Integumentary Full
Integumentary System and Skin Trauma
Epidermis: prevents water loss and phagocytosis
Definition of Pressure Injuries
Localized tissue destruction caused by lasting compression of soft tissue over bony prominences for a prolonged period of time.
Examples of Bony Prominences:
Nose
Ears
Back of the head
Elbows
Ankles
Hip (greater trochanter)
Consequences of Pressure Injuries:
Infection
Loss of function
Pain
Terminology:
Bed sore, decubitus ulcer, pressure sore
Risk Factors for Pressure Injuries
Incontinence
Poor nutrition
Friction and shear
Immobility
Caused by lying in one position for too long.
Shearing Forces:
Tissue layers sliding over one another, common in repositioning.
Common Areas for Pressure Injuries
Heels, sacrum, greater trochanter, elbows, ears, back of the head
Incidence in hospitals: approximately 8%
Incidence in long-term care: 2.4% - 23%
Deaths from complications: 60,000 yearly
Annual costs for treatment: $11 billion
Medicare/Medicaid will not reimbursement for pressure injuries acquired during hospital stay.
Stages of Pressure Injuries
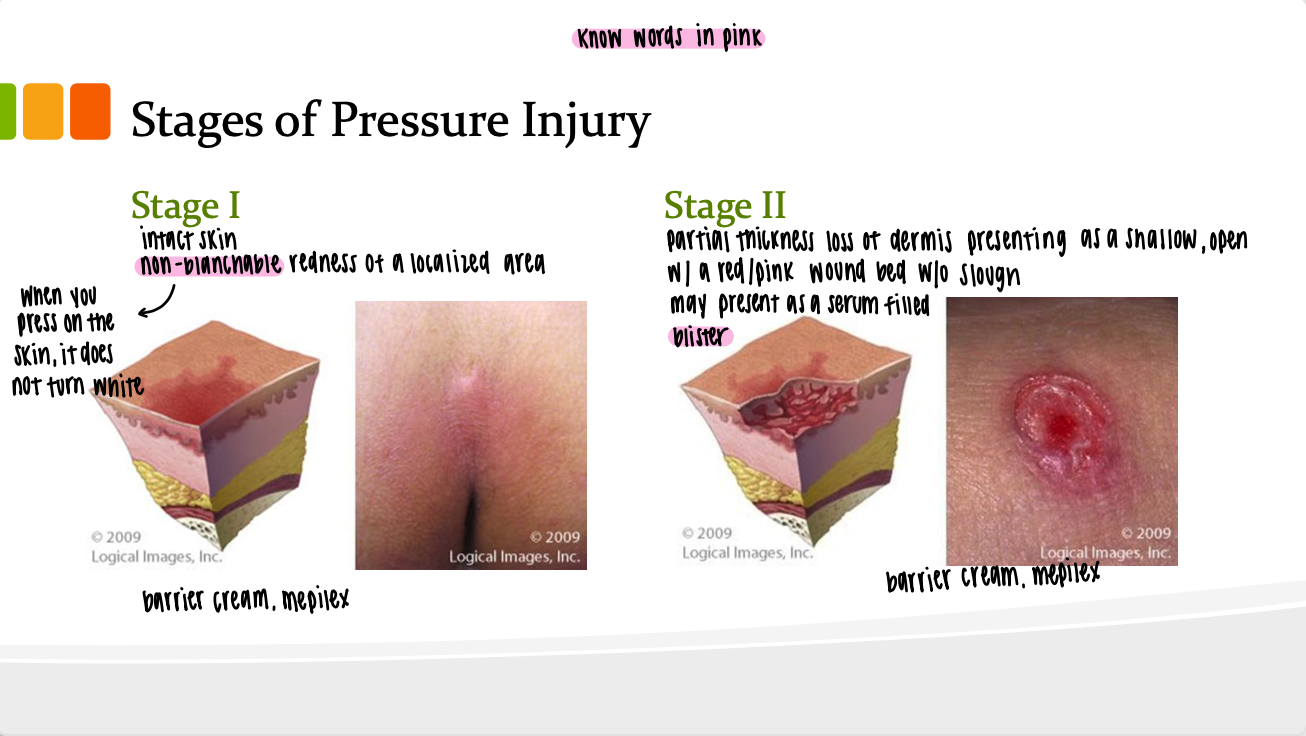
Stage 1:
Intact skin with non-blanchable redness in a localized area.
