Renal System
Body Fluids:
Intracellular - represents all fluid inside cells.
Provides a stable medium for normal cell functioning.
Consists mainly of water, dissolved ions, small molecules, and larger proteins.
Makes up 2/3 of total body fluid.
Extracellular - represents all fluid outside cells.
Interstitial fluid - largest sub-compartment, and contains nutrients, oxygen, waste, chemical messengers and a small amount of protein.
Plasma - exists in the vascular system, and differs from interstitial fluid as it has a high protein concentration and helps suspend vascular cells.
Trans-cellular fluid - separated from plasma by an additional epithelial layer.
Makes up 1/3 of total body fluid.
Plasma proteins are responsible for osmotic gradient across capillary walls which counteracts the hydrostatic pressure of capillary blood.
Hydrostatic and Colloid Osmotic Pressure:
Hydrostatic - the forces exerted by a fluid against a wall, causing movement of fluid between different compartments.
This is the fluid pressure of the solution.
Particularly important in the kidney to ensure proper filtration of blood to form urine.
Colloid Osmotic - the pressure exerted by proteins in the blood plasma that attracts water into the circulatory system, counteracting hydrostatic pressure of the capillary blood.
It relies on the selective permeability of membranes.
Ions can move rapidly between the plasma and interstitial fluid, making them ineffective osmotic agents.
Proteins are largely restricted to plasma, making them effective osmotic agents.
Distribution of Ions:
Cell Membrane Selectivity:
Allows movement of solutes across the membrane at different rates.
Distribution of ions on either side of a membrane is not equal, for example Na+ is less permeable than K+ and Cl-.
Active Sodium-Potassium Pump for Concentration Gradient:
Osmolality - concentration of substance in 1L solvent, measured in mosmoles.
The osmolality of the extracellular fluid depends on Na+ content, whereas the osmolality of the intracellular fluid depends on K+.
Basics of Kidney Function:
The renal system consists of the kidneys, ureters, bladder and urethra. The overall function is the filtration of roughly 200L of fluid per day from renal blood, allowing for excretion of toxins, metabolic waste, and excess ions, and the reabsorption of water.
Homeostasis - the kidney plays a vital role; it controls concentration of waste products, osmolality, volume, acid-base status and ionic composition of extracellular fluid.
The renal cortex is the outer region of the kidney, containing the glomeruli and proximal tubules, which are essential for the initial filtration of blood and reabsorption of essential nutrients.
The renal medulla is the inner region of the kidney, made up of the renal pyramids and the Loop of Henle.
The Nephron:
The human kidney has roughly 1.5 million nephrons, which play a role in:
Glomerular filtration
Tubular reabsorption and secretion
Urine formation
Each nephron contains a vascular component and a tubular component.
Glomerular Filtration:
Glomerular filtration is dependent upon:
Capillary permeability
Hydrostatic pressure in capillaries
Hydrostatic pressure in tubules
Osmotic pressure of plasma in glomerular capillaries
Osmotic pressure of tubular filtrate
The Juxtaglomerular Apparatus
Located between the afferent arteriole and the distal convoluted tubule.
Macula Densa Cells - cells at distal end of the thick ascending limb, and ones lining the wall of the DCT that sense changes in NaCl delivery (tubular component).
Granular Cells - found mainly in walls of afferent arterioles, which synthesise and store renin (vascular component).
Mesangial Cells - located between vessels, forming connections via actin and microtubules, and facilitating vasoconstriction or vasodilation of the arterioles when mesangial cells contract.
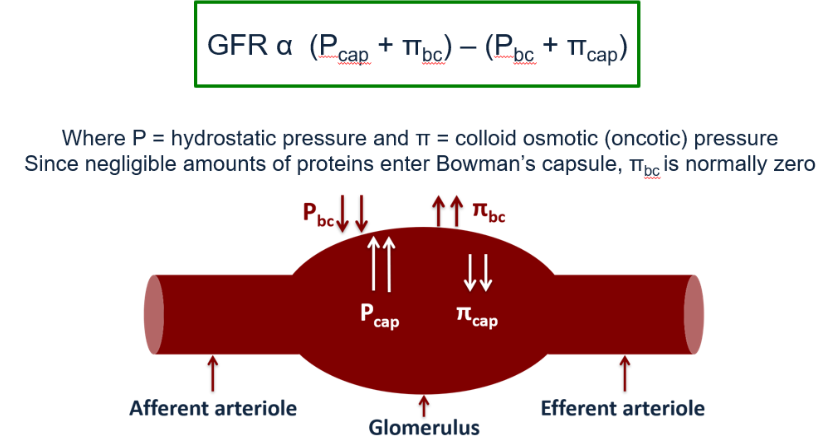
The Blood Pressure within a capillary (Pcap) is around 35mmHg, whereas in the Bowman’s Capsule, the pressure (Pbc) is lower.
