Infancy and Childhood: Gender Development
Infancy and Childhood Development
Introduction to Gender
Gender development involves multiple stages throughout human life, including prenatal factors, and culminates in adult gender identity.
Prenatal: Chromosomes at conception: Fetal gonads, Fetal hormones
Infancy and Childhood: Sex assignment at birth: Rearing of child boy/girl: Child’s own body image
Hormonal Changes:
Historical Context of Gender Understanding
Prior to 19th Century:
General ignorance on gender; lack of scholarly interest and few substantial case studies existed.
1890s:
Classification of gender based on gonads. Possession of ovaries classified individuals as women regardless of their outward masculine appearance.
1910:
Biopsies were established as definitive measures to determine functional ovaries/testes, although societal classification leaned towards perceived believability rather than biological fact.
1950:
Wilkins and Money introduced the idea of 'sex normalizing' surgeries and hormonal treatments.
Post-1950:
Milton Diamond highlighted severe issues stemming from these practices, noting frequently adverse outcomes.
Biological Sex Variations
Intersexed Individuals:
Defined as possessing biological traits of both sexes.
Genital structures may range between penis and vagina.
The term "hermaphrodite" is outdated and deemed inaccurate.
Occurs in about 2% of live births (Blackless et al., 2000).
Conditions Leading to Biological Variations:
