Drug Addiction
Drugs
· Chemical substances which interact with the biochemistry of the body:
o Inhibit or reinforce enzyme activity
o Block or activate receptors
o Interact with neurotransmitters or hormones in other ways
o Attack “invaders” (e.g. antibiotics)
What are psycho-active drugs?
· Any chemicals that influence the way we feel or act.
· Usually they interact with the nervous system and/or the endocrine system
· Mostly, they act at synapses (among other places)
Agonist vs. Antagonist
At the synapse level (effect on post-synaptic cell):
Agonist: mimics/increases action of the neurotransmitter
Antagonist: blocks action of the neurotransmitter
At the receptor level (effect on receptor):
Agonist: mimics action of the neurotransmitter
o Antagonist: blocks action of the neurotransmitter
Possible sites of Drug Action
Example (do not need to learn these examples):
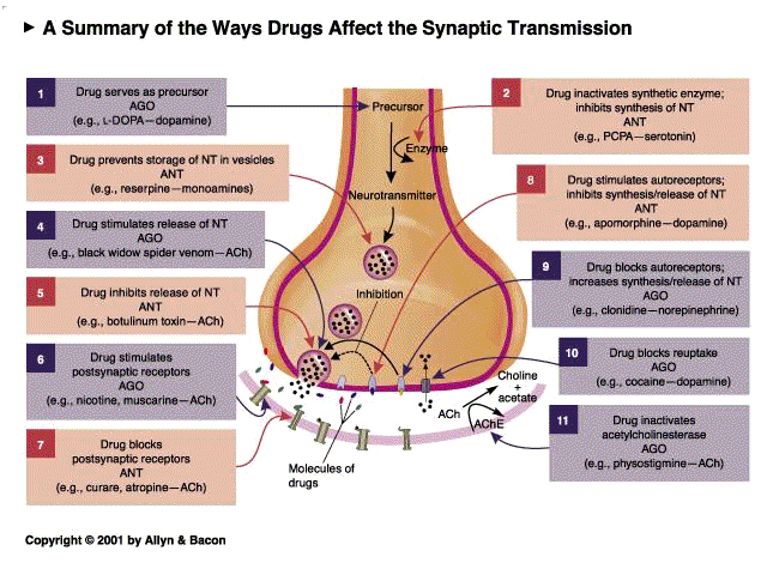
Drugs can interact with synapse in many ways
Blue = Agonist may mimic or bind to NT
Red = Antagonist Block the receptors in post-synaptic neuron
Autoreceptor receptor located in the pre-synaptic membrane
· Some NTs bind to these receptors
· Function as a negative feedback loop
· Reduce release of more neurotransmitters
· Mechanism to not waste NTs
Agonist at presynaptic level:
· If a drug binds to the presynaptic receptor, it views it as an agonist
· Stops the release of more neurotransmitters
· If it is specific only to the presynaptic terminal, it is an antagonist at a synapse level.
Antagonist at presynaptic level
· If a drug is an antagonist in the presynaptic receptor, it binds to it.
· Stops/prevents feedback of autoreceptor
· Is therefore an antagonist at a synapse level because more NTs continue to be released into the synapse.
Pharmacokinetics
Intake
How does a drug:
· Get into your body
· Distribute
· Get into the brain
· Leave the body
Many routes:
· Digestive tract
· Respiratory tract
· Through skin
· Through mucous membranes
· Intravenous injection (directly into the blood)
· Intramuscular injection (into the muscles)
· Subcutaneous injection (under the skin)
Fastest route = intravenous injection
Slowest route = digestive tract
Skindepends on how easily the drug can penetrate skin/if at all
Example: Cocaine
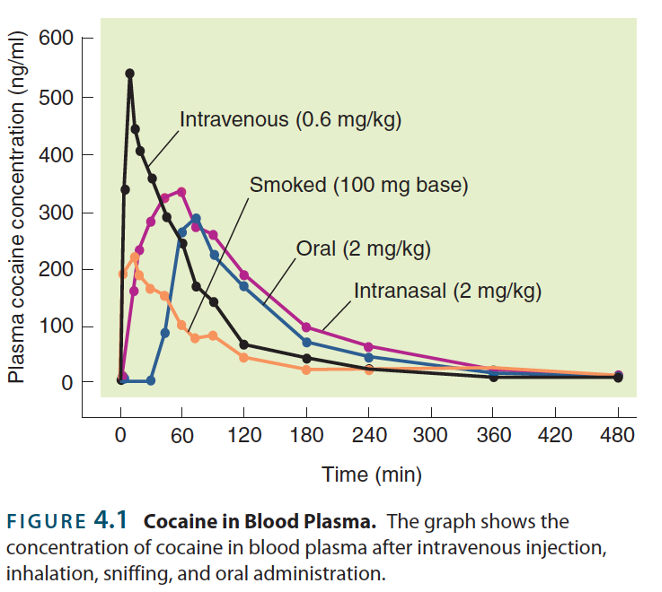
Fastest Slowest
1. Intravenous
2. Smoked
3. Intranasal
4. Oral
Quicker the concentration of the drug goes up in your blood, the stronger the effect.
