Chapter 12: Touch
I need you to organize these notes better for when I’m studying please. Make sure to include all information becuase my exam will be on the extensive details. Include all studies and such. Thank you.
Introduction to Touch and Somatosensation-
Definition of Touch:
Refers to sensations caused by mechanical displacements of the skin.
Occurs upon contact with an object or due to physical interaction like being poked or licked.
Tactile Sensation:
Refers to mechanical interactions, expanding touch to include:
Perception of temperature changes (thermal sensation).
A sensation of pain caused by tissue damage or potential harm.
Itchiness.
Internal sensations informing about limb positions and movements (kinesthesis).
Kinesthesis:
Definition: Perception of limb position and movement in space.
Arises from muscles, tendons, and joints.
Part of proprioception, a broader system including the vestibular system.
Proprioception:
Perception is mediated by kinesthetic and vestibular receptors.
Includes information about body position and movement.
Somatosensation:
Collective term encompassing sensory signals from the body.
Includes tactile, thermal, pain, itchiness, and kinesthetic sensations.
soma means body
Significance of Pain and Temperature Sensations:
Pain: Serves as a warning system indicating internal issues or external dangers, enabling quick defense mechanisms.
Temperature Sensations: Help in seeking or creating a thermally safe environment.
Role of Touch:
Mechanical sensations play an important role in our intimate sexual and reproductive activities and they provide a powerful means of communicating our thoughts and emotions nonverbally
Importance of Touch:
Object Identification and Manipulation: Essential for identifying and manipulating unseen or unheard objects.
Action Involvement: Involves action to a greater extent compared to other senses.
Touch Physiology
Touch Physiology:
Sense organs and receptor units for touch are embedded in the skin's epidermis and dermis layers.
Epidermis: Outer layer of the skin.
Dermis: Inner layer of the skin containing nutritive and connective tissues housing mechanoreceptors that converge to smaller neurons to different areas of the brain
Receptor Units for Touch:
Embedded in both epidermis and dermis layers.
Mechano receptors are located within the dermis.
Receptor Diversity:
Similar to the eye's rods and cones, the skin hosts multiple types of touch receptors.
These receptors form the basis of multiple channels, each contributing to the overall sense of touch.
The 3 Characterizations of Touch Receptors:
1) Type of Stimulation: Receptors respond to various stimulus events such as pressure, vibration, and temperature changes.
2) Size of Receptive Field: Activation of receptors occurs when stimulation is applied to a specific area, termed the receptive field. The size of the receptive field indicates the extent of the body area eliciting the receptor response.
3) Rate of Adaptation:
Fast Adapting (FA) Receptors: Respond with bursts of action potentials when the preferred stimulus is applied or removed. They do not respond during the steady state between stimulus onset and offset.
Slow Adapting (SA) Receptors: Remain active throughout the period when the stimulus is in contact with their receptive field.
Tactile Receptors and Associated Types
Tactile Receptors Overview:
Tactile receptors are a type of mechanoreceptor responsive to mechanical stimulation, particularly pressure.
Consists of nerve fibers and associated expanded endings.
Classified as A-beta fibers, characterized by wide diameters facilitating fast neural conduction.
Mechanoreceptors:
Sensory receptors are responsive to mechanical stimuli like pressure, vibration, and movement.
Major Types of A-beta Tactile Receptors:
Found in regions covered with hairy skin (e.g., forearm).
Properties are similar in both hairy and hairless skin.
Consists of two slowly adapting and three fast-adapting receptors.
Types of A-beta Tactile Receptors: a. Meissner Corpuscles:
Type of tactile receptor.
Involved in sensitivity to light touch.
Functions as a fast-adapting receptor.
b. Merkel Cells:
Tactile receptors associated with detecting sustained pressure and shapes.
Classed as a slowly adapting receptor.
c. Ruffini Endings:
Detects stretching of the skin.
Categorized as a slowly adapting receptor.
d. Pacinian Corpuscles:
Sensitive to vibration and deep pressure.
Functions as a fast-adapting receptor.
Tactile Nerve Fibers and Endings:
Assumed that different types of tactile nerve fibers terminate in distinct expanded endings.
Controversy exists among scientists regarding the specific expanded endings for each type due to challenges in directly observing physical connections.
Mechanoreceptor Populations and Sensitivity
Response Characteristics of Mechanoreceptor Populations:
Meissner Corpuscle (FA I):
Specialized nerve ending, Fast-adapting fibers with small receptive fields.
Merkel Cell Neurite Complex (SA I):
Specialized nerve ending, Slow-adapting fibers with small receptive fields.
Pacinian Corpuscle (FA II):
Specialized nerve ending, Fast-adapting fibers with large receptive fields.
Ruffini Ending (SA II):
Specialized nerve ending, Slow-adapting fibers with large receptive fields.
Location of Receptor Endings:
Meissner and Merkel receptors: Located at the epidermis-dermis junction.
Pacinian and Ruffini receptors: Situated deeper in the dermis and subcutaneous tissue.
Classification based on Adaptation Rates and Receptive Field Sizes:
The four types of mechanoreceptors can be categorized independently according to adaptation rates and sizes of receptive fields.
Feature Sensitivity and Primary Functions of Each Tactile Fiber Type:
SA I (Merkel):
Best response to sustained downward pressure, spatial details, and very low-frequency vibrations (<5 Hz).
assumed to terminate in Merkel cell neurite complexes.
Crucial for texture, pattern perception, Braille reading, and object orientation.
single SA I fiber = feel pressure
SA II (Ruffini):
Responds to sustained pressure and lateral skin stretch.
Important for determining proper finger shaping when grasping objects.
single SA II fiber = don’t experience any tactile sensation at all
assumed to terminate in Ruffini endings.
FA I (Meissner):
Best response to low-frequency vibrations (5-50 Hz).
Critical for detecting motion across the skin and correcting grip.
single SA I fiber = get a localized sensation known as a wobble or flutter
assumed to terminate In Meissner corpuscles.
FA II (Pacinian):
Responds best to high-frequency vibrations (50-700 Hz).
