Expanded Programs on Immunization
Immunization (WHO meaning)
Immunization is the process whereby a person is made immune or resistant to an infectious disease, typically by the administration of a vaccine.
Immunization is a proven tool for controlling and eliminating life-threatening infectious diseases
Immunity
The condition of being secure against any particular disease.
Immunity is the ability of the human body to tolerate the presence of material indigenous to the body, and to eliminate foreign material.
Two basic mechanisms for acquiring immunity:
Active immunity is protection that is produced by the person’s own immune system. This type of immunity usually lasts for many years, often during a lifetime
Passive immunity is protection by products produced by an animal or human and transferred to another human, usually by injection.
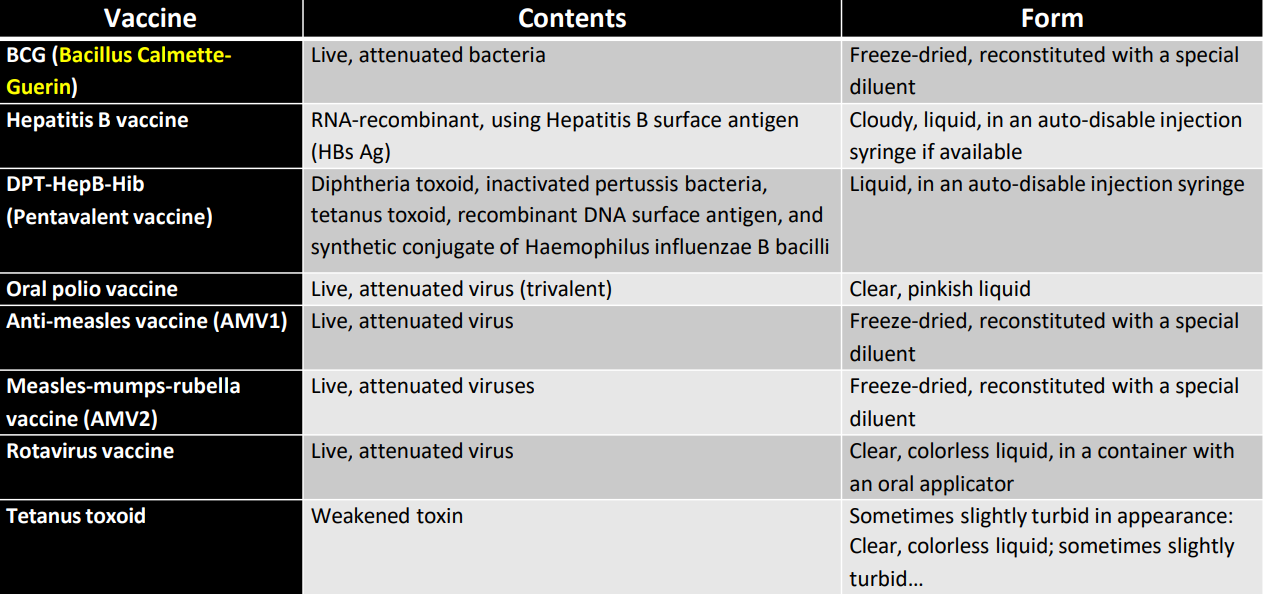
Vaccine
A vaccine helps the body’s immune system to recognize and fight pathogens like viruses or bacteria, which then keeps us safe from the diseases they cause.
Types of Vaccines:
Live-attenuated vaccines (LAV) - harmless germ is alive and can replicate
Inactivated vaccines (killed antigen) - germ cannot replicate, booster shots are needed
Subunit (purified antigen) - piece of germ causing strongest response can be used
Protein-based
Polysaccharide
Conjugate
Toxoid (inactivated toxins) - inactivated harmful parts of germs
Expanded Program on Immunization
The Expanded Program on Immunization (EPI) was established in 1976 to ensure that infants/children and mothers have access to routinely recommended infant/childhood vaccines.