Pharmacokinetics: distribution
· Bloodstream goes all across the body
· Water-soluble molecules
o Can be directly dissolved in the blood, but do not pass through cell membranes
· Lipid-soluble molecules
o Need carriers to transport them through the blood, but can pass directly through cell membranes
Fat and water do not mix, therefore lipid soluble molecules are harder to transport around the body.
Cell membranes are made of fats:
· Lipid soluble molecules can go through skin
· Skin designed to be water resistant, water-soluble molecules cannot penetrate skin
Blood-Brain Barrier
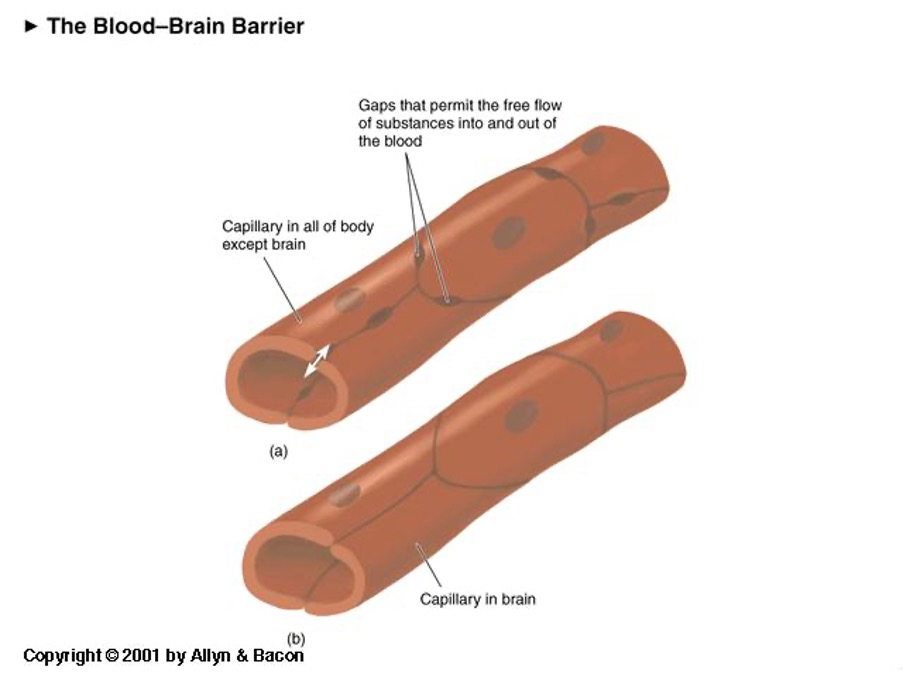
Capillaries around the body – gaps between endothelial cells
· Allows blood to flow in and out
Capillaries in the brain – no gaps between endothelial cells
· Stops molecules in blood stream to get to brain unless they are needed (e.g. glucose)
· Special transport molecules that get molecules to the brain
Except if toxin is very fat soluble – endothelial cell’s membrane has a lipid bilayer
· Therefore, lipid soluble drugs can easily cross blood-brain barrier.
Non-lipid soluble drugs cannot break the blood-brain barrier
· E.g. Alcohol is both water and libid-soluble, so can pass blood-brain barrier.