Detects initial object contact, aiding in understanding the force of contact and object manipulation.
single FA II fiber = more diffused sensation in the skin like a buzz
shown to terminate in Pacinian corpuscles
Integration of Mechanoreceptors:
Similar to rods and cones contributing to visual perception, all four types of mechanoreceptors work together to provide comprehensive information about touched objects.
Maximal Feature Sensitivity and Primary Functions of Mechanoreceptors:
SA I: Sustained pressure, very low frequency (<5 Hz), texture, and pattern/form detection.
FA I: Temporal changes in skin deformation (5-50 Hz), low-frequency vibration detection.
SA II: Temporal changes in skin deformation (50-700 Hz), high-frequency vibration detection.
FA II: Sustained downward pressure, lateral skin stretch, less sensitivity to vibration across frequencies, finger position, stable grasp.
Specialized Mechanoreceptors: there is specialized mechanoreceptors for certain things like body movement
Kinesthetic Receptors and Muscle Spindles
Kinesthetic Receptors Overview:
Apart from tactile mechanoreceptors in the skin, there are mechanoreceptors present within muscles, joints, and tendons.
Collectively known as kinesthetic receptors, they play a vital role in sensing limb positions and movements.
Role of Kinesthetic Receptors:
Provide essential information about limb positioning and types of movements being executed.
Muscle spindles, tendon receptors, and joint receptors contribute to this sense of limb positioning and movement.
Types of Kinesthetic Receptors:
Muscle Spindles:
Sensory receptors within muscles that detect muscle tension.
Embedded within the main muscle fibers (extrafusal) and contain inner fibers (intrafusal).
Convey information about muscle length and regulate muscle tension by contracting inner fibers to produce a sensory response back to the central nervous system.
come into play particularly when a joint is bent to an extreme angle.
Importance of Kinesthetic Receptors - Ian Waterman's Case:
Ian Waterman suffered from a viral infection that destroyed the cutaneous nerves connecting his kinesthetic and other mechanoreceptors to his brain when he was 19 years old.
Without kinesthetic senses, Waterman became entirely reliant on vision to perceive the positions of his limbs in space.
In the absence of light, Waterman couldn't perform basic tasks like tying shoes, walking up/down stairs, or clapping his hands due to a lack of awareness of his limbs' positions.
Waterman's experience demonstrates the crucial role of kinesthetic receptors in daily motor functions and spatial awareness.
Definitions:
Kinesthetic: About perception involving sensory mechanoreceptors in muscles, tendons, and joints.
Muscle Spindle: A sensory receptor located within a muscle that senses its tension, aiding in the regulation of muscle length and tension. Contains intrafusal fibers that contract to convey information about muscle length to the central nervous system.
Thermoreceptors and Temperature Sensation
Thermoreceptors Overview:
Thermal receptors are situated in the epidermal and dermal layers of the skin, signaling changes in skin temperature.
They inform us about alterations in skin temperature, detecting both warmth and cold sensations.
Types of Thermal Receptors: we have 2 thermoreceptors
Warmth Fibers:
Sensory nerve fibers are activated when skin temperature increases.
Cold Fibers:
Sensory nerve fibers are activated when skin temperature decreases.
Outnumber warmth fibers by a ratio of approximately 30:1.
Normal Skin Temperature Range:
Under normal conditions, skin temperature is maintained between 30°C and 36°C.
Both cold and warm fibers have a minimal response within this temperature range.
Response of Thermoreceptors to External Objects:
Thermoreceptors are activated when encountering objects warmer or colder than the skin's temperature.
Environmental objects are typically cooler than 30°C, hence cold fibers predominantly relay information about such objects to us.
Nociceptors and Pain Sensation
Introduction to Pain and Nociceptors:
Pain, an unpleasant sensation, begins with signals originating from nociceptors, which are touch receptors responding to various forms of tissue damage or potential tissue-damaging stimuli.
Types of Nociceptors:
Nociceptors can be categorized into two types based on nerve endings:
A Delta Fibers:
Myelinated nerve fibers respond primarily to strong pressure or heat.
Transmit signals rapidly due to their myelination.
C Fibers:
Unmyelinated nerve fibers respond to intense stimulation like pressure, heat, cold, or chemicals.
Transmit signals more slowly compared to A Delta fibers.
Comparison with Non-Nociceptive Mechanoreceptors:
Pain fibers (A Delta and C fibers) are smaller in diameter compared to those from non-nociceptive mechanoreceptors in the skin, such as type A-Beta fibers. (has a wider diameter)
Importance of Nociceptors:
Nociceptors play a crucial role in sensing dangerous objects or stimuli that could potentially cause tissue damage.
Lack of nociceptor function can lead to severe consequences, as seen in diseases like Hansen's disease (leprosy) and diabetes, where the loss of pain sensation results in injury unawareness.
Case Study: "Miss C" - Insensitivity to Pain:
Miss C was born with insensitivity to pain, lacking sensations like pain, sneezing, coughing, gagging, or reflexive eye protection.
She sustained childhood injuries due to the inability to perceive pain, resulting in burns and tongue biting during eating.
As an adult, she faced joint problems attributed to the absence of discomfort, such as standing in the same position for too long.
Miss C's case highlights the significance of pain sensation in preventing injuries and infections, as her lack of awareness led to avoidable health complications and her eventual demise at age 29.
Definitions:
Nociceptors: Sensory receptors transmitting information about painful stimulation causing damage or potential damage to the skin.
A Delta Fiber: Intermediate-sized myelinated sensory nerve fibers transmitting pain and temperature signals rapidly.
C Fiber: Narrow-diameter, unmyelinated sensory nerve fibers transmitting pain and temperature signals at a slower pace compared to A Delta fibers.
Transmission of Touch Sensation from Skin to Brain
Differences in Sensory Pathways:
Visual and Auditory Pathways vs. Touch:
Few optic and auditory nerves, but numerous somatosensory nerve trunks across hands, feet, etc.
Axons in visual/auditory nerves directly reach the brain, while older nerve trunks synapse in the spinal cord initially.
