327 Lec 1: Intro
327 Topics in Clinical Psychology
Introduction to Clinical Psychology
Lecture 1:
Instructor: Dr Calum Hartley
Email: c.hartley@lancaster.ac.uk
Affiliation: Lancaster University
327 Overview
Teaching Content
Lectures:
20 x 2-hour in-person lectures (every Monday) with recordings available on Moodle.
Several “special guest” sessions.
- Online discussion forum on Moodle; encourage posting questions.
Core Lectures
Introduction to Clinical Psychology (CH)
Common Conditions & Cognitive Therapy (RHu)
EMDR & Evaluating Therapies (RHu)
Schizophrenia (TC)
Parkinson's Disease (TC)
Alzheimer's Disease (TC)
Autism (CH)
Eating Disorders (RHa)
Critical Realist Perspective on Psychiatric Diagnosis (D. Pilgrim / Southampton; Guest)
Life as a Clinical Psychologist (S. Story / Lancaster; Guest)
Revision session (all staff)
Additional Guest Contributions (Online)
Week 1: Michaela Leeming on “Becoming a clinical psychologist” (Wednesday 8th Oct)
Week 4: Sahir Hussain on “Addiction and community interventions” (Tuesday 28th Oct)
Week 5: Critical Review Clinic (core teaching team; Tuesday 4th Nov)
Week 8: Lettie Wareing on “Theories on the development of anorexia nervosa” (Tuesday 25th Nov)
Expectations
Clinical psychology training spans 3 years, making comprehensive coverage in a 10-week course impractical.
Focus will be on a broad range of topics rather than in-depth analysis.
Subject areas align with core populations in DClinPsy training: children, adults, neuropsychology, and more.
Module Objectives
By the end of this module, students will:
Understand clinical psychology and the role of clinical psychologists.
Be familiar with various aspects of clinical psychological research and practice, including selected forms of psychotherapy/counseling.
Be knowledgeable about prominent psychological conditions affecting core clinical populations.
Reflect on theoretical and professional issues facing clinical practitioners in various specialisms.
Certification Limitations
By the end of the module, students will NOT:
Be qualified to administer psychotherapies!
Assessment & Contact Details
Assessment Components
Coursework:
1 x 1000-word critical review (50%)
1-hr Summer Exam: Write one essay based on core content from weeks 1 to 8 (50%).
Contact Information:
Module Coordinator: Dr Ruth Hurley
Email: r.hurley@lancaster.ac.uk
Coursework Details
1 hour summer exam
- one essay on core teaching content weeks 1 to 8
1000 word Critical Review Assignment:
Critically review one of the four intervention studies listed below, highlighting strengths and weaknesses structured around Summary, Methods, Theory, and Impact on subsequent research.
AMBER level AI use: check specifics
Study Examples:
David, D., et al. (2008). Rational emotive behavior therapy, cognitive therapy, and medication in the treatment of major depressive disorder: a randomized clinical trial, post-treatment outcomes, and six-month follow-up.
Lovaas, O.I. (1987). Behavioral treatment and normal educational and intellectual functioning in young autistic children.
Leff, J., et al. (2013). Computer-assisted therapy for medication-resistant auditory hallucinations: Proof-of-concept study.
Lawrence, N.S., et al. (2015). Training response inhibition to food is associated with weight loss and reduced energy intake.
Critical Review Feedback Criteria
Clarity and accuracy of expression
Clarity and coherence of argument
Depth of knowledge and understanding
Concise summary of key aspects of article (approx. 200 words)
Critical evaluation of methodological strengths and weaknesses
Critical evaluation of theoretical framework and authors' conclusions
Critical evaluation of impact on subsequent research
Breadth of reading beyond target article, including subsequent clinical research
Appropriate use of evidence
Proper referencing (APA 7)
Transferable Skills
Critical Review Skills
Obtain, extract, synthesize, and critically evaluate scientific information.
Conduct literature searches for relevant sources.
Effectively communicate in writing, including drafting, editing, and proofreading.
Work independently and manage time effectively.
Ability to meet deadlines.
Further guidance available on Moodle and during the online Critical Review ‘Clinic’ on Tuesday 4th November (Week 5).
Exam Skills
Communicate and evaluate scientific information effectively under pressure.
Requires discipline, planning, and effective time management.
