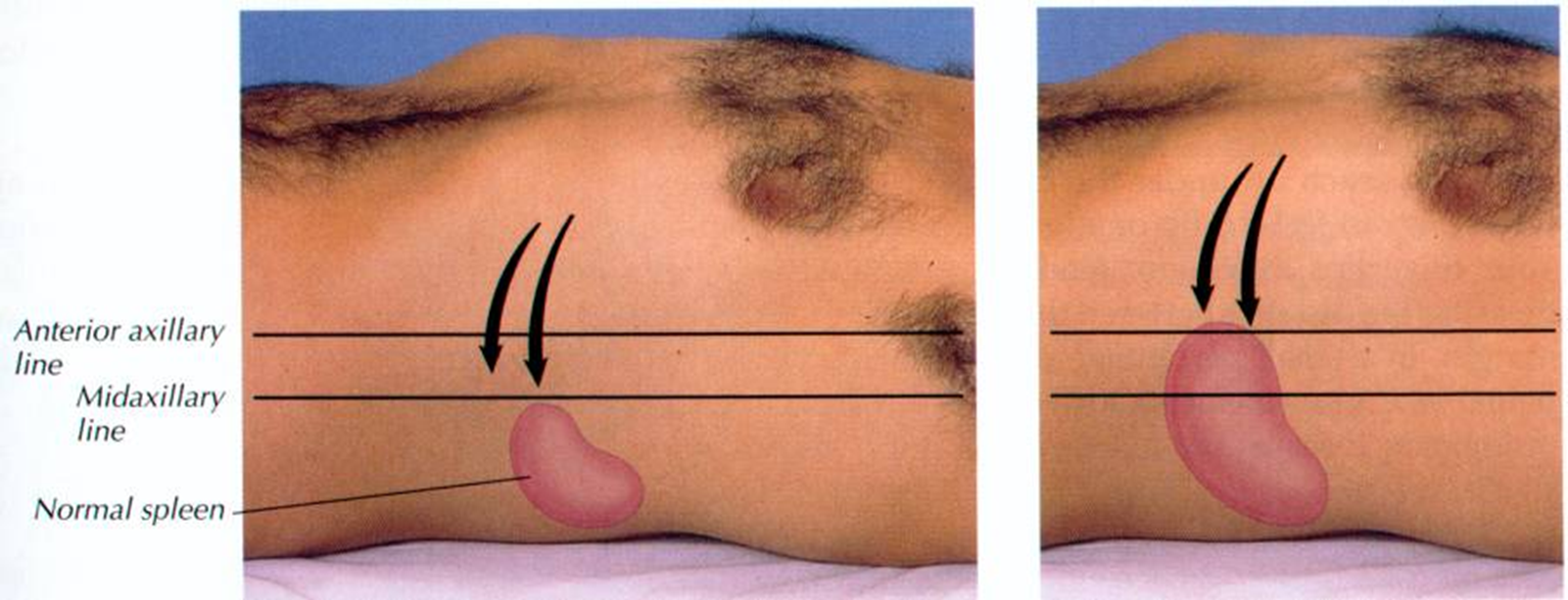
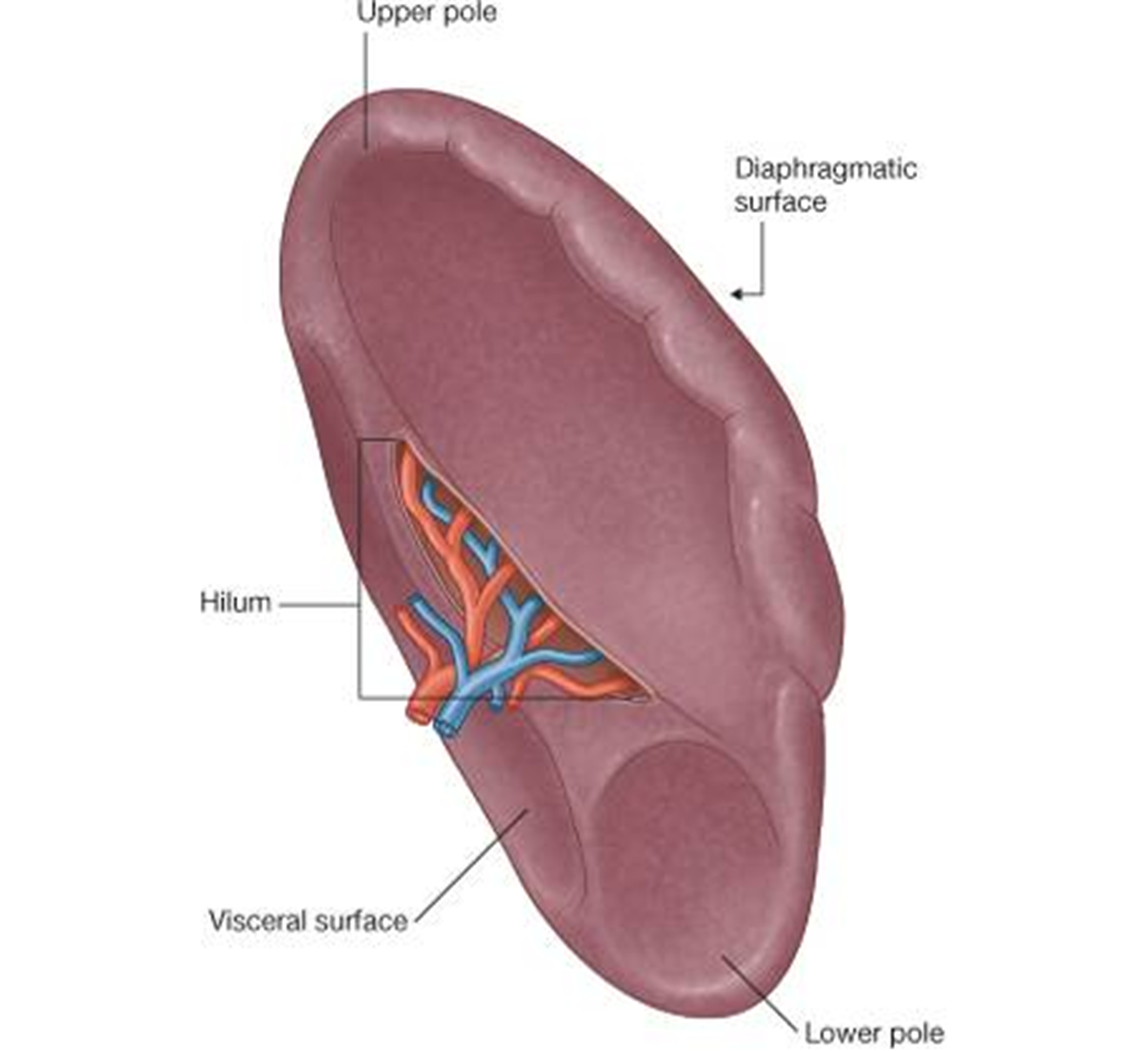
spleen
note derived from foregut
immune organ
highly vascular: filters blood
located on L sd within greater sac
It lies against the 9th-11th ribs
Clinical note: Trauma to these ribs can rupture the spleen causing profuse internal bleeding
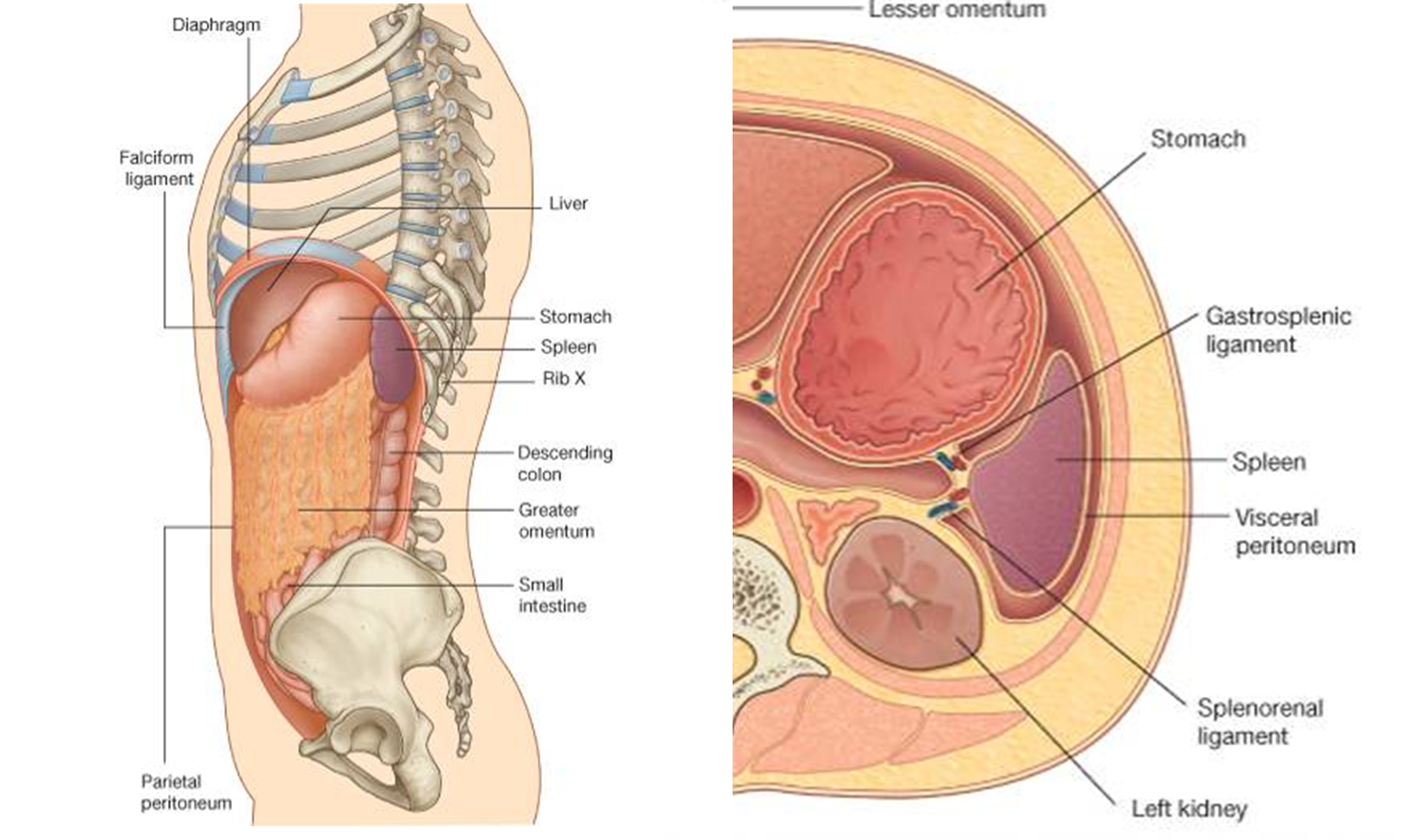
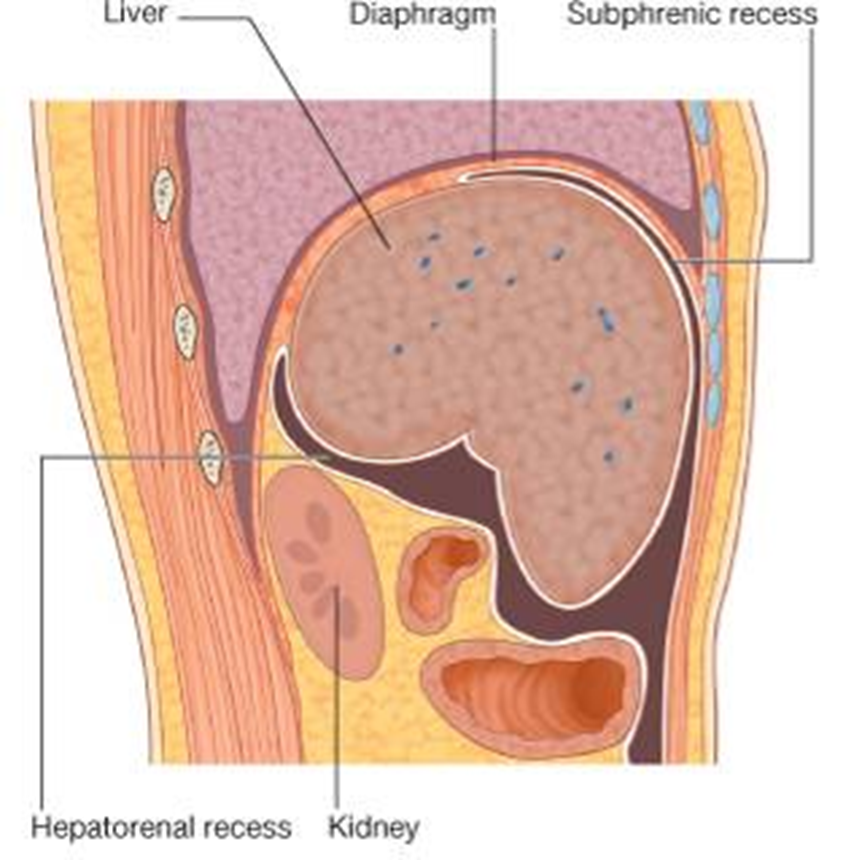
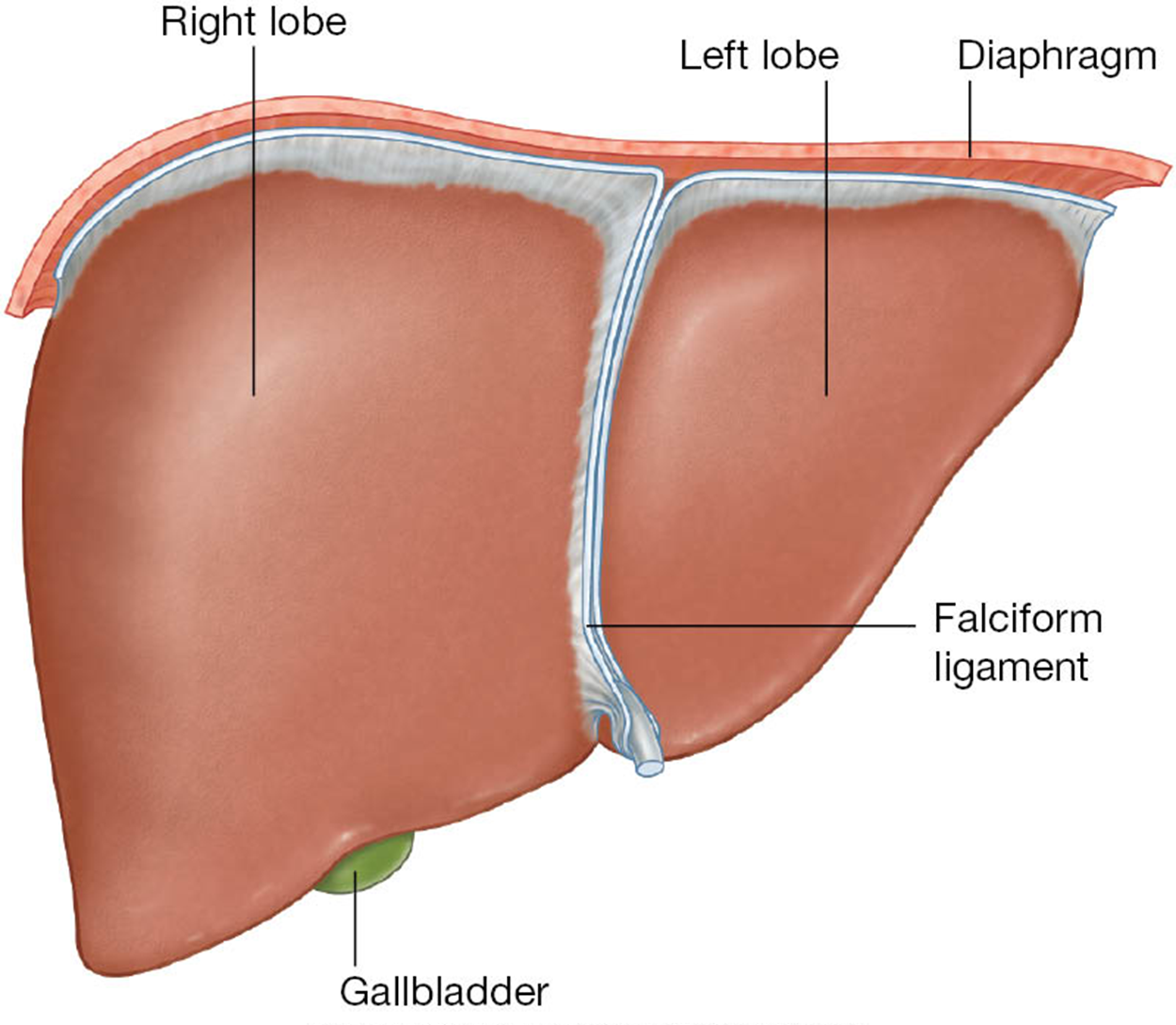
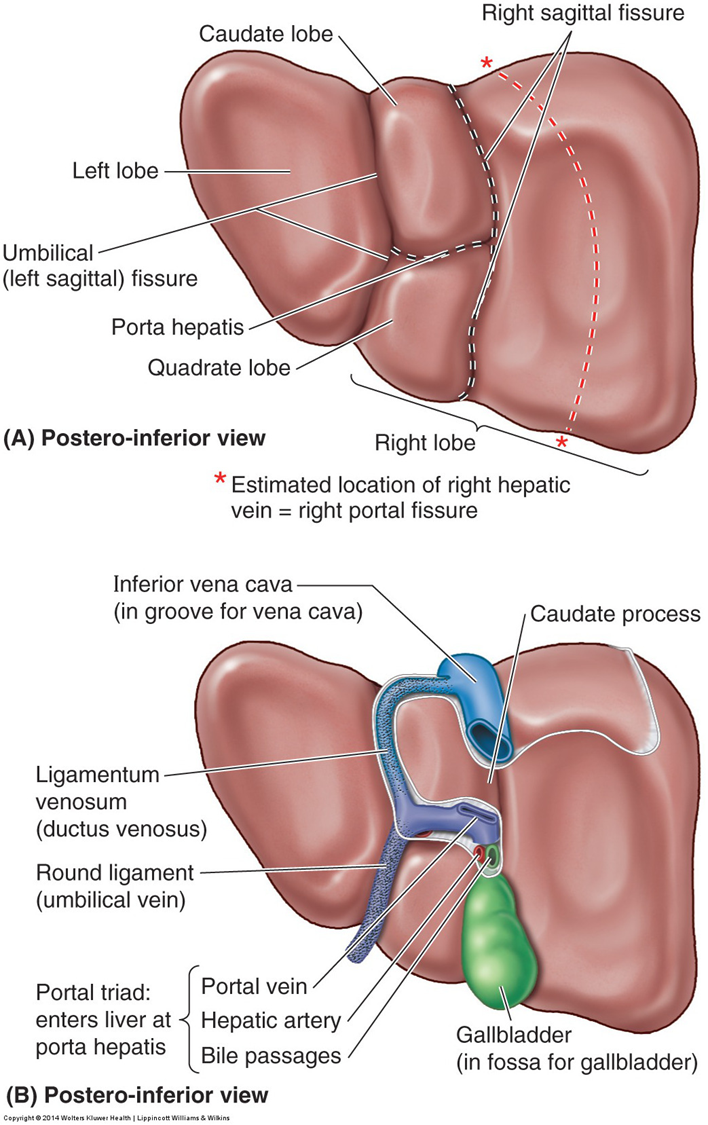
liver
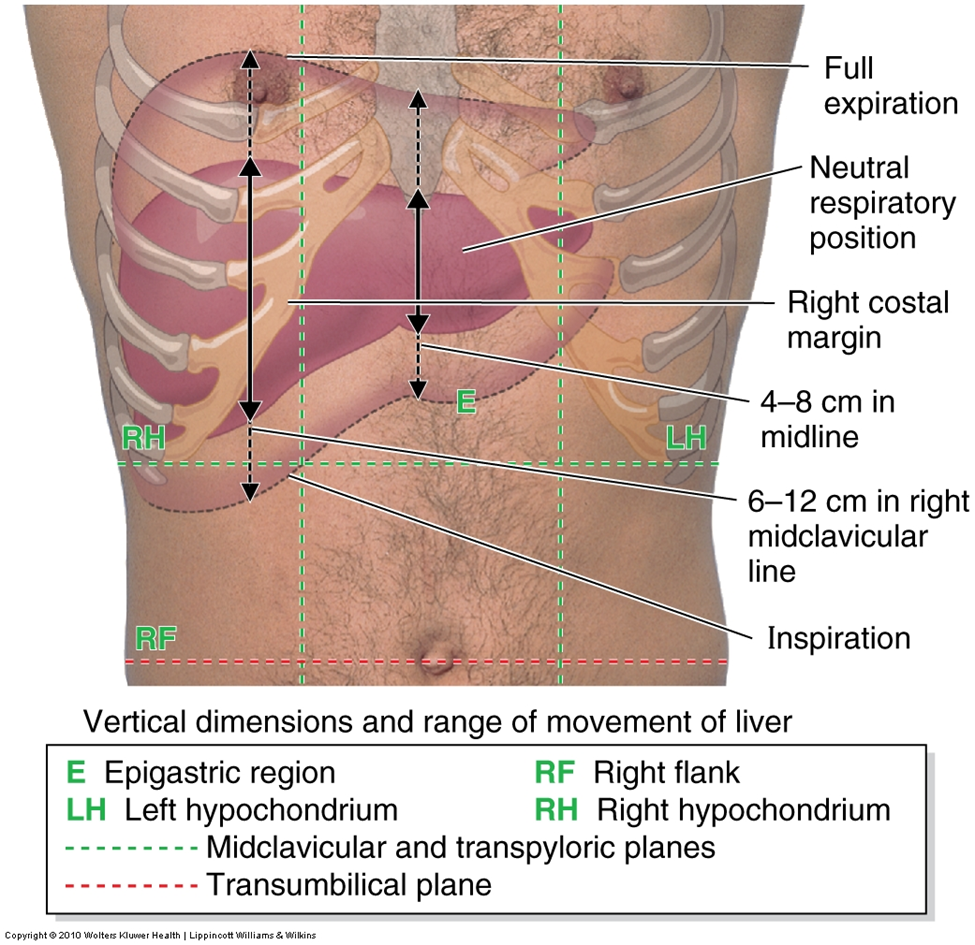
Largest, most vascular organ of abdominal cavity
Two surfaces
Diaphragmatic
Visceral
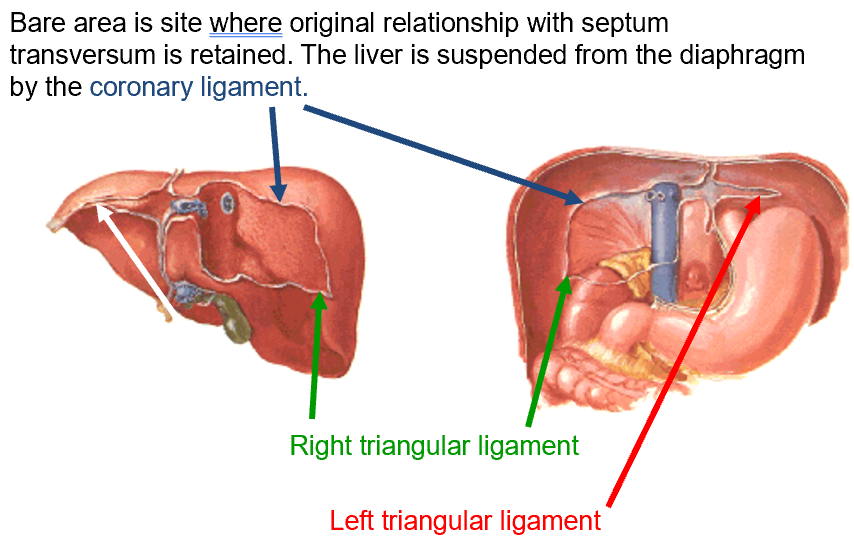
Bare area in direct contact with diaphragm
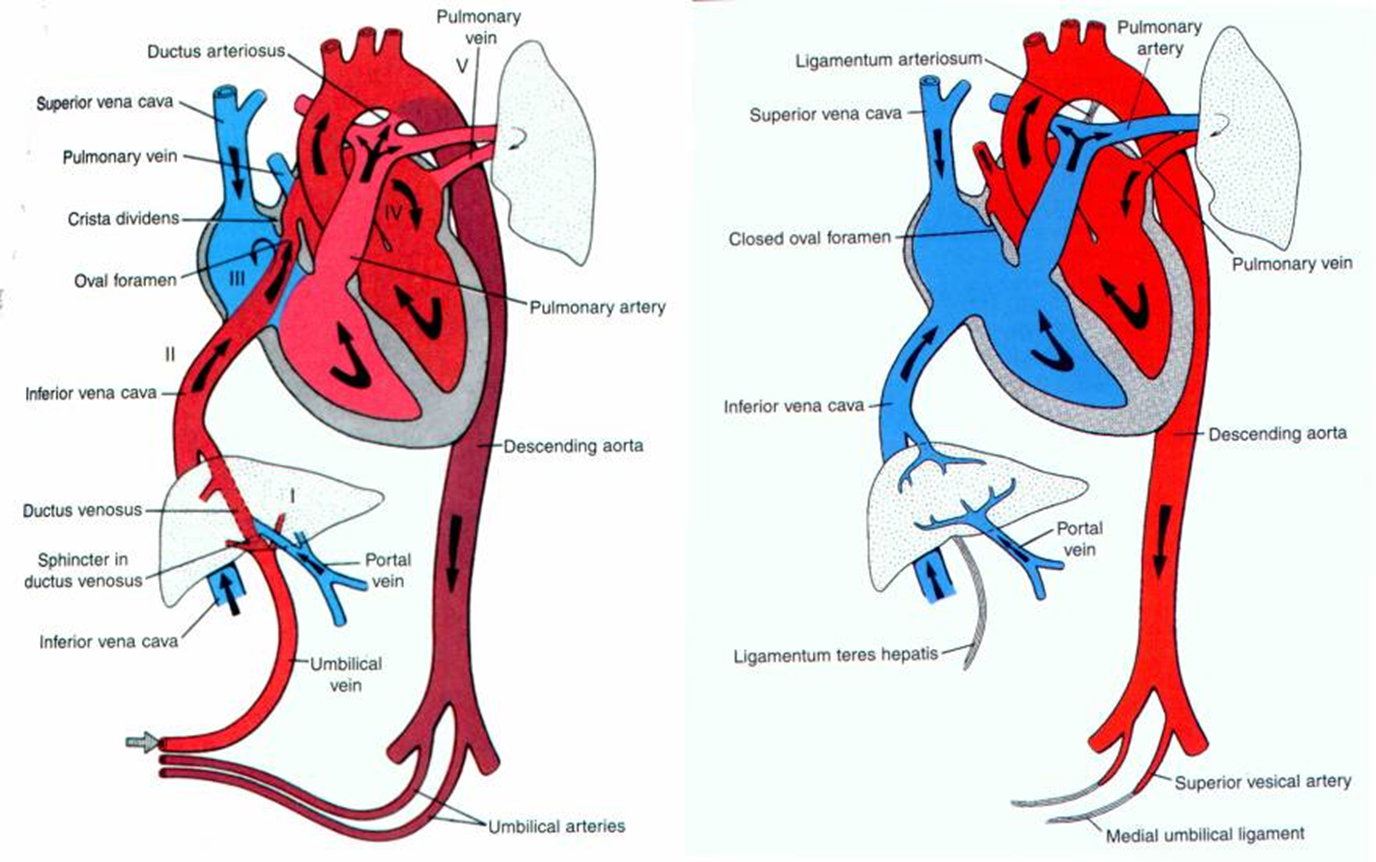
change from fetal to newborn circulation
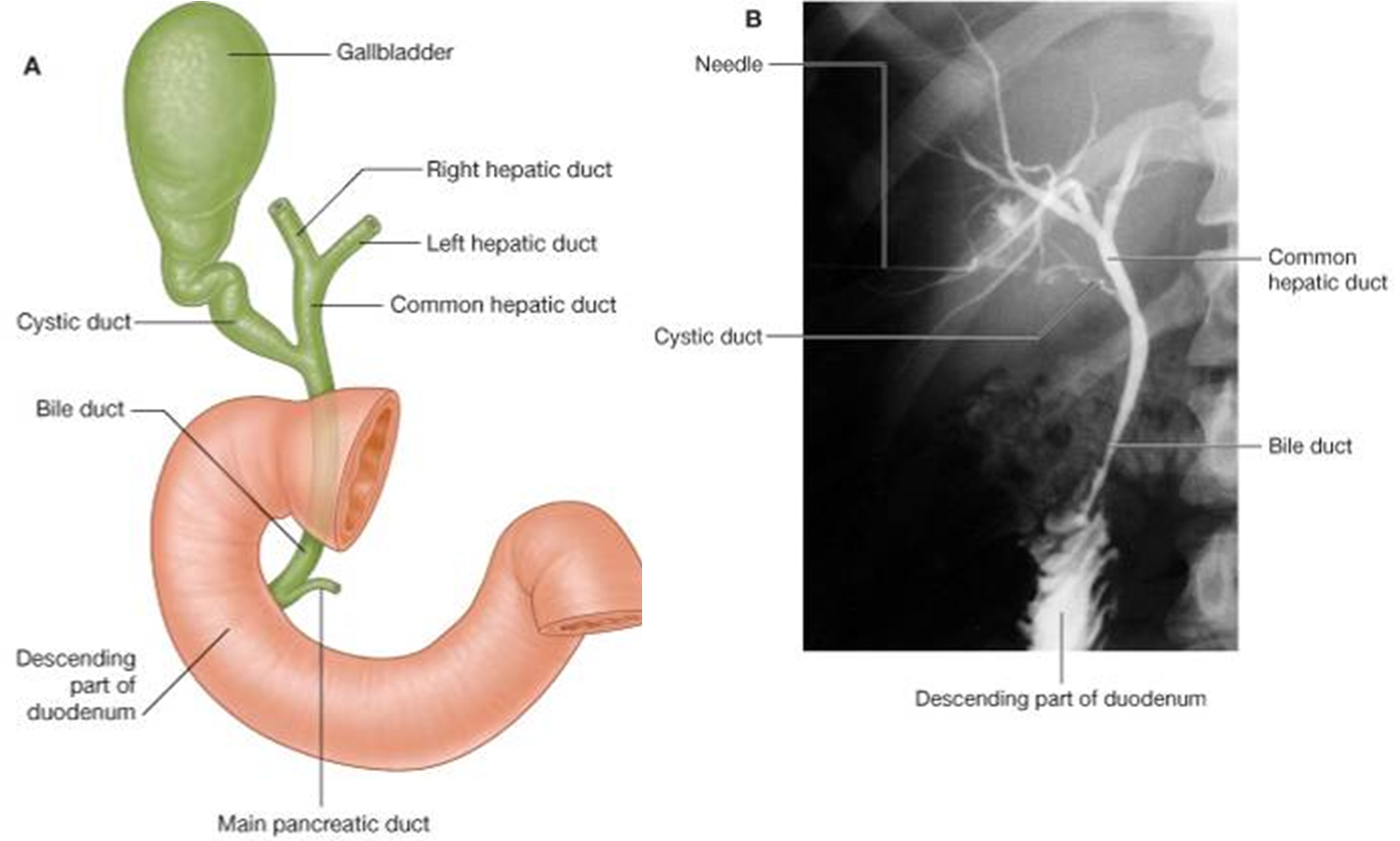
biliary tree
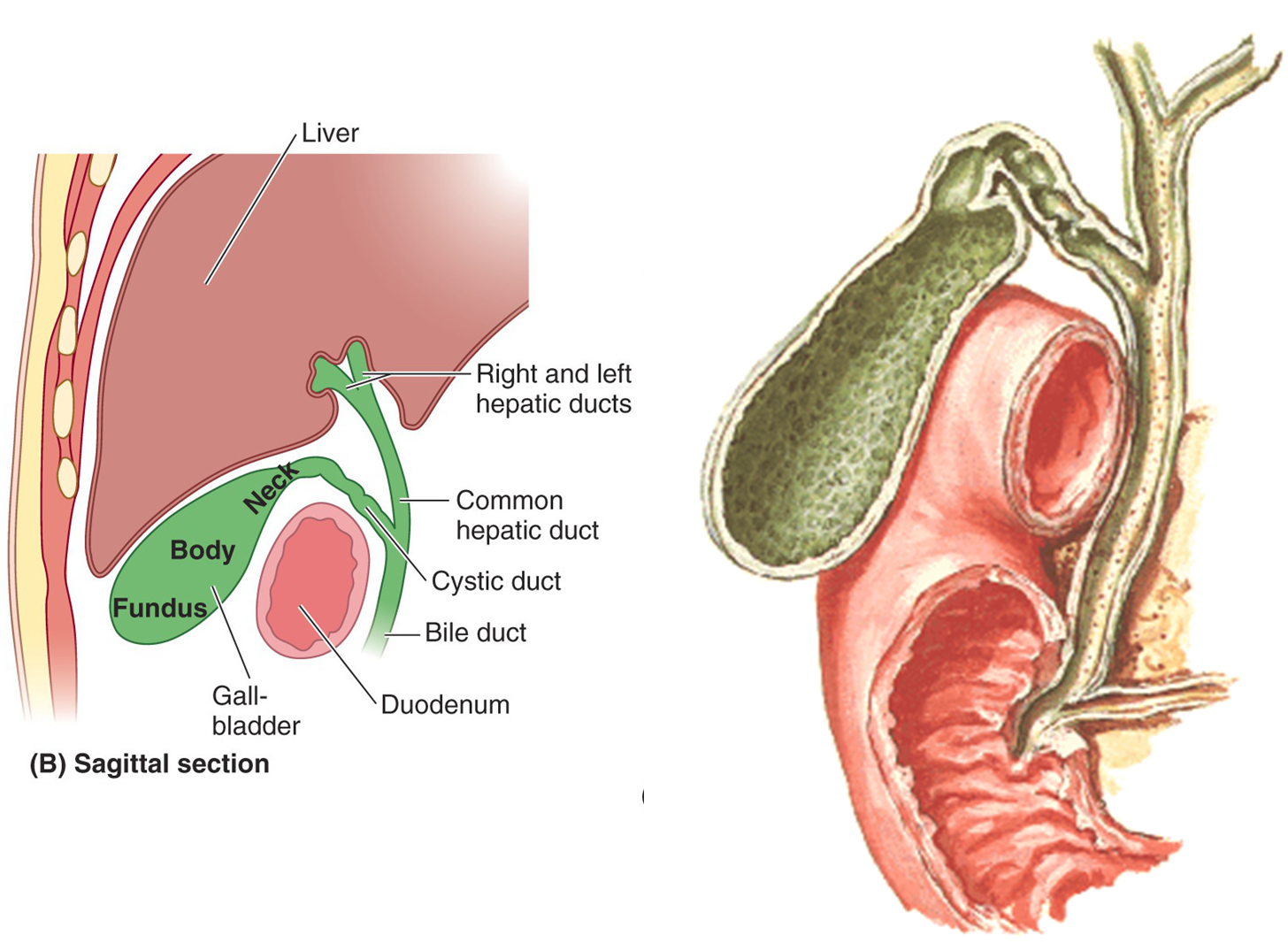
clinical note: gallstones