Transmission to the Brain:
Thalamus to Cortex:
Thalamus routes touch data to Somatosensory Area 1 (S1) in the parietal lobe, similar to the primary visual cortex (V1) in vision.
S1 communicates with Somatosensory Area 2 (S2) and motor areas, fostering touch-motor coordination.
Cortical Mapping and Sensory Homunculus:
Spatial Mapping in S1:
Touch sensations spatially represented in S1, forming a sensory homunculus, mapping the body's layout in the brain.
Dr. Penfield's brain stimulation mapped somatotopic representations, unveiling the sensory homunculus concept.
Multiple Sensory Maps and Neuroplasticity:
Varied Sensory Maps:
Separate sensory maps exist in S1's subareas and secondary regions (S2), akin to retinotopic maps.
Neuroplasticity observed in the brain's response to touch; changes in V1 activation during Braille reading demonstrate adaptability.
Phantom Limb Sensation and Somatotopic Confusion:
Phantom Limb Phenomenon:
Missing limb leads to sporadic activity in the corresponding S1 area, creating perceptions of a phantom limb and potential discomfort.
Somatosensory confusion is traced to homunculus idiosyncrasies; altered connections induce sensations in missing limbs.
those neurons are still there and will rapidly fire, hence you will feel something
Neurons don’t move, they are active and have always existing lateral connections in which neighbors can have an influence (create silent synapses)
less activity = lateral connection
see cross-talk across the corpus callosum
Advanced Studies and Concepts:
Object Analysis via Touch:
The division between "what" and "where" systems in touch sensation is observed in higher cortical centers.
FMRI studies show varied brain activation for object recognition and location through touch.
Key Definitions:
Neural Plasticity: Ability of neural circuits to reorganize due to previous activity.
Phantom Limb: Sensation from a physically amputated limb.
Homunculus: Map-like representation of body regions in the brain.
Somatotopic: Spatial mapping in the somatosensory cortex corresponding to events on the skin.
Spinothalamic Pathway: Route from the spinal cord to the brain, carrying skin temperature and pain information.
DCML Pathway: Route from the spinal cord to the brain, transmitting signals from skin, muscles, tendons, and joints.
Somatosensory Area 1 (S1): Primary cortical region for touch reception.
Somatosensory Area 2 (S2): Secondary cortical region for touch reception.
Ramachandran and Leone and Hamilton's Experiments
Ramachandran Observations and Somatosensory Confusion in Amputees:
Phantom Sensations in Amputees:
Amputees often report feeling sensations in phantom arms/hands when their faces or remaining limbs are touched.observations and Somatosensory Confusion in Amputees:
Source traced to a homunculus idiosyncrasy: face-touch area adjacency to hand/arm areas in S1 (Somatosensory Area 1).
Altered connections between face and hand/arm areas cause confusion, attributing face stimuli to the missing limb.
Implications of Homunculus Alterations:
Projections from S1 assist in object and surface analysis in the brain's cortex.
Analogous to vision, touch might exhibit a "what" and "where" division in higher cortical centers.
Studies show varied brain activation in recognizing and locating objects through touch (fmri imaging).
Leone and Hamilton's Experiment on Neural Plasticity:
Neural Adaptability in Touch Perception:
Experiment involved blindfolding normal-sighted volunteers for five days, presenting Braille patterns.
Initially, Braille task activated left S1 (responding to the right side of the body) but later declined, with increased activation in V1 (associated with vision).
Removal of blindfold restored the initial brain activation pattern, highlighting remarkable neuroplasticity in the somatosensory system.
Pain Perception and Processing:
Anatomy and Signal Transmission:
Substantia Gelatinosa: Found in the dorsal horn of the spinal cord, involved in pain modulation.
Dorsal Horn: Receives inputs from skin receptors, and contributes to pain signal transmission.
Pain Signal Transmission and Modulation:
Sensations triggered by nociceptors.
Nociceptive signals arrive at the substantia gelatinosa in the dorsal horn.
Gate Control Theory: Modulation of pain through inhibitory and excitatory connections in the spinal cord.
Interactions in the spinal cord affect somatosensory areas S1 and S2 in the brain. (bottom-up style)
Emotional Aspects of Pain:
Brain imaging studies (PET scans) demonstrated emotional aspects of pain.
Participants under hypnosis experienced hot water stimuli, revealing:
Activation of S1 and S2 by hot water.
Anterior Cingulate Cortex (ACC) responds to suggestions of increased or decreased pain unpleasantness.
Emotional responses involve higher brain regions like the ACC, influencing perceived unpleasantness.
Secondary Pain Effects:
Emotionally associated responses with long-term suffering or recalling painful events.
Prefrontal Cortex involvement in emotional aspects of pain and executive control.
Tickling and Itchiness:
Tickling may involve nociceptors; self-induced tickling leads to reduced laughter due to less somatosensory cortex activity.
Research suggests separate neural systems mediate pain and itch, with limited understanding of itch relief mechanisms.
Examples:
Dread: Associated with the prefrontal cortex, linked to anticipation or recollection of painful experiences.
Secondary pain effects can manifest when painful events are remembered or imagined.
Key Definitions:
Substantia Gelatinosa: Gel-like region in the dorsal horn of the spinal cord involved in pain processing.
Dorsal Horn: Region in the spinal cord receiving inputs from skin receptors, contributing to pain sensation.
Gate Control Theory: Explains pain modulation through spinal cord inhibitory and excitatory signals.
Anterior Cingulate Cortex (ACC): Brain region associated with the perception of pain unpleasantness.
Secondary Pain Effects: Emotional responses related to long-term suffering or recalling painful events.
Prefrontal Cortex: Brain area involved in cognition and executive control.
Nociceptors: Sensory receptors signaling pain due to tissue damage
The Process of Gate Control Theory (Melzack and Wall)
Nociceptors Activation:
Pain signals (bottom-up pain signals) originate from specialized sensory nerve endings called nociceptors, which are activated by various harmful stimuli like tissue damage, extreme temperatures, or intense pressure.