Six vaccine preventable diseases were initially included in the EPI:
TB
poliomyelitis
diphtheria
tetanus
pertussis
measles
Supporting Legislations
PD No. 996 of 1976
providing compulsory basic immunization for infants and children below 8 years old
R.A. 7846 of 1994
Provided for compulsory immunization against hepatitis B for infants and children below 8 years old.
Provided for hepatitis B immunization within 24 hours after birth of babies of women with hepatitis B.
Presidential Proclamation No. 6 of 1996
Implementing a United Nations Goal on Universal Immunity by 1990; and designating Wednesdays as Immunization day
R.A. 10152
Mandatory Infants and Children Health Immunization Act of 2011
mandates basic immunization covering the vaccine-preventable diseases
Goals of EPI
To immunize all infants/children against the most common vaccine-preventable diseases.
To sustain the polio-free status of the Philippines.
To eliminate measles infection.
To eliminate maternal and neonatal tetanus.
To control diphtheria, pertussis, hepatitis B, and German measles.
To prevent extrapulmonary TB among children
Diseases
Tuberculosis (TB)
Case Definition
A child with history of contact with a suspect or confirmed case of pulmonary tuberculosis
Any child who does not return to normal health after measles or whooping cough
Loss of weight, cough, and wheeze which does not respond to antibiotic therapy for acute respiratory disease.
Abdominal swelling with a hard painless mass and free fluid
Painful firm or soft swelling in a group of superficial lymph nodes
Any bone or joint lesion or slow onset
Signs suggesting meningitis or disease in the central nervous system
Agent
Mycobacterium tuberculosis
Reservoir
Man
Diseased cattle
Sources of Infection
Droplet infection, that is through inhalation of bacilli from patients
Occurence
Worldwide
Mortality and morbidity higher in developing countries
Transmissible Period
A person who excretes tubercle bacilli is communicable
The degree of communicability depends upon:
The number of bacilli in the air
Virulence of bacilli
Environmental conditions like overcrowding
Duration of Natural Immunity
Not known
Reactivation of old infection commonly causes disease
Risk Factor for Infection
Low access to care
Immunodeficiency
Malnutrition
Alcoholism
Diabetes
Diphtheria
Case Definition
It is an acute pharyngitis, acute nasopharyngitis or acute laryngitis with a pseudo membrane
Agent
Corynebacterium diphtheriae
Reservoir
Man
Sources of Infection
By respiratory droplets from discharge of a case or carrier
Occurence
Worldwide
Endemic in developing countries with unimmunized populations
Transmissible Period
May last for 2-3 weeks
Maybe shortened in patients with antibiotics treatment
Diphtheria transmission is increased in schools, hospitals, households and in crowded areas
Duration of Natural Immunity
Usually Lifelong
Risk Factor for Infection
Crowding
Low Socio-Economic Status
Poliomyelitis (polio)
Case Definition
any patient below 15 years of age with acute flaccid paralysis (including those diagnosed to have Guillain-Barre Syndrome) for which no other cause can be immediately identified.
