Module AA- Measurement (Vital Signs)
]]Vital Signs]]
- Shows us how well vital organs are functioning.
- Include temperature, pulse, respiration, and blood pressure
{{Importance{{
- Changes in vital sign measurements can indicate that resident’s condition is worsening
- Can reflect how body is responding to medication and/or treatment
- Report abnormal vital sign immediately to the nurse and per facility policy and per facility policy
- Never guess when taking vitals
{{5th Vital Sign- Pain{{
- Whatever the resident says it is and response to pain varies from resident to resident.
- Other vital signs are objective, while pain is subjective
{{Respiratory System{{
- Involves the breathing in of oxygen and the breathing out of carbon dioxide.
- The left lung has two lobes and three lung has three lobes
Respiration
- The process that supplies oxygen to the cells and removes carbon dioxide from cells
- Involves inspiration and expiration
- Each respiration involves one inspiration and one expiration
- Respiratory rate is the number of inspirations the person takes in one minute. * We count as the chest rises (inspirations)
<<Respiration Values- Abnormal<<
- Bradypnea: Less than 12 breaths per minute
- Tachypnea: more than 20 breaths per minute
- Apnea: no breathing
- Hypoventilation: slow, shallow breathing that may be irregular
- Hyperventilation: rapid, deep breathing
- Dyspnea: painful or difficult breathing
- Cheyne-Stokes: Alternating periods of slow, irregular breathing and rapid, shallow breathing, plus short periods of absent breathing.
- Document and notify nurse
}}Checking Respiration}}
- Equipment * Analog watch * Note pad/assignment sheet and pen
- Analog Watch * When counting respiration for 60 seconds, while watching the second hand, start counting and stop counting on the SAME number.
- Respiration Observation
1. The nurse aide counts respiratory rate for 60 seconds 2. While watching the second hand of an analog watch, the nurse aide starts counting and stops counting on the same number; do not wait until 12 3. Document on the resident’s record if the respirations…
1. Fall between 12-20 2. Regular, quiet, with both sides of chest rising and falling equally. 4. Document on resident’s record and notify the nurse, if respirations are abnormal.
- Stealth Respirations * Check respirations right after checking pulse (without moving hand from wrist), so resident does not realize respirations are being counted; patients tend to change breathing pattern if they are aware that it is being checked.
{{Cardiovascular System{{
- Cardiovascular system: continuous movement of blood through the body.
Structure and Function of the Blood Vessels
- Veins: Blood vessels that carry blood with waste products away from the cells and to the heart.
- Arteries: Blood vessels that carry blood with oxygen and nutrients away from the heart and to the cells.
- Pulse: Is the beat of the heart felt at an artery, as a wave of blood passes through the artery * Pulse rate: The number of heart beats (or pulses) per minute. * Pulse Rhythm: The regularity of the heart beats (pulses) and should be the same interval between beats. * Pulse force: The strength of the pulse and should be easy to feel.
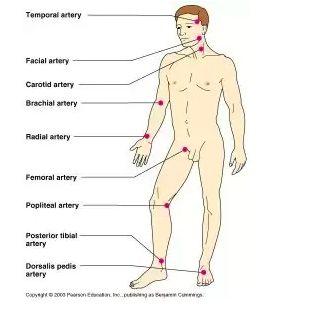
}}Pulse Sites}}
- Temporal
- Carotid: never check pulse rates on both carotid arteries at the same time
- Apical: Over the heart, taken with a stethoscope
- Brachial: typically used during BP checks
- Radial: used most often, easy to reach, easy to find, used for routine vital signs * Typically used to take pulse during during routine vital signs checks * Does not expose resident * Located on the thumb side of the wrist * Use first two or three fingers; NEVER thumb
- Pedal: used to check circulation of the leg
<<Pulse Values<<
- Normal pulse for adults (document) * Rate between 60-100 beats per minute * Regular, and strong
- Abnormal pulse for adults (document and notify nurse) * Bradycardia: less than 60 beats per minute * Tachycardia: more than 100 beats per minute * Irregular pulse rhythm * Weak in strength
}}Counting Pulse}}
- Analog watch * When counting pulse for 60 seconds, while watching the second hand, start counting and stop counting on the same number. * Document on the resident’s record if the pulse falls within the range of 60-100 and is regular and strong * Document and notify nurse, if it is abnormal
- Notepad/assignment sheet and pen
Structure and Function of the Heart
- The pump of the circulatory system
- Consists of four chambers (right and left atria, right and left ventricles)
- Has two phases * Systole: The working phase of the heart when the heart is pumping blood to the body; the top number of a blood pressure reading. * Diastole: The resting phase of the heart when the heart fills with blood; the bottom number of a blood pressure reading (diastolic
Blood Pressure
- Blood Pressure: The amount of force exerted by the blood against the walls of the artery.