Transmission to Spinal Cord:
These pain signals are transmitted via small nerve fibers (A-delta and C fibers) from the site of injury or stimulation to the dorsal horn of the spinal cord.
transmission cells combine pain signals from the small diameter fibers with signals inhibiting pain produced by stimulation of the large diameter fibers
Gate Mechanism in Dorsal Horn:
At the spinal cord level, the substantia gelatinosa, a region in the dorsal horn, acts as a 'gate'. (moderates)
When pain signals reach this gate, they encounter inhibitory and excitatory interneurons that can either allow the signals to pass through or block their transmission
the dorsal horn regulates pain signals:
Inhibitory and Excitatory Signals:
Excitatory signals from nociceptors stimulate the transmission cells, allowing the pain signals to continue their journey to the brain.
Inhibitory signals from other non-nociceptive fibers (such as larger A-beta fibers related to touch) or downward pathways from the brain inhibit the transmission cells to somatosensory areas S1 and S2
These inhibitory signals essentially 'close the gate', preventing or reducing the transmission of pain signals to the brain.
direct excitatory Pathways from both types of fibers are also found outside of the substantia gelatinosa as with the large diameter fibers the central control excites mechanisms in the substantia gelatinosa that inhibit activation of transmission cells thus decreasing the pain response
Signal to the Brain:
The pain signals that successfully pass through the gate travel along the spinothalamic tract and ascend to higher brain centers involved in pain perception, including the somatosensory cortex.
Brain Processing and Perception:
Once in the brain, these pain signals are further processed in regions like the somatosensory cortex (S1 and S2), the thalamus, and higher cortical areas involved in the emotional and cognitive aspects of pain perception.
Emotional responses and cognitive factors can modulate the perception of pain, influencing its intensity and unpleasantness.
Where It Travels:
Pain signals travel from the site of injury through peripheral nerves to the spinal cord.
Within the spinal cord, the gate control mechanism operates in the dorsal horn, where inhibitory and excitatory signals regulate the transmission of pain signals.
Signals that pass through the gate then ascend to the brain via the spinothalamic tract, reaching various brain regions involved in pain processing and perception.
Pain Modulation and Factors Influencing Pain Perception
Analgesia and Pain Damping:
Analgesia: Decreasing pain sensation without losing consciousness.
Responses to noxious stimulation can be affected by analgesic drugs.
Various factors can attenuate pain sensations:
Anticipation, religious belief, prior experience, or excitement can have attenuating effects on responses to noxious stimulation.
Social influences and interpersonal factors significantly impact the emotional component of pain.
Gate Control Theory and Counter Irritation:
Gate neurons in the spinal cord can dampen pain and be activated by counter irritation or diffuse noxious inhibitory control (DNIC):
Examples include extreme pressure, cold, or noxious stimulation applied to a distant site from the source of pain.
Counterstimulation involves relatively benign stimuli. For instance, rubbing the skin near a mosquito bite can relieve pain by stimulating fibers other than nociceptors, affecting spinal cord neuron interactions. (looking at mechanoreceptors)
Pain-induced analgesia
refers to the body's natural pain-relief response triggered by experiencing pain. It involves the release of natural painkillers, such as endorphins and enkephalins, which bind to specific receptors in the brain and spinal cord, reducing the perception of pain. Essentially, when the body experiences pain, it can produce its own pain-relieving substances to help alleviate the discomfort.
create pain to ignore others (can be emotional or physical)
low-level pain = can tell where the pain is, what it is, how strong it is
high-level pain = in the prefrontal, (ex: i feel anxious) (if this is damaged, then the pain will no longer bother you, no longer represent something unpleasant)
asymbolia shows a distinction between high and low level of pain
Endogenous Opiates and Pain Modulation:
Soldiers experiencing painful wounds post-battle when the stress is over suggest an analgesic effect likely due to endogenous opiates released by the body.
Endogenous opiates block neurotransmitter release or uptake necessary for pain transmission.
Variations in pain responsiveness among individuals might be due to differences in baseline levels of these substances.
Externally produced substances like morphine, heroin, and codeine have similar analgesic effects due to their chemical similarity to endogenous opiates.
Pain Alleviation Medications:
Acetaminophen and ibuprofen alleviate pain by counteracting chemicals that would otherwise activate nociceptors.
Social Influences on Pain Perception:
Research indicates that contact with loved ones reduces brain activation in areas regulating emotions and bodily arousal in response to the threat of painful stimulation.
Studies using fMRI demonstrated reduced neural responses when women held their husband's hands during a threatening task compared to holding an unknown male's hand or no hand at all.
Broader social influences on pain include reports of painful experiences spreading among groups through communication, impacting people's sensitivity to suffering, and providing a collective identification of pain experiences.
Key Definitions:
Analgesia: Decreasing pain sensation during conscious experience.
Endogenous Opiates: Chemicals released by the body that block neurotransmitter release or uptake necessary for transmitting pain sensations to the brain.
Pain Sensitization
Nociceptors and Types of Pain:
Nociceptive Pain:
Nociceptors signal impending or ongoing tissue damage.
Hyperalgesia:
Increased sensitivity triggers heightened pain response post-tissue damage. (to normal painful stimulus)
Inflammatory Pain:
Results from tissue damage, leading to heightened sensitivity but typically diminishes as tissue heals.
Neuropathic Pain:
Arises from nervous system damage or dysfunction without immediate trauma.
Neuropathic Pain Phenomena:
Allodynia:
Non-painful sensory fibers induce pain due to alterations, causing pain from typically non-painful stimuli.
Peripheral vs. Central Changes:
Peripheral changes occur at the skin level, while central changes occur in the dorsal horn of the spinal cord.
Mechanisms at Cellular and Molecular Level:
Understanding neuropathic pain mechanisms at a deeper cellular and molecular level.
Implications of Sensitization Research:
Different Analgesics for Different Pain Mechanisms:
Distinct mechanisms underlying nociceptive, inflammatory, and neuropathic pain—both peripheral and central—require different types of analgesics.
Studies and Research:
Understanding Mechanisms:
Ongoing research aimed at comprehending the cellular and molecular basis of sensitization.