May be painful, firm, soft, and warm/cool compared to adjacent tissue.
Dark pigmented skin may not show visible blanching.
Treatment
Barrier Cream, Mepilex
Stage 2:
Partial loss of dermis, appearing as a shallow open ulcer with red/pink wound bed without slough. May present as intact or ruptured serum-filled blister.
Non-inclusion of: skin tears, tape burns, maceration, or excoriation.
Treatment
Barrier Cream, Mepilex
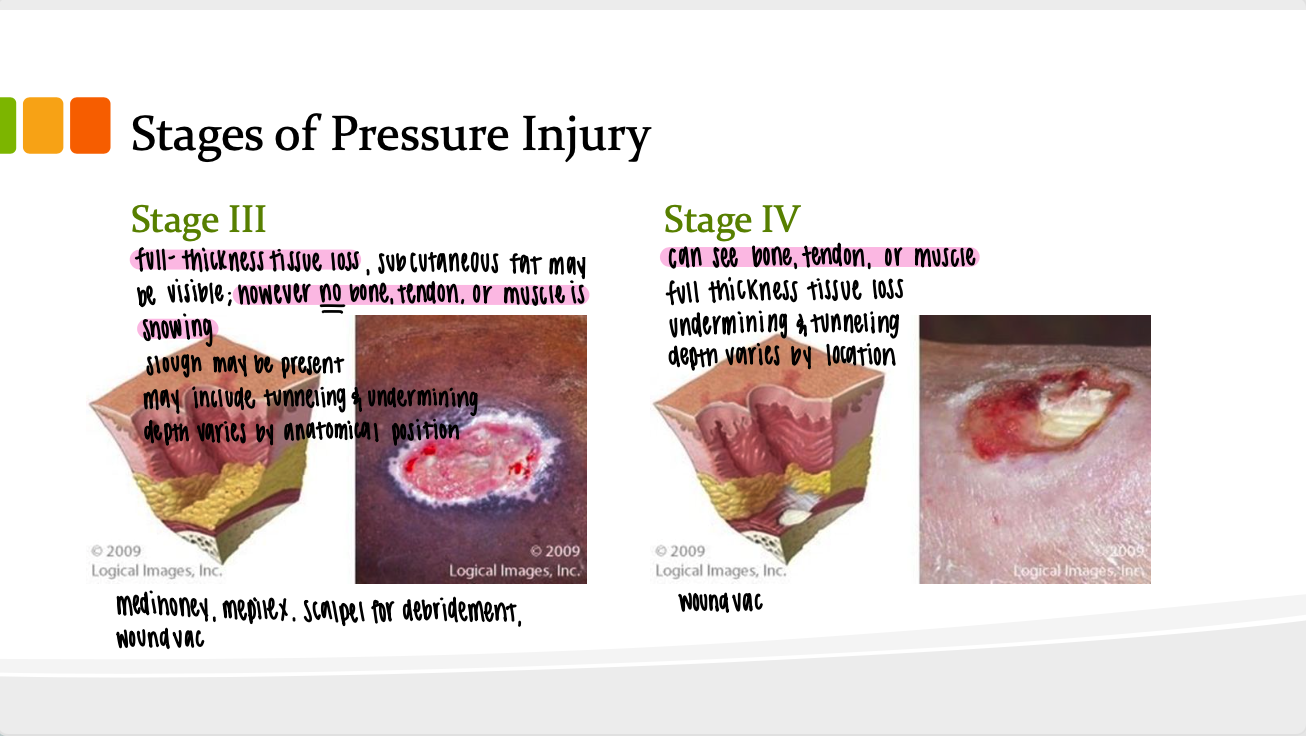
Stage 3:
Full thickness tissue loss: subcutaneous fat may be visible. Muscle, bone, or tendon is not exposed. Slough may very well present as a yellow or white mucus that can complicate healing and may require debridement to promote granulation.