Congenital Adrenal Hyperplasia (CAH)
Swyer Syndrome
Complete/Partial Androgen Insensitivity Syndrome
5-Alpha-Reductase Deficiency
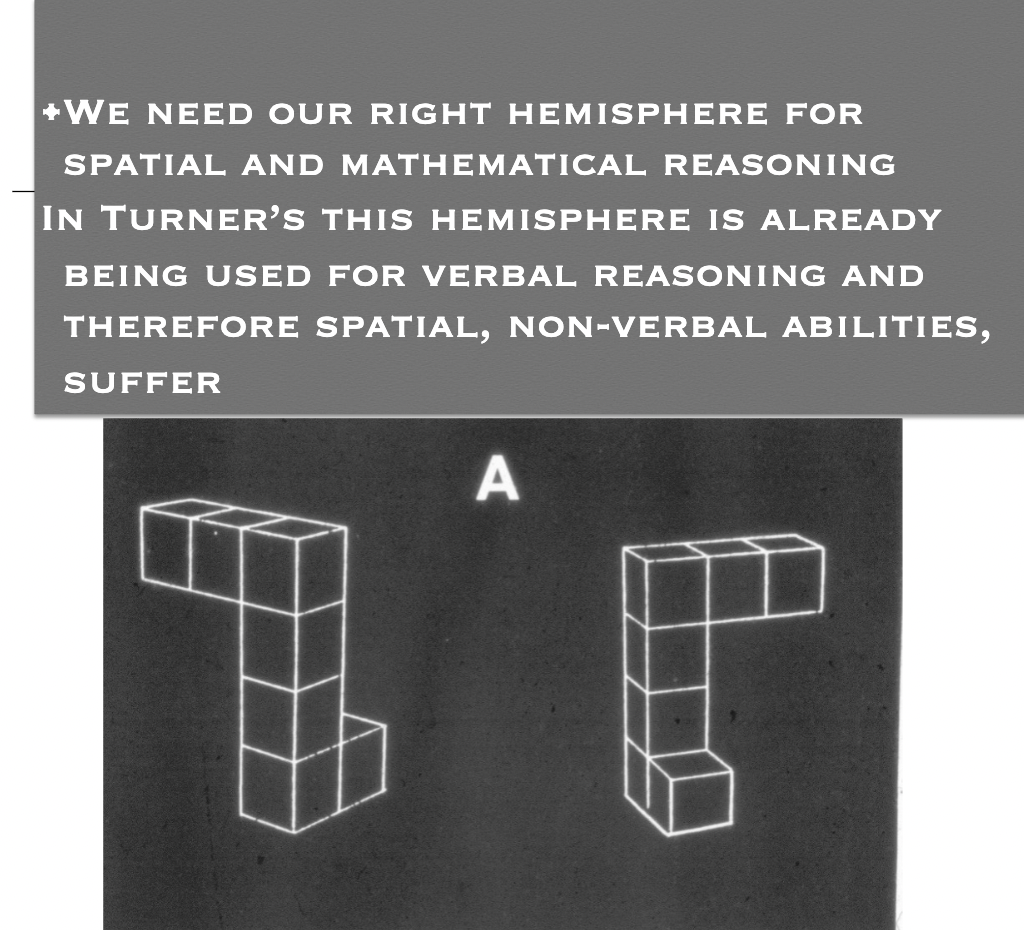
Turner’s Syndrome
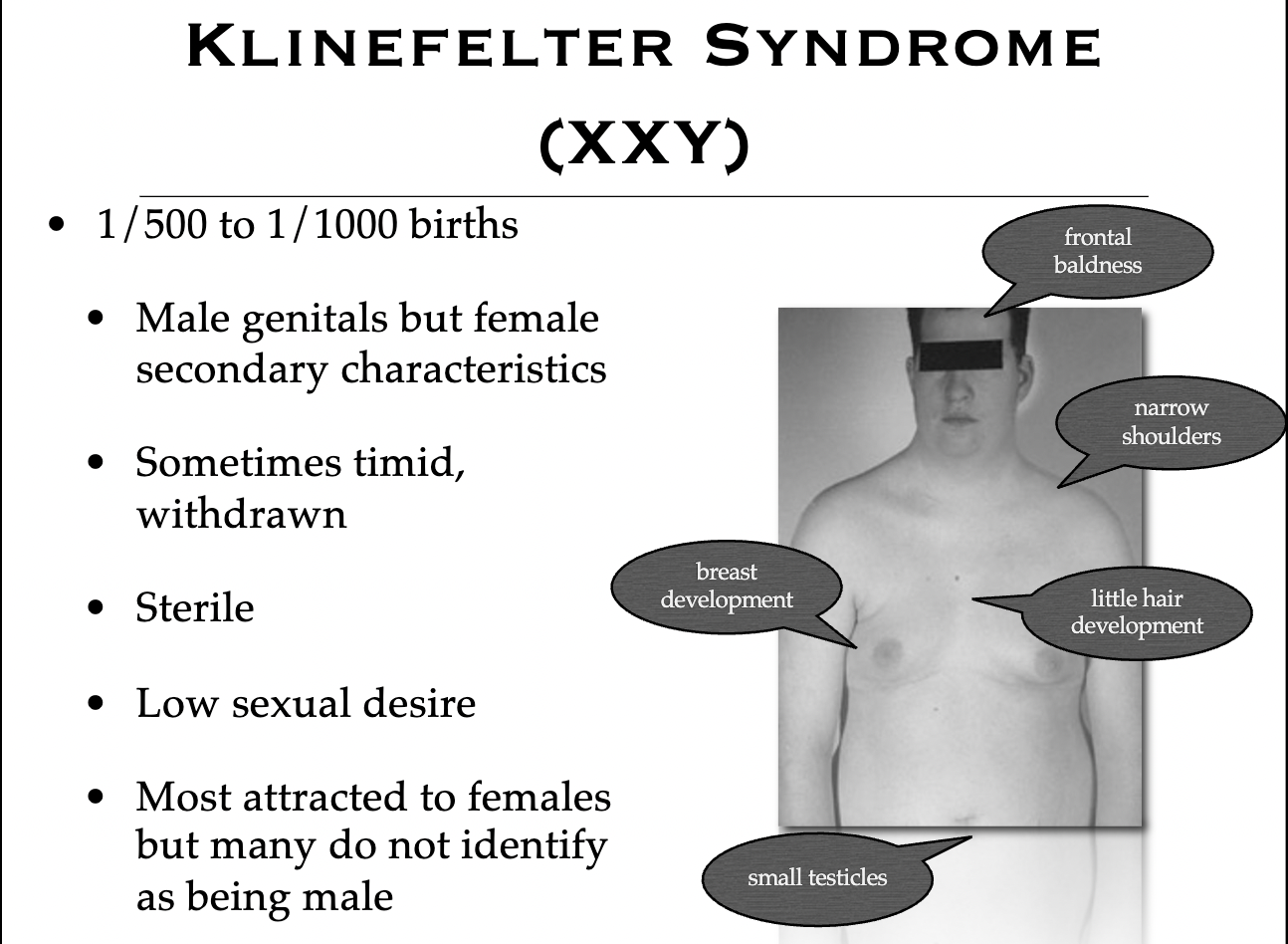
Klinefelter’s Syndrome
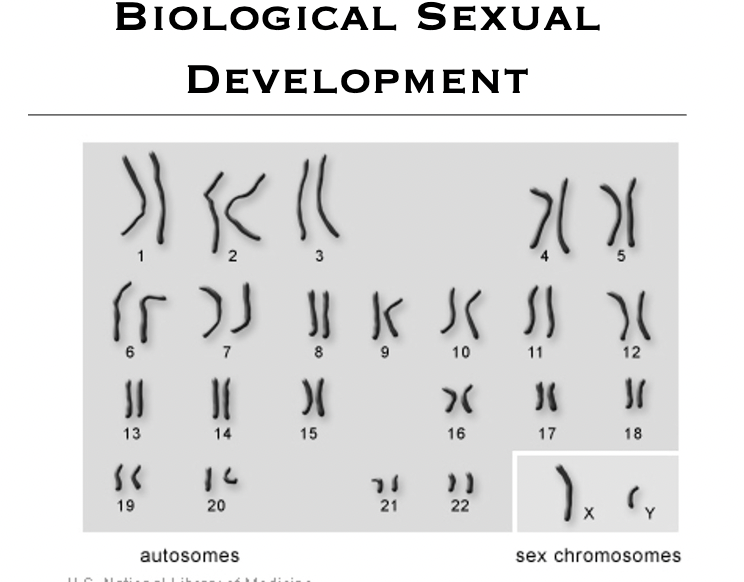
Biological Sexual Development
Carnegie Stages of Human Development:
Key stages range from Zygote (1 day) to week 8+ gestation, highlighting critical phases of development, including sexual differentiation.
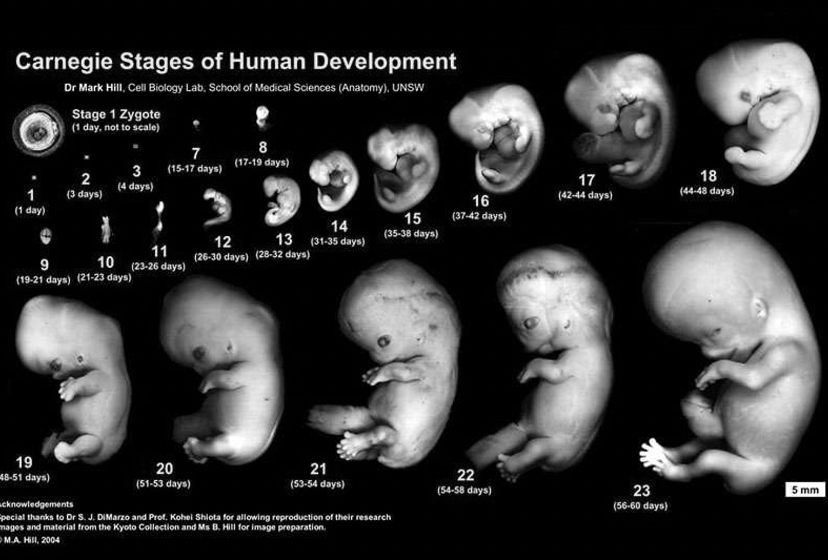
Early Week Development:
By ~3 weeks, a primitive heart circulates embryonic blood.
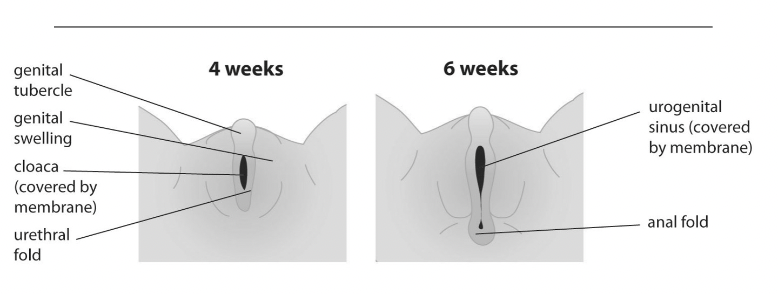
By 5-6 weeks, undifferentiated genitalia form.