Gallstones common in Western society
Twice as likely in female than male
Americans have extraordinary rate of gallstones
Can remain asymptomatic
But, can cause severe epigastric or right upper quadrant pain
Pain can be referred to right shoulder
Some authors (your book) say that the right phrenic nerve provides sensory innervation to the gallbladder and that explains referred pain to the right shoulder
Others (your book in Blue Box) say that irritation of diaphragm explains referred pain
Large gallstones can cause obstructive jaundice
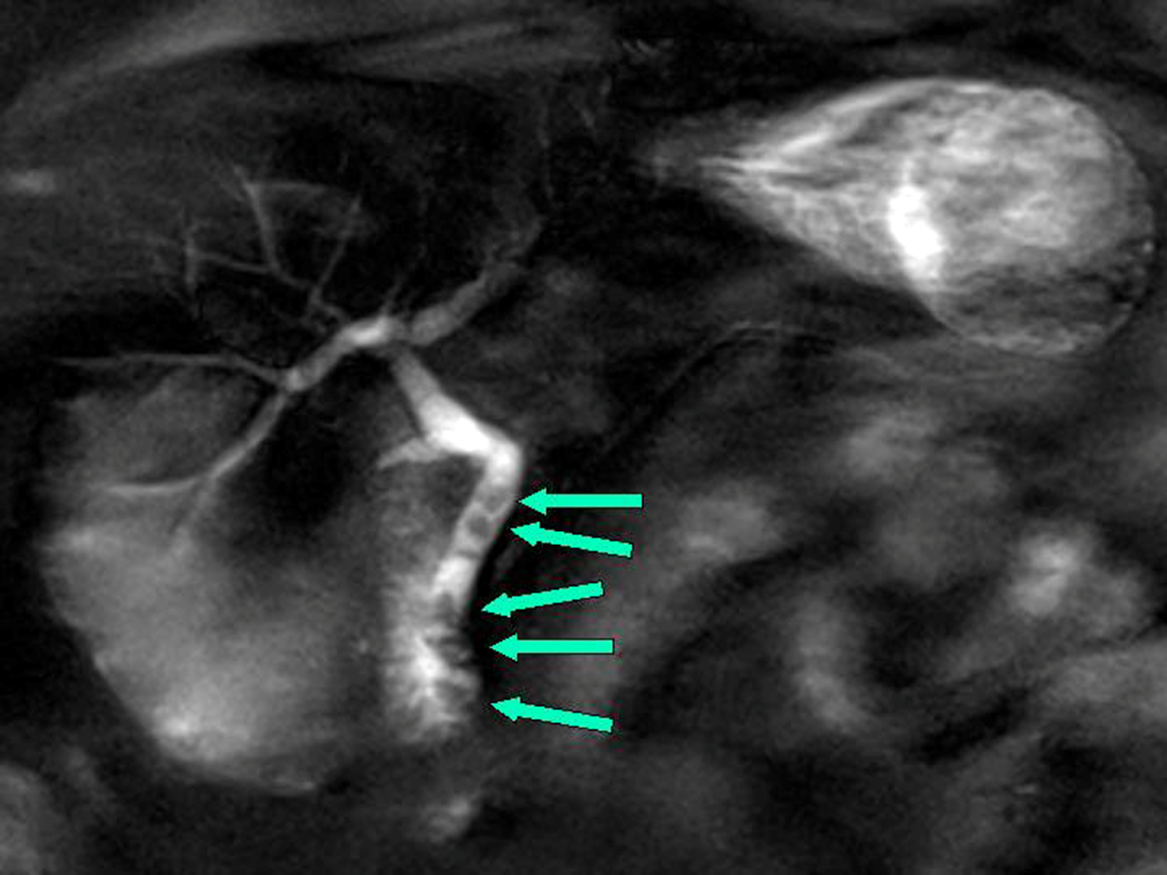
Magnetic Resonance Cholangiopancreatography (MRCP)
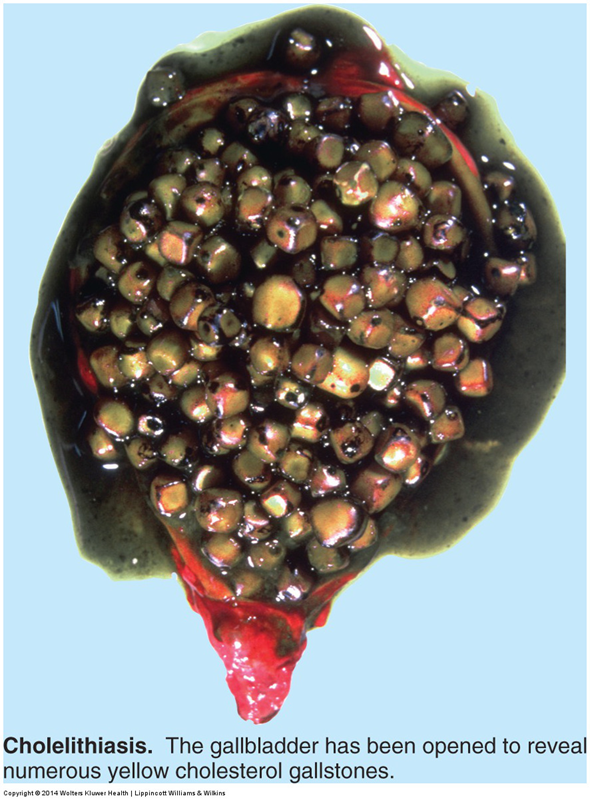
cholelithasis: cholesterol stones
Cholesterol gallstones are common in US
20% of men over 75yo
35% of women over 75yo
During reproductive years, women 3x more likely to develop cholesterol gallstones than men
cholelithiaisis: brpown pigment gallstones
Brown pigment stones almost always associated with bacterial cholangitis
Related to increased concentration of unconjugated bilirubin in bile

clinical note: gallbladder syndrome
Also known as 5F Syndrome
Fair – white with a light complexion
Fat – BMI>30
Female - XY
Fertile – one or more children
Forty or older
Right shoulder pain with dyspeptic flatulence is the best indicator.
clinical note: referred pain to R shoulder
Pain associated with visceral disease and inflammation is often referred to the body wall. This is because visceral afferents enter the spinal cord with somatic afferents.
Many texts say that the inflamed gallbladder can irritate the underside of the diaphragm, the patient may feel pain in their right shoulder.
Note: Your book says that the right phrenic nerve directly innervates the gallbladder. There may be some evidence supporting this proposition.
