Sleep Apnea and Neuromuscular Respiratory Disorders
sleep apnoea syndrome - upper airway obstruction leading to apnoea during sleep
stopping breathing is apnoea
associated with heavily snoring
•Nocturnal polyuria when you wake up a lot in the night to pee
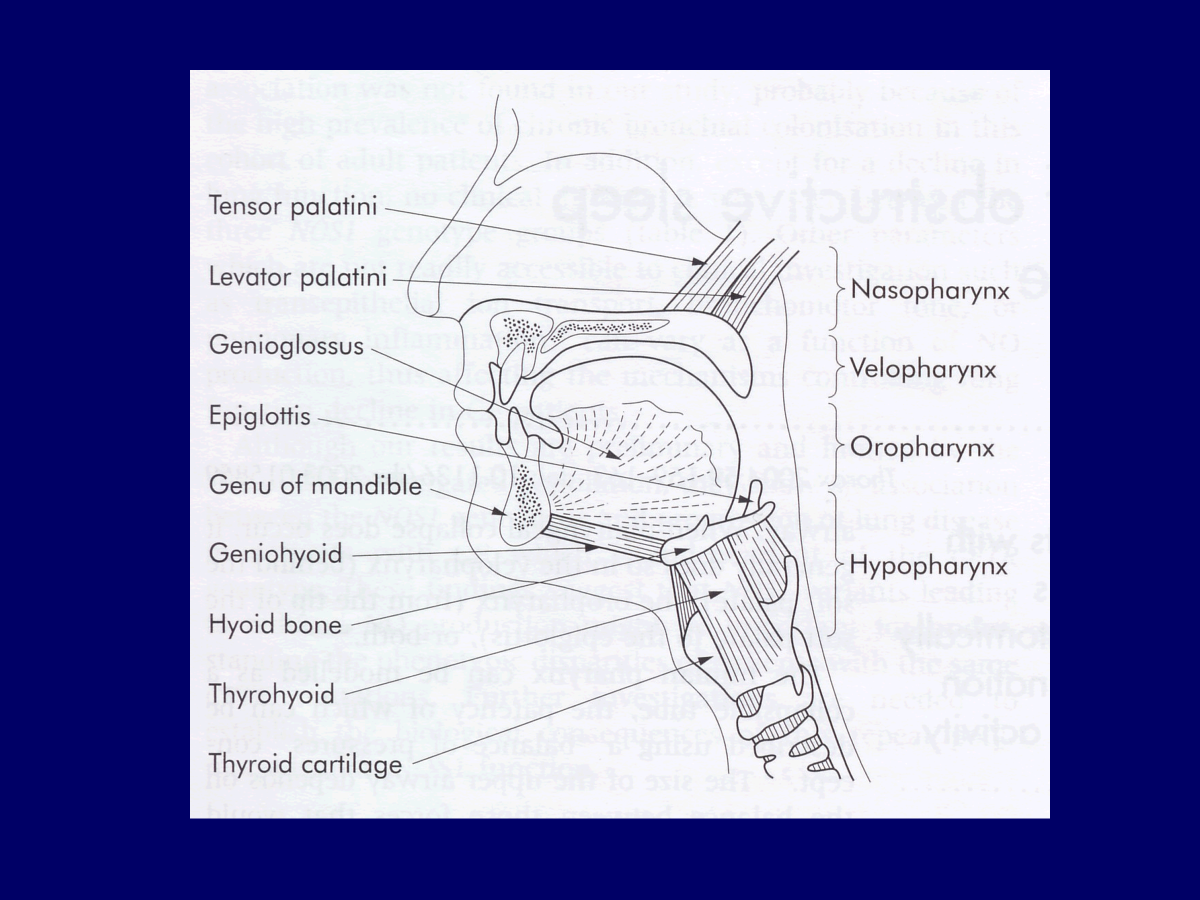
muscle in pharyngeal wall that can activate and open the throat if it closes off
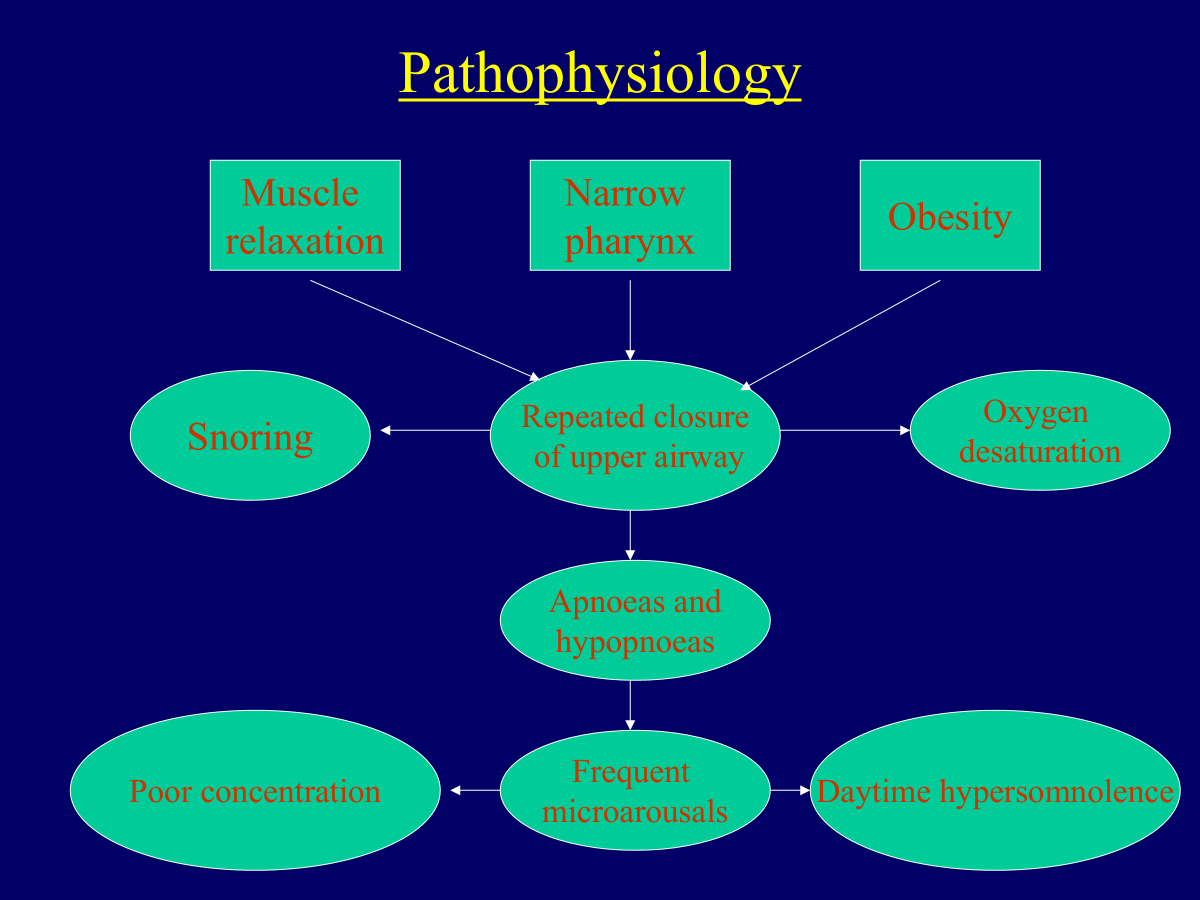
sleep apnoea combination of muscle relaxation, narrow pharynx, obesity
all pharyngeal muscles become relaxed