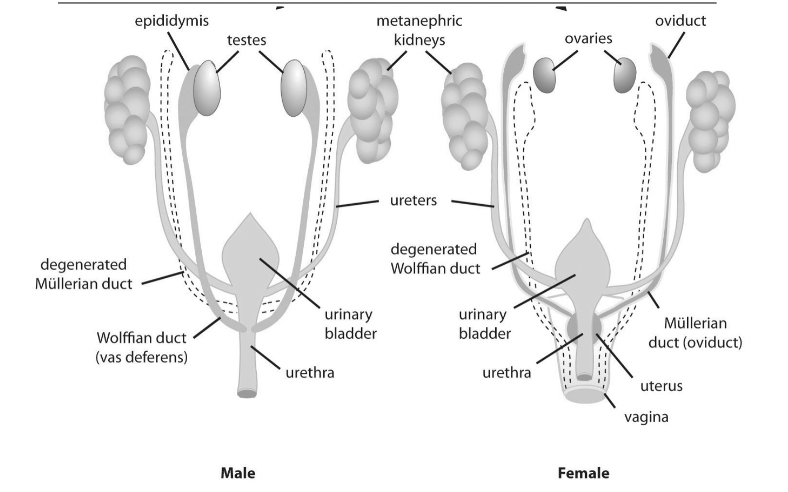
Both male and female embryos exhibit primitive external genitalia, undeveloped gonads, and two sets of primitive ducts: Mullerian (female) and Wolffian (male).
Default Development Pathway:
Both sexes resemble primitive female structure during the frist 6 weeks.
Most mammalian fetal tissues predominantly develop towards female unless interrupted by male hormones.
By the 7th week, genetic coding (XX for female, XY for male) directs sexual differentiation.
Presence of the Y chromosome activates the development of testes; absence leads to ovarian development around weeks 11-12.
Fetal Gonadal Development
Mullerian Ducts:
Develop into female sexual and reproductive organs unless inhibited by male hormones.
Wolffian Ducts:
Develop into male sexual and reproductive organs if male hormones are present.
Specific Biological Conditions
Congenital Adrenal Hyperplasia (CAH):
Results from an inherited recessive gene leading to cortisol production deficiency and overproduction of adrenal androgens.
Between weeks 9-13, excess androgens can cause genital ambiguity in female fetuses.
Affects both XX (female) and XY (male) individuals:
XX individuals may show increased masculine traits.
XY individuals generally follow a typical male developmental pattern.
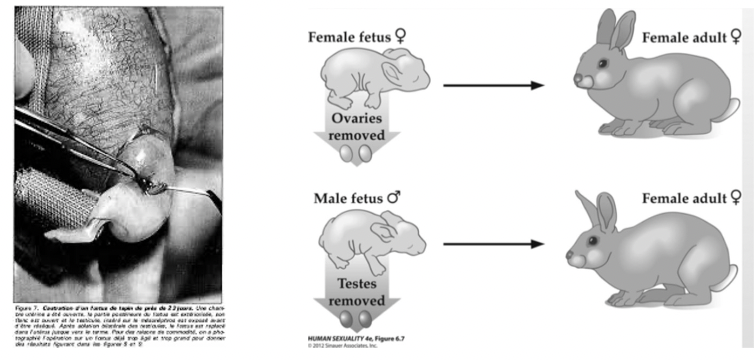
Alfred Jost:
Default pathway of most fetal tissues in mammals is to develop in the female direction.
7th Week: Genetic Code (XX/XY) Asserts itself
Activity on the Y chromosome causes the testes to begin to differentiate.
If the Y chromosome is absent, the ovaries develop and begin to form LATER at 11-12.
Fetal Gonades
Mullerian Ducts:
Embryonic structures that develop into female sexual and reproductive organs unless inhibited by male hormones.
Wolffian Ducts
Embryonic structures that develop into male sexual and reproductive organs if male hormones are present.