The hydrostatic pressure causes outward filtration force from plasma into the Bowman’s capsule.
The Colloid Osmotic Pressure within the capillary (πcap) is around 25mmHg, whereas it is 0mmHg in the Bowman’s Capsule (πbc).
Fluid leaves the capillary and enters the Bowman’s Capsule as ultrafiltrate.
GFR decreases during afferent vasoconstriction, and GFR increases during efferent vasoconstriction.

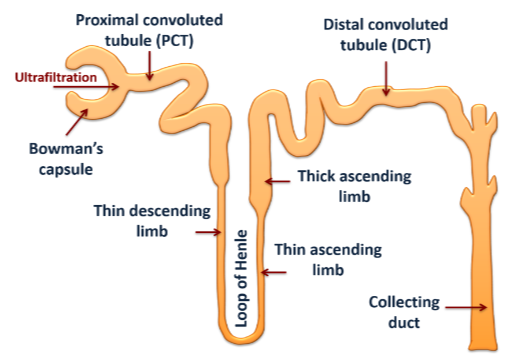
Proximal Convoluted Tubule:
Fluid entering the PCT has similar composition to plasma.
It actively reabsorbs Na+ so only a small concentration is delivered to sites downstream, and is driven by the Na+/K+-ATPase transporter.
Reabsorption of glucose and bicarbonate.
Almost all linked directly to reabsorption of Na+ ions.
Loop of Henle:
Water reabsorption occurs in the descending limb.
Water leaves the filtrate and diffuses through aquaporins into the surrounding tissues via osmosis.
This happens due to the high concentration of sodium and chlorine ions outside of the tubular environment.
The filtrate now enters the thin ascending limb which is impermeable to water, but permeable to ions.
Ions move out of the filtrate passively via diffusion.
In the thick ascending limb, the body makes sure essential ions are recovered.
Impermeable to water, with active transport moving Na+ and K+ out of the filtrate, along with 2 chlorine ions to maintain electro-neutrality.
Presence of K+ channels where K+ can passively move back into loop, creating an electrochemical gradient for other ions (i.e. Ca2+ and Mg2+) to be reabsorbed.
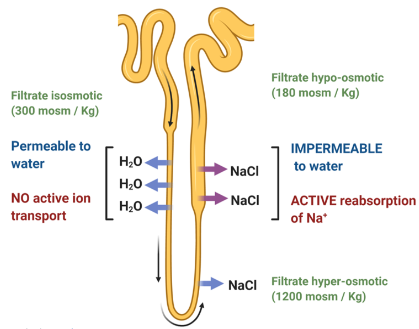
Counter-Current Multiplier:
This process is aided by active transport of solutes out of the ascending limb of the loop of Henle.
This concentrates the interstitium, facilitating movement of water via osmosis from the descending limb - the filtrate is hyperosmotic.
The tubule epithelium of the ascending limb is impermeable to water, and the solutes are pumped out - the filtrate is hypo-osmotic.
Distal Convoluted Tubule and the Collecting Duct
Distal Convoluted Tubule
Active reabsorption of Na+.
Secretion of K+ and H+ ions.
Stimulated by the actions of aldosterone.
Collecting Duct
Urea is free to move out of the collecting duct in the presence of ADH.
ADH opens water channels, increasing reabsorption of water, which ultimately concentrates urine.
Renin-Angiotensin-Aldosterone System:
Hormone system that is essential for regulation of fluid balance and blood pressure.
Stage 1 - release of the enzyme renin from granular cells of the juxtaglomerular apparatus in response to decreased perfusion pressure, increases sympathetic response and decreased sodium ion concentration at DCT.
Stage 2 - release of enzyme angiotensin converting enzyme (ACE) which converts angiotensin I to angiotensin II.
Stage 3 - angiotensin II exerts its actions on the body.
The renin-angiotensin-aldosterone system (RAAS) controls fluid and electrolyte balance, and therefore blood pressure, through well-controlled and coordinated effects on organs.