- Shows how well the heart is working
- Can change minute to minute depending on: * The activity of the resident (for position, BP is higher lying in bed than seated in chair or standing; for exercising, BP increases) * Lifestyle choices (BP increases with smoking and drinking; BP higher if resident is overweight and decreases as weight is lost; BP may be high if resident eats a high salt diet) * Reaction to stressful events (BP increases with anxiety, emotional responses, and stress) * Acute injury or emergency (a blood volume decrease from injury will decrease BP; BP increases with pain) * Medications (raises or lowers BP depending on the medication)
- Genetic factors affect blood pressure: * Age (BP increases with age) * Gender (women’s BP usually lower) * Race (black residents BP higher than white
- Blood Pressure Site * The brachial artery and the upper arm are sites most often used by nurse aide when checking blood pressure
- %%The blood pressure Value%% * Measured in mm Hg * Recorded in a fraction * Normal Blood Pressure ranges of adult * Systolic (top number): 90 mm Hg to 119 mm Hg * Diastolic (bottom number): 60 mm Hg to 79 mm Hg * Document on record * Abnormal Blood Pressure Values * Elevated blood pressure ranges (likely to develop high blood pressure unless steps are taken to control the blood pressure) * Systolic: 120 mm Hg to 129 mm Hg @@AND@@ * Diastolic: below 80 mm Hg * Hypertension: consistent elevated systolic or diastolic values * Systolic: 130 mm Hg or higher OR * Diastolic: 80 mm Hg or higher * Hypotension: too low systolic and/or diastolic values * Systolic: less than 90 mm Hg * Diastolic: less than 60 mm Hg * Always document on the record and report abnormal blood pressures to nurse
- The nurse aide uses three senses simultaneously when checking a resident’s blood pressure: * Seeing: watches the needle’s movement in relation to the numbers on the manometer * Hearing: using the stethoscope, listens for sounds indicating changes in blood flow in the brachial artery * Touching: controls the inflation and deflation of the cuff using the thumb and index finger
- Checking Blood Pressure * Stethoscope * Sphygmomanometer: BP cuff * Alcohol wipes * Note pad/assignment sheet and pen
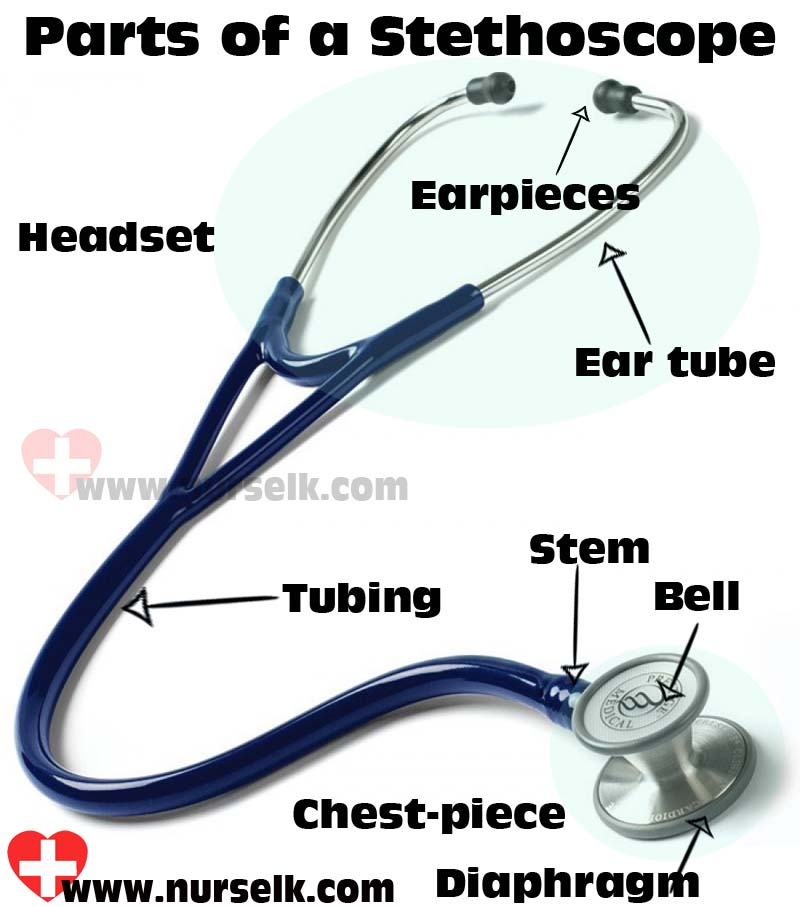
- Stethoscope
* Used to listen to brachial artery
* May be single-head (with diaphragm only) or dual-head (with diaphragm and bell)
* Parts
* Ear pieces
* Binaurals
* Rubber or plastic tubing
* Chest-piece (with diaphragm or diaphragm/bell)
* Ear Pieces
* To prevent infection, always clean before and after use with an alcohol wipe
* Insert ear pieces into ears so that they point forward toward the nose
* Should snugly fit in ears to block out noise.