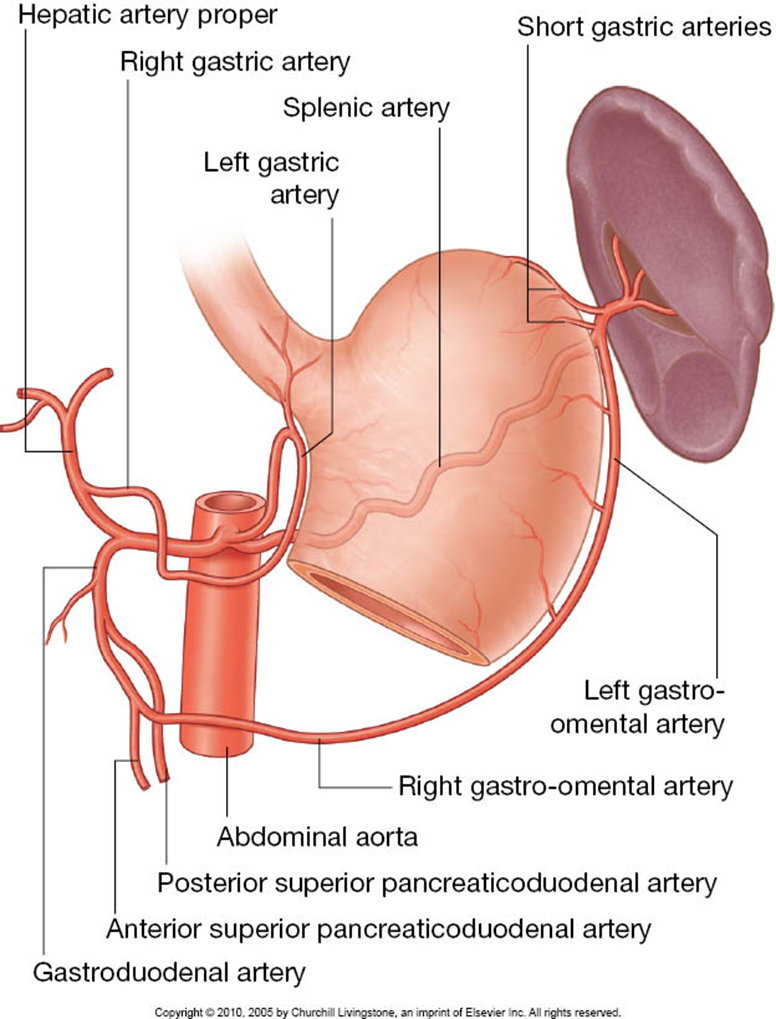
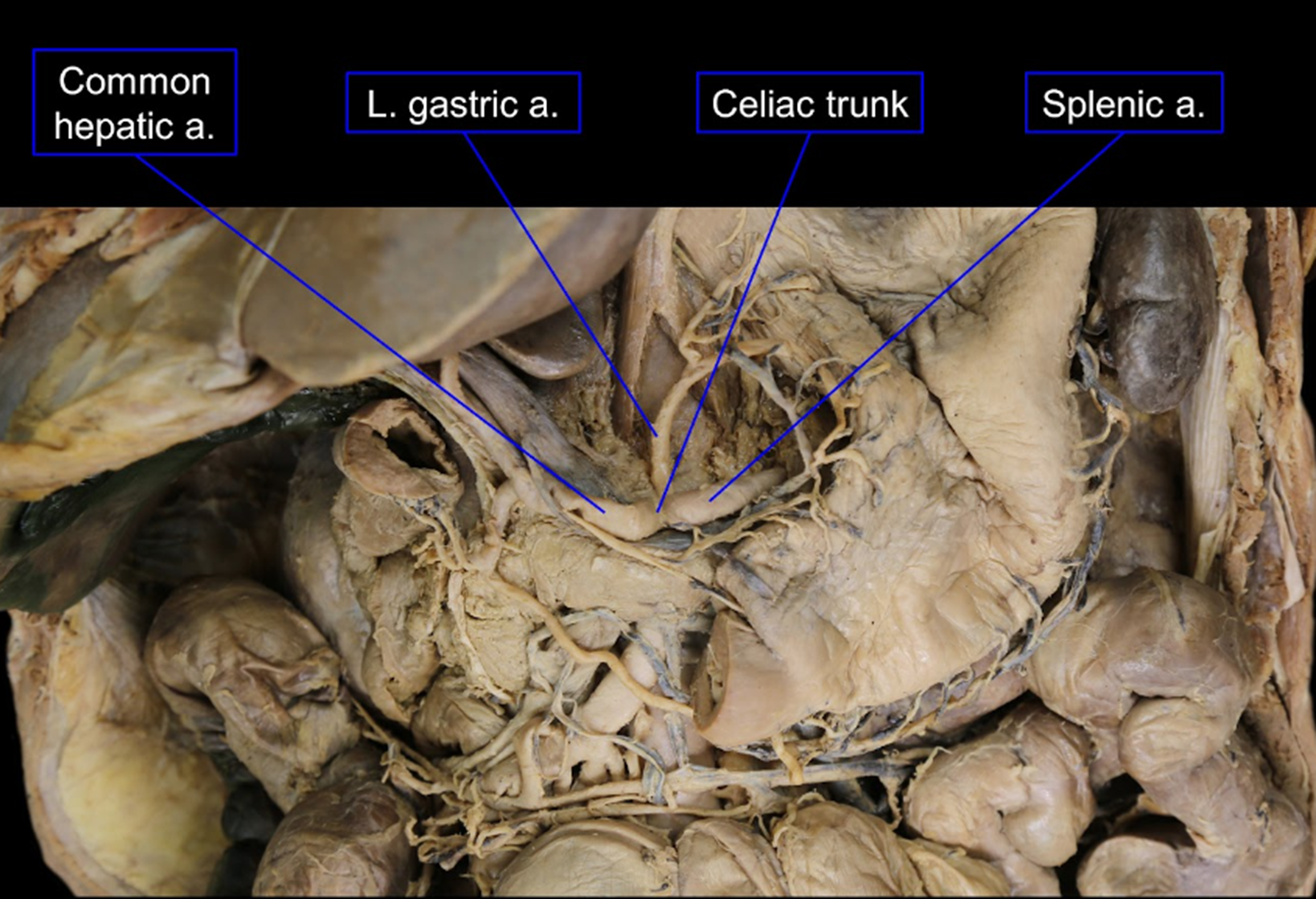
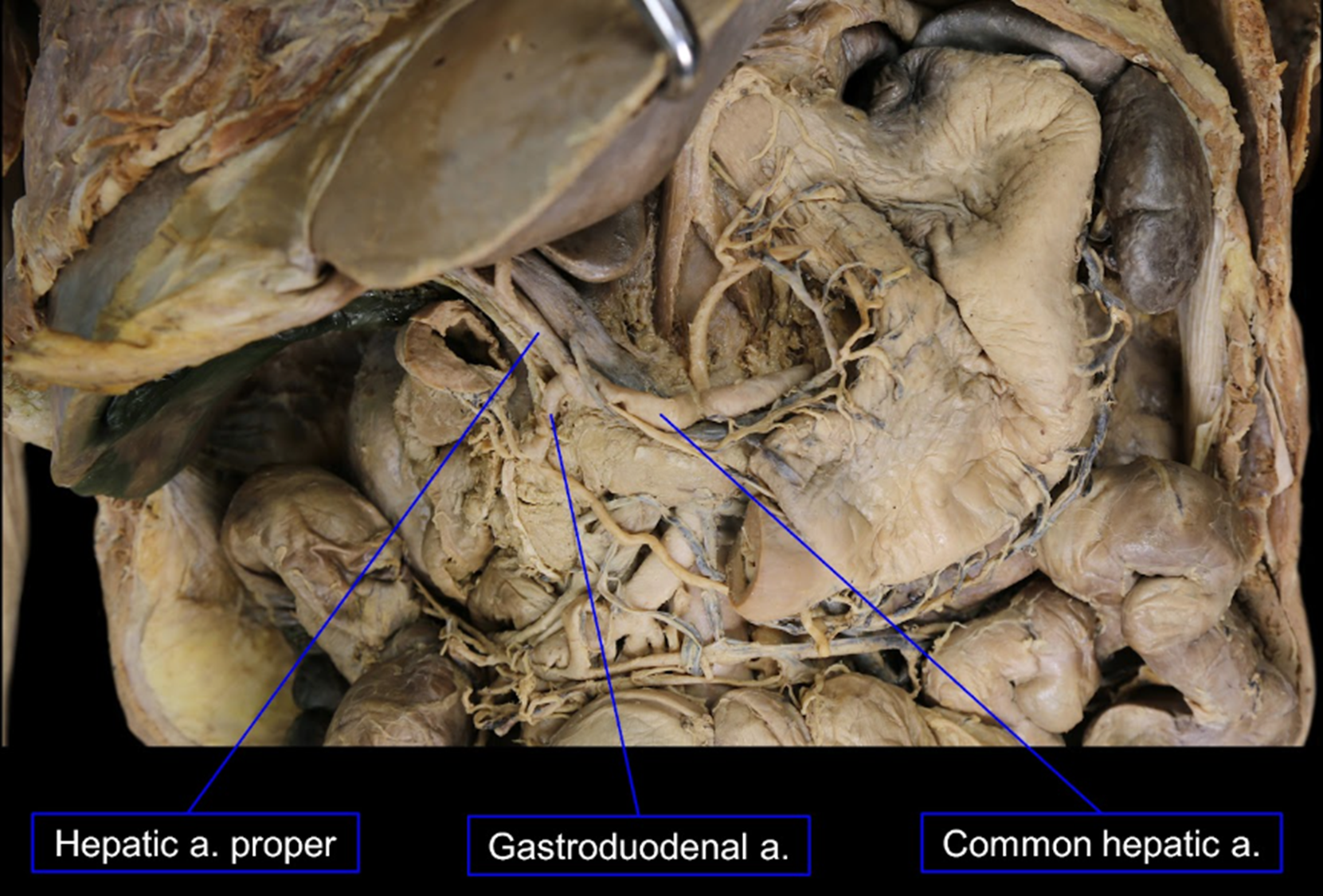
blood supply to foregut derivatives: celiac trunk
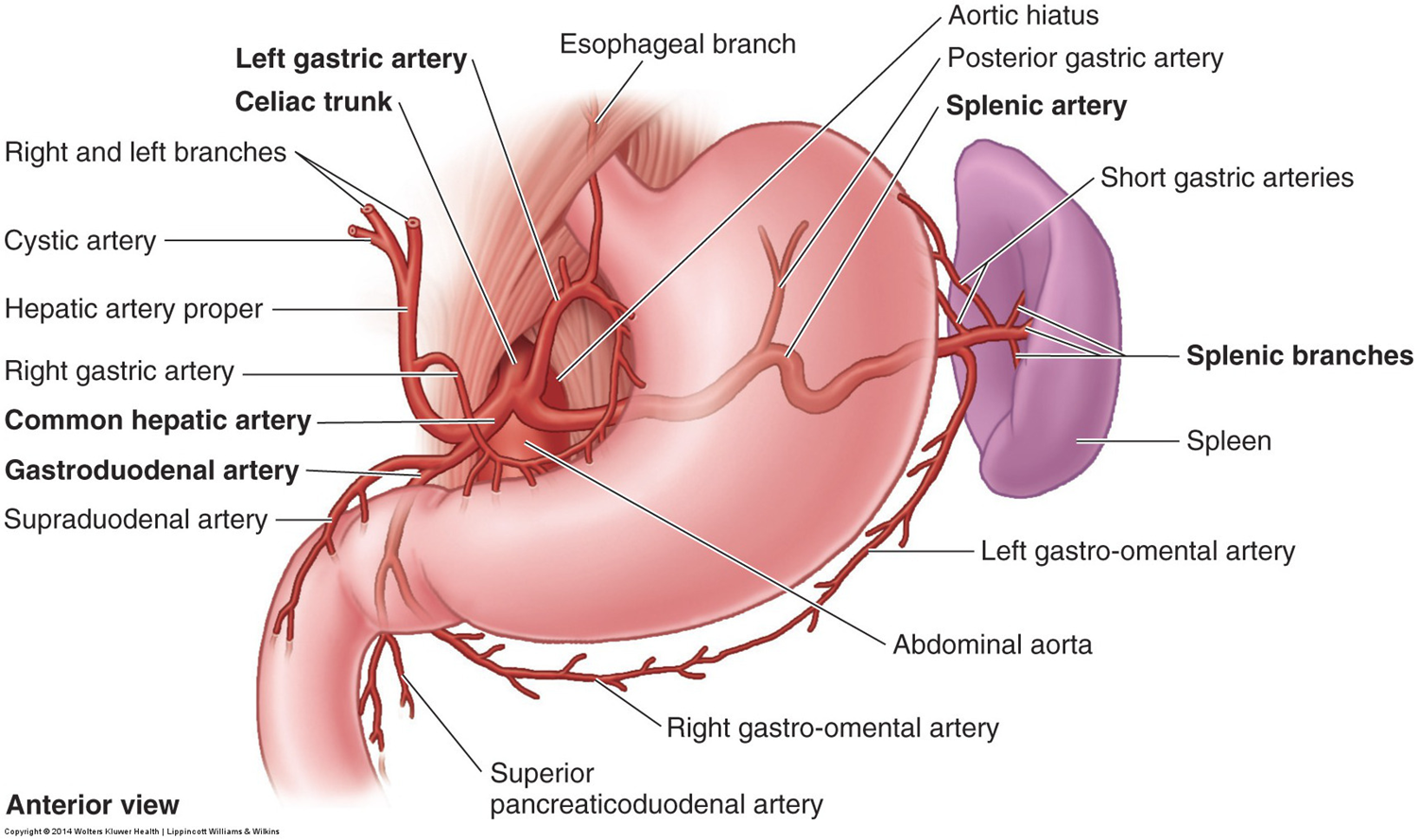
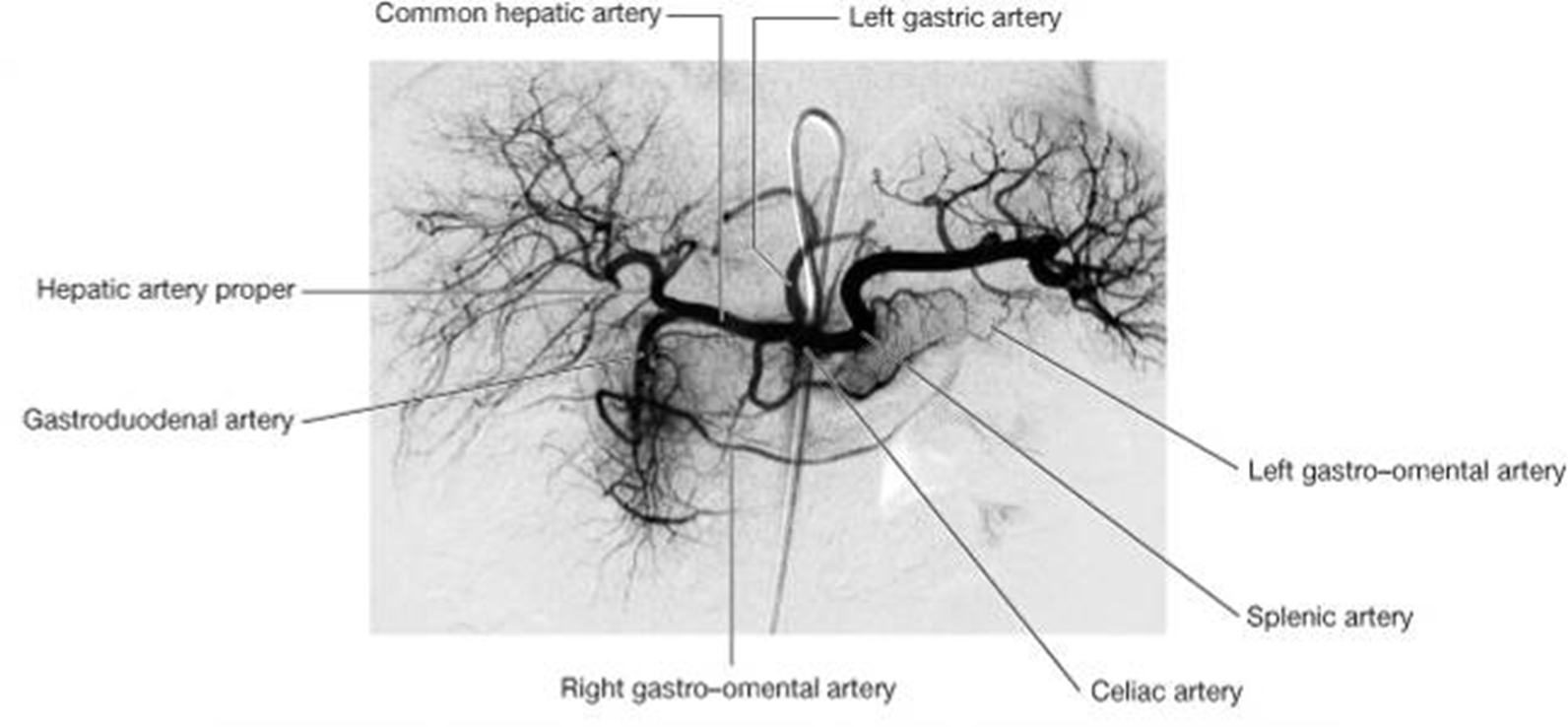
The pancreaticoduodenal arteries are anatomoses between the celiac trunk and the SMA.