Implications for Medication Development:
No single medication addresses all types of pain; diverse underlying mechanisms necessitate different analgesics tailored to specific pain types.
Pleasant Touch Sensation
Traditional Sensation Classification:
Discriminative Touch:
Tactile, thermal, pain, and itch sensations are categorized as traditional sensations.
Discovery of Pleasant Touch:
Fifth Sensory Component:
Recent scientific classification of a new component is known as Pleasant or Emotional Touch.
CT Afferents:
Peripheral C tactile afferents (CT afferents) mediate emotional properties of non-painful bodily touch.
CT afferents, distinct from pain-related C fibers, prefer slow, light mechanical stimulation (e.g., petting).
Characteristics and Location of CT Afferents:
Preference for Mechanoreception:
CT afferents exhibit a preference for mechanical stimulation, particularly slow, light forces akin to petting.
Hairless Skin Presence:
Research suggests CT afferents are possibly exclusive to hairy skin, and
not found in hairless areas.
Emotional and Neural Processing:
Neural Subsystem for Emotional Responses:
Proposed role of CT afferents as part of a neural subsystem supporting emotional, hormonal, and behavioral responses to skin-to-skin contact, especially with social partners.
Brain Processing of Pleasant Touch:
Discriminative touch is processed in primary somatosensory cortex.
Orbital frontal cortex is involved in processing pleasant qualities of mechanical stimulation, activating in response to both painful and pleasant touch.
Physiological Responses and Psychological Impact:
Endorphin and Oxytocin Release:
Indications that pleasant bodily contacts stimulate endorphin and oxytocin responses, contributing to feelings of well-being, confidence, and calmness.
Studies and Ongoing Research:
Location and Function of CT Afferents:
Ongoing studies to determine the exact location, function, and distribution of CT afferents.
Impact on Emotions and Neurobiology:
Research aimed at understanding the influence of pleasant touch on emotions and its neurobiological basis.
Tactile Sensitivity and Acuity
Historical and Modern Sensitivity Measurements:
Max von Frey's Method:
Developed a technique in the 19th century to measure minimum pressure sensed by the skin using calibrated stimuli like horse and human hairs.
Modern Techniques:
Researchers utilize nylon monofilaments with varying diameters, measuring the skin's sensitivity based on the force needed to buckle the filament.
Variation in Skin Sensitivity:
Differences Across Body Sites:
Data indicates varying pressure sensitivity across different body parts; higher sensitivity observed on the face, followed by the trunk, upper extremities, and lower extremities.
Women generally display higher sensitivity to pressure compared to men across body sites.
Detection of Raised Elements:
Detection Sensitivity:
People can detect a raised dot as small as one micrometer high on an otherwise smooth surface, contributing to detection by FA I receptors.
Texture Sensitivity:
Detection of vibrations caused by many raised dots, even smaller than a micrometer in height, allows differentiation of textures on the skin.
Tactile Vibration Sensitivity:
Vibratory Threshold:
People can detect vibrations from approximately 5 Hertz to 700 Hertz, with the highest frequency tested to date.
Mechanoreceptor Population and Sensitivity:
Detection of vibration at specific frequencies relies on mechanoreceptor populations sensitive to those frequencies.
Psychophysical function for vibration detection involves different mechanoreceptor populations along the skin, each sensitive to distinct frequencies.
Overall Sensitivity and Receptor Contribution:
Frequency and Receptor Sensitivity:
Sensitivity to vibration depends on mechanoreceptor populations sensitive to specific frequencies, contributing to overall tactile perception.
Psychophysical Function of Vibration Detection:
Different mechanoreceptor populations contribute to the overall psychophysical function for vibration detection.
Resolving Spatial Details in Tactile Perception
Two-Point Touch Threshold:
Definition:
The smallest distance at which two stimuli are perceived as separate points rather than a single touch.
low threshold = 2. (higher acuity)
Experimenting with Two-Point Touch Threshold:
Experimental Setup:
Best conducted with a partner to test the two-point touch threshold.
Involves determining the minimum separation at which two touches are discernible.
Factors Affecting Two-Point Touch Threshold:
Receptor Concentration and Receptive Field Sizes:
Determined primarily by touch receptor concentration and the size of receptive fields in the skin.
Higher receptor density and smaller receptive fields contribute to better spatial resolution.
Spatial Resolution in Different Body Parts:
Variation Across Body Sites:
Spatial resolution varies across the body, with extremities like fingertips, face, and toes exhibiting higher resolution.
Psychophysical studies indicate the ability to resolve separations as small as 1 mm on the fingertips.
Determining Two-Point Touch:
Acuity Density and Cortical Processing: (convergence or not)
Aquity depends on a high density of receptors, small receptive fields, no convergence of signals in the cortex,
high convergence = large receptive field,
Requires separate signals sent to the cortex, necessitating adequate receptor density and limited convergence.
Challenges and Alternatives in Two-Point Testing:
Limitations of Traditional Tests:
Subjective nature of determining whether a sensation is perceived as one point or two.
The difference between feeling like one point or two can vary, especially in sensitive areas like fingertips.
Objective Alternatives for Spatial Judgment:
Objective Methods Proposed:
Suggestions for more objective tests, such as judging the presence of gaps in an edge or identifying features of a grating.
Resolving Temporal Details in Touch Perception
Temporal Resolution Testing:
Human Temporal Discrimination in Tactile Perception:
Temporal Threshold:
Subjects can discern a temporal difference as small as five milliseconds between tactile pulses.
Touch perception in temporal resolution performs better than vision (25 milliseconds) but lags behind audition.
Comparative Temporal Resolution across Sensory Modalities:
Temporal Comparison Across Senses:
Auditory perception demonstrates the highest temporal resolution among the senses.
Vision shows lower temporal resolution compared to touch and audition.
Positioning of Touch in Temporal Resolution:
Touch's Position in Temporal Perception:
Touch perception falls between vision and audition concerning temporal resolution.
Touch perception is better than vision but not as refined as audition in discerning temporal differences.