* Dual-head Stethoscope- Diaphragm
* Before using dual-head stethoscope to take blood pressure, determine which side of chest-piece is active
* To check blood pressure, diaphragm needs to be active
* Two Ways to Check for an Active Diaphragm
* After inserting ear pieces into ears, tap diaphragm lightly to determine if tap is heard; if tap not heard, rotate chest piece at tubing, and repeat the tap
* If chest piece has an indicator dot, rotate chest-piece so indicator dot is closed
* Diaphragm Concepts
* To prevent infection, always clean before use, between residents, and after use with an alcohol wipe
* Warm diaphragm with hand before making contact with resident
* To use diaphragm, apply enough pressure to make a seal against the brachial artery at the crook of the elbow
*
- BP Cuff * Two types * Manual (aneroid) * Electronic (digital) * Aneroid BP Cuff- Parts * Manometer * Cuff with bladder * Inflation bulb with air-release valve * Tube from cuff to manometer * Tube from cuff to the handheld inflation bulb * Manometer * Marked with long and short lines and has a needle * the long lines mark 10 mm Hg * The short lines mark 2 mm Hg * Watch the needle as the cuff inflate while listening for sounds through stethoscope * If needle lands between two dashes, the number is rounded up to the next dash. * Odd numbers are not recorded when using a manual BP cuff * When checking a blood pressure, you will be watching the needle as it drops from a higher number to a lower number, so you will be counting backwards * Cuff * After wrapping the cuff around the bare upper arm * the cuff inflates and puts pressure on the brachial artery * As cuff deflates, BP is determined. * Comes in child size (7-9 inches) and regular (9-13 inches), and extra large (13-17 inches) * Important to choose the correct size because a too big or too small cuff can impact accuracy of reading. * Typically has 1 or 2 arrows (left arm/right arm) on cuff which align with brachial artery * Cuff positioned/wrapped at least an inch above the elbow * Cuff or stethoscope should not be placed over clothing * \
- Tubing * Made of rubber
- Inflation Bulb with the Air-release Valve * To inflate cuff, turn air-release valve clockwise to close valve; then squeeze the bulb; remember thumb goes up, needle goes up * To deflate cuff and open valve, turn air release valve counterclockwise with the thumb and index finger in a slow and controlled manner, remember thumb goes down, needle goes down. * Inflate cuff to between 160 mm Hg to 180 mm Hg * If a beat is heard immediately, deflate the cuff; wait 30-60 seconds; inflate cuff to no more than 200 mm Hg.