Agent
Poliovirus type 1,2 & 3
Reservoir
Man. Mostly children
Sources of Infection
Fecal-oral route
Oral route through pharyngeal secretion
contact with infected persons
Occurence
Cyclical
Worldwide
Morbidity and mortality higher in developing countries
Transmissible Period
7 to 16 days before onset of symptoms
first few days after onset of symptoms
Duration of Natural Immunity
Type specific immunity lifelong
Risk Factor for Infection
Poor environmental hygiene
Measles
Case Definition
A highly communicable disease with the history of the following:
Generalized blotchy rash, lasting for three of more days
Fever (above 38⁰C or “hot” to touch and
Any of the ff:
Cough
Runny nose
Red eyes/conjunctivitis
Agent
Rubeola Virus
Reservoir
Humans
Sources of Infection
Close respiratory contact and aerosolized droplets
Occurence
Worldwide
Mortality and morbidity higher in developing countries
Transmissible Period
4 days before until 2 days after rash
Duration of Natural Immunity
Lifelong after attack
Risk Factor of Infection
Crowding
Low socio-economic status
Pertussis
Case Definition
History of severe cough and history of any of the following
Cough persisting 2 or more weeks
Fits of coughing, and
Cough followed by vomiting
Agent
Bordetella Pertussis
Reservoir
Man
Sources of Infection
primarily by direct contact with discharges from respiratory mucous membranes of infected persons
Airborne route probably by droplets
Indirect contact with articles freshly soiled with the discharges of infected persons
Occurence
Worldwide
Morbidity higher in developing countries
Transmissible Period
Highly communicable in early catarrhal stage, before paroxysmal cough
Antibiotics may shorten the period of communicability from 7 days after exposure to 3 weeks after onset of typical paroxysms to only 5 to 7 days after onset of therapy
Duration of Natural Immunity
Usually lifelong
Risk Factor for Infection
Young age crowding
Neonatal Tetanus
Case Description
A newborn with history with all three of the following:
Normal suck for the first two days of life
Onset of illness between 3 to 26 days
Inability to suck followed by stiffness of the body and/or convulsions (Opisthotonos position- extended back position)
Agent
Clostridium Tetani
Reservoir
soil
intestinal canals of animals (esp horses)
man
Sources of Infection
Unhygienic cutting of umbilical cord, improper handling of cord stump esp when treated with contaminated substance
Occurence
Worldwide
Morbidity higher in developing countries more common in agricultural and underdeveloped areas where contact with animal excreta is more likely
Transmissible Period
Susceptibility is general (all)
immunity can be obtained after 2 primary doses of tetanus toxoid at 4 weeks interval in mothers one month before delivery
three booster doses increase antibody levels in mothe
Duration of Natural Immunity
No immunity induced by infection
Risk Factor for Infection
Contamination of umbilical cord
Agricultural work
Hepatitis B
Case Description
It is the liver infection caused by type B of hepatitis virus. It attacks the liver often resulting in inflammation
Agent
Hepatitis B virus
Reservoir
Man
Sources of Infection
From child to child or mother to child after birth
From mother to child during birth
through sharing unsterilized needles, knives or razors
through sexual intercourse
Occurence
In the Philippines, approximately 12% of the population are chronic carriers
Most Filipinos are infected before the age of 6 years
Some infected infants are not able to develop immunity and become chronic carriers
Hepatitis B is especially dangerous for children
Transmissible Period
If develops, lifelong
Duration of Natural Immunity
Infants born to immune mothers may be protected up to 5 months
Recovery from clinical attack is not always followed by lasting immunity
Immunity is often acquired through inapparent infection or complete immunization series with diphtheria toxoid
Risk Factor for Infection
HBeAG + mother
Multiple sexual partners
Yellow fever
Case Description
Yellow fever is an acute viral hemorrhagic disease transmitted by infected mosquitoes.
The "yellow" in the name refers to the jaundice that affects some patients.
Symptoms of yellow fever include fever, headache, jaundice, muscle pain, nausea, vomiting and fatigue.
A small proportion of patients who contract the virus develop severe symptoms and approximately half of those die within 7 to 10 days.
Large epidemics of yellow fever occur when infected people introduce the virus into heavily populated areas with high mosquito density and where most people have little or no immunity, due to lack of vaccination.
In these conditions, infected mosquitoes of the Aedes aegypti specie transmit the virus from person to person.
Agent
Yellow Fevr Virus
Reservoir
aedes aegypti
Sources of Infection
Occurence
The virus is endemic in tropical areas of Africa and Central and South America.
Transmissible Period
Duration of Natural Immunity
Yellow fever is prevented by an extremely effective vaccine, which is safe and affordable.
A single dose of yellow fever vaccine is sufficient to confer sustained immunity and life-long protection against yellow fever disease
The vaccine provides effective immunity within 10 days for 80-100% of people vaccinated, and within 30 days for more than 99% of people vaccinated.