Reliability and Studies on Temporal Discrimination:
Reliability of Temporal Discrimination Testing:
This method serves as a reliable means to assess the human ability to discriminate temporal differences in tactile perception.
Studies consistently demonstrate the ability to detect minimal temporal variations in tactile stimuli.
Haptic Perception
Definition and Components:
Definition of Haptic Perception:
Involves processing inputs from various sensory systems within the skin, muscles, tendons, and joints.
Actively explores and seeks information from the environment.
Components of Haptic Perception:
Derives knowledge of the world through sensory receptors in skin, muscles, tendons, and joints.
Typically involves active exploration and engagement with the external world.
Perception for Action:
Active Exploration and Somatosensation:
Action for Perception:
Utilizing hands for active exploration of external surfaces and objects.
Engaging somatosensation to control precise grasping and manipulation of objects.
Perception for Action:
Leveraging somatosensory information to execute stable and coordinated object manipulation.
Essential for maintaining posture, balance, and executing precise movements.
Complementary Roles of Touch:
Active Touch and Perception:
Active exploration of surfaces and objects outside the body enhances perception.
Leveraging somatosensation facilitates accurate manipulation and stability.
Perception for Action and Sensory Integration:
Employing somatosensation to control object manipulation and maintain body balance.
Touch, in its active and passive forms, crucially supports actions and informs perception.
Studies and Observations:
Studies on Haptic Perception:
Research supports the integral role of haptic perception in active exploration and object manipulation.
Observations highlight the link between somatosensation, active touch, and precise motor control for tasks
Action for Perception: Exploratory Procedures
Exploratory Procedures:
Definition:
Specific ways of feeling an object to gather information about its properties.
Each procedure isn't optimized for precise details of specific properties but aims for general property assessment.
Roughness Perception:
Different processes employed for judging roughness of coarse versus fine surfaces.
Mechanisms in Roughness Perception:
Role of Slow-Adapting Mechanoreceptors (SA I fibers):
Activity of SA I fibers is pivotal in perceiving moderately rough surfaces.
These receptors are highly responsive (10 times more) to relative motion between skin and surfaces compared to static touch.
Sweeping fingers across surfaces generates varying force patterns sensed by SA I fibers, forming a spatial map of skin deformation.
Higher-Level Processing:
Neural structures integrate lower-level information from SA I fibers to estimate surface roughness.
SA I fibers (and potentially FA I fibers) transmit this information for the brain's estimation of surface roughness.
Role of Fast-Adapting Mechanoreceptors (FA II fibers):
Recent studies suggest FA II fibers encode surface roughness for very fine surfaces, especially responsive to high-frequency vibrations.
Scientific results support a dual-coding theory for roughness perception, challenging the concept of a single coding mechanism (Hollins' work).
Experimental Confirmation:
Selective Adaptation Experiment (Hollins' Study):
Used a psychophysical method known as selective adaptation.
Tested the impact of selectively adapting fingertips to intense high-frequency vibrations (250 Hz) on perceived roughness of fine surfaces.
Predicted that adapting FA II receptors to intense vibrations would reduce the perceived roughness of fine surfaces.
Selective adaptation results confirmed the predictions, supporting evidence for a dual-coding mechanism in roughness perception.
Selective Adaptation as a Psychophysical Method:
Offers non-invasive, comprehensive insights into sensory processing.
Helps identify the specific receptors responsible for encoding perceptions of surface characteristics
The Role of Somatosensation in Object Perception
Importance of Somatosensation:
General Functions:
Essential for simple actions (like standing, grasping) and warning signals (pain) for detecting danger.
Value of Somatosensation in Object Recognition:
Material vs. Geometric Properties:
Material Properties: Easy to perceive through haptic (tactile) contact with objects. Crucial in haptic object recognition.
Geometric Properties: More crucial for visual object recognition where physical contact is absent.
Haptic Object Recognition:
Performance:
People excel at haptic object recognition.
Experiment: Subjects identified 100 common objects placed in their hands almost perfectly without visual aid, responding in under 2 seconds.
Information Used:
In haptic perception, physical contact allows easy perception of material properties, which play a critical role in recognition.
Unlike visual recognition, where thermal and textural properties are challenging to perceive without physical contact.
Differences in Recognition Process:
Visual Recognition:
Emphasizes geometric properties. Sparse line drawings are easier to recognize visually.
Limited capability in recognizing raised contours and overall shape when presented haptically.
Haptic Recognition:
Tracing contours with fingers is common for haptic exploration.
Integration of tactile information over time is possible but less efficient; hence, instantly recognizable material properties hold greater importance in haptic recognition.
Conclusion:
Comparison:
Visual recognition relies more on geometric properties, while haptic recognition leans towards material properties due to direct physical contact.
Perceiving Patterns with the Skin
Efficiency of Pattern Perception by Touch:
Efficiency and Limitations:
Pattern perception via touch is not highly efficient, especially for larger patterns.
Small patterns, however, can be perceived, especially by a single fingertip.
Comparison of Tactile and Visual Pattern Perception:
Loomis' Study:
Methodology:
Tested people's ability to identify patterns (Braille symbols, English and Japanese letters, geometric forms).
Presented patterns:
Tactile: Raised elements on the fingertips.
Visual: Presented behind a blurring screen to simulate fingertip resolution.
Findings:
Similar patterns of visual and tactile confusion errors occurred.
Suggested a common decision-making process for both visual and haptic pattern perception.
Limitations in Tactile Field of View:
Tactile Field of View:
Inability to read more than one finger at a time suggests a very narrow tactile field of view.
Two-point thresholds on fingertips are about 1 mm, limiting the number of dots that can be included within the tactile field.
Tactile Agnosia
Definition:
Tactile Agnosia: The inability to identify objects by touch.
Diagnosis and Characteristics:
Lesion Effect:
Lesions in the parietal lobe can lead to tactile agnosia.
Neurologists need to rule out other possibilities before diagnosing tactile agnosia.
has to do with S1 and S2
Case Study:
Patient Description:
A patient unable to recognize objects by touch with the right hand due to a lesion in the left inferior parietal region.