Pharmacokinetics: elimination
· All drugs are eventually eliminated from the body:
o By chemical breakdown (by enzymes)
o By excretion (filtered by kidneys and released in urine)
· Some drugs can be stored in the body for a long time (e.g. lipid-soluble drugs in fat tissue)
o Can only be eliminated from the body if they are in the blood stream
o Fat soluble drugs remain in fat cells – takes longer to be cleared
· Biological Half-Life can vary from minutes to weeks
Biological Half-Life = Rate it takes for drug to be eliminated
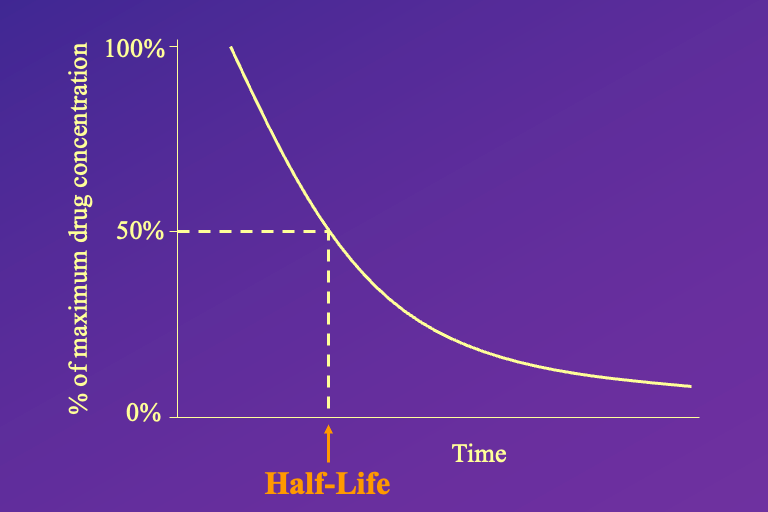
Different drugs have different half-lives
· Pharmaceutical companies will design drugs to either have a short or long half-life (e.g. benzodiazepine, short half-life to help sleep at night not during day)
Half-life because it is difficult to measure when a drug gets to 0.
· Lipophillic drugs have a LONGER half-life.
Physical Drug Dependence
Drug Tolerance
Dose response curve:
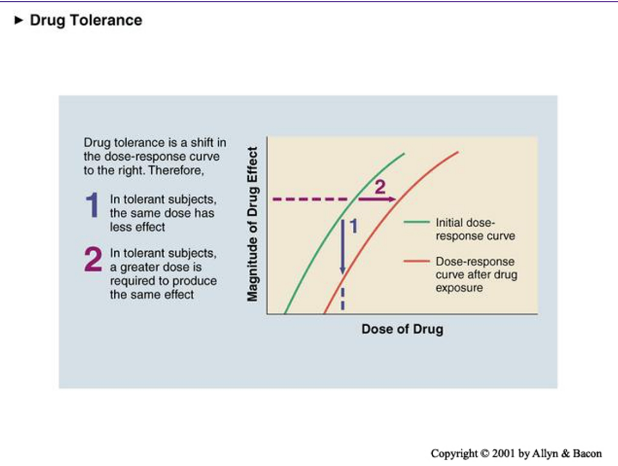
Plot dose vs effect
More drug = more effect
Minimum amount of drug = strong effect
Tolerance = shifts whole curve to the right
1. In tolerant subjects, the same dose has less effect
2. 2. In tolerant subjects , a greater dose is required to produce the same effect
Body maintains Homeostasis
· Mechanisms to maintain a state in the body:
– Metabolic tolerance (better elimination of the drug)
– Functional tolerance:
• change in receptor numbers
• change in receptor sensitivity
• change in intracellular cascades
E.g. Negative feedback systems counter the feedback of the drug
Often these mechanisms are slow. Not an immediate physiological response. May involve:
· Better elimination of the drug
· Increase or decrease the number of receptors that react to the drug
· May change receptors to be less sensitive to the drug.
TOLERANCE IS AN ACTIVE RESPONSE OF YOUR BODY TO A DRUG, AND IT TAKES TIME TO RESPOND.
Mechanism doesn’t disappear when drug disappears:
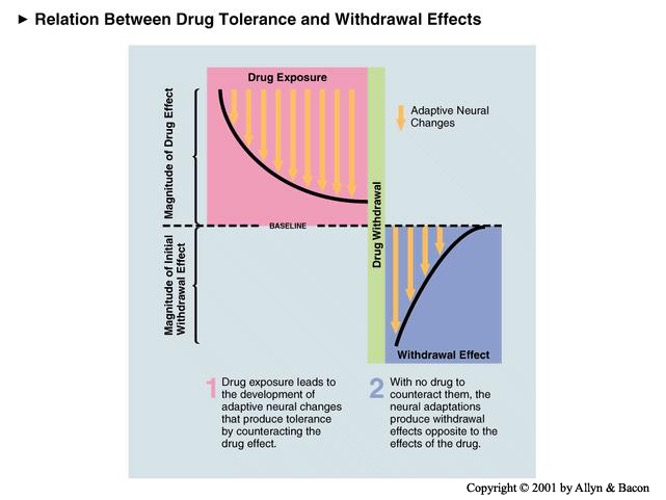
Withdrawal = Physical dependence on drug
1. The body builds up a tolerance response.
Withdrawal effect = tolerance mechanisms are still there.
