Anterior Segment Trauma
Overview of Ocular Trauma
The eye is protected from direct injury by:
Eyelids
Eyelashes
Projecting margins of the orbit
Various causes of ocular injury include:
Chemicals
Heat
Radiation
Mechanical Trauma
Importance of Ocular Trauma
Ocular trauma is the number one most important ocular emergency.
It is the leading cause of blindness, with around 40% of cases being monocular blindness, affecting individuals regardless of age, sex, or geographic location.
Males and younger individuals are at a higher risk.
Efficient referral and management by ophthalmologists are essential.
Prophylaxis is always preferred over treatment (wearing eye protection)
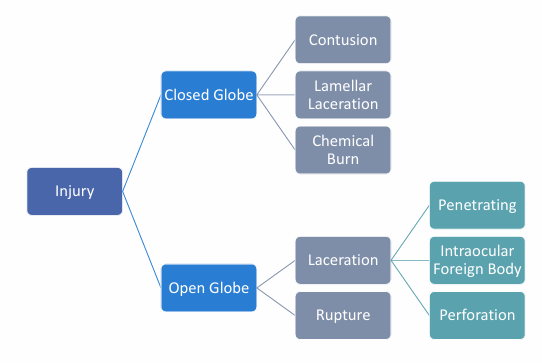
Classification of Trauma
Closed Globe: No full-thickness wound of eye wall, but there is intraocular damage
Open Globe: Full thickness injury of the eye wall and the intraocular structures
Contusion: result of direct energy delivery to the eye, by a blunt object. Injury may be at the site of impact or a distant site
Rupture: Full thickness wound of the eyeball, caused by a blunt object
Lamellar laceration: partial-thickness wound of the eye wall
Laceration: full-thickness wound of the eye wall by a sharp object
Penetrating injury: an injury where a foreign object has been embedded in the eye. Usually full thickness with a site of entrance
Perforating injury: full thickness injury, with both entry and exit wounds
Classification based on nature:
Physical trauma: perforating, non-perforating
Chemical Trauma: acid, alkali, dye (salt)
Ocular Injuries Overview
History Taking in Eye Injuries
Document a detailed history to assess:
Time and nature of injury
Past ocular history
Immunization history (e.g., Tetanus)
Rule out globe-threatening injuries
Examination of both eyes
Necessary documentation and, if possible, photographs
Timely referral to specialists
Assessment Pitfalls
Common pitfalls in assessment:
Failing to ascertain the mechanism of injury can miss serious injuries.
Not everting the upper eyelid can miss foreign bodies.
Attempting to remove foreign bodies in cases of suspected open globe injury.
Reduced concern if no red eye in chemical injuries can lead to limbal ischaemia being overlooked.
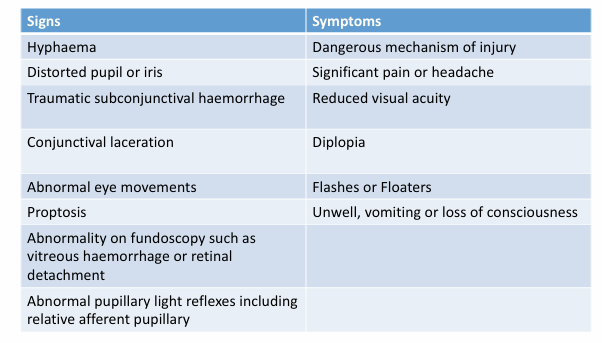
Red Flags in Eye Injury
Signs and symptoms indicating severe damages:
Hyphaema
Distorted pupil or iris
Significant pain or headache
Traumatic subconjunctival hemorrhage
Reduced visual acuity
Conjunctival laceration
Diplopia and abnormal eye movements
Flashes or floaters
Proptosis and associated systemic symptoms such as vomiting or loss of consciousness
Abnormalities upon fundoscopy (e.g., vitreous haemorrhage)
Abnormal pupillary light reflexes
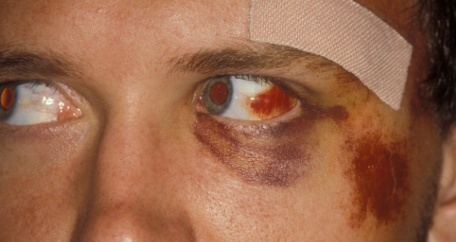
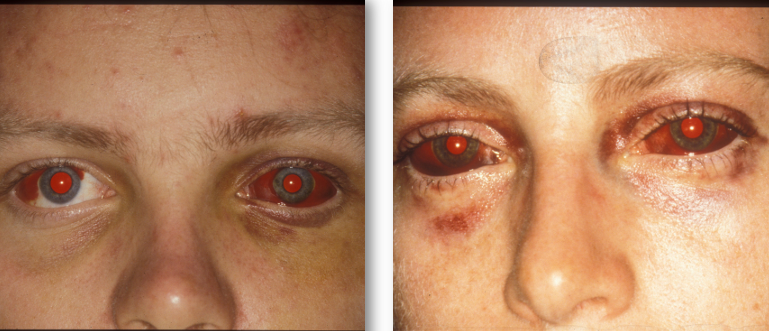
Haematoma / Ecchymoses
Typically referred to as a “black eye”, often resulting from blunt trauma to the eyelid or forehead.