Congenital Adrenal Hyperplasia
Inherited recessive gene resulting in a deficiency in the production of cortisol and the overproduction of adrenal androgens.
Between the 9th and 13th week of gestation, excessive androgens negatively affect the female fetus.
Gender ambiguity can result.
CAH can occur in XX and XY.
XY: Physical and psychological development follows a typical male pattern.
XX: become more physically and psychologically masculine.
At birth, genitals appear partially or completely masculine, although internally, female gonads are present.
Masculinization of the female CAH psyche:
Interest in boys’ toys (e.g., vehcles, military accessories) and disinterest in girl toys (e.g., dolls)
Drawings contain boy motifis (e.g., vehicles, mechanisms) rather than feminine (e..g, human, animals).
During adolescence prefer male activites (e.g., martial arts, angliing, looking after motorcylce.)
Masculinization of the female CAH psyche:
Particularly good spatial ability (targeting, maze task).
Less interst in being mothers
5% identify with being male.
In terms of sexuality (CAH females):
Most report attraction to men.
Some studies find higher raes of same-sex attraction and bisexual orientaiton.
Controversial treametn with dexamethasone.
Potent synthetic steroid.
Administered almost as soon as mother is pregnant and before 7th week when humans start to differentitate into m/f.
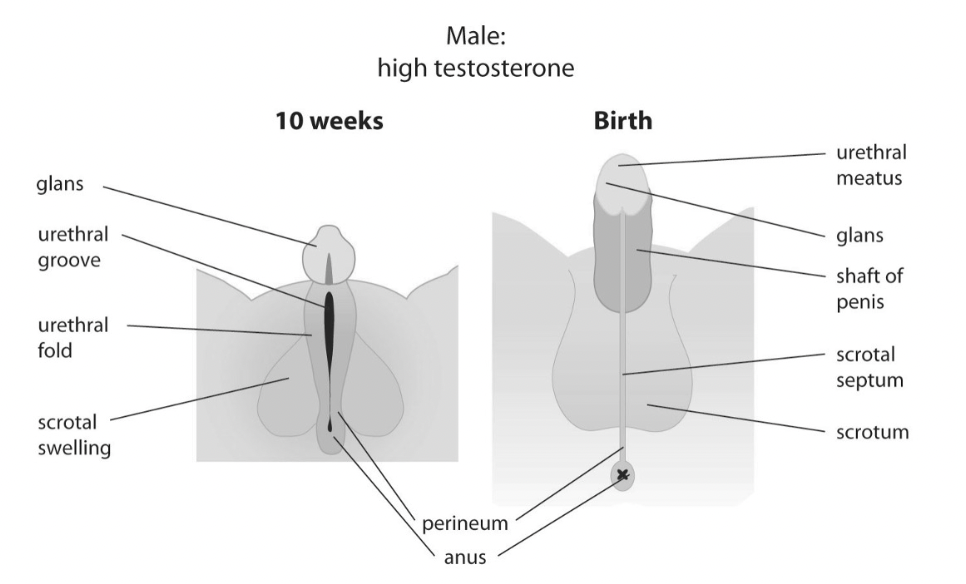
10 Week Male
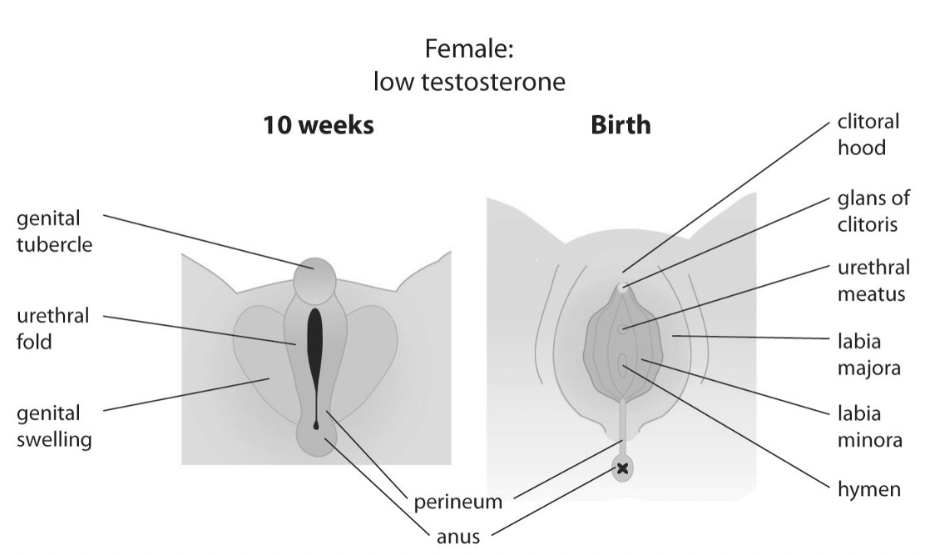
10 Week Female
Biological Sxual Development
Specific region on the Y chromonsomes important for directing sexual development: SRY
SRY gene: causes precursor cells in the embryo to develop into Sertoli cells (produce anti-Mullerian hormone) and Leydig cells (produce testosterone) which cause the gonads to develop into testes.