2. Still changes in receptors.
· The tolerance mechanism pushes in the opposite direction to what the drug did.
3. Pushes your body away from homeostasis
· Results in the opposite effect to the drug.
E.g. take away painkillers more pain
TAKES TIME TO GET RID OF WITHDRAWAL SYMPTOMS.
Tolerance is Context Dependent
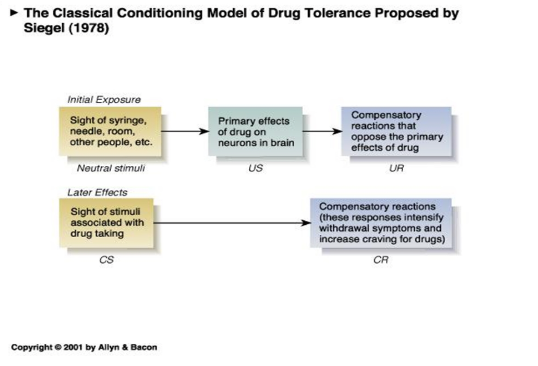
Classical conditioning – Siegal (1978)
Tolerance is triggered by context at which you took it
· Overdosing is easier in novel surroundings
o The body wasn’t prepared for it – context triggers compensatory response that raises tolerance
o E.g. more likely to overdose on holiday
· Withdrawal symptoms also occur in familiar settings
· Possibly a reason for relapsing
o Even people who have been clean, context triggers withdrawal leading to relapse
Psychological Drug Dependence
Based in the brain, but different mechanism for withdrawal symptoms
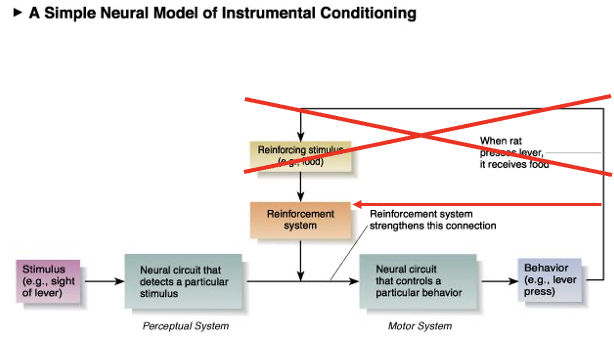
Operant conditioning
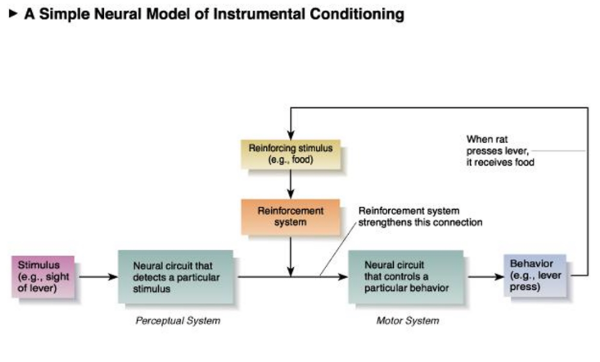
1. Stimulus
2. Perceptual - Neural circuit detects stimulus
3. Motor - Neural circuit controls particular behaviour
4. Behaviour
5. Reinforcing stimulus (reward)
6. Reinforcing system
· Strengthens connection between the Perceptual and Motor system
Intra-Cranial Self-Stimulation
Experiment – wanted to control rats
· Stimulated the rats brain when they were in a certain place
· If it hurt the rat, it would avoid that area
· ACTUALLY found rat went to that area more and more
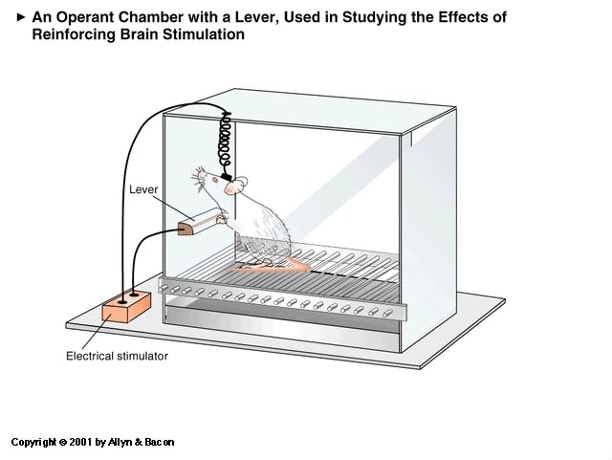
· Stimulated same part of brain when pressing the lever
· Rat repeatedly pressed the lever
· Indicates REWARD SYSTEM was stimulated
Major Brain Subdivisions
Developing human brain
Early front of hollow neural tube three nodules that form
1. Forebrain
2. Midbrain
3. Hindbrain (then spinal cord)
Then brain splits into four/ five parts
1. Telencephalon – cortex and basal ganglia and
2. Diencephalon – Thalamus and Hypothalamus
3. Mesencephalon - Midbrain stays the midbrain (Tectum and Tegmentum)
4. Metacephalon – Cerebellum and Pons
5. Mylencephalon – Medulla
(and spinal cord)
ULTIMATELY 5 subdivisions
Most areas need a very strong stimulus
BUT some areas require less…
Mesotelencephalic Dopamine System
Connects midbrain to end brain
(meso as in midbrain, telen as in cortex)
· Dopamine functions as a neurotransmitter
· Cell bodies in the mesencephalon
· Makes lots of synapses in the telencephalon
Ventral tegmental area
- Lots of dopaminergic neurons
Nucleus accumbens
- Where dopaminergic neurons make synapses
Medial forebrain bundle
- A bundle of axons running from mesencephalon and telencephalon
^^ If you stimulate this bundle of axons – easier to hit than VTA
- Triggers the release of dopamine
Plant an electrode into the bundle of axons
- The animal presses the lever during intracranial self-stimulation of MTP dopamine system
- The dopamine levels go up.