Usually innocuous but must be monitored for associated globe or orbit injuries:
Orbital roof fracture: Can cause black eye + subconjunctival hemorrhage (SCH) without posterior limits.
Basal skull fracture: Can cause bilateral “ring” haematomas (panda eyes).



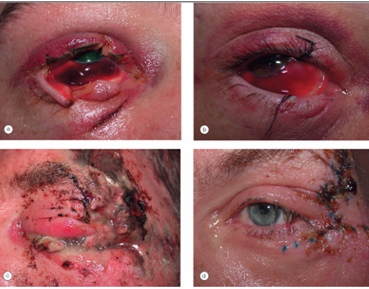
Eyelid Lacerations
Lacerations can be classified as:
Superficial Lacerations
Lid Margin Lacerations
Lacerations with Mild Tissue Loss
Lacerations with Extensive Tissue Loss
Canalicular Lacerations
Surgical repair may be required.
without surgery it may result in a notching of eyelids which can predispose to corneal exposure, ulceration and infection
Consider the potential for globe trauma with penetrating injuries.
Require protective eye shield and immediate emergency transport.
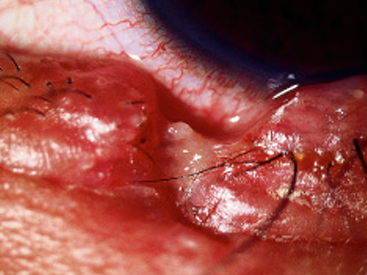
Canalicular Lacerations
very delicate area that is prone to tearing
silicon stents used to keep open (more difficult to create a new cuniculus if it scars)

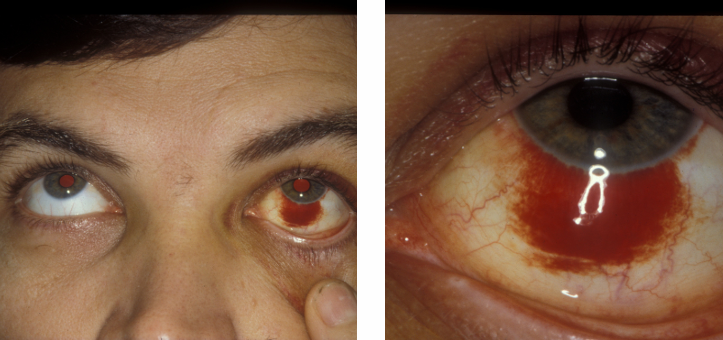
Subconjunctival Haemorrhage (SCH)
Often spontaneous, occurring after manoeuvres such as coughing or heavy lifting, vomiting, sneezing.
Might indicate underlying systemic conditions (e.g., hypertension).
Important to assess the posterior limits to ensure they are clear of damage.
if you cannot see the posterior limits it may indicate an orbital fracture.
Dense SCH could obscure occult globe damage
VA, pupils, asymmetric ACD, abnormally low IOP, history
Treatment typically involves monitoring as most cases resolve spontaneously.
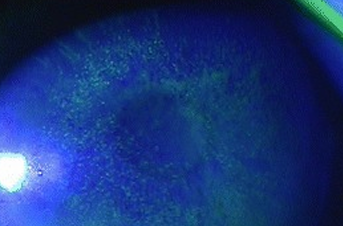
Corneal Abrasions
Result from abrasions caused by various foreign objects (e.g., fingernails, paper).