Risk Factor for Infection
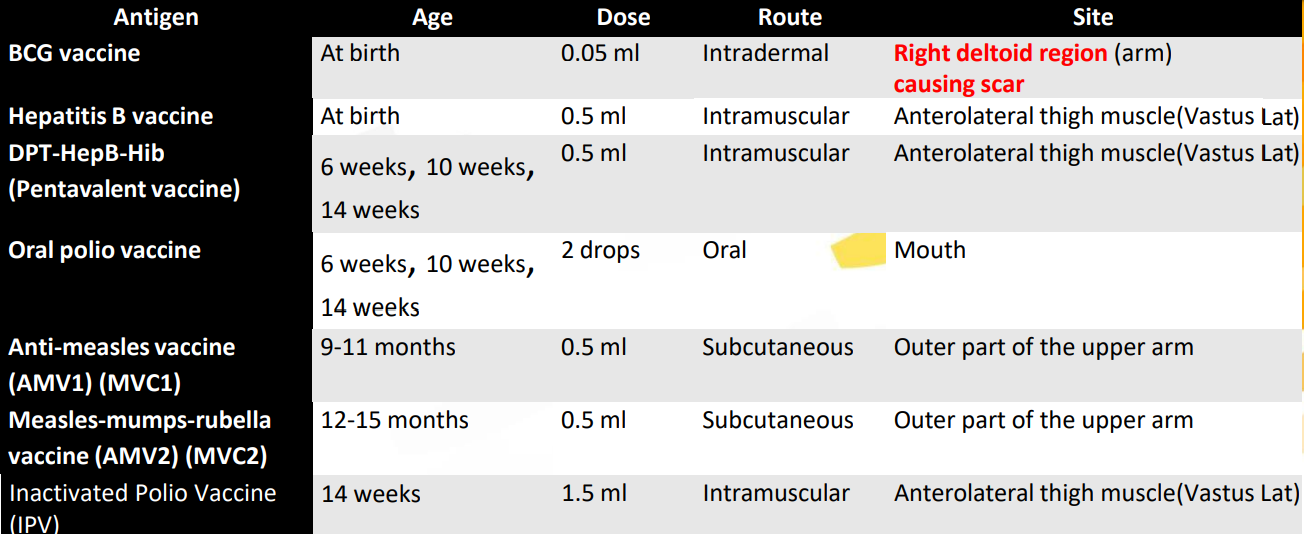
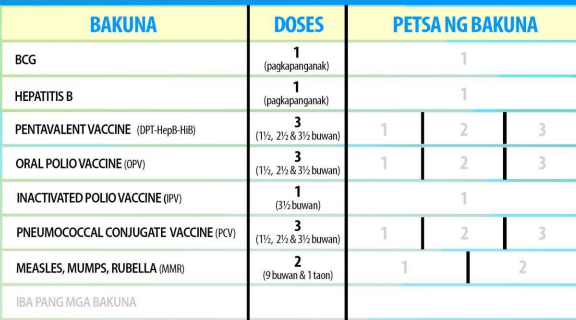
Schedule and manner of administering infant immunizations:
Use only sterile syringe and needle per client
There is no need to restart a vaccination series regardless of the time that has elapsed between doses.
All the EPI antigens are safe and effective when administered simultaneously.
same immunization session but at different sites
NOT Recommended
to mix different vaccines in one syringe
to use a fluid vaccine for reconstitution of a freeze-dried vaccine.
If more than one injection has to be given on the same limb:
injection sites should be 2.5-5cm apart
Recommended sequence of coadministration:
OPV first followed by Rotavirus vaccine, then other appropriate vaccines
OPV administration
drops of vaccine straight from the dropper onto the child’s tongue
DO NOT let the dropper touch the tongue
Only monovalent hepatitis B vaccine must be used for the birth dose.
Pentavalent vaccine must not be used for the birth dose because DPT and Hib vaccine should not be given at birth.
Shall be given:
AMV1 (MCV1) ASAP
AMV2 (MCV2) one month after the AMV1
All children entering day care centers/ preschool and Grade I shall be screened for measles immunization
Rotavirus Vaccine
First Dose: Administered to infants 6 - 15 weeks
Second Dose: Administered to infants 10 weeks to 32 weeks max
Administer the entire dose of the Rotavirus vaccine slowly down one side of the mouth with the tip of the applicator directed toward the back of the infant’s mouth.