May include undermining and tunneling. Depth can vary.
Treatment:
medihoney, mepilex, scalpel for debridement, wound vac.
Stage 4:
Full thickness tissue loss with exposed bone, tendon, or muscle.
Often includes undermining and tunneling. Depth varies by location.
Treatment:
wound vac.
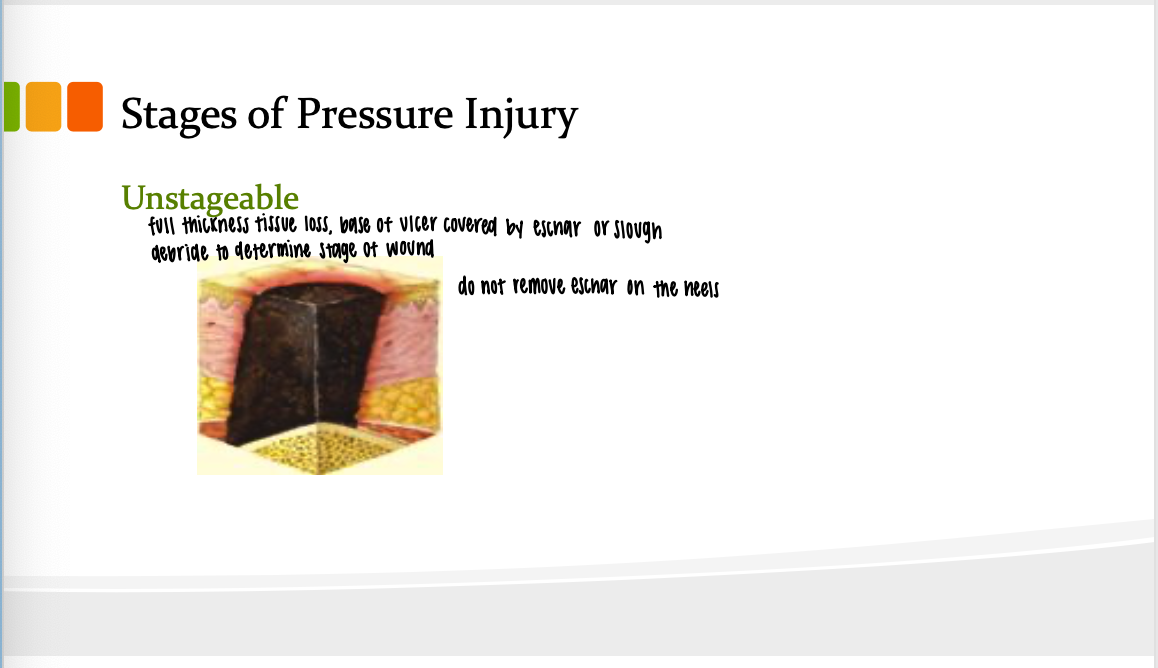
Stage 6: Unstageable Pressure Injury:
Full thickness tissue loss with slough/eschar covering the wound base.
Cannot determine stage until slough/eschar is removed.
Do not remove eschar on heels as it acts as a biological cover.
Undermining vs. Tunneling:
Undermining is below the surface of the wound; tunneling goes deeper into subcutaneous tissue.
Risk Assessment Tool: Braden Scale
Assesses sensory perception, moisture, activity, mobility, nutrition, and friction/shear.
Lower numbers signify higher risk for pressure ulcer formation.