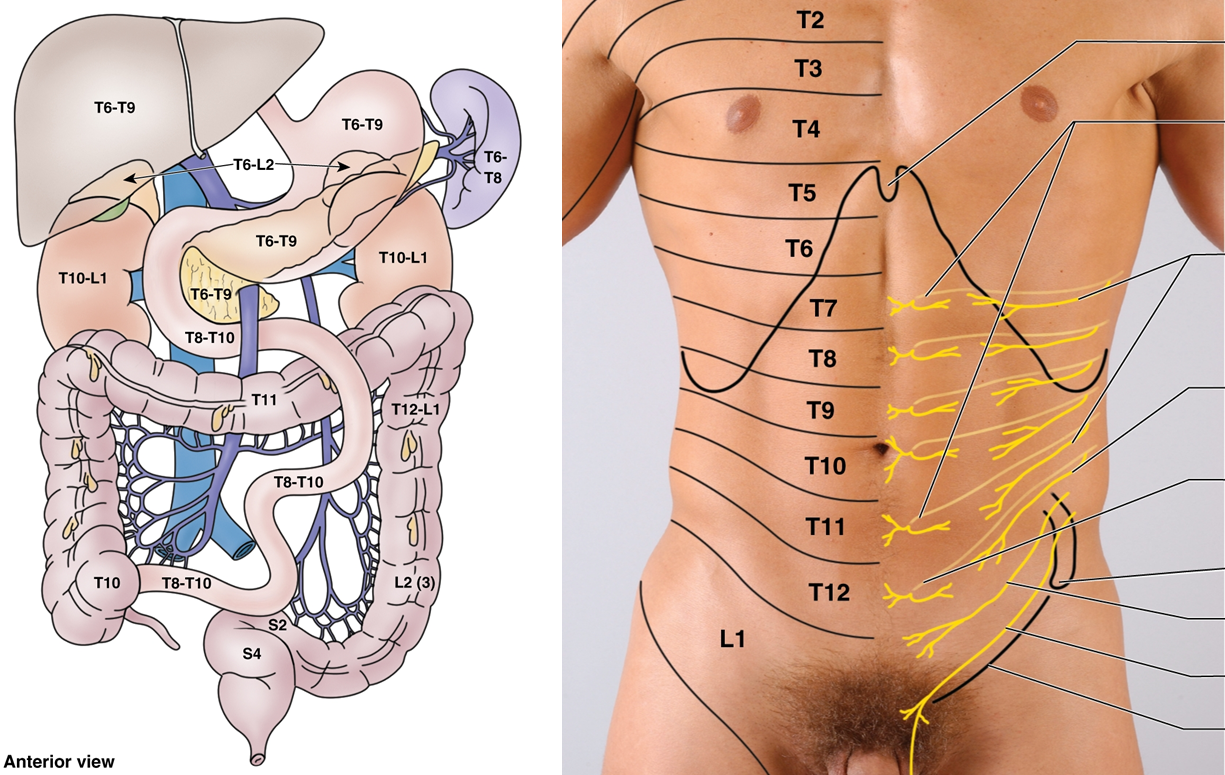
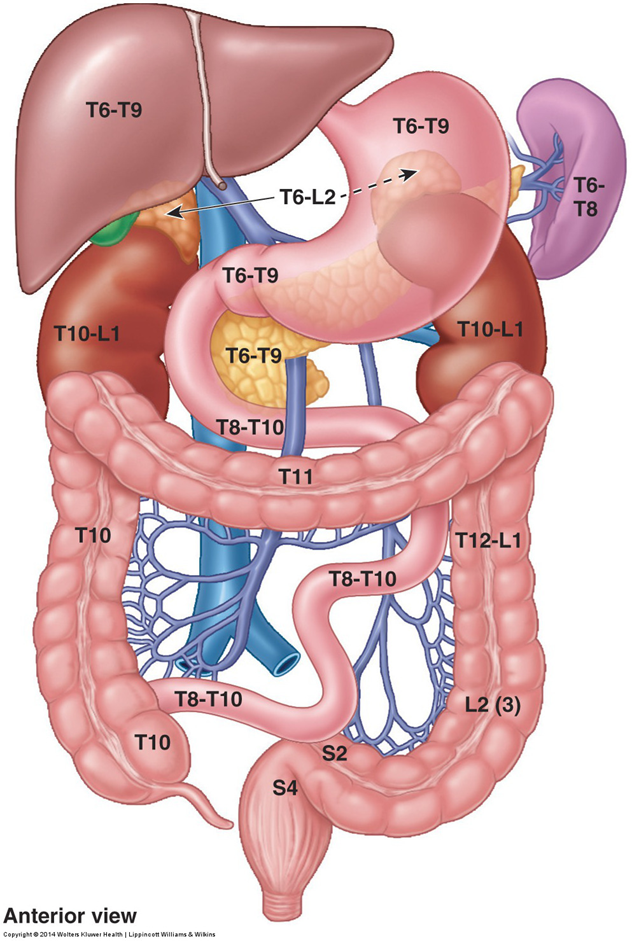
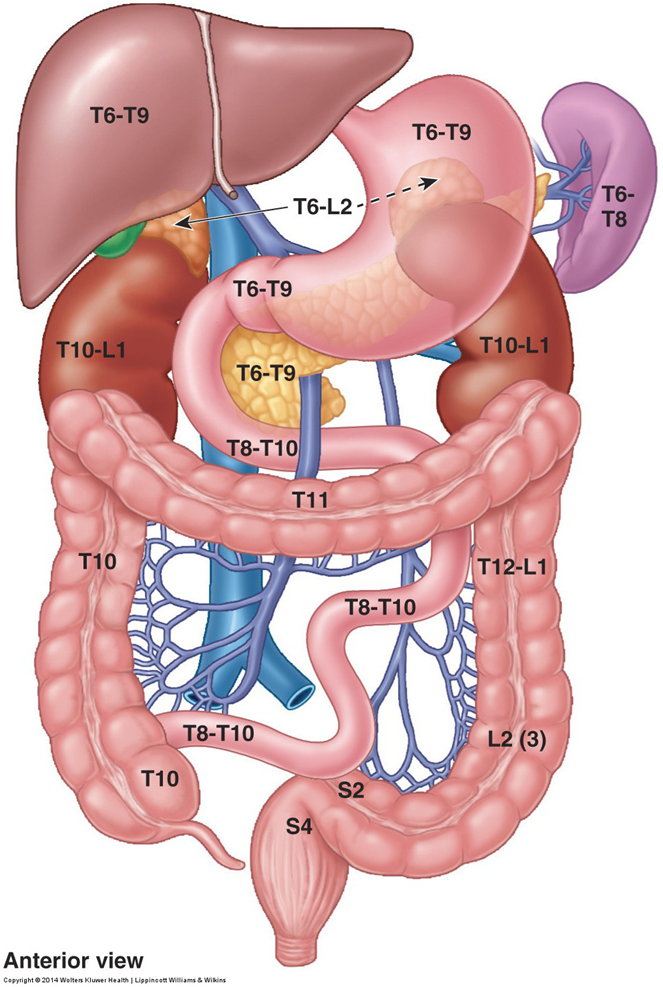
foregut innervation
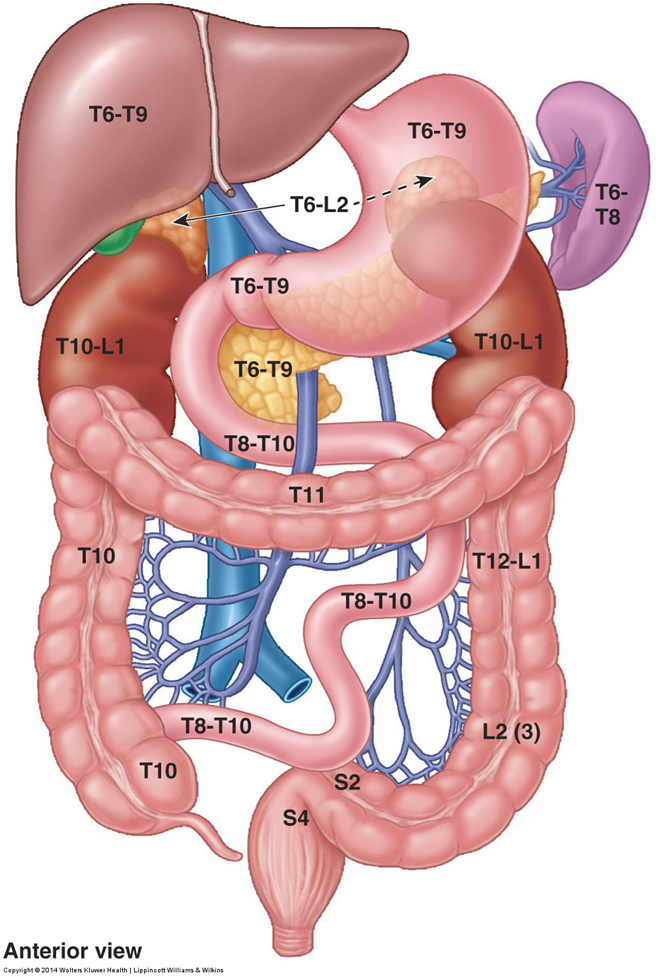
Receives sympathetic innervation from spinal cord segments T6-T9 via the greater splanchnic nerve that contains preganglionic sympathetic axons that synapse predominantly in the celiac ganglion.
Pain afferents run with the sympathetics.
Other afferents, such as stretch and distension, run with the parasympathetics (vagus).
midgut derivatives
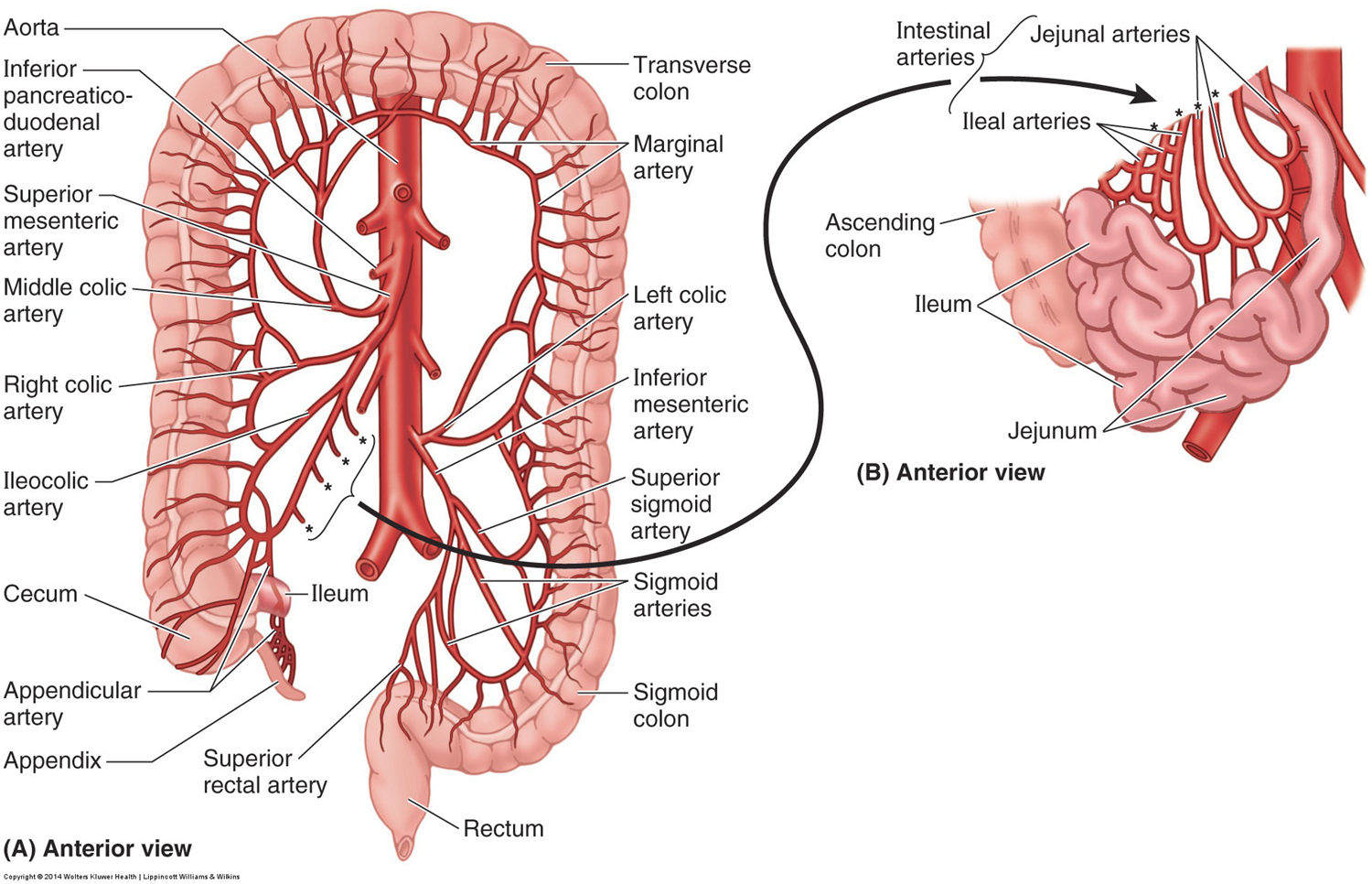
Supplied by branches of the superior mesenteric artery
Distal duodenum
Jejunum
Ileum
Cecum and appendix
Ascending colon
Proximal 2/3rds of transverse colon
Relationship of superior mesenteric vein and artery to the uncinate process of the pancreas is an important one.
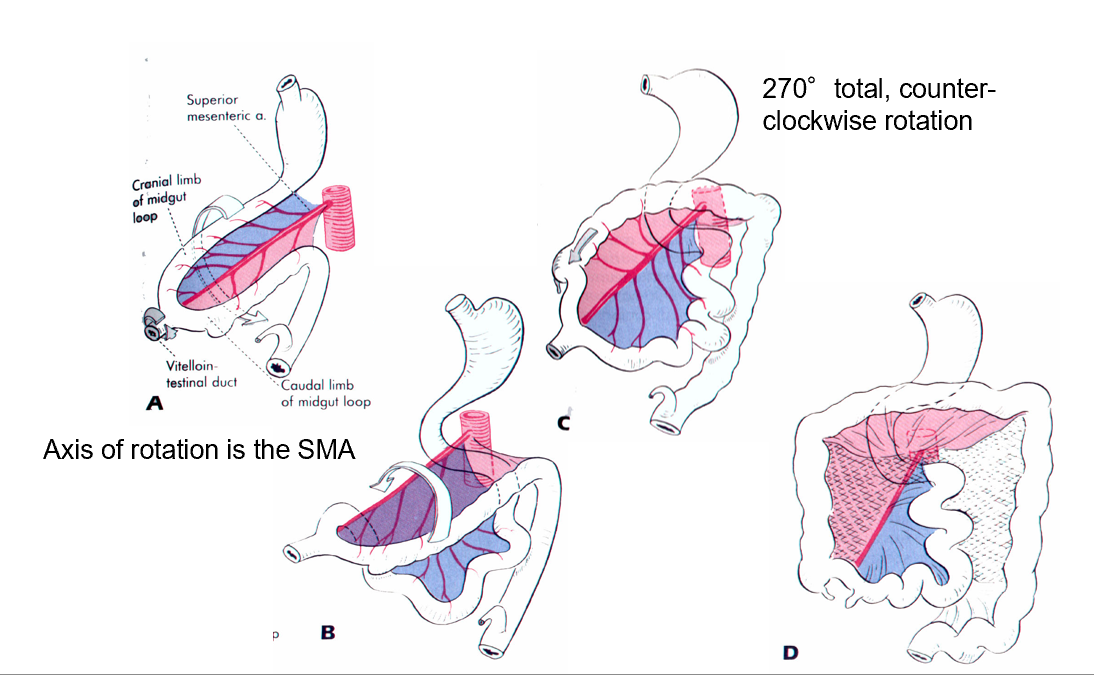
development
small intestine