To prevent spitting or failed swallowing, stimulate the rooting or sucking reflex of the young infant.
For infants aged 5 months or older, lightly stroke the throat in a downward motion to stimulate swallowing.
Target Setting
100% immunization of infants/children against the most common vaccine-preventable diseases
In RHU/health center level the public health nurse is responsible for:
Preparing vaccine requirements
Overseeing vaccine allocation
“Vaccine requirement is calculated based on eligible population.”
𝐸𝑠𝑡𝑖𝑚𝑎𝑡𝑒𝑑 𝑛𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑖𝑛𝑓𝑎𝑛𝑡𝑠 = 𝑡𝑜𝑡𝑎𝑙 𝑝𝑜𝑝𝑢𝑙𝑎𝑡𝑖𝑜𝑛 𝑥 2.7%
𝐸𝑠𝑡𝑖𝑚𝑎𝑡𝑒𝑑 𝑛𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 12 𝑡𝑜 59 𝑚𝑜𝑛𝑡ℎ 𝑜𝑙𝑑 𝑐ℎ𝑖𝑙𝑑𝑟𝑒𝑛 = 𝑡𝑜𝑡𝑎𝑙 𝑝𝑜𝑝𝑢𝑙𝑎𝑡𝑖𝑜𝑛 𝑥 10.8%
𝐸𝑠𝑡𝑖𝑚𝑎𝑡𝑒𝑑 𝑛𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑝𝑟𝑒𝑔𝑛𝑎𝑛𝑡 𝑤𝑜𝑚𝑒𝑛 = 𝑡𝑜𝑡𝑎𝑙 𝑝𝑜𝑝𝑢𝑙𝑎𝑡𝑖𝑜𝑛 𝑥 3.5%
Considerations for Potency
Vaccines confer immunity only when they are potent. To retain the potency vaccines must be properly stored, handled, and transported.
Maintain the COLD CHAIN
system for ensuring the potency of a vaccine from the time of manufacture to the time it is given to an eligible client.
Person responsible: Cold Chain Officer
COLD CHAIN Equipment and Supplies:
Freezer/refrigerator
Transport box
Vaccine bags/carriers
Cold chain monitors
Thermometers
Cold packs (COLD DOGS)
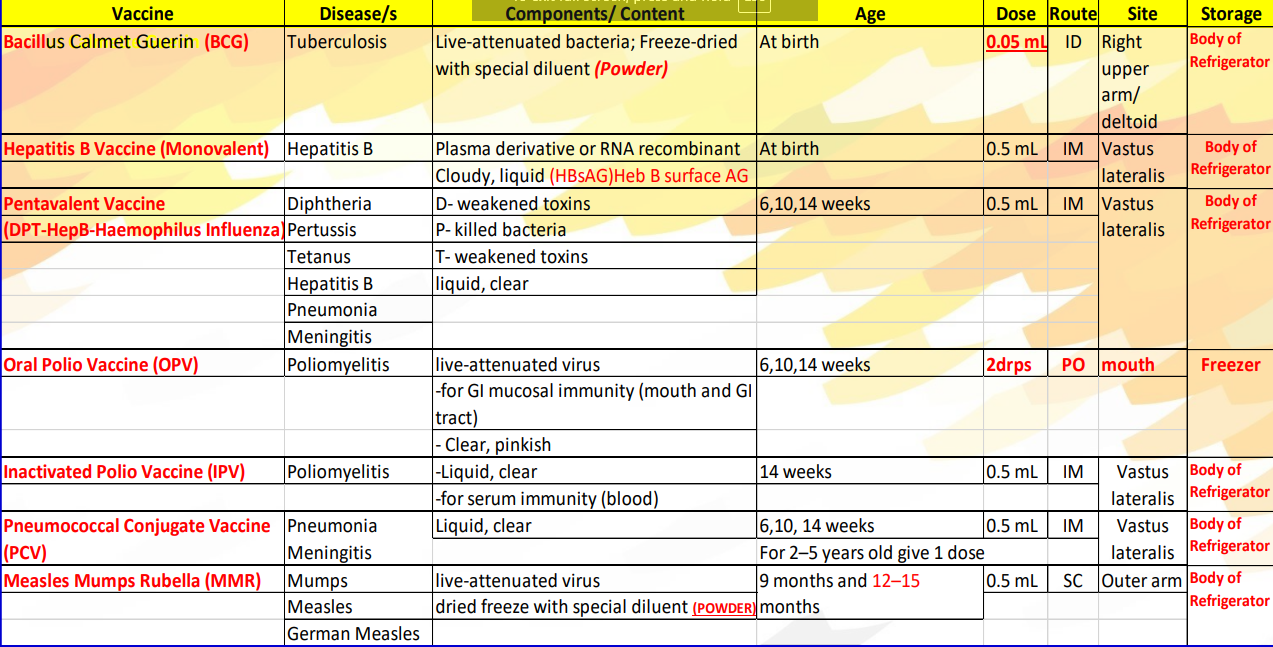
OPV: -15 to 25⁰C.