No deficit in object recognition with the left hand.
Reed and Caselli's Study:
Patient could recognize objects visually or with her left hand, ruling out a general loss of object knowledge.
Normal sensory threshold and other capabilities in both hands.
Patient's Abilities and Limitations:
Discrimination of Object Properties:
Patient could discriminate between objects based on weight and roughness using either hand.
Could answer questions about haptic properties of named objects, indicating retained knowledge.
Limitation in Integration or Matching:
Impaired Integration:
Lack of connection between perceived properties and coherent object representation.
Unable to integrate perceived properties into a complete object representation.
Memory and Representation:
Ability to acquire information about object properties and intact haptic knowledge of encountered objects.
Deficit in connecting perceived representation to stored memory representations.
Conclusion:
Integration or Matching Issue:
Inability to integrate perceived object properties or match them to stored representations in memory.
The Where System of Touch: Locating Objects
Haptic Object Localization
Similar to visual and auditory localization, haptic object localization involves determining the location of a haptic stimulus.
Establishment of a frame of reference is essential for haptic object localization.
Frames of Reference in Haptic Perception
Ego Center:
Vision's ego center is near the bridge of the nose between the eyes.
Auditory ego center is between the two ears in the middle of the head.
Lack of Fixed Frame of Reference:
Haggard's analysis revealed no single fixed frame of reference for haptic perception of locations.
Spatial Errors in Haptic Perception
Frame of Reference Definition:
Frame of reference: The coordinate system used to define locations in space.
Egocenter: The center of a reference frame used to represent locations relative to the body.
Kappers' Experiment on Haptic Perception of Tabletop Space:
Kappers demonstrated that orientation judgments of two rods differed by an average of 40° across individuals.
Deviation range varied from 8 to 91°, showcasing considerable discrepancies.
Spatial errors in the haptic parallelism task were significant but consistent.
Subjects tended to judge parallelism based on two spatial frames of reference:
Egocentric frame, centered around the body or hand.
Allocentric frame, relating to external space.
Conclusion
Haptic perception of location involves errors in determining object orientation.
Subjects use multiple spatial frames of reference, including egocentric and allocentric, which leads to significant but consistent spatial judgments.
The lack of a fixed frame of reference in haptic perception results in considerable discrepancies in spatial judgments.
Body Image: Perception of Our Bodies in Space
Changeability of Body Image Perception
Understanding haptic perception of space reveals the high variability of body image, our impression of our bodies in space.
Ehrsson's Illusory Out-of-Body Experience Experiment
Experiment Setup:
Participants wearing VR goggles connected to cameras perceived their body from a stereo view.
Experimenters stroked the participant's physical chest unseen by the cameras and simultaneously stroked a "phantom" chest in front of the cameras.
Results:
Participants reported experiencing an illusion of viewing their own body from behind with their hands located at the camera site.
Sensation of touch on the phantom chest was reported just below the cameras.
Rubber Hand Illusion
Provides further insight into the malleability of body image by simulating an illusion where a rubber hand is perceived as one's own hand.
Iriki, Tanaka, and Iwamura's Study on Tool Use in Japanese Monkeys
Experiment Description:
Japanese monkeys practiced using a handheld tool to retrieve distant food objects for 5 minutes.
Neuroscientific Findings:
Bimodal cells receiving inputs from vision and touch increased their visual receptive fields to include the entire length of the tool, besides the hand.
Suggested Neural Modifications: Represented how the monkey brain incorporated the tool into its body image as an extension of its own hand.
Tactile Spatial Attention
Types of Tactile Spatial Attention:
Endogenous Spatial Attention:
Description: Voluntarily directed attention to a specific location, anticipated based on prior knowledge or cues.
Example Study: Participants predicting tactile stimulation on either left or right hand based on visual cues (pre-cues in the form of arrows).
Observation: Faster responses when pre-cues accurately predicted the stimulated hand. Slower responses when the pre-cue directed attention to the wrong hand.
Comparison to Vision/Audition: Similar to attentional cueing effects observed in vision and audition.
Exogenous Spatial Attention:
Description: Reactively directed spatial attention to a sudden tactile stimulus occurring at a particular location or body part.
Nature: Bottom-up or stimulus-driven attentional control.
Characteristics of Tactile Spatial Attention:
Limited Resource:
Tactile attention, similar to visual and auditory attention, is a limited resource that needs allocation.
Attention Allocation:
Allocation of attention can occur through top-down (endogenous) or bottom-up (exogenous) mechanisms.
Concluding Remarks:
Understanding tactile spatial attention involves the voluntary direction of attention (endogenous) based on anticipation and reactive direction of attention (exogenous) due to an abrupt tactile stimulus.
Studies on tactile spatial attention, like the one involving pre-cued tactile stimulation, show how attentional mechanisms operate similarly to visual and auditory domains, demonstrating allocation effects and cueing responses.
Interactions Between Touch and Other Sensory Modalities
Attentional Competition between Modalities:
Spence, Nicholls, and Driver's Cross-modal Queuing Experiment:
Participants directed to expect a stimulus via one modality but presented with a different modality.
Results indicated faster responses when cues were valid; slower responses when cues were invalid.
Greater cost for invalid cues occurred when expecting touch but presented with visual or auditory stimuli.
Implies touch might have a more restricted attentional channel compared to visual and auditory modalities.
Inter-sensory Integration and Competition:
Lederman, Thorne, and Jones Experiment:
Participants felt different sandpaper surfaces that they believed were the same.
Vision more influential in judging surface roughness, touch more critical in other circumstances.
Rock and Victor's Experiment:
Experiment involving grasping a square while looking at it through a distorting lens.
Illustrated cases where touch and vision influence perception differently.
Ernst and Banks' Study on Sensory Integration:
Demonstrated integration of touch and sight using a virtual display.
Showed perceived height of an object was a weighted compromise between vision and touch.
Relative weighting reflects the quality of signal from each modality.
Complementary Contribution of Modalities:
Newell's Study on Object Perception:
Studied how subjects perceived Lego shapes through vision or touch.