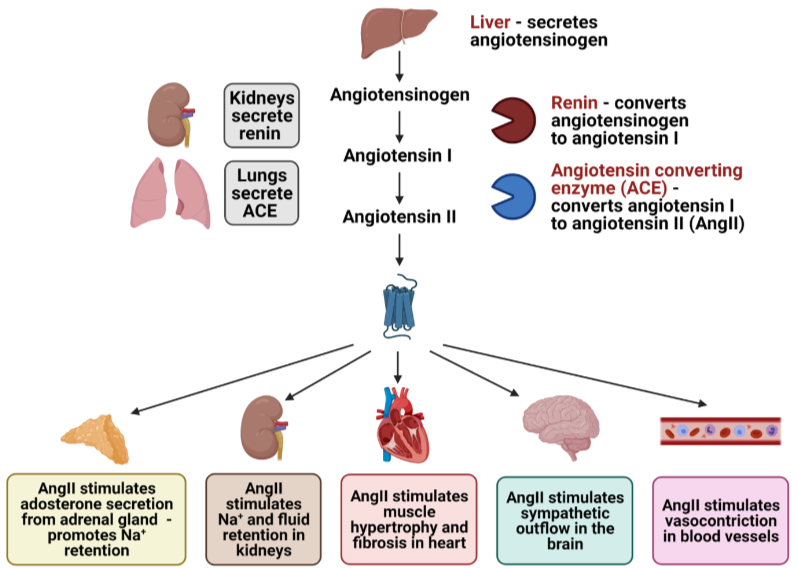
Angiotensin II is the active peptide in the RAAS, which binds to angiotensin receptors (AT1R and AT2R).
Increases blood pressure by constricting arterioles, mediated at AT1R.
Stimulates reabsorption of Na+, meaning water is also reabsorbed.
Stimulates the release of aldosterone from the adrenal gland, which acts on the DCT to increase reabsorption of Na+ and water.
Aldosterone is a steroid hormone released from the zona glomerulosa of the adrenal cortex.
Increases in plasma K+ and angiotensin II, or decreases in plasma Na+ lead to elevated levels of aldosterone.
It acts on intracellular receptors in the DCT to increase Na+ channels.
Antidiuretic Hormone (ADH)
ADH is synthesised in the hypothalamus and stored in the posterior pituitary.
Osmoreceptors and Baroreceptors regulate the release of ADH.
Changes in the osmolality of body fluids are sensed by osmoreceptors in the hypothalamus which trigger release of ADH, whereas changes in blood pressure are sensed by cardiopulmonary baroreceptors, which triggers release (when reduced), or inhibition (when increased) of ADH.
ADH regulates extracellular fluid volume - it acts on V2 receptors at the collecting ducts.
When more ADH is present, more water is reabsorbed, so antidiuresis.
When less ADH is present, less water is reabsorbed, so diuresis.
ADH also evokes vasoconstrictor and vasopressor cells - it acts on V1 receptors on vascular smooth muscle cells.
ADH involves the insertion of aquaporin-2 channels into the apical membrane.
Atrial Natural Peptide (ANP):
28 amino-acid peptide that is synthesised within the atrial myocytes - it is released in response to an increase in blood pressure.
It opposes the RAAS and inhibits the release of renin.
Causes sodium ion and water loss by inhibition of aldosterone and ADH synthesis.
Increases GFR.
Acts as a vasodilator, and stimulates beta-adrenoceptors.
ANP acts acutely to REDUCE plasma volume by:
Increased renal excretion of salt and water.
Vasodilation.
Increased vascular permeability.
Osmotic Diuretics:
Substances that work in the proximal convoluted tubule, that alter the osmolality of the plasma to retain water in the PCT and the descending limb. This dilutes the electrolyte concentration, and increases urinary output. For example, mannitol.
Carbonic Anhydrase Inhibitors:
Carbonic Anhydrase in the lumen of the PCT converts carbonic acid to water and CO2.
Water enters the brush border cells via diffusion.
Intracellular carbonic anhydrase then converts water and CO2 back into carbonic acid, which dissociates.
The inhibitors block this exchange of ions, which reduces the H+ concentration in the PCT.
However, there is still some Na+ reabsorption, and reduced GFR, so they are not potent.
Loop Diuretics:
They act on the ascending limb of the loop of Henle to block the Na+/K+/2Cl- symporter, preventing creation of a hypertonic interstitium in the medulla.
Increases Na+ delivery to the DCT, promoting K+ loss.
Promotes renin release, and therefore increased angiotensin II activity.
Potent - they cause 15-25% of filtered Na+ to be excreted, and they may cause hypokalaemia.
Thiazides:
Blocks Na+ and Cl- reabsorption at the beginning of the DCT.
Inhibits the electrochemically neutral Na+/Cl- co-transporter by competitively binding to the chlorine binding site.
Increases solute in the tubular fluid, decreasing water reabsorption gradient.
It is not effective at low GFRs, and rely on being secreted into the PCT.
Example is bendroflumethiazide.
Potassium Sparing Diuretics:
These do not act directly on sodium transport pumps.
Some drugs within this class are aldosterone receptor antagonists which act at the distal end of the DCT.
They block the actions of aldosterone, meaning that less K+ and H+ is exchanged, meaning less is lost.
This means that there is less risk of hypokalaemia.
Example is spironolactone.