2% of adult men, 1% adult women
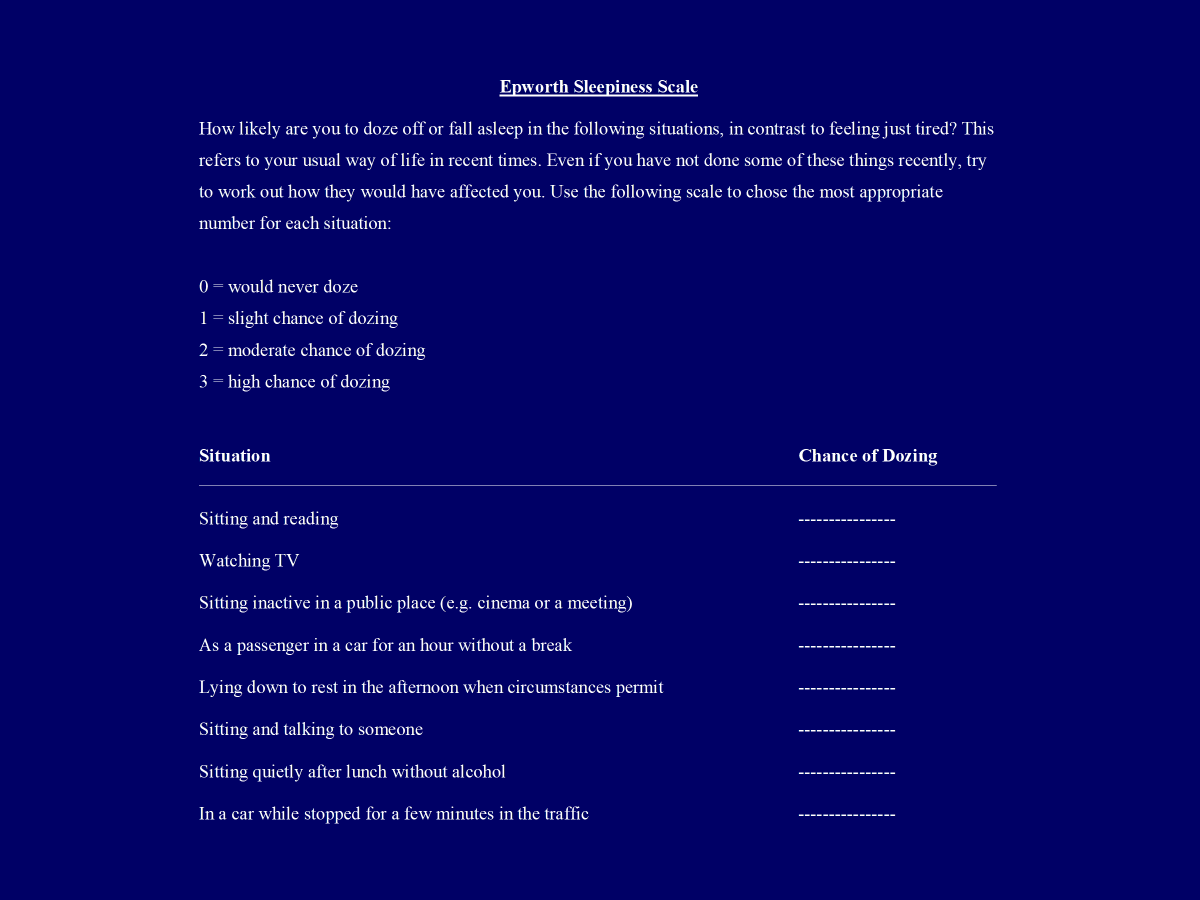
diagnosed by -clinical history and examination
-epworth questionnaire
-overnight sleep study → pulse oximetry (O2 sats and pulse rate overnight)
→limited sleep studies
→full polysomnography
polysomnography most sophisticated study
electroesephonogram (EEG)
includes light sleep, REM sleep, deep sleep
severity of OSA
0-5 normal
5-15 mild
15-30 moderate
>30 severe
desaturation rate/AHI
Treatment
weight reduction, alcohol avoidance, diagnose and treat endocrine disorders (which mostly present in sleep apnoea) e.g. hypothyroidism, acromegaly
continuous positive airways pressure (CPAP) *main treatment - like breathing device in night
mandibular repositioning splint - guard in mouth, brings lower jaw forward, advances jaw as much as you want
positional therapy devices - stops them sleeping on their back, some only get sleep apnoea on their back
Narcolepsy
•Associated with HLA - DRB1*1501 and HLA DQB1* 0602
with a specific haplotype, gene that codes for mite cell antigens?