Interventions for Prevention of Pressure Injuries
Maintain hydration of the skin
Incontinence care
Use lifting sheets
Maintain head of bed at 30 degrees or lower to reduce sliding.
Reduce pressure through special beds (e.g., air fluid support).
Avoid rings, donuts, and sheep skins.
Turn patients every two hours; hourly repositioning for those in chair.
Relieve pressure under heels using pillows and cushioning devices.
Encourage a high-protein diet.
Nursing Management of Patients with Pressure Ulcers
Assess for complications (fistulas, abscesses, osteomyelitis, bacteremia, cellulitis).
Monitor ulcers daily for progress and management of pain.
Use appropriate dressings and perform debridement as needed.
Documentation Requirements:
Location, stage, dimensions, presence of tunneling/undermining, condition of wound bed (slough, eschar, odor).
Types of Debridement
Mechanical Debridement
Involves wet-to-dry dressings.
Example: Pack with saline-soaked gauze (4x4s) and cover with dry dressings.
Pros: Debrides necrotic tissue.
Cons: Healthy tissue may be removed; their use can prolong healing time.
Autolytic Debridement: own digestive enzymes to breakdown necrotic tissue
Utilizes a semi-occlusive transparent film or hydrocolloids.
Creates a moist environment, enabling body’s enzymes to break down necrotic tissue.
Products like "Duoderm" and "MetaHoney" often used.
New products regularly emerge; focus on understanding the types over brand names.
Enzymatic Debridement
Uses proteolytic enzymes or specific dressings to break down necrotic tissue effectively.
Sharp Debridement
Involves the use of scalpels or lasers to remove necrotic tissue.
Notably the most effective and quickest method.
Biological Debridement
Historically utilized maggots for debridement; known as maggot therapy.
Maggots are bred specifically for medical use.
Video reference for historical context, but not commonly practiced today.
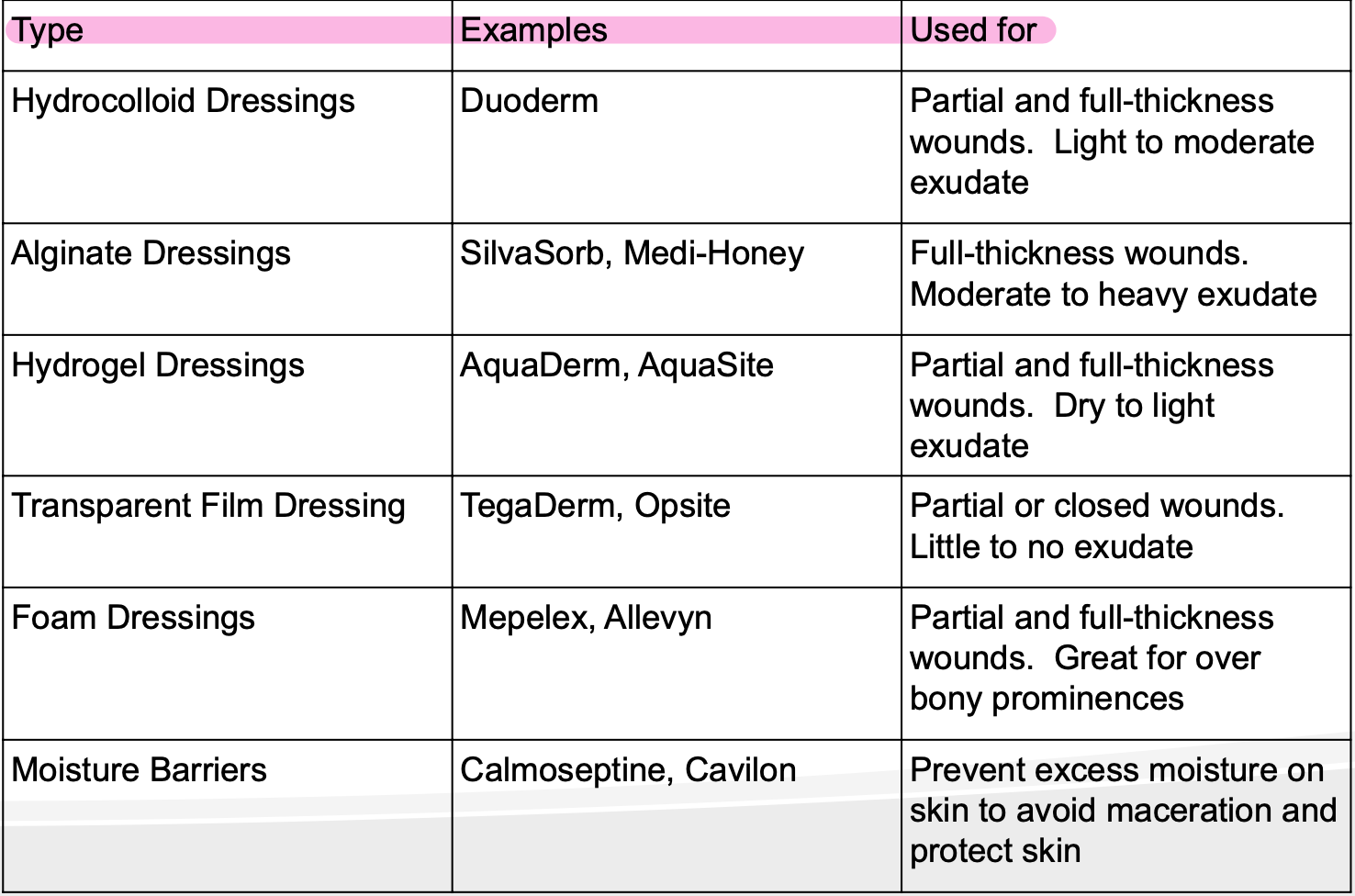
Products for Treating Pressure Injuries