- Nevers * Do not take blood pressure on an arm with an IV, dialysis shunt, or other medical device in place * Avoid taking blood pressure on a side that has been injured or burned, is paralyzed, has a cast or had a mastectomy
- Orthostatic Hypotension * Abnormal low blood pressure occurring when the resident suddenly stands up; resident complains of weakness, faintness, dizziness, and seeing spots * May be a complication from bed rest * Nurse aide may be asked to take an orthostatic blood pressure measurement; process includes; * BP checked while laying down, record in note pad * Have resident sit up, wait two minutes, check BP, record in notepad * Have resident stand up, wait 2 minutes, check BP, record in notepad * Record and report findings to nurse * Throughout process, nurse aide should check to see if resident is feeling weak, dizzy, faint, or seeing spots * Prevention * Per care plan and directive from nurse * Increase activity in stages: bed rest then sitting on side of bed (dangling) then walking * Before standing, while sitting on side of bed (dangling), have resident cough/deep breathe and move legs back-and-forth in circles, 1 to 5 minutes * Ask resident to report weakness, dizziness, faintness, or seeing spots. * May need two people if resident has an inability to stand
Body Temperature
- How much heat is in the body and balances the heat created by the body and heat lost to the environment.
- Is typically stable
- Produced: created in the body when cells use food for energy
- Lost to the environment through skin, breathing, urine, and stool
- Terminology * Fever: an elevated temperature * Febrile: with a fever * Afrebile: without a fever * Thermometer: device used to measure body temperature * Fahrenheit and Centigrade: scales used to measure temperature; stated in degrees
- Factors Affecting Temperature * Age (older lower temperature than younger) * Illness (typically increases with infection) * Stress (causes an increase) * Environment (dependent upon humidity and temperature) * Exercise (causes an increase) * Time of day (lowest in the morning; higher in afternoon and evening)
- Sites * Important to check with nurse or care plan to see what type of thermometer is used * Mouth (oral) * Rectum (rectal): most accurate; never let go of rectal thermometer while checking temperature * Armpit (axilla): least accurate * Ear (tympanic) * Temporal artery (forehead)
- When to NOT take oral temperature * Is unconscious * Recent facial or mouth surgery * Recent injury to face * Has sores, redness, or mouth pain * Is confused or agitated * History of seizure * Is using oxygen * Is a mouth breather * Has a feeding tube
- When to NOT Take a Rectal Temperature * Has Diarrhea * Has rectal problem * Has heart disease * Recent rectal surgery * Is confused or agitated
- Temperature Values * Oral * Baseline- 98.6 F * Normal Range: 97.6-99.6 F * Rectal * Baseline- 99.6 F * Normal Range- 98.6-100.6 F * Axillary * Baseline- 97.6 F * Normal range- 96.6-98.6 F * Tympanic Membrane * Baseline- 98.6 * Normal Range- 97.6-99.6 F * Temporal * Baseline- 98.6 F * Normal Range- 97.6-99.6 F
- Types of Thermometers * Digital: oral, rectal, axillary * Electronic: oral, rectal, axillary * Tympanic: ear * Temporal: forehead * Non-mercury, liquid-filled glass (oral- green tipped) * Non-mercury, liquid-filled glass (rectal- red tipped)
- Digital Thermometer * Oral, rectal, or axillary * Display results digitally and is quick, within 2-60 seconds, and beeps or flashes when done * Battery-operated * Requires a disposable sheath
- Electronic Thermometer * Oral, rectal, or axillary * Have oral (blue tipped) and rectal (red tipped) probes; for axillary temperature use oral (blue tipped) thermometer * Displays results digitally and is quick, within 2-60 seconds, and beeps or flashes when done * Battery-operated and stored in recharging device * Requires a probe cover
- Tympanic Thermometer * Ear * Registers temperature in seconds * May need practice to operate accurately
- Temporal Thermometer * Measures heat from skin over the forehead, specifically over temporal atery * Done by a stroke or scan over the area * Registers within 3 seconds * Noninvasive
- Non-mercury, Liquid-filled Glass Thermometers- Equipment * Thermometer * Sheath * Gloves * Watch * Pen * Notepad * alcohol wipe * Water soluble lubricant (rectal temperature only)
- Non-mercury, Liquid-filled Glass Thermometers * Oral, rectal, or axillary * Color-coded * Either blue or green for oral * Red for rectal * Takes a long time to register- 3 to 10 minutes based on site * Held at the stem of the thermometer and read at eye level * The nurse aide must read the thermometer after it registers the temperature; held at stem; read at eye level * Most health care providers use the Fahrenheit scale to measure temperature, even though both Fahrenheit and Celsius values are typically seen on thermometer
- Reading the Non-mercury, Liquid-filled Glass Thermometer * For Fahrenheit readings: * the long line represents 1 degree * The short line represents two tenths (2/10) of a degree
\