Lecture Skills
Comprehend complex theoretical and scientific information.
Attentively listen and accurately take notes.
Maintain good concentration.
LECTURE CONTENT STARS HERE
What is Clinical Psychology?
Definition
Clinical psychology is defined as:
“An integration of science, theory and clinical knowledge for the purpose of understanding, preventing and relieving psychologically-based distress or dysfunction and to promote subjective and behavioural well-being” (APA).real world applications of psychological knowledge
Clientele
Clinical psychologists (CPs) work with clients presenting psychological difficulties including all age groups and groups (e.g. families, couples)
Common problems addressed:
Anxiety and depression
Enduring mental illness
Neurological conditions
Addictive behaviours
Developmental conditions
Family relationships
Learning disabilities
Eating disorders
Workplace Locations
Primarily NHS services, also non-statutory mental health providers and private practice.
Levels of healthcare delivery include:
Primary Care: First contact points (e.g., GP surgeries).
Secondary Care: Community or hospital-based services like Community Mental Health Teams (CMHTs) and psychiatric wards.
Tertiary Care: Specialist services for complex needs such as eating disorder wards.
Academia
Roles of Clinical Psychologists (CPs)
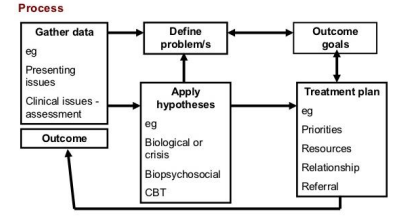
Assessment: Conduct assessments to understand psychological and/or behavioral problems. Involves gathering insights and forming hypotheses, often leading to treatment planning.
CPs are skilled in various assessment types.
Formulation: Use assessment data to develop a therapeutic understanding of clients' difficulties and create treatment plans.
Diagnosis may involve International Statistical Classification of Diseases (ICD-11) or Diagnostic and Statistical Manual of Mental Disorders (DSM-V-TR).
Intervention: Engage clients in therapy to alleviate problems and improve mental health. Formal therapeutic relationships are established with clients.
Evaluation: Assess the ongoing effectiveness of interventions, identifying which approaches yield the best outcomes.
Research: Contribute to the scientific knowledge in clinical psychology. CPs blend practice with research and are viewed as scientist-practitioners.
Other Responsibilities:
Consultation within multidisciplinary teams.
Training and supervision of other professionals.
Teaching new clinical psychologists.
Providing expert testimony in legal contexts.
1. Assessments in clinical psych
Conduct assessments to understand psychological and/or behavioural problems. Involves gathering insights and forming hypotheses, often leading to treatment planning.
Assessment Types in clinical psychology
Clinical Interviews:
Initial contact with service users to gain insight into the client's problems and history. Limitations include low reliability and interviewer bias.
Psychological Tests:
Quantitative assessments evaluating specific characteristics or traits.
Popular tests are standardized – they have been administered to large numbers of people and statistical norms have been established.
The client’s score may also indicate whether they meet diagnostic criteria for a psychological condition
Ensure validity and reliability.
Types of Psychological Tests
Standardized Tests:
Administrated widely to create normative data, allowing practitioners to identify where a client falls on the distribution of scores.
Personality Inventories:
Describe patterns of behaviour, thoughts and feelings.
Such as the Minnesota Multiphasic Personality Inventory (MMPI), which assesses multiple dimensions of psychological functioning through self-statements.
The questions relate to mood, physical concerns, social attitudes, psychological symptoms and feelings of well-being.
Also contains items that allow the clinician to estimate whether the client is providing false information.
Specific Trait Inventories:
Focus on specific psychopathologies. Hone in one one specific psychological functioning e.g. measuring individual differences in autistic traits
e.g., Obsessive Belief Questionnaire : assesses beliefs and appraisals considered critical to the acquisition and maintenance of obsessions: 1. Intolerance of uncertainty 2. Overestimation of threat 3. Control of thoughts 4. Importance of thoughts 5. Beliefs about responsibility 6. Perfectionism
Projective Tests:
A set of ambiguous stimuli are presented for the client to interpret in their own way.
The objective is to reveal unconscious psychological dynamics such as motivations and perceptions of the self and the world.
Often substantial variation between clients’ responses and clinicians’ interpretations.