Small intestine is 7 meters long
Duodenum, described above, is the initial portion of small intestine
Jejunum is the upper 2/5ths of the remainder
Mostly located in left upper quadrant
Ileum is lower (more distal) 3/5ths
Mostly in right lower quadrant
Suspended in abdominal cavity by mesentery (mesentery proper)
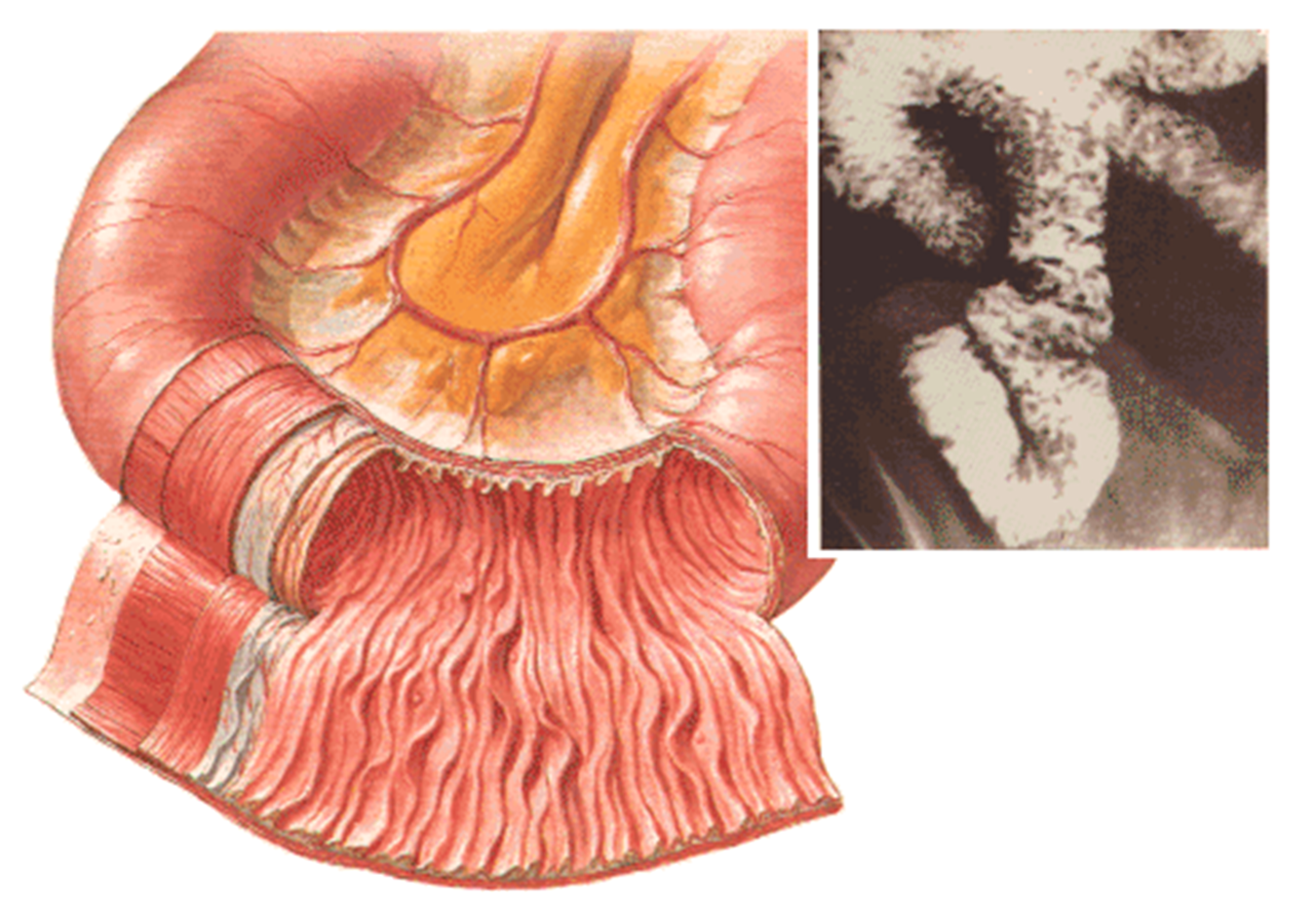
jejunum
Prominent plicae circulares, intestinal folds
blood supply: Less prominent arterial arcades and long vasa recta are a feature of the jejunum
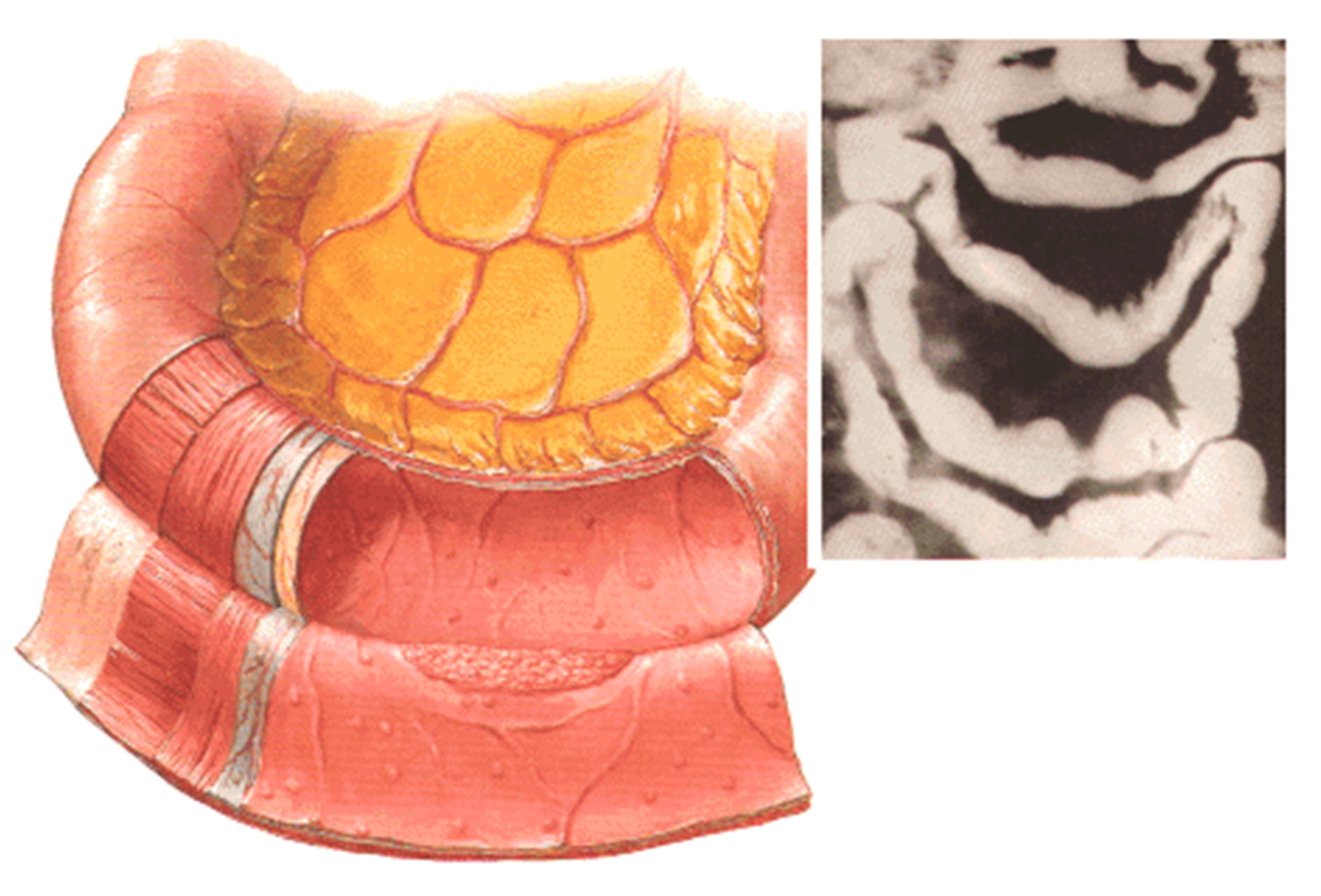
ileum
Less prominent plicae circulares, intestinal folds. Has antimesenteric Peyers patches (arrow).
blood supply Compared to the jejunum (A), the ileum (B) has more arterial arcades and shorter vasa recta.
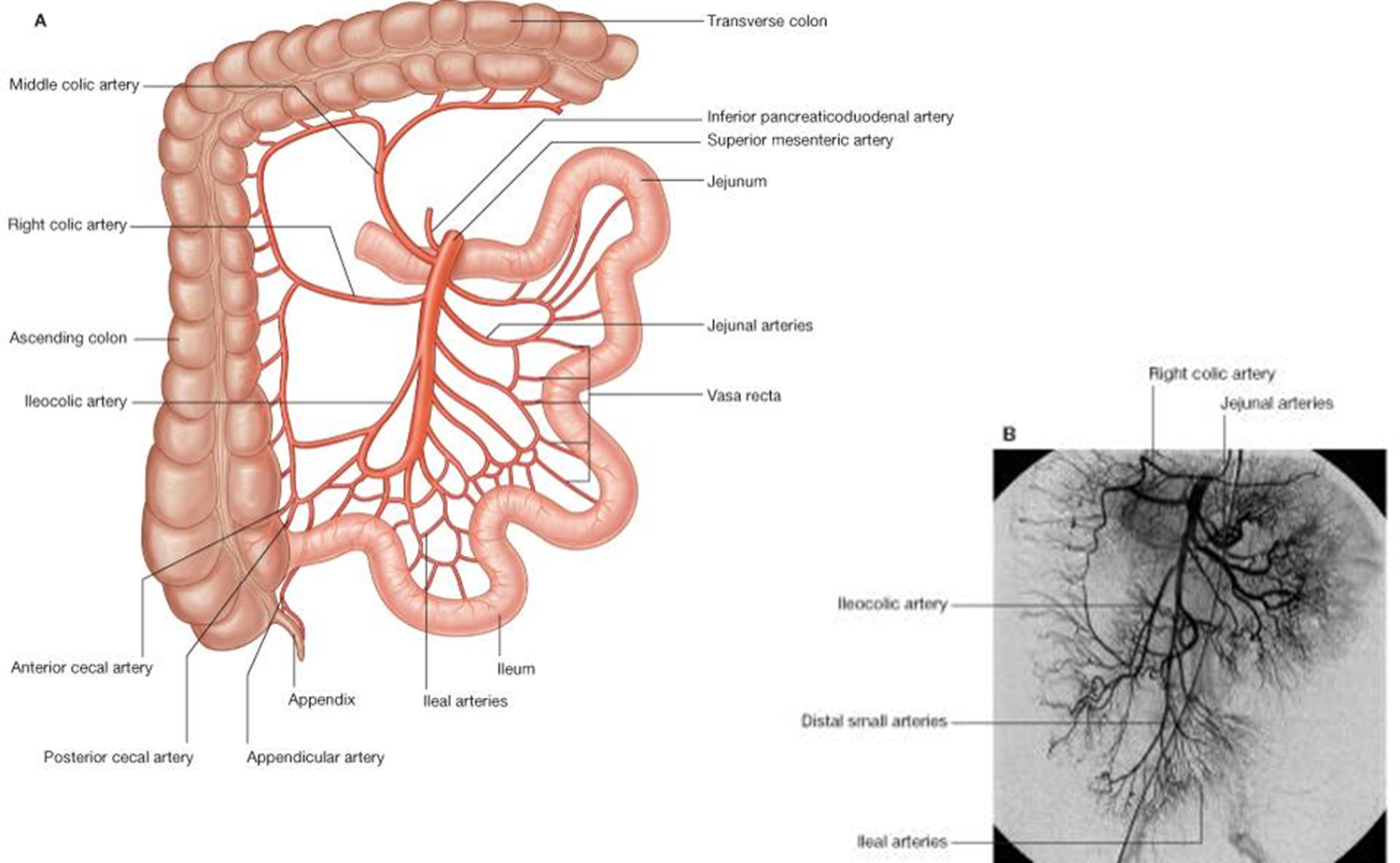
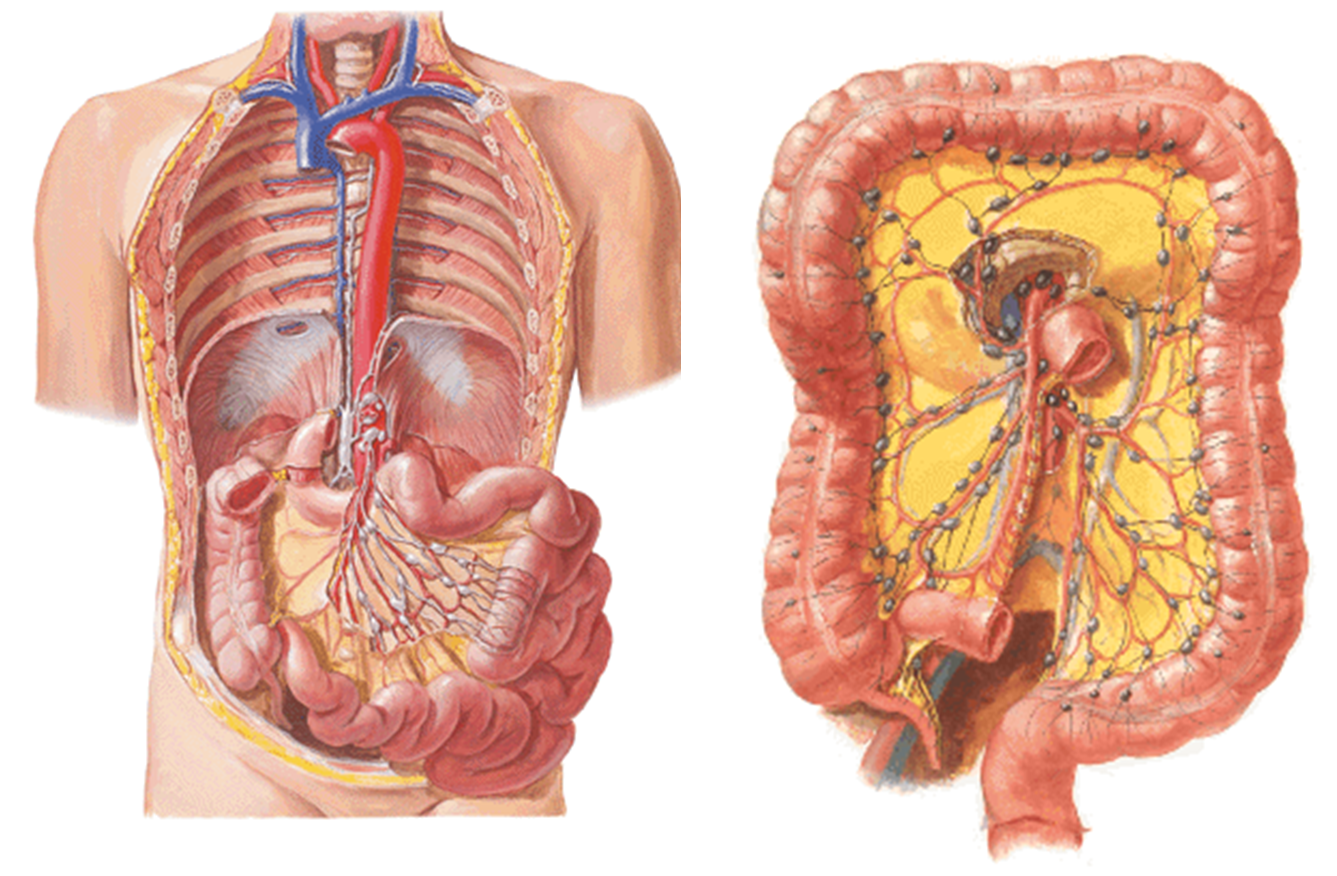
blood supply to midgut
SMA arises at the level of the lower border of L1.
