Pre Lab
💧 KEY FORMULAS TO REMEMBER
1⃣ Drip Rate Formula (drops per minute)
Used when IV is delivered manually via drip chamber
Drops/min = (Volume (mL) × Drop factor) ÷ Time (mins)
🧪 Drop factor = found on IV tubing (gtts/mL)
Microdrip: 60 gtts/mL
Macrodrip: 10, 15, or 20 gtts/mL
🧠 TIP: Always convert hours to minutes (e.g., 8 hrs = 480 mins)
2⃣ Pump Rate Formula (mL/hr)
Used when IV is delivered by infusion pump
mL/hr = Total volume (mL) ÷ Time (hr)
✅ This is the most common calculation on placements and exams!
🧠 Nursing Mnemonic: "Do The Math Right!"
D – Drop factor (check tubing type)
T – Time in minutes (if calculating gtts/min)
M – Multiply volume by drop factor
R – Rate = divide by total time in minutes
🧪 Example 1: Drip Rate
💉 You need to give 1000 mL over 8 hours using macrodrip set (15 gtts/mL)
👉 Formula:(1000 mL × 15 gtts/mL) ÷ (8 × 60 mins)= 15,000 ÷ 480 = 31.25 → 31 gtts/min
⚙ Example 2: Infusion Pump
💉 Order: 500 mL NS over 4 hours
👉 Formula:500 mL ÷ 4 hrs = 125 mL/hr
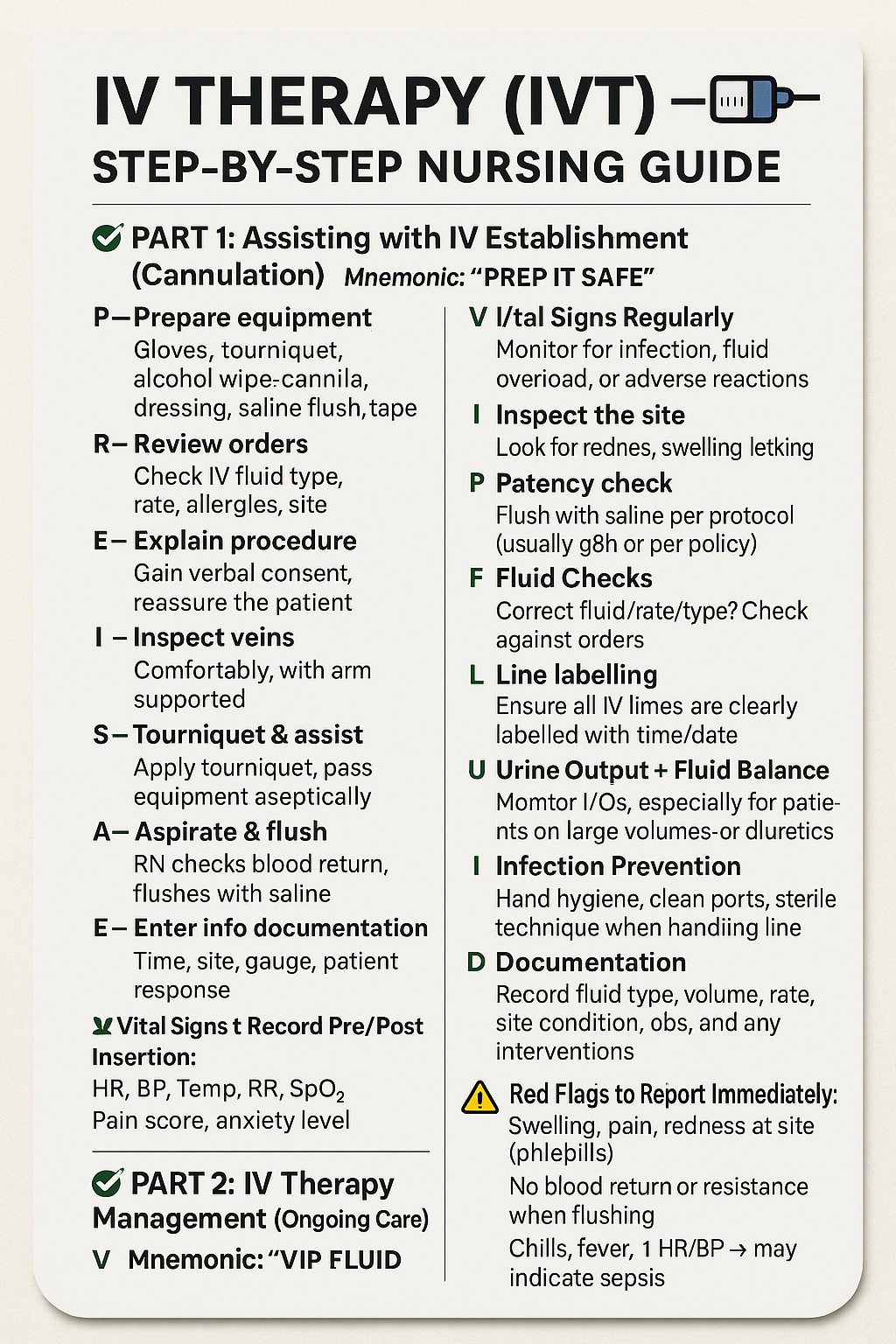
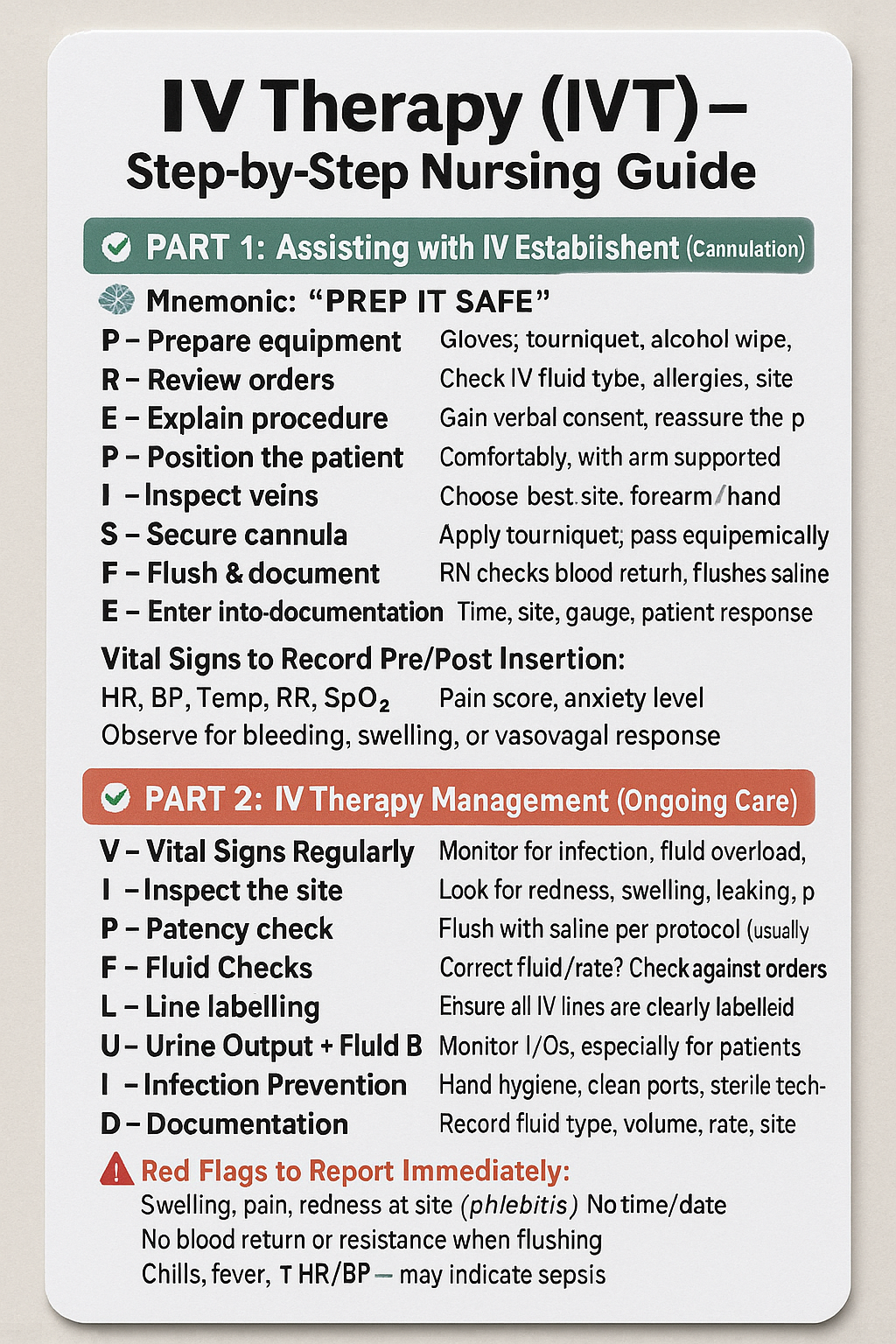
IV Therapy (IVT) – Step-by-Step Nursing Guide
✅ PART 1: Assisting with IV Establishment (Cannulation)
You assist the RN or doctor inserting the IV
🧠 Mnemonic: “PREP IT SAFE”
P - Prepare equipment
Gloves, tourniquet, alcohol wipe, cannula, dressing, saline flush, tape, sharps bin
R - Review orders
Check IV fluid type, rate, allergies, site
E - Explain procedure
Gain verbal consent, reassure the patient
P - Position the patient