XY males lacking SRY develop as females (Swyer syndrome)
XX with a misallocated SRY develop as males.
Swyer Syndrome: XY Lacking SRY (Complete 46, XY Gonadal Dysgenesis)
1 in 80,000 births
Genetic male (XY).
The body does not respond to testosterone during development.
Have gondal streaks instead of sex glands. Ovaries are replaced by functionless (fibrous) scar tissue. Consequently, do not produce sex hormones and do not undergo puberty.
Possible female genital appearance at birth (but with undescended testes and an unusually short vagina, and no cervix).
Case Study
15-year-old primary amenorrhea.
Prescribed Estrogen and Progestrone whihc she stopped taking.
Married at 15. Shorter than husband but considerably taller at age 50.
Swyer’s Advocate:
Sara Forsberg
Complete Androgen Insensitivity Syndrome
XY fetus insenstive ot production of its own androgens.
Despite XY, the body and genitals have a feminine genital appearance.
The child appears typical female with a shallow vagina.
Usually not detected until puberty, a failure to menstruate or underdeveloped testicles appears as a mass in the groin or abdomen.
Usually raised as girls and adopt a female gender identity.
Most becomes sexually active, and the majority are attracted to men.
Similarities/Differences
Swyer:
Little or no breast development.
Testes are replaced by fibrous streaks that don’t secrete testosterone.
CAIS:
Normal breast development.
Testes ar eusually well formed and located in the labia or abdomen.
Presence of testis-like masses in a phenotypically female suggests the diagnosis.
ASI Variant Hanne Gaby Odiele:
Born with XY chromosomes and had internal testes surgically removed as a child.
Identifies as intersex and non-binary.
Underwent surgery at 18 to reconstruct the vagina.
Partial Androgen Insensitivity Syndrome
XY male that partially responds to androgens.
Gentials appear to be a mix of male and female structures and not clearly identifiable.
Hypospadias (urethral opening on the underside of the corona).
Can identify as male or female
Sexual attraction is variable.
5-Alpha-Rductase-Deficiency
XY male fetus is unable to convert testosterone to dihydrotestosterone (DHT) due to insufficient levels of 5-alpha reductase enzyme.
DHT is necessary for the development of male external genital structures.
Depending on the amount of feministion they may appear completely female, a mix of male/female structures or incomplete male.
Regardless of external appearanc emale gonads are present internally.
Most 5-alphaRD babies raised as girls and adopt female gender identity during childhood.
But, upon reaching puberty, testosterone production results in masculinization.
Testes descend, genital sturcutre grow into a small penis, and secondary sex characteristics.
Most then switch to male gender identity. Those who do, are typically attracted to women.
Turner Syndrome (XO)
Prevalence: 1/2,500 females births
Female genitalia
Lack of ovaries, menstruation, pubic hair, and breasts with widely spaced nipples.
Stunted growth.
Treatemetn include growth hormones and hormonal replacement therapy
Most identify as female.