Symptoms include:
Intense pain
Photophobia
Redness and watering
Confirm and document the size of the epithelial defect using fluorescein.
Larger abrasions may indicate a potential anterior chamber reaction.
Healing epithelial defect may resemble HSV dendrite (tapered ends, normal corneal sensitivity)
test corneal sensitivity to rule out HSV
Risks of corneal abrasions
recurrent corneal erosions: epithelial basement membrane dystrophy
organic material: fungal infections
High speed foreign bodies: penetration / perforation risk
Blunt trauma: related damage.
assessment:
track staining - retained foreign body under upper lid
lid eversion
if px is in too much pain, sweep fornices using a moist sterile cotton bud.

Management of Corneal Abrasion
Treatment involves:
Broad-spectrum antibiotics (e.g., Chlorsig)
Non-preserved lubricant until healing occurs.
Daily follow-up and monitoring for any signs of complications.
Avoid patching if the cause of abrasion is organic material.
managed anterior chamber reactions with cycloplegics (phenylephrine or tropicamide)
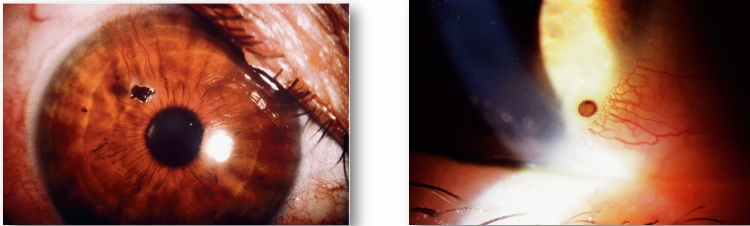
Ocular surface foreign body
Often repeat injury!
Most not associated with ocular morbidity.
Consider possibility of perforating injury especially with high-speed projectiles.
Corneal foreign bodies may be coincidental (e.g., wind-blown debris).
Most commonly occur from higher risk activities without protective eyewear, such as:
Cutting
Grinding
Drilling
Hammering
Corneal Foreign Body Assessment
Pain or foreign body sensation
photophobia
redness
watering
conjunctival hyperaemia and chemosis
secondary infection risk
possible anterior chamber reaction - irritative miosis and photophobia
perforation
reduced VA
asymmetric IOP
shallow or flat AC
iris defects (transillumination)
lens capsule defects or opacities.
Management of Corneal Foreign body
assess depth of FB
posterior stroma: Seidel test before and after removal
“waterfall” sign indicates aqueous leakage and complete perforation. These patients need urgent referral / hospitalisation. Do not try to remove FB.
infection risk: metallic FBs may be sterile due to heat
organic or stone, grit, plant material, higher infection risk.
associated rust ring may give secondary keratitis
often white cellular infiltrate around FBs
Corneal Foreign Body Removal
tangential approach:
with a 25-guage needle with flattened upturned tip
FB spud
Bailey Loop - wire or nylon loop
Fine point jewellers forcep
Alger brush - to remove rust ring (may need to remove after couple of days)
topical antibiotic cover
24 hr review
safety spectacles
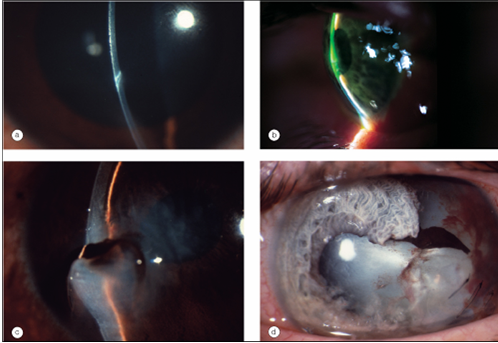
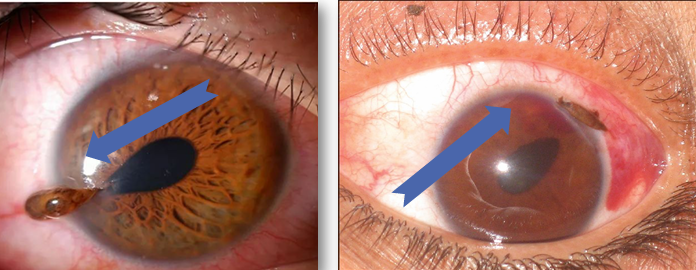
Corneal Lacerations
shallow lacerations effectively corneal abrasions
Lager lacerations: surgical repair, cyanoacrylate glue, suturing
In Practice: eye shield, immediate transport.
pointed pupil is a sign of serious injury as often the iris is getting sucked up to a wound
the point of the pupil will point the site of the injury
Photokeratopathy
“welder’s flash”, “arc eye”, “snow blindness”
Ultraviolet burn often as welding arc is struck
Denude epithelium of conjunctiva and cornea
symptoms: pain, photophobia, tearing, lid and conjunctival swelling
management: heals in 2-3 days, advice on proper protection, non-preserved lubricants, ice packs, sunglasses. Antibiotics are usually not necessary.