Popular examples include the Thematic Apperception Test, the Sentence Completion Test and the Rorschach Inkblot Test.
E.G Rorschach Inkblot Test
-Ink dropped on paper and client is times and asked what they see
- 10 official inkblots and clinicians interpret responses using a structured scoring system (e.g. Exner & Weiner, 1995) that provides personality norms and indicators of psychopathology.
E.G Sentence Completion Test
-Clinician provides the first half a sentence and client must finish it
-“my father”, “I feel”
Intelligence Tests:
Measure a client’s IQ in comparison to a population of people with similar characteristics (e.g. age or education).
Most have a M of 100 and an SD of 15-16; 68% of the population score between 84-116 and approx. 2-3% score <70.
Intelligence tests are used by CPs for a number of purposes:
Diagnose intellectual & learning disabilities.
Identify specific areas of need.
Research
help diagnose specific areas of need and learning disabilites
Neurological Impairment Tests:
Identify psychopathologies caused by damage to the structure and functioning of the brain or CNS rather than problematic life experiences or dysfunctional thinking.
Neurological damage can be caused by traumatic injury (e.g. car accident), cardiovascular problems (e.g. stroke), cerebral infection (e.g. meningitis), a brain tumour, or a degenerative brain condition (e.g. Alzheimer’s disease).
CPs employ a battery of tests, including EEG, PET and fMRI scans and blood tests.
Measure cognitive, perceptual and motor performance indicate underlying brain dysfunction (Rao, 2000).
Different psychological functions are localised in different areas of the brain, so discovering a specific cognitive deficit can help identify which brain region is damaged.
Clinical Observations
In addition to conducting psychological tests, CPs need to assess behaviour in its natural context (e.g. home, classroom, community setting).
Involves recording behaviour frequencies and allows identification of events that trigger (precede) or reinforce (follow) problem behaviours.
Excellent ecological validity and can suggest workable solutions. However, training takes time, behaviour can be context specific, and raters may code behaviours differently.
2. Formulation
Information generated through assessment is used to formulate an understanding of the client’s difficulties and develop a treatment plan.
The medical approach is to establish a diagnosis using the International Statistical Classification of Diseases and Related Health Problems (ICD-11) or the Diagnostic and Statistical Manual of Mental Disorders (DSM-V-TR).
- They describe categorical conditions that can be identified by set lists of criteria. The practitioner will work out whether the client’s symptoms meet criteria for a specific condition in the DSM or ICD.
Many CPs believe that each client’s problems are unique and thus require an individualised approach (Persons, 1989).
In collaboration with the client, the CP will develop a precise psychological account of their problems (not imposed on them like a psychiatric diagnosis)
They will establish goals and methods for change with client
Persons’ (1989) 6 formulation components:
1. Create a list of the client’s problems.
2. Identify and describe the underlying psychological mechanisms that might be mediating these problems.
3. Understand the way that these psychological mechanisms generate the client’s problems.
4. Identify the events that may have precipitated the client’s problems.
5. Identify how these precipitating events may have caused the current problems through the proposed psychological mechanisms.
6. Develop a treatment plan based on these explanations and predict any obstacles.
5 advantages over diagnosis/medical approach (Tarrier, 2006):
1. Flexible and idiosyncratic understanding of each client’s problems irrespective of diagnostic labels. Focus on the person not that label
2. Collaborative, treats the client with regard.
3. Based on a theoretical understanding of causal psychopathology (diagnosis is based on description of symptoms).
4. Can include information about a client’s history and their personal, social, and familial circumstances.
5. Allows development of treatment strategies that are moulded to the individual’s needs.
3. Intervention
Involves using a psychological model or therapeutic approach to facilitate the relief of problems.
Involves a formal relationship between the CP and client(s) – an individual, couple, or family.
Employs a set of procedures intended to form a therapeutic alliance, explore the nature of psychological problems, and encourage new ways of thinking, feeling, or behaving.
The nature of intervention will differ depending on the CP’s theoretical affiliation and specific training.
Intervention Types
Psychodynamic:
“Psychoanalysis” – based on the work of Sigmund Freud (1856-1939).
Assumes that unconscious conflicts (the cause of psychopathology symptoms) develop early in life, and psychodynamic interventions aim to identify these events.