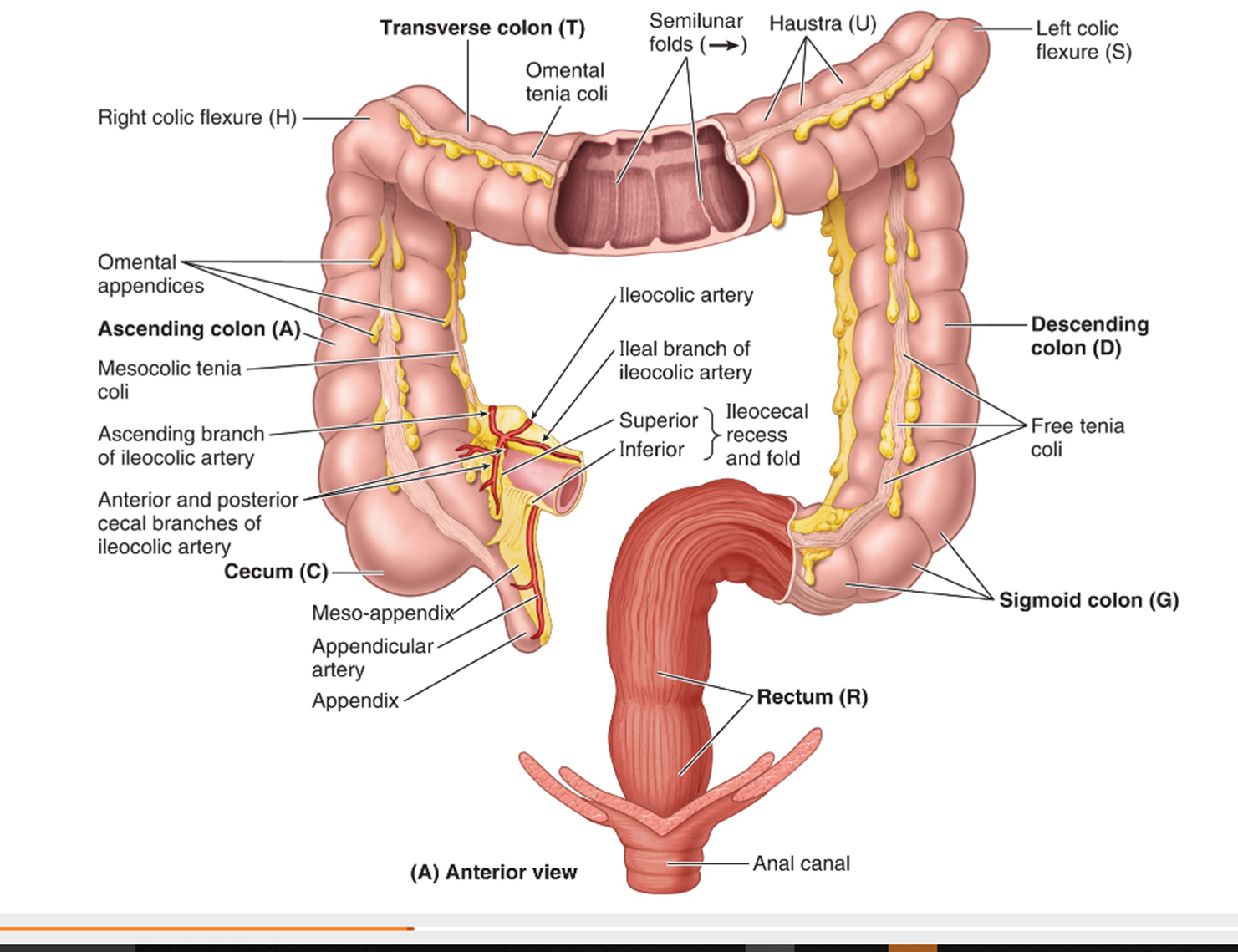
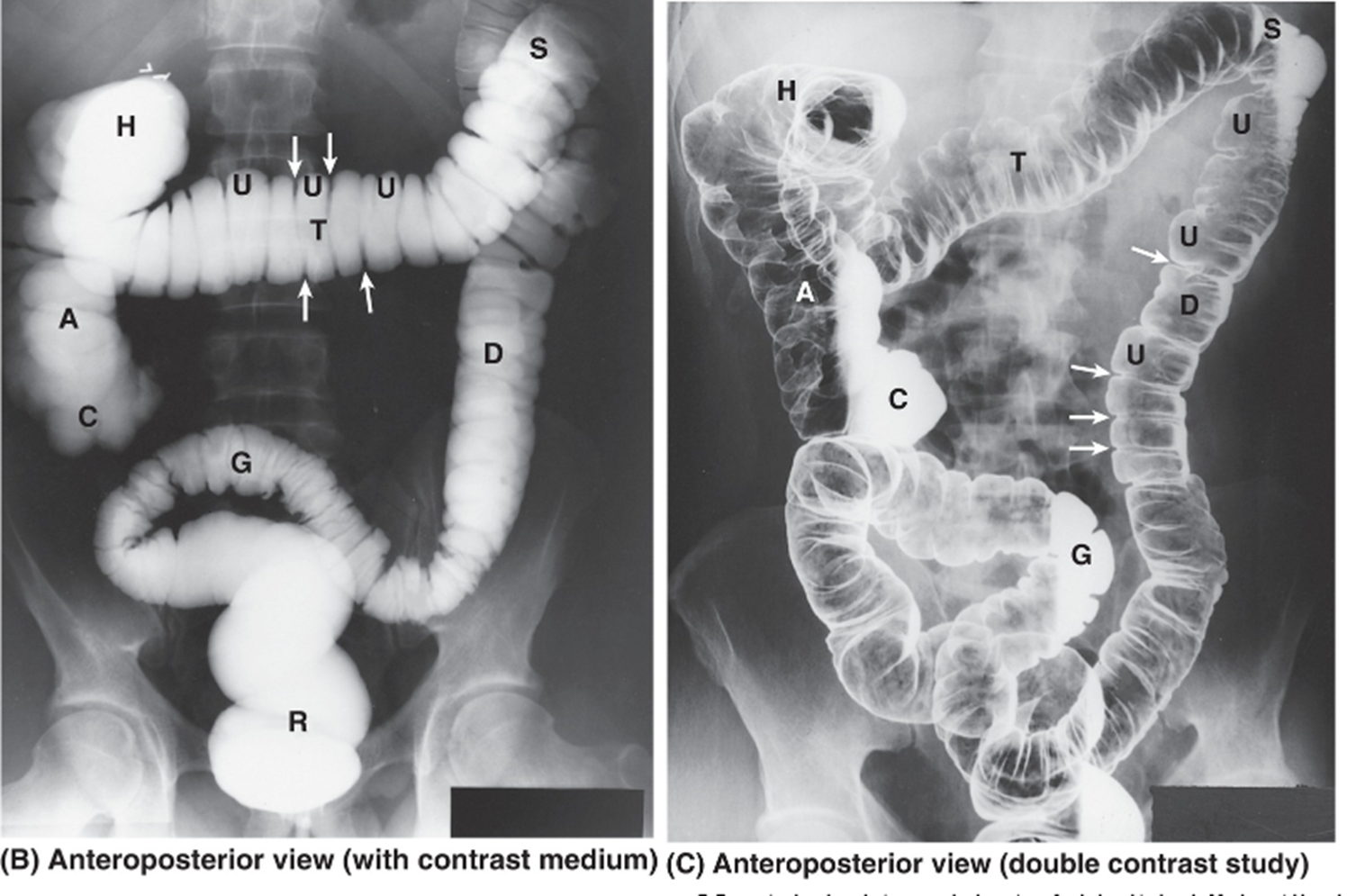
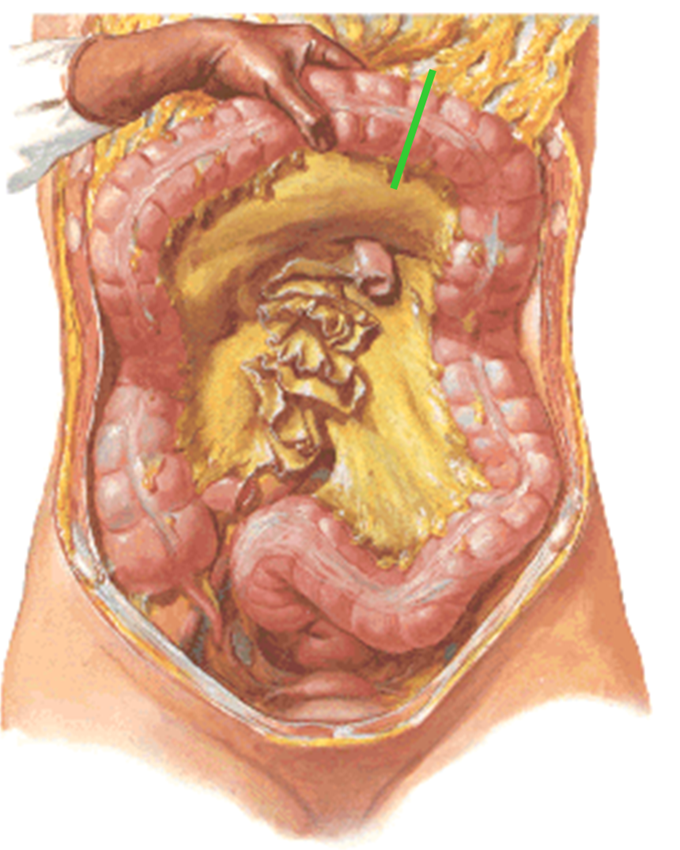
large intestine or colon
1.5 meters long
Made up of 7 parts
Midgut derivatives
Cecum
Dilated saccular pouch in right iliac fossa
Appendix attached about 2cm below ileocecal junction
Ascending colon
Proximal 2/3rds of transverse colon
Hindgut derivatives
Distal 1/3rd of transverse colon
Descending colon
Rectum
Anal canal
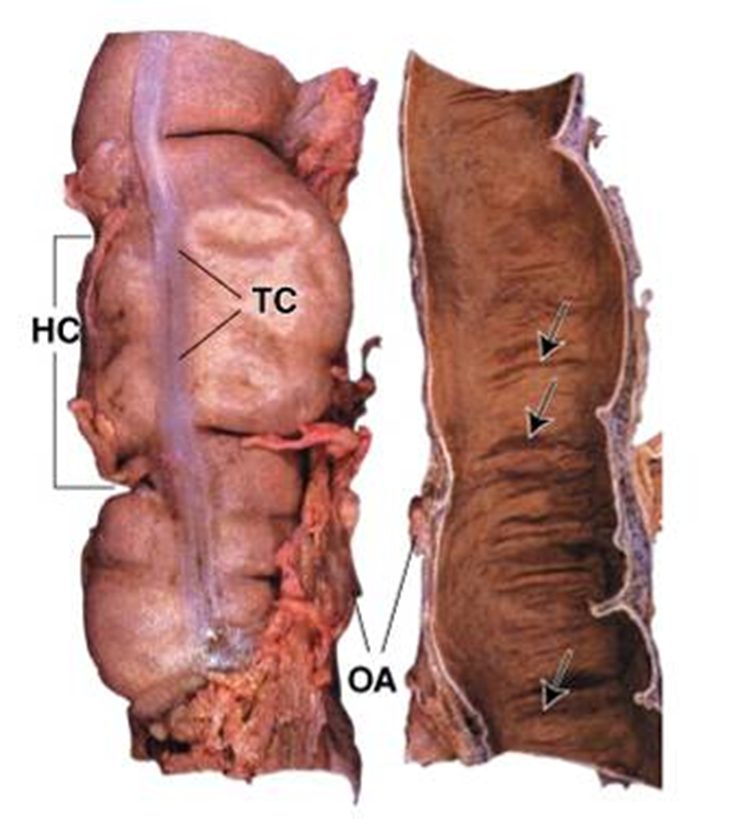
Teniae coli (TC): Three distinct bands of longitudinal muscle
Haustra coli (HC): Sacculations evident between teniae
Omental appendages (OA): Tabs of fat
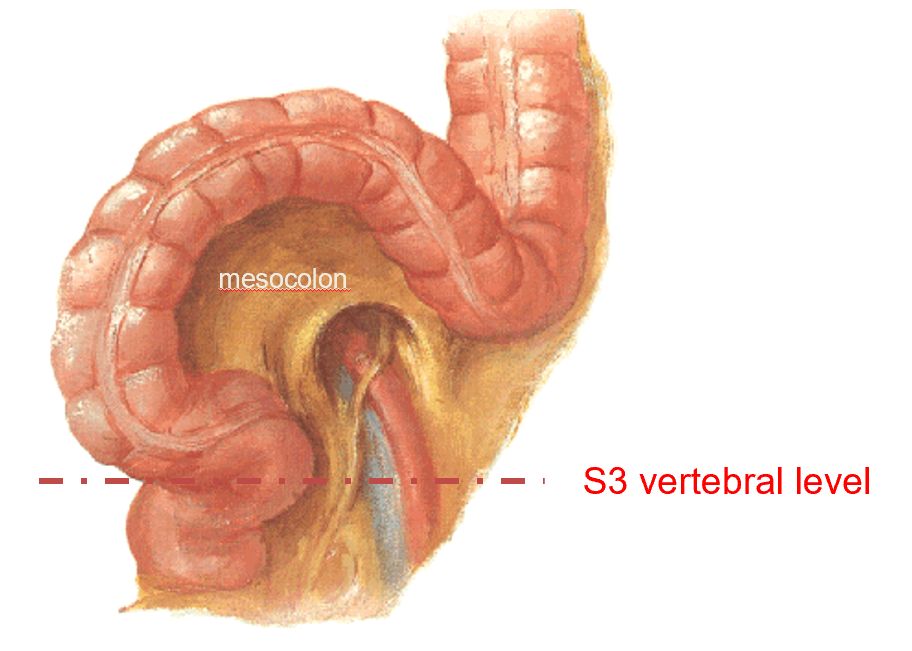
The rectosigmoid junction is at the S3 vertebral level.
midgut innervation
Receives sympathetic innervation from spinal cord segments T8-T12 via preganglionic sympathetic axons in the greater, lesser and least splanchnic nerves that synapse in the celiac, aorticorenal, superior and inferior mesenteric ganglia. The postganglionic sympathetic axons follow the arteries to their targets.
Pain afferents run with the sympathetics.
Other afferents, such as stretch or distension, run with the parasympathetics (vagus).
hindgut derivatives
Supplied by branches of the inferior mesenteric artery
Distal 1/3rd of the transverse colon
Descending colon
Sigmoid colon (rectosigmoid junction at S3)
Rectum
Upper part of anal canal
blood supply of hindgut
arises at L3
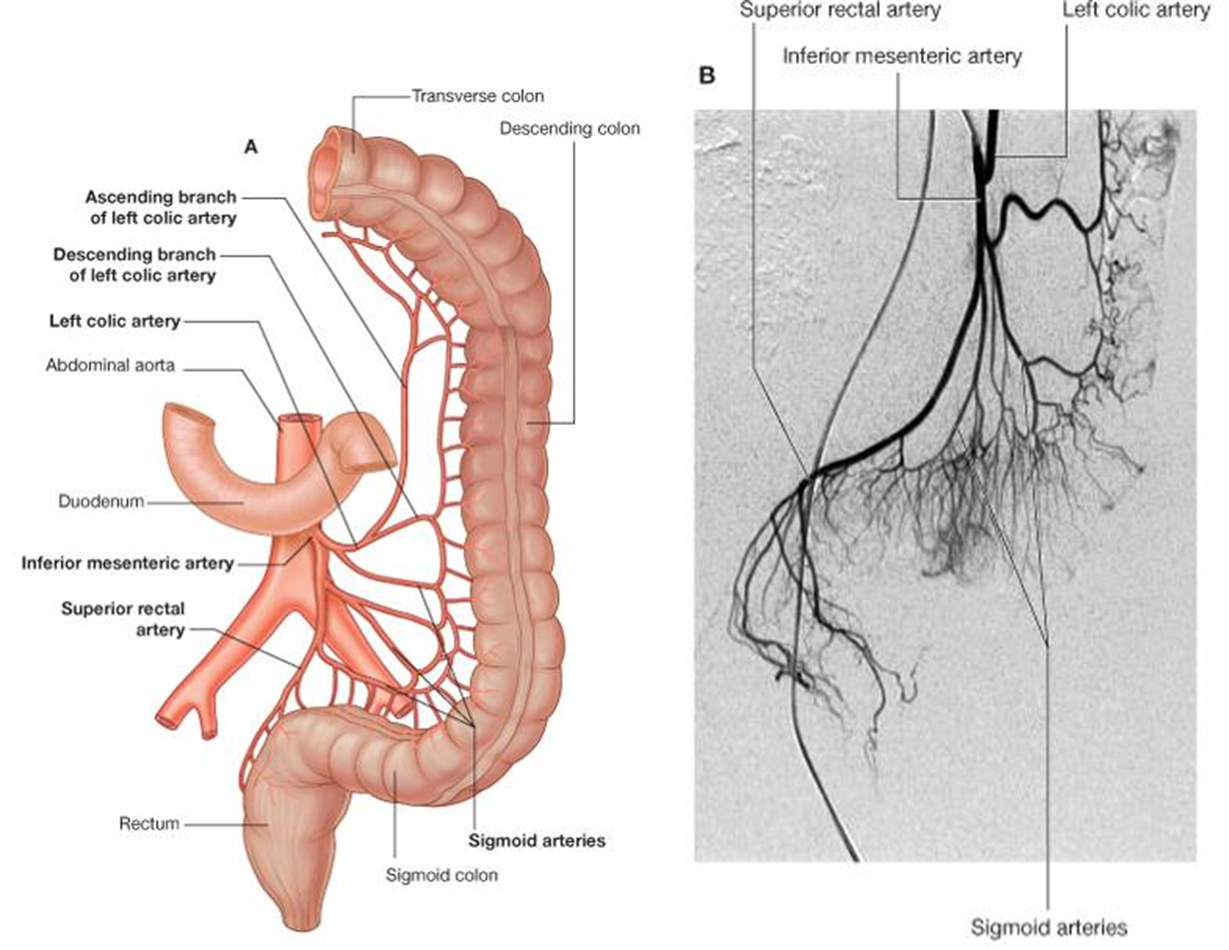
At the left colic flexure, there is an anastomosis between the SMA and IMA.