Chemical Trauma: Acids vs alkalis
Alkalis tend to penetrate the eye more readily (2x more common) and result in significantly higher ocular morbidity. They:
Saponify cell membranes
Denature collagen
Thrombose vessels
Acids precipitate and coagulate protein, preventing further penetration through the cornea, while binding to the epithelial surface.
Acids include:
Sulfuric – car batteries
Hydrochloric – swimming pool additives
Concrete cleaners
Acetic acid
Hydrofluoric - glass etching
Alkalis include:
Ammonia, ammonium hydroxide
Sodium hydroxide (caustic soda)
Calcium hydroxide (lime, cement, plaster)
Others: shampoos, facial cleansers, etc.
Chemical trauma
necrosis of conjunctiva and corneal epithelial cells
disruption and occlusion of limbal vasculature
loss of limbal stem cells
Potential for:
conjunctivalisation and vascularisation of the cornea
persistent epithelial defect
OSD
symblepharon
cicatricial entropion
Deeper penetration causes stromal opacification
Iris and lens damage if penetrates to AC
damage to ciliary epithelium impairs ascorbate secretion
necessary for collagen production and repair of the cornea.
Management of chemical trauma
First aid / irrigation:
immediate first aid
irrigate, irrigate, irrigate
instil local anaesthetic
sterile saline, eyestream, tap water
15 minutes minimum - 30 (better)
Prior to assessment
for severe burns - continue irrigation until attend emergency.
Grading (roper-Hall classification):
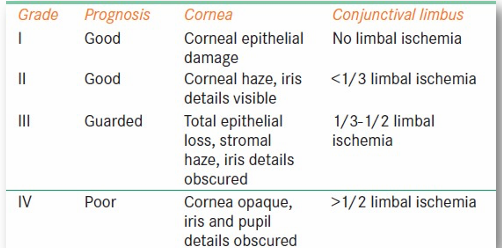
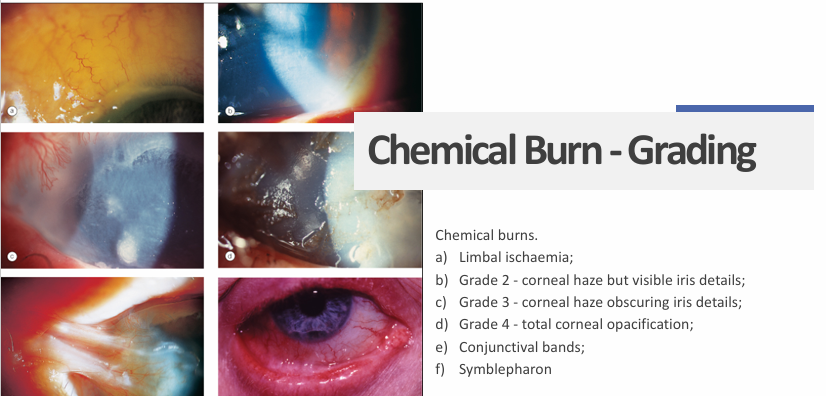
management: aimed at promoting re-epithelialisation + minimising inflammation
reduce risk of performation
Grade 1 + 2:
prophylactic antibiotics (e.g., chlorsig qid)
cycloplegic for ciliary spasm if AC reaction
topical steroids (e.g., FML) qid for 7 days + rapid taper.
steroid reduces collagen synthesis and inhibit fibroblast migration
affect stromal repair.
Grade 3 + 4:
high dose vitamin C (2g QID)
10% sodium ascorbate q2h topically
reverses localised scorbutic state and promotes healing by promoting synthesis of collagen by fibroblasts
10% sodium citrate q2h topically
chelation of calcium inhibits collagenase
tetracyclines - doxycycline 50-100 mg bd
inhibit collagenase and may reduce risk of perforation.