Hydrocolloid Dressings
Water impermeable, with a polyurethane outer layer separating the wound from a hydrocolloid material.
Functions: Absorbs moisture (softens and discolors), promotes autolysis, reduces infection risk, protects the wound, and aids healing.
Easy to use, can be removed without damage, suitable for partial and full thickness wounds.
Available as sheets and gels, changes recommended regularly depending on exudate.
Alginate Dressings
Derived from algae/kelp; absorbent calcium alginate fibers.
Best for moderate to highly exudative wounds like pressure injuries and venous ulcers.
Hydrogel Dressings
Available as impregnated sheets or gels; maintain moisture in the wound bed.
Comfortable, soothing for painful wounds; requires a secondary dressing to secure.
Ideal for partial/full thickness dry to lightly exudative wounds (e.g., necrotic wounds, minor/radiation burns).
Transparent Film Dressings
Products: "Tegaderm" or "Opsite"; allow moisture vapor and oxygen in, but block water/liquids/bacteria.
Used for closed or partially open wounds (e.g., IV sites, skin donor sites).
Vacuum-Assisted Closure (VAC) Systems
Examples: wound vax, Prevena, and PICO.
Designed for draining large amounts of exudate from deep wounds.
Prevena is for shallower wounds, often identifiable by its purple color.
PICO resembles Prevena but comes in a different design.
Skin Trauma: Frostbite
Definition: Injury of skin from freezing, primarily affects extremities (fingers, toes, nose, ears).
Initial vasoconstriction leads to blood vessel dilation, causing swelling.
Continued exposure can lead to necrosis; treatment can include debridement of blisters.
Manifestations:
Superficial Frostbite: Symptoms include numbness, itching, skin changes (cyanosis, redness, white).
Deeper Frostbite: Stiffness, pain, edema, blisters, and gangrene appearance possible.
Treatment Strategy:
Rewarming affected area (preferably in warm water).
Avoid massaging the area to prevent cell destruction.