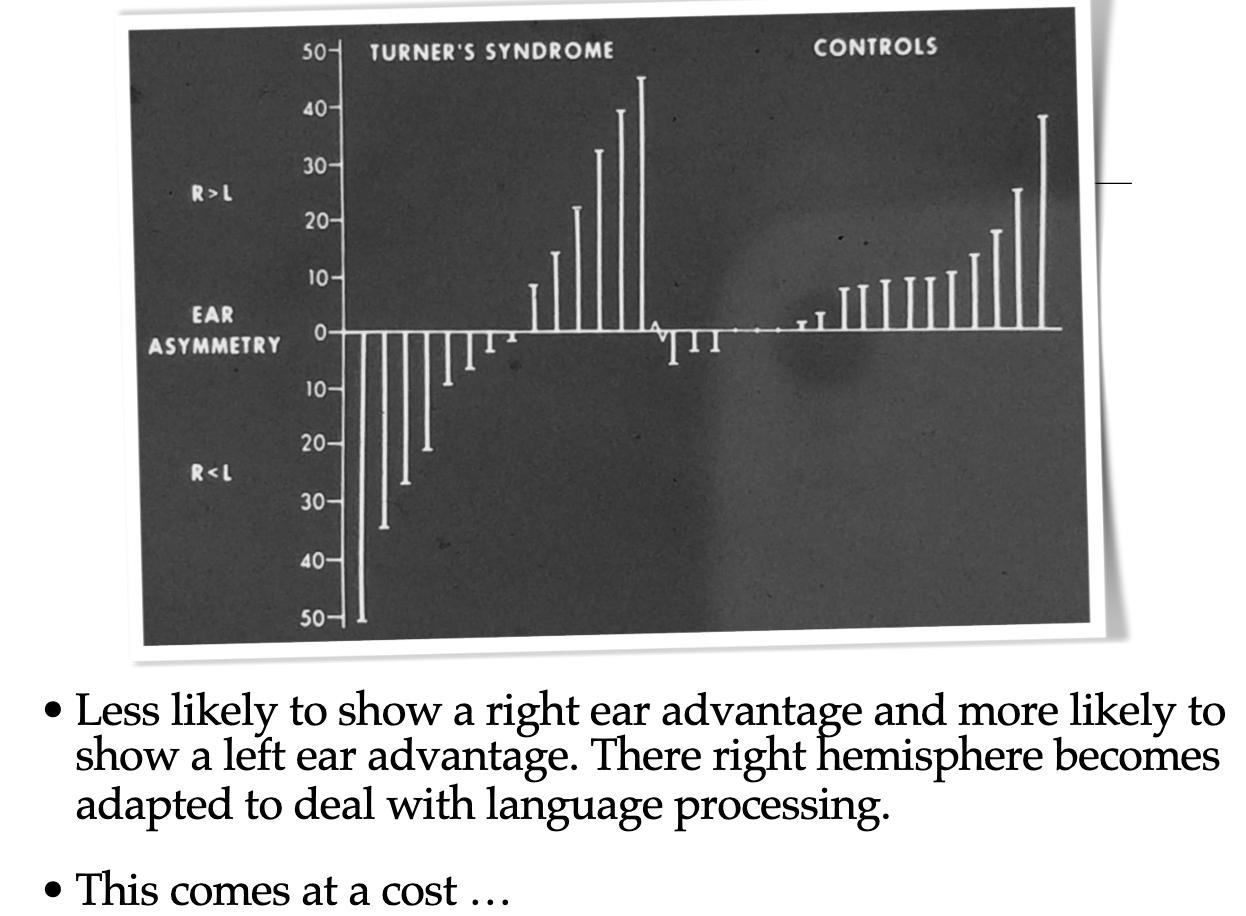
Dichotic Listening Task:
Most people have a left hemisphere dominance for verbal listening.