Comfortably, with arm supported
I - Inspect veins
Choose best site: forearm/hand preferred
T - Tourniquet & assist
Apply tourniquet, pass equipment aseptically
S - Secure cannula
Secure with Tegaderm/tape, label dressing (date, time, initials)
A - Aspirate & flush
RN checks blood return, flushes with saline
F - Flush & document
Assist with patency check (5–10 mL saline)
E - Enter into documentation
Time, site, gauge, patient response
📋 Vital Signs to Record Pre/Post Insertion:
HR, BP, Temp, RR, SpO₂
Pain score, anxiety level
Observe for bleeding, swelling, or vasovagal response
✅ PART 2: IV Therapy Management (Ongoing Care)
🧠 Mnemonic: “VIP FLUID”
V - Vital Signs Regularly
Monitor for infection, fluid overload, or adverse reactions
I - Inspect the site
Look for redness, swelling, leaking, pain
P - Patency check
Flush with saline per protocol (usually q8h or per policy)
F - Fluid Checks
Correct fluid/rate/type? Check against orders
L - Line labelling
Ensure all IV lines are clearly labelled with time/date
U - Urine Output + Fluid Balance
Monitor I/Os, especially for patients on large volumes or diuretics
I - Infection Prevention
Hand hygiene, clean ports, sterile technique when handling line
D - Documentation
Record fluid type, volume, rate, site condition, obs, and any interventions
⚠ Red Flags to Report Immediately:
Swelling, pain, redness at site (phlebitis)
No blood return or resistance when flushing
Chills, fever, ↑ HR/BP → may indicate sepsis
Fluid overload signs: crackles, ↑ RR, ↓ SpO₂, edema