HOWEVER, this is correlational, NOT causal
How to test whether dopamine release is causally involved in rewarding effect of intercranial stimulation?
· Block the action of dopamine while stimulating
Stellar, Kelley & Corbett (1983)
1. Stimulated Medial Forebrain bundle
o Releasing dopamine, get rats to self-stimulate
2. Infuse dopamine antagonist (receptor blocker) in nucleus acumens
a. Rats did NOT learn to press the lever
3. Shows that dopamine released by stimulation is responsible for learning.
VTA nucleus accumens release of dopamine is part of reinforcement system in the Neural Model of Instrumental Conditioning
Something in the brain is causing reward VTA and nucleus acumens are part of that.
Reward: Pleasure or ?
· Dopamine is released with punishing stimuli as well
o Definitely not pleasure
· Overtrained rats do not release dopamine upon reward
o Even if they enjoy the food
· Dopamine blockers make rats work less hard for food, but they still enjoy it
o Antagonists – won’t learn but still enjoy food
SEEKING OR WANTING HYPOTHESIS – Dopamine is not associated with pleasure
It is to do with:
1. Gathering information
2. Compulsion to do something again and again
E.g. Drug addicts have a compulsion to take the drug even if they do not enjoy it anymore
Evidence for seeking
Dopamine levels in male rat NA
1. New environment (sex chamber) – increase dopamine levels
o No reward, info gathering
2. Female gets introduced
o Next to male (cant reach)
3. Introduced in the same compartment
4. Female is taken away again
Dopamine increases where you wouldn’t expect “pleasure”
DOPAMINE IS LINKED TO
1. Novelty seeking, exploration
2. Compulsion to repeat behaviour (even if pleasure has worn off)
• When drugs directly interact with the brain’s reward system
• Mesotelenphalic Dopamine System
• System evolved to make animals do something to increase their survival
• Addict will crave the drugs, even while disliking their effects
Cocaine and Amphetamine increases Dopamine Levels
^^Psychologically addictive
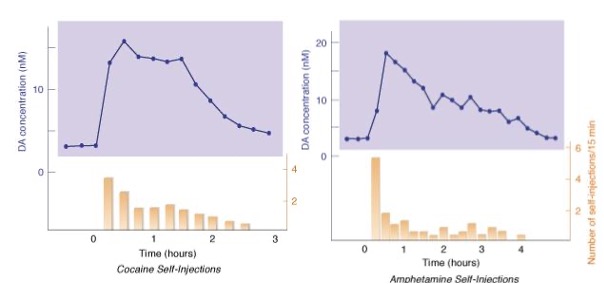
Rat study
1. Self-injections into NA when lever pressed
o Dopamine increases
2. Repeatedly press lever
o Learning to repeat behaviour that led to dopamine release
Psychological Drug Dependence in Humans:
· Bypass systems in brain that assess whether something is good or bad
· Straight to releasing dopamine from VTA into NA
· Compulsion to take drugs in the future (behaviour that led to release in dopamine)
Summary
• Different drugs have different pharmacokinetics
• Physical drug dependence is due to drug tolerance
• The Ventral Tegmental Area and Nucleus Accumbens are involved in the “reward” or “seeking” system in the brain
Psychological dependence works through this Mesotelencephalic dopamine pathway