E.g a childhood trauma has shaped the way a person is in adulthood because of unconscious mechanisms
Once identified, the CP will help the client to acknowledge these conflicts, bring them to conscious awareness, and develop strategies for change.
Techniques: Free association, transference, dream analysis
Behavioural:
In the 1940s and 1950s, there was growing dissatisfaction with the unscientific psychodynamic approach.
Many psychologists turned to behaviourism for objective knowledge that could inform conceptualisation and treatment of psychopathology.
Wanted to make psychology more quantifiable
Turning psychological experiences into numbers and scores to be easier understood.
Numerous psychological conditions were the result of “faulty learning” and symptoms were acquired through simple conditioning processes.
For example, anxiety symptoms could be acquired through classical conditioning, and behavioural problems could be acquired through operant conditioning.
E.G little albert learned fear/ anxiety through classical conditioning
Behavioural interventions use conditioning principles to “unlearn” problematic associations and behaviours.
Techniques: Flooding, systematic desensitisation, exposure therapy, aversion therapy, functional analysis.
Cognitive:
Current most popular model of psychopathology; 28% of CPs identify with this approach (Norcross et al., 2005).
CBT is a very popular form of therapy
Believe that some psychopathologies are caused by dysfunctional thinking about the self or the world, or dysfunctional processing and interpretation of incoming information.
Aim to confront these thoughts and solve them. Aim to rationalise these negative thoughts e.g. discuss catastrophising
For example, anxiety conditions are characterised by a bias towards processing threatening information and interpreting ambiguous information negatively.
Cognitive treatments try to change dysfunctional processing in order to relieve related psychopathology. A popular and varied therapeutic approach is Cognitive Behavioural Therapy (CBT).
A CBT intervention often has the following characteristics:
1. The client keeps a diary noting how events, feelings, moods and thoughts co-occur.
2. The CP helps the client to challenge irrational, dysfunctional or biased thinking.
3. At home, the client is instructed to test the rationality of their thoughts via behavioural experiments.
4. The client is trained to think, behave and react differently in situations that evoke their psychopathology.
Train the client to think differently by challenging irrational thoughts using logic and reasoning. Could be done by asking questions about a situation that a patient was asking about to help challenge and disprove a worst case scenario
Family Systems/Family Therapy:
Addresses psychopathology resulting from relationships within the family.
It views the family as a social system. It seeks to identify the complex relationships and alliances that exist between family members, and re-mould these into those expected in a well functioning family.
Usually involves ensuring the primary relationship in the family – between the two parents – is strong and functional (Minuchin, 1985).
4. Evaluation
Continuous assessment of the effectiveness of an intervention and the client’s ongoing needs.
Which treatment approaches are most effective?
Several studies have shown that most common therapies do not differ in their effectiveness, but are all more effective than “placebo” and “no treatment” conditions (Gibbons et al., 1993; Smith et al., 1980).
Common themes between therapies include: a strong bond between CP and client, clear communication, a positive mindset
“Dodo Bird Verdict”
5. Research
CP’s as “scientific practitioners”
Widely held view that CPs should be scientist-practitioners: applied scientists with expertise in research and therapeutic practice. • Most clinical training courses are based in University psychology departments and involve substantial research components. •
Current view in the UK is that research methods and findings should be systematically integrated into clinical work (Barker, Pistrang & Elliott, 2002).
Mental health services are increasingly required to provide scientific evidence that treatments are effective.
In the UK, the National Institute for Health and Care Excellence (NICE; see link to NICE webpage) recommends treatments that are “evidence-based” – their efficacy has been demonstrated through scientific research.
Many forms of therapy are not amenable to assessment through traditional scientific methods (e.g. psychoanalysis).
Types of Research Designs
Correlational Designs:
Very common; determine whether there is a statistically significant relationship between variables.
Examples: - Is trait anxiety associated with worrying? - Is body dissatisfaction associated with excessive dieting? - Is the drug availability associated with substance abuse?
Does not imply a causal relationship or explain why the variables are related.
Longitudinal Designs:
Measures the same participants on two or more occasions to specify time relationships between variables.
As measurements are taken at Time 1 and Time 2, it is possible to identify concurrent and longitudinal predictive relationships between variables.
For example, does body dissatisfaction in childhood predict harmful eating behaviour during childhood (Time 1) and/or adolescence (Time 2). Indicative of causal relationships.