Bed rest with elevation of affected parts, pain relief, and anti-inflammatory medications.
Summary: Understanding various types of debridement and wound dressings is essential for effective treatment of wounds and pressure injuries, while also recognizing the serious implications of frostbite injury and its treatments.
Functions of the Skin
Largest organ system of the body
Barrier Formation: Protects internal environment from external threats.
Defense Mechanism: Protects body from pathogens.
Temperature Regulation: Maintains body temperature and water balance.
Sensory Input: Provides sensory information about the environment.
Age-Related Changes to the Skin
Children
Decreased subcutaneous fat.
Epidermis loosely attached to dermis.
Thinner
Vessels closer to surface
more water
less pigmented
Older Adults
Increased skin pallor. (paleness)
Progressive wrinkling.
Thinner, drier skin.
Vessels closer to surface, leading to fragile skin.
Decreased perspiration, reduced pigmentation.
Assessment Process
Assessment Components:
Health history.
Physical assessment: check color, temperature, hydration, integrity, and odor.
Use Braden Scale to assess risk for pressure ulcers.
Nursing Concerns
Impaired skin integrity.
Acute pain.
Risk for infection.
Disturbed body image.
Risk for fluid volume deficit.
Altered nutrition.
Diagnostic Tests
Complete Blood Count (CBC): Evaluates overall health.
Erythrocyte Sedimentation Rate (ESR): Indicates inflammation.
Biopsy: Assesses skin lesions.
Culture Exudate: Identifies organisms causing infection.
Potassium Hydroxide Prep: “wet prep”, looking for yeast. Tests for fungal infections.
Skin Testing: Assesses for allergies and inflammation.
Skin Trauma Types
Pressure Injury: Damage to skin from prolonged pressure.
Frostbite: Ice crystal formation in skin leading to damage.
Braden Scale for Predicting Pressure Ulcer Risk
Sensory Perception: Ability to respond to pressure-related discomfort.
Completely Limited
Very Limited
Slightly Limited
No Impairment
Moisture: Degree to which skin is exposed to moisture.
Constantly Moist
Very Moist
Occasionally Moist
Rarely Moist
Activity: Physical activity level.
Bedfast
Chairfast
Walks Occasionally
Walks Frequently
Mobility: Ability to change position.
Completely Immobile
Very Limited
Slightly Limited
No Limitation
Nutrition: Usual food intake pattern.
Very Poor
Probably Inadequate
Adequate
Excellent
Friction & Shear: Impact of skin movement against surfaces.
Problem
Potential Problem
No Apparent Problem
Integumentary Disorders
Bacterial, viral, fungal, and parasitic infections.
Bacterial Skin Infections
Impetigo: Face
Highly contagious! bacterial infection. Prior to crusting (within 24hrs)
Symptoms: Papules vesicular with honey-colored crust; located on body, face, extremities.
Treatment: Antibiotics, good hand hygiene.
can be spread through towels
once crust forms- > not contagious
on antibiotic

Folliculitis: Hair
Superficial infection of hair follicles.
Symptoms: Pain, itching, burning.: near beard and legs
Risks: Poor hygiene, prolonged skin moisture, vaseline, heavy fabric
Topical antibiotic

Furuncles:
“Boil”Acute inflammation within a hair follicle.
Manifestations/Symptoms: Raised, painful pimple; cyst may drain.
Treatment: Manage similar to folliculitis.

Carbuncles: Worst one
Group of infected hair follicles; deeper infection.
Abscesses located in subcutaneous/dermis
Symptoms: Painful, swollen mass, systemic symptoms like fever.

Cellulitis:
Localized infection of the dermis and subcutaneous tissue.
Symptoms: Red, swollen, painful area; systemic symptoms such as fever and chills, swollen lymph glands
Risk of complications: Osteomyelitis, sepsis.