OPV has to be stored in the freezer.
In the vaccine bag, OPV is placed in contact with cold packs.
All other vaccines, including measles vaccine, MMR, and Rotavirus vaccine, have to be stored in the refrigerator at a temperature of +2 to +8⁰C.
Hepatitis B vaccine, Pentavalent vaccine, Rotavirus vaccine, and TT are damaged by freezing, so they should NOT be stored in the freezer.
Wrap the containers of these vaccines with paper before putting them in the vaccine bag with cold packs.
Keep diluents cold by storing them in the refrigerator in the lower or door shelves
Observe the first expiry-first out (FEFO) policy.
Comply with the recommended duration of storage and transport.
At the health center/RHU with a refrigerator, the duration of storage should not exceed one month.
Using transport boxes, vaccines can be kept only up to maximum of 5 days.
Take note if the vaccine container has a vaccine vial monitor (VVM) and act accordingly.
VVM is a round disc of heat-sensitive material placed on a vaccine vial to register cumulative heat exposure.
the lower the temperature, the slower the color change
the higher the temperature, the faster the color change.
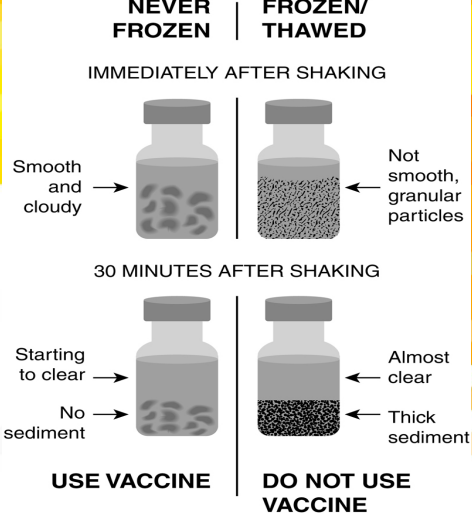
Shake Test
This approach can be used to determine if the biological should be used or discarded. If the vial is smooth and cloudy immediately after shaking, the biological can be used. However, if it appears granular and not smooth, it should be discarded
Abide by the open-vial policy of the DOH
A multi dose vial may be opened for one or two clients if the health worker feels that a client cannot come back for the scheduled immunization session. BCG, PentaHib, AMV(MCV)
Multi dose liquid vaccines, such as OPV, Pentavalent vaccine, hepatitis B vaccine, and TT from which one or more doses have been taken following standard sterile procedures, may be used in the next immunization sessions for up to maximum of 4 weeks, provided that all the following conditions are met:
The expiry date has not passed.
The vaccine has not been contaminated.
The vials have been stored under appropriate cold chain conditions.
The vaccine vial septum has not been submerged in water.
The VVM on the vial, if attached, has not reached the discard point
Reconstitute freeze-dried vaccines such as BCG , AMV, and MMR only with the diluents supplied with them.
Discard reconstituted freeze-dried vaccines 6 hours after reconstitution of at the end of the immunization session, whichever comes sooner. BCG, AMV(MCV), and MMR
Protect BCG from sunlight and Rotavirus vaccine from light.