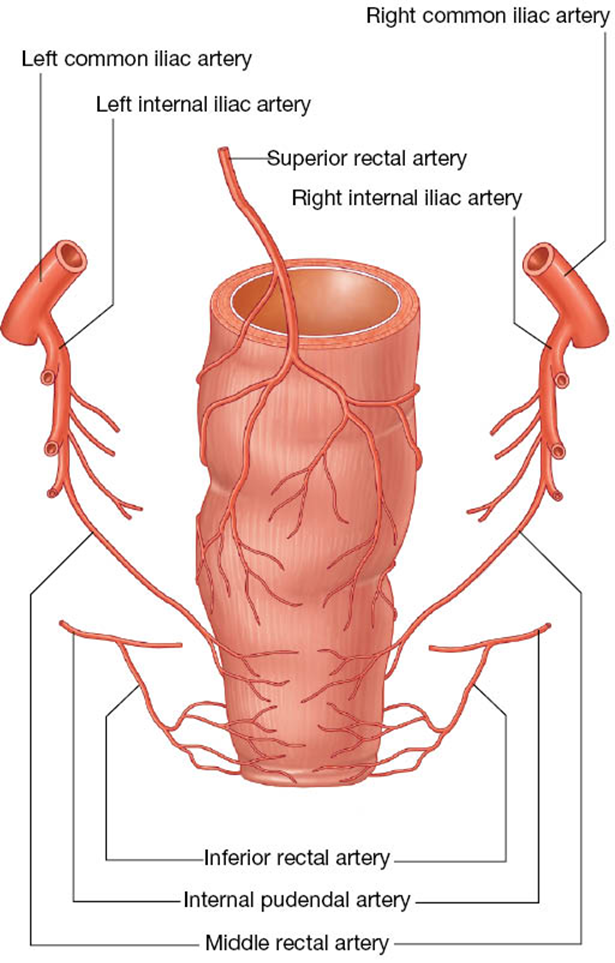
blood supply to rectum & anal canal
Superiorly is the terminal branch of the inferior mesenteric artery, the superior rectal.
The middle portion is supplied by the middle rectal off the internal iliac.
Inferior portion is supplied by the inferior rectal off the internal pudendal artery.
hindgut innervation
Receives sympathetic innervation from spinal cord segments T12-L2 via preganglionic axons in the lesser and lumbar splanchnics that synapse in the inferior mesenteric ganglion. From there, postganglionic sympathetics follow the branches of the inferior mesenteric artery.
Above a line passing through the middle of the sigmoid colon, pain afferents run with the sympathetics.
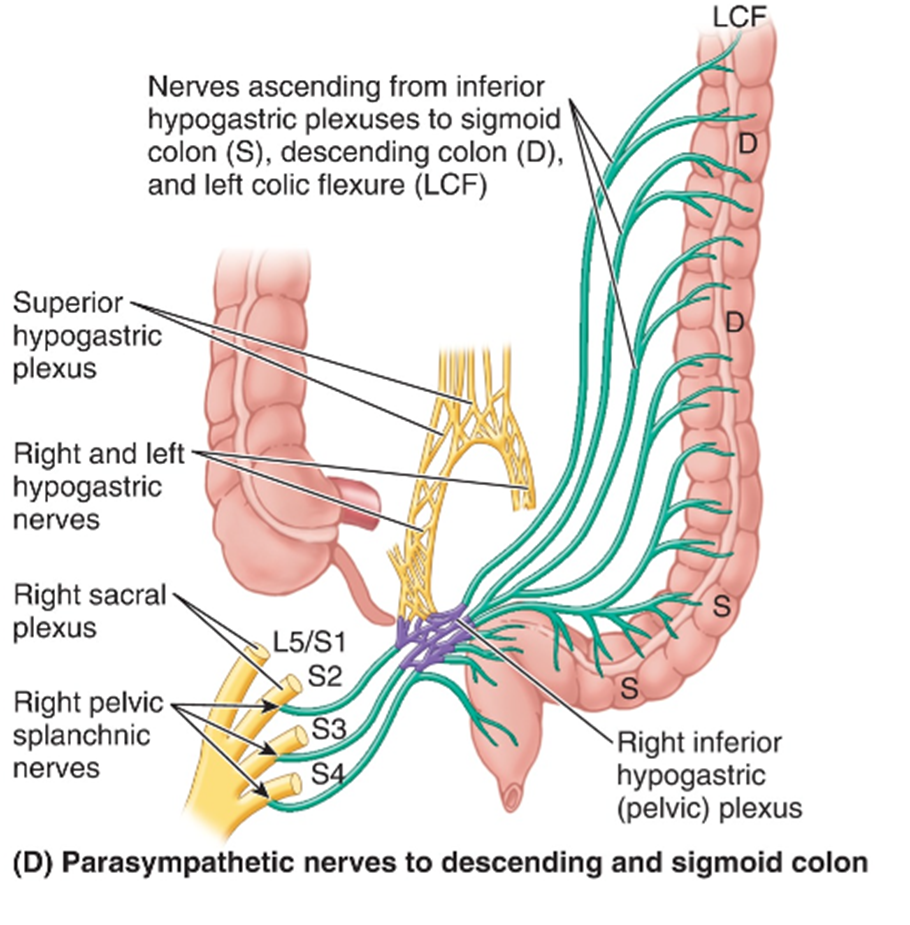
Below a line passing through the middle of the sigmoid colon, all afferents, including pain afferents, travel with parasympathetics to S2-S4.
parasympathetic innervation to the descending colon, sigmoid colon, rectum and upper part of anal canal is via the pelvic splanchnics (S2-S4).
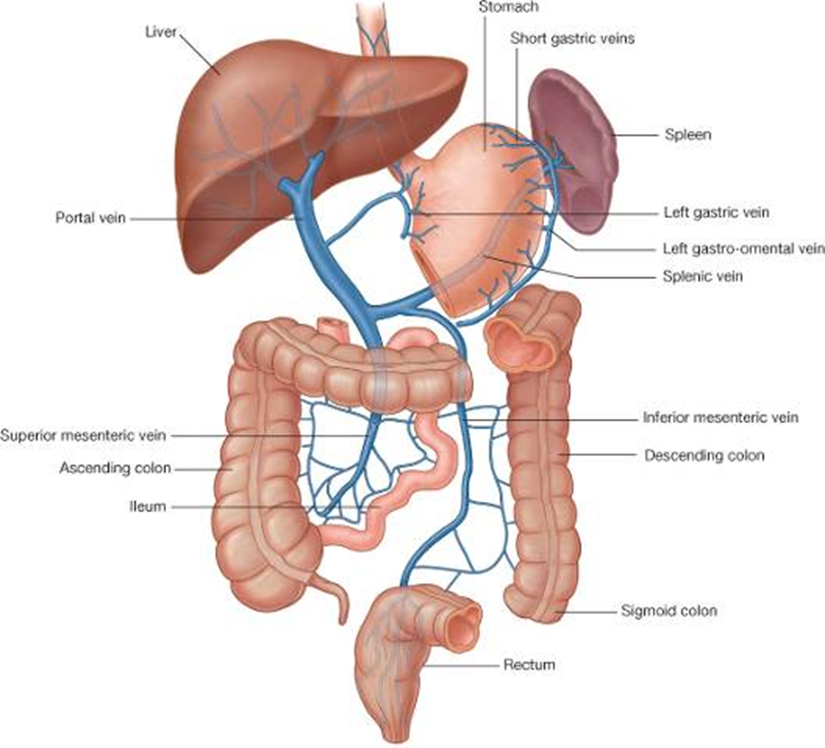
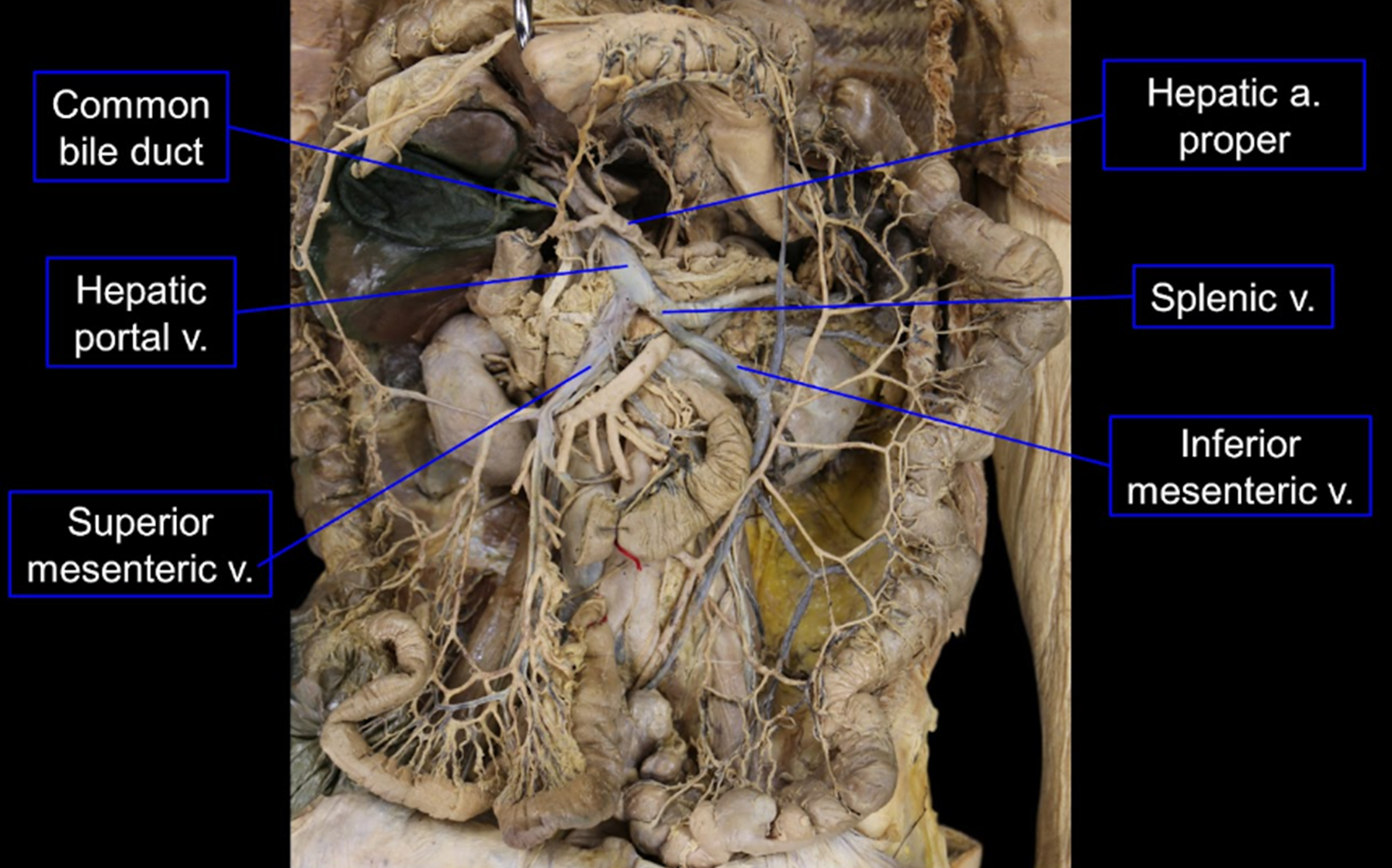
portal vein
Formed when the splenic and superior mesenteric vein join posterior to the neck of the pancreas at the level of the L2 vertebra. It receives all the blood from the GI tract and spleen.
The blood from the kidneys does not drain into the portal vein.
clinical note: portal-caval anastomoses
The anastomoses of the portal venous drainage with the somatic (caval) venous drainage has important clinical significance.
There are 4 sites of anastomosis:
Esophageal veins
Veins of anal canals
Paraumbilical veins
Paracolic
The first and third are often associated with alcohol abuse and cirrhosis.
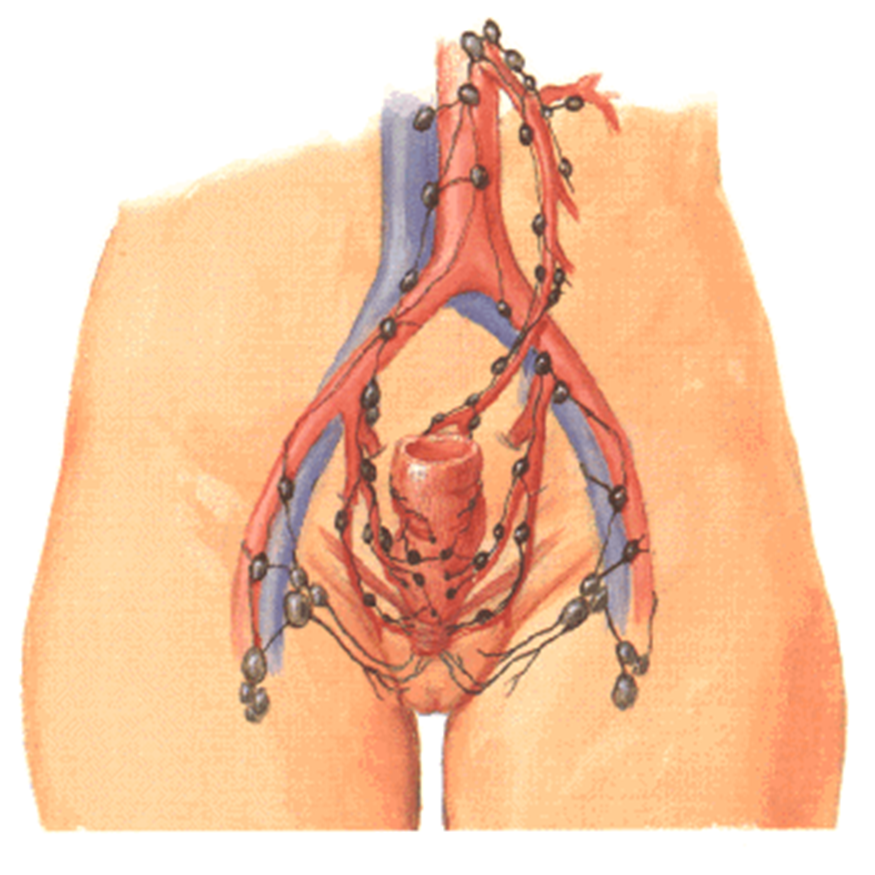
lymphatic drainage
clinical noteL recto-anal watershed
In this region of multiple vascular supply, the lymphatics follow the arteries.
The upper portion of the rectum drains along the route of the inferior mesenteric A.
The middle And lower portions drains back toward the internal iliac arteries.
Below the pectinate line, drainage is to the superficial inguinal nodes.
segmental innervation of GI tract