IV antibiotic

Causes of Bacterial Skin Infections
Staphylococcus aureus
Streptococcus pyogenes
CA-MRSA and HA-MRSA
Treatment for Bacterial Infections
Obtain cultures from drainage
Cover draining lesion w/ dressing
Antibiotics (oral, topical, IV).
Do not rupture abscesses.
Impetigo: soak crust with cool compresses, remove crust, Use Oral and topical antibiotics ( contagious 24 hrs after antibiotic ointment is started).
Handwashing to minimize spread.
Viral Infections
Herpes Simplex Virus (HSV):
HSV 1: Cold sores.
HSV 2: Genital herpes.
Goal Decrease spread of disease
Herpes Zoster/Shingles: Clustered Skin Vesicles
Reactivation of chickenpox virus.
Goal: pain control and infection
Treatment: Pain control, antiviral medications (zostavax and shingrix), lidocaine patch to affected area to alleviate discomfort.
People that have been exposed to, or vaccinated against, varicella are not at risk for infection after exposure to Herpes Zoster.
Tinea (Ringworm Types):
Tinea pedis (Athlete’s foot). Topical antibiotic
Tinea capitis (Scalp ringworm). Oral antifungal and topical
Tinea corporis (Body ringworm). topical therapy 2/day for 2 weeks
Tinea cruris (Jock itch). topical antifungal
Treatment includes topical antifungals.
Parasitic Skin Infestation
Pediculosis (Head Lice)
Treatment includes medicated shampoos and thorough cleaning of personal items.
shampoo use once then comb through hair every night
repeat shampoo in 7-10 days
shampoo only kills live lice
Wash infected person's clothes in hot water and dry in hot dryer.
Vacuum the floor and furniture in the infected person's living areas.
Soak combs and brushes in hot water (at least 130 degrees F) for 5-10 minutes.
Seal non-washable clothing or personal items in a plastic bag for 2 weeks.
Types
Pediculosis corporis (body lice)
Pediculosis pubis (genital lice)
Sarcoptes Scabei ( Scabies)
Itches
highly contagious through bedding or clothing
Malignant Skin Disorders
Benign Skin Lesions
Cysts: closed sac in or under skin
Keloids: progressive, enlarging scar
Nevi: moles
Angiomas: hemangiomas

Skin tags: soft papules

Keratosis: benign overgrowth, and thickening of the horny layer of the skin

Non-Melanoma Skin Cancers:
Basal Cell Carcinoma (BCC):
Characteristics: Most common and least aggressive, doesn't typically metastasize.
Risk factors:
fair skin, freckles, blue/green, blonde/ red hair, family hx, excessive uv exposure, severe sunburns, occupational exposure
Management: Surgery excision
Moh’s Surgery: remove thin layers of tumor
Radiation Therapy: External beam

Malignant Skin Disorders: Squamous Cell Carcinoma (SCC):
Can metastasize; prognosis depends on invasion depth.
Firm, scaly, erythematous ”red from inflammation”, or ulcerated
Invasive: goes into squamos epithelium
Prognosis: depends on metastatic incidence

Malignant Melanoma “Worst”
Arises from melanocytes; poor prognosis if diagnosed late, high mortality rate
Risk factors include family history and significant sun exposure.
Diagnosis involves biopsy and assessing for metastasis.
Tests for metastasis
Liver Function Tests
CT of Liver
CBC
Chest X-Ray
Bone Scan
CT Scan of head
“nevi”, benign tumor is a risk factor
Treatment for Malignant Melanoma
Surgical excision
Biological therapy
Immunotherapy
Radiation therapy
Nursing Management
Assess coping mechanisms and family involvement.
Monitor for signs of metastasis to lungs, bones, and liver.
Educate on preventive measures like sun protection.
Skin Specialist look:
20-40 yrs old: every 3 yrs
40+: every year
Malignant Melanoma:
Asymmetry, Border, Color, Diameter (moles should be <6mm), Evolving
Integumentary Disorders Overview
The video addresses several integumentary disorders: cirrhosis, pruritus, acne vulgaris, psoriasis, and inflammatory skin disorders.