Experimental Designs:
Typically a large-scale survey that provides descriptive details about the prevalence of psychological conditions.
Can identify what factors correlate with a specific condition, whether it is more prevalent in a particular group (e.g. men vs. women, young vs. old), associated risk factors, and whether incidence rate is increasing or decreasing.
Require a large sample that is representative of all types of people in the specified population.
Involves recording how the manipulation of a variable (e.g. mood) influences an outcome measure (e.g. worrying).
Enables the determination of causal relationships and the direction of causal effects.
Vital to developing theories and models about the aetiology of psychopathologies (Field & Davey, 2005)
Mixed Designs:
Experimental study in which participants are NOT randomly assigned to conditions.
If we wished to discover whether negative mood caused anxious individuals to worry more than depressed individuals, we would ensure that one group contained only anxious individuals and another group contained only depressed individuals.
Used frequently to assess the effectiveness of a particular intervention on people with different psychiatric diagnoses.
Qualitative Methods:
Rather than numbers, the data for qualitative research is often language (e.g. a participant’s description of themselves, their feelings, thoughts about the world, emotions etc).
Participants are selected based on the psychopathology or phenomenon of interest (e.g. sufferers of childhood abuse, parents of autistic children etc; Cresswell, 1998).
Data usually collected in a semi-structured, open-ended interview (Kvale, 1996). The researcher tries to interpret the transcript, picking out consistent themes and deciding how these themes relate to their research question.
Natural Experiments:
Data collected in non-laboratory contexts following natural events (e.g. large scale disasters & pandemics). • Griensven et al. (2006) found that survivors of the 2004 tsunami in Thailand exhibited increased symptoms of PTSD, anxiety and depression. • Weems et al. (2007) found that PTSD symptoms in children after Hurricane Katrina were highest in those with previously high trait anxiety.
Single Case Studies:
Most employ an “ABA” design:
1. An initial baseline stage involves measurement of behaviour prior to intervention (A).
2. Next comes a treatment stage where the experimental manipulation is introduced and its effect on behaviour is measured (B).
3. Finally, a second baseline stage is included to assess effect longevity and ensure changes at B were not random (A).
One individual is both an experimental and control participant. Enables inferences about causal relationships.
6. Other responsibilities
Consultation; provide psychological perspective as part of a multi-disciplinary team.
Supervision & training; train other professionals in specific psychological assessments and interventions.
Teaching; contribute to training of new clinical psychologists as part of a DClinPsy programme.
Expert testimony; offer scientific expertise in legal contexts.
Becoming a Clinical Psychologist
Training Pathway in the UK
31 universities offer NHS-funded Doctorate in Clinical Psychology (DClinPsy) degrees, all accredited by BPS & HCPC.
Duration: 3 years of full-time doctoral level training (academic, clinical placements, and research).
Position: Paid as a “Trainee Clinical Psychologist.”
Competitiveness: Highly competitive; 5910 applicants vied for 1179 places in 2025 (20% success rate).
Academic Qualifications for DClinPsy
BPS Graduate Basis for Chartered Membership.
Minimum 1st or 2:1 class degree in Psychology; lower class degrees may be accepted with additional qualifications.
Optional: Relevant MSc, which can enhance applications by providing specialization.
Optional: Relevant PhD for the highest qualification and additional experience.
Relevant Experience for DClinPsy Application
Must include voluntary or paid work with vulnerable populations, ideally before applying; this strengthens CV and gives firsthand experience.
Application Process
Apply through the Clearing House webpage.
Select multiple institutions in a single application.
Multi-stage selection process including tests, presentations, and role plays.
Additional Resource Recommendations
Books and Websites
Books:
"How to Become a Clinical Psychologist" by Alice Knight
"Clinical Psychology for Trainees" by Andrew C. Page and Werner G. K. Stritzke
"Clinical Psychology: An Introduction" by Alan Carr
Websites:
BPS Division of Clinical Psychology
Clearing House for Postgraduate Courses in Clinical Psychology
Clinical Psychology Forum
Conclusion
Overview of the module, including expectations around clinical psychology and the pathways towards becoming a clinical psychologist.
Next Lecture Preview
Topic: Common Psychological Conditions & Cognitive Therapy
Instructor: Ruth Hurley
Date: To be determined.