Results indicated memory for shapes was orientation-sensitive.
Observation: Different modalities might efficiently process an object's shape by utilizing complementary sources of information.
The object's front processed better with vision, and its back processed better with touch.
Concluding Remarks:
Interaction between touch and other sensory modalities varies based on the task and information provided.
Studies show instances of competition for attentional resources among modalities and instances of collaboration where different modalities offer complementary information about an object's properties.
This interaction and integration provide insights into how our perception synthesizes information from multiple modalities to form a comprehensive understanding of the environment
Virtual Haptic Environments
Tadoma and Low-Tech Inference:
Tadoma Method:
Used by individuals who are deaf and blind to perceive speech through hand sensations.
Involves spreading fingers across the speaker's lips, jaw, and throat to interpret speech movements and vibrations.
Virtual Haptic Displays:
Inspired by Tadoma, researchers developed devices like the "tactuator" to transmit information from speakers' speech apparatus to the hand of a recipient.
These devices aim to translate spoken words to the hand of a deaf-blind user.
Haptic Feedback in Virtual Environments:
Lack of Haptic Feedback in Current Environments:
Current virtual environments lack haptic feedback, limiting the user's tactile experience.
Development of Haptic Interfaces:
Recent developments include interfaces providing feedback in the form of vibration or sustained forces to the hand.
Applications and Capabilities:
Applications Beyond Gaming:
Virtual haptic environments have applications beyond gaming, such as in medical training and e-commerce.
Use in Medical Training:
Training physicians for minimally invasive surgery by connecting them to surgical tools that are linked to a computer.
The computer simulates patient responses based on the trainee's movements, aiding in surgical skill development.
Commercial Applications:
Potential use in e-commerce by allowing customers to feel products along with visual representation.
Definition:
Virtual Haptic Environment Defined:
A synthetic world that can be experienced haptically by employing electromechanical devices delivering forces to the user's hand.
TENS machines
A TENS (Transcutaneous Electrical Nerve Stimulation) machine is a device that uses electrical currents to alleviate pain. It works by sending low-voltage electrical impulses through electrodes placed on the skin. These electrodes deliver the electrical pulses to the nerves, which can help disrupt or block pain signals from reaching the brain.
Regarding the mechanoreceptors of the somatosensory system, TENS machines primarily work through the gating theory of pain control. This theory suggests that the electrical stimulation provided by TENS can interfere with and modify the transmission of pain signals from reaching the brain.
By activating these mechanoreceptors, TENS can potentially override the pain signals carried by smaller nerve fibers (such as A-delta and C fibers) that transmit pain sensations. This mechanism of action is one way TENS may help in pain relief by essentially "closing the gate" to prevent or reduce the perception of pain.
The slip detection reflex
travels through mechanoreceptors
will group back to muscle then back to hand
rapid and automatic response triggered when our grip on an object starts slipping.
activation of the Fast fast-adapting interneurons (FAI), which are specialized nerve cells that respond quickly to changes in pressure or force.
These FAI detect the slip-through mechanoreceptors
When a slip is detected, the signal travels through these mechanoreceptors to the FAI. The FAI then sends signals back to the muscles involved in the grip, activating them to tighten and regain control of the object.
This reflex pathway works swiftly and helps in preventing the object from slipping out of our hand by quickly adjusting the grip strength.
Comparing S1 and M1
Homunculus Representation
Both S1 (primary somatosensory cortex) and M1 (primary motor cortex) have somatotopic maps (homunculus).
Larger representations exist for highly sensitive or controlled body parts like the hands (large homunculus hands)
S1 Functions
S1 primarily processes sensory information.
Involved in interpreting tactile sensations from the body.
M1 Functions
M1 primarily generates voluntary motor movements.
Controls voluntary movements
Differentiation in Neural Activity
S1: Recognizable patterns in neural activity linked to genital sensation or touch.
M1: More involved in motor control, potentially indirectly related to movements but not specific to gender or sexual characteristics.
S1 = Sensory processing (including genital sensation)
M1 = Motor control (indirectly related to genital movements, but not gender-specific
Tinnitus and phantom pain
Tinnitus:
extreme pain in the ears
usually due to being deaf or developing deafness
so it is a lack of input from the sensory receptors while keeping the central nerves for sound (the same thing happens with phantom limbs)
being deaf what you can hear is neural activity
How to get better at detecting and discriminating textures
with more practice
specific fingertip used will have a cortical area that gets bigger
recruiting more neurons to do some tasks
take over neighboring
TRUE OR FALSE
noise receptor system allows for modulation in top-down processing.
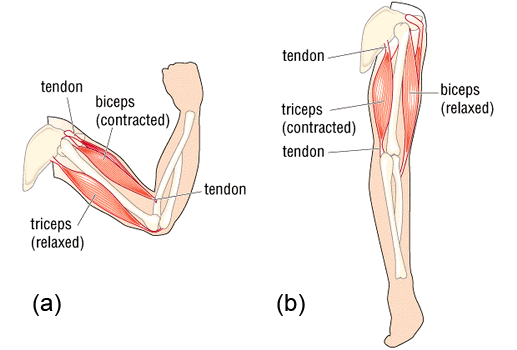
Flexing and Contraction
you flex your joints, not your muscles
muscle tries to make joint flex
muscle trying to shorten in which the joint angle will change
muscles contract not flex
muscle contraction can do both lengthening and shortening (creates tension)
triceps extend the arm
Major reflex (modified muscle)
if muscle gets longer so does this
if muscles get shorter so does this
within tendon itself
if the muscle gets longer, the reflex makes the muscle contract enough to maintain that length
goes right to the spinal cord
what is the role of Golgi Tendon?
They play a role in preventing excessive force on the muscle-tendon unit by causing muscle relaxation when tension becomes too high. This mechanism helps protect the muscle from potential damage due to excessive force.
they initiate a reflex arc that goes directly to the spinal cord, resulting in the relaxation of the muscle attached to that tendon.
Golgi's tendons don’t respond to changes in length but instead, respond to changes in force (respond to increased force and tension)