Cirrhosis (Xerosis)- “Dry Skin”
Definition: Cirrhosis refers to dry skin often seen in older adults due to decreased activity of sebaceous and sweat glands.
Skin Care Recommendations:
Use mild pH balanced soap for cleansing.
Bathe in warm water, limiting bath time to < 10 minutes to prevent skin drying.
Apply moisturizers twice a day.
Address incontinence promptly to prevent skin issues.
Use skin barrier creams like Calmoceptine.
Management Practices:
Frequent repositioning to prevent pressure sores.
Utilize pressure redistribution devices, e.g., waffle cushions.
Possible Causes: Exposure to environmental heat, low humidity, sunlight, excessive bathing, or dehydration can exacerbate dry skin.
Manifestations: Generally include itching and flaky skin.
Pruritus
Definition: Pruritus is intense itching caused by the stimulation of nerve receptors in the skin, further releasing histamine and mediators that promote itching.
Characteristics:
Itching can lead to increased inflammation and skin damage, leading to risks like cellulitis and excoriation.
Triggers:
Internal (diseases like cancer, diabetes, etc.) and external factors (insects, certain fabrics, medications).
Secondary to disease: DM, Liver, Renal, Hypothyroid
Management:
Identify and eliminate triggers.
Medications: antihistamines, topical corticosteroids ( every 3- 4 hours) , anesthetics.
Ex: Fexofenadine(Allegra), hydroxyzine, is a nonsedating antihistamine
Therapeutic baths (e.g., cornstarch, baking soda).
Use mild soaps when bathing, especially in children.
mild detergent
no fabric softeners
avoid perfumes / lotion containing alconol
do not bathe daily
apply skin lubricants post shower
keep nails trimmed
wear loose fitting clothing
brief application of pressure or cold
cotton gloves to prevent scratching enight

Acne Vulgaris: Secretory Disorder
Definition: A common disorder affecting hair follicles primarily on the face, back, chest, and upper arms.
adolescence: male
adult: women
Prevalence: affects up to 80% of Americans across their lifespan, mostly teenagers; prevalent in adulthood among women.
Management Goals:
Reduce bacterial colonies, sebaceous gland activity, prevent follicle blockage, and minimize scarring.
Nutrition and Hygiene:
Diet has no conclusive impact but may correlate with certain foods.
Hygiene is crucial for managing acne.
Pharmacological Treatments:
Common treatments include topical agents like clindamycin and doxycycline.
Psychological Care:
Encourage outdoor activity and social interaction to improve mental health regarding acne self-image.
Psoriasis
Definition: A chronic immune inflammatory skin disorder with no known cure.
Pathophysiology:
The immune system mistakenly activates T cells, causing rapid skin cell production.
New skin cells form in days instead of weeks; results in plaque buildup with silvery scales.
Management:
Topical corticosteroids & tar preparation are the most frequently prescribed treatments, applied with careful adherence.
Other treatments include coal tar, vitamin D3 preparations, retinoids, light therapy “ Laser therapy, UV B Light” , or systemic medications like “methotrexate, retinoids” (severe).
Triggers: Stress, infections Strep throat, skin trauma, certain medications, and seasonal changes can exacerbate symptoms.
Nursing Interventions:
Emphasize lifetime management, avoid frequent washing, and educate on gentle scale removal.
Complications:
Psoriatic
Arthritis
Irritant Contact Dermatitis
Definition: A type of dermatitis caused by irritation from substances like soaps or chemicals, rather than an allergic reaction.
Generalized Exfoliative Dermatitis:
Severe inflammatory reaction over the entire skin surface from medications, pre-existing conditions, or types of cancer.
Conclusion
Comprehensive understanding of these integumentary disorders is vital for nursing care and patient management. Employ appropriate interventions tailored to each condition for effective patient support.