cataplexy, laughing or crying might induce cataplexic attack, can be confused with fainting, not everyone has cataplexia with narcolepsy
excessive daytime somnolence
hypnagogic- just about to sleep and hallucinate or hear voices, hynopompic hallucinations - just coming around from sleep
sleep paralysis- seeing something in the room and can’t move
Sleep Onset Rem Sleep (SOREM)
rem sleep is the state which we dream, rapid eye movement
narcolepsy go straight into rem sleep, all skeletal muscles paralysed, explains why they get hyponogic and paralysis
PSG -polysonograpahy to diagnose
can also sample CSF, if orexin low in CSF, feature of narcolepsy
Treatment
-modafinil
-dexamphetamine
-venlafaxine (for cataplexy)
-sodium oxybate (xyrem), can be used for sleepiness and cataplexy
Chronic Ventilatory Failure
also called chronic type 2 respiratory failure
elevated pCO2 >6.0 kPa (high)
pO2 <8kPa (low)
normal blood pH
(unlike acute ventilatory failure where body hasn’t compensated, compensation here leads to normal pH)
elevated bicarbonate, how body compensates (HCO3-)
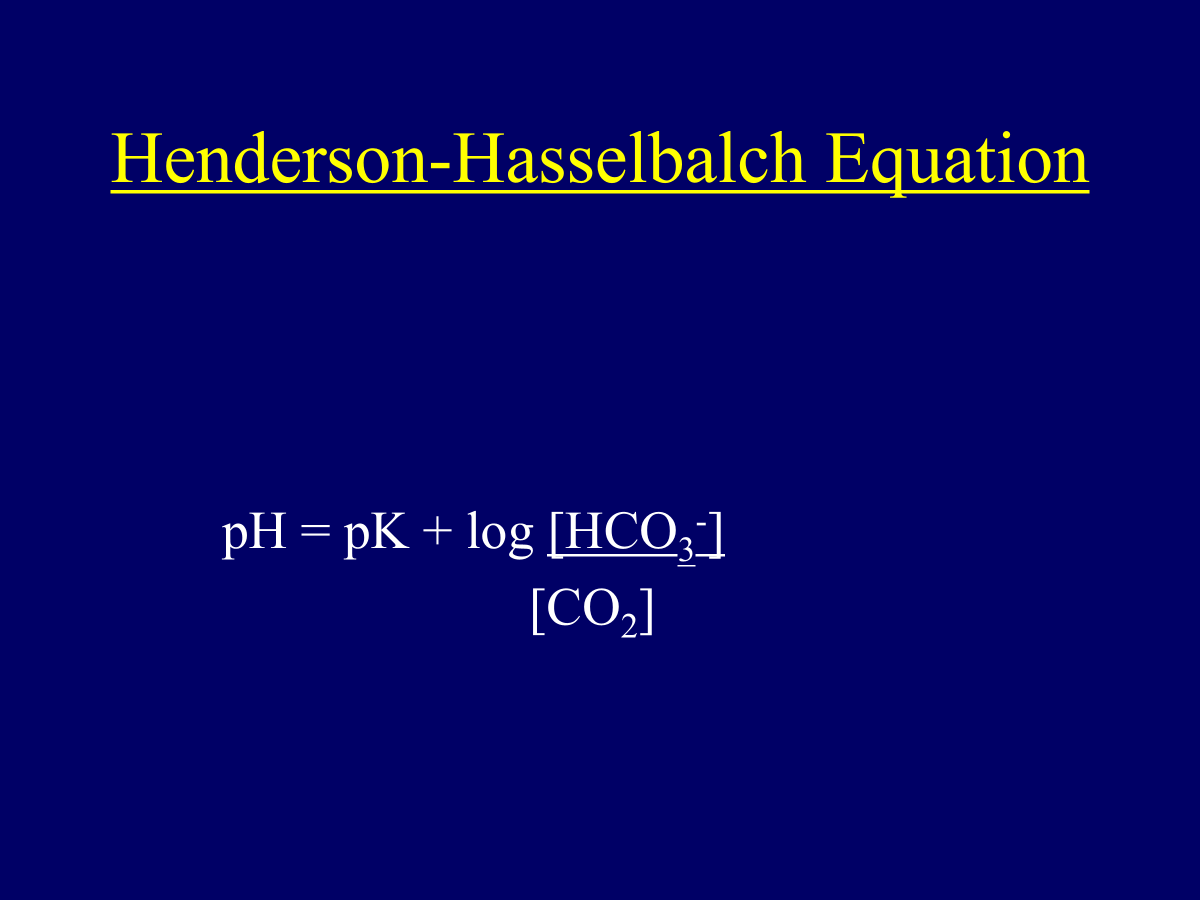
pK a constant
in order to maintain normal pH body compensated by retaining carbonate, leading to rise of bicarbonate in blood, hence turning this ratio back to normal
most people with COPD DON’T have chronic ventilatory failure but a chronic proportion of the spectrum do
symptoms depend on the condition causing the CVF
orthopnoea is breathlessness lying flat, if weakness of diaphragm when you lie flat no gravity to help muscle descend and abdominal organs pushing on it making it difficult for diaphragm to descend causing people to feel breathless lying flat
morning headache because vasodilation of brain vessels? CO2 too much
PI max is maximum inspiratory pressure
PE max is maximum expiratory pressure