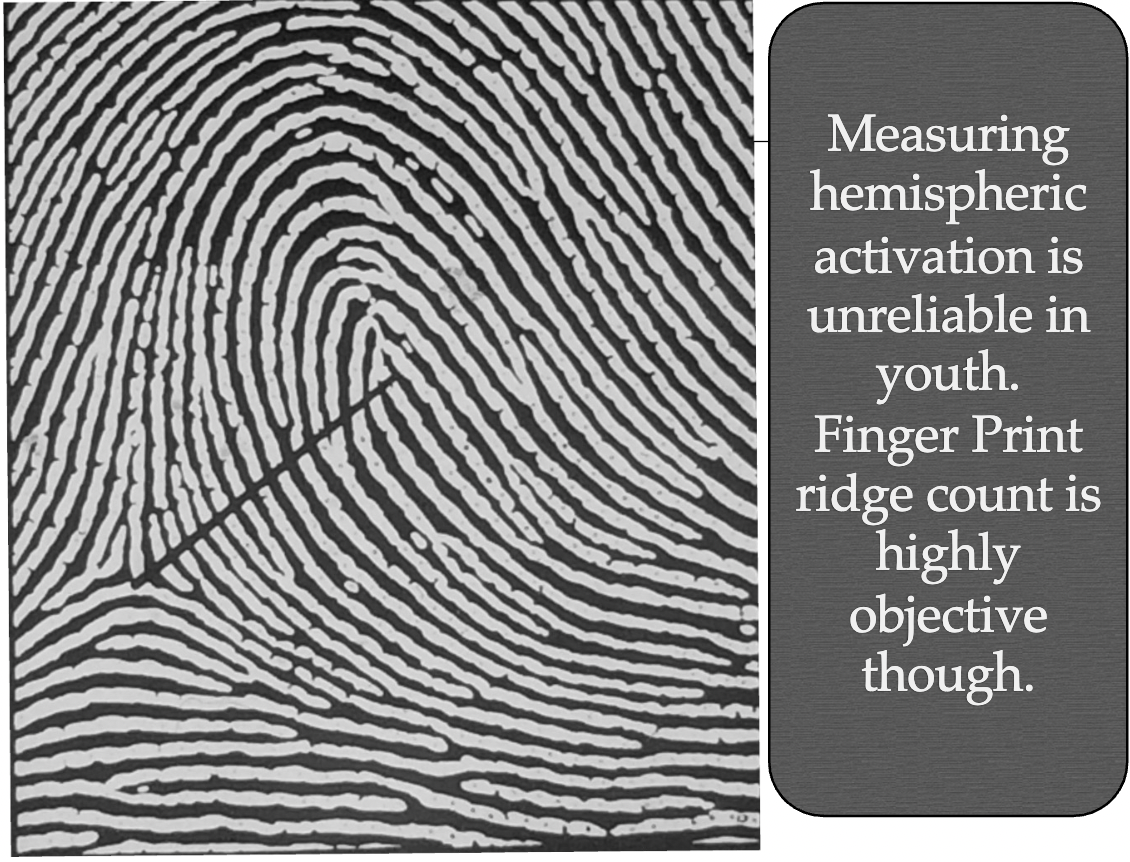
Finger Print Ridge Count:
Low ridge count signifies a slower cell division rate during gestation and results in a smaller left hemisphere development.
Hence, the language deficits are in Klinefelter’s but not Turner’s.
Lower ridege count associated with worse verbal ability.
Dr. C. Netlet Supported 30 Years Later With fMRI
Developments…Less Common
Supernumery Y Syndrome (XYY)
Appearance of a normal male
Tend to be taller stature
Some lack of control over impulses
Usually average intelligence.
Triple X Syndrome (XXX)
Appearance of a normal female
Sometimes infertile
Occasional intellectual impairment.
Biological Sexual Development
Possible True Hermaphrodite (XX/XY)
Exceptionally rare, 5% or less of all intersex conditions. Often reported only in case studies.
Variable. A combination of ovarian and testicular tissue.
Usually have a uterus.
At puberty, most experience breast enlargement and the majority menstruate.
Note the Importance Of Pre-Natal Exposure TO Hormones.
For both 5-alphaRD and AIS we have XY males who do not get the full androgen exposure. But in...
5-alphaRD - result is a male identity
• 5-RD prevents external genitalia from developing BUT the brain is still masculinized
AIS - result is a female identity
the ENTIRE body, including the BRAIN doesn’t respond to androgens and doesn’t have the opportunity to be masculinised
CAH in women and tendency toward mroe masculine traits.
Thus, it may be the impact of the pre-natal hromones that play a role in organising the brain toward certain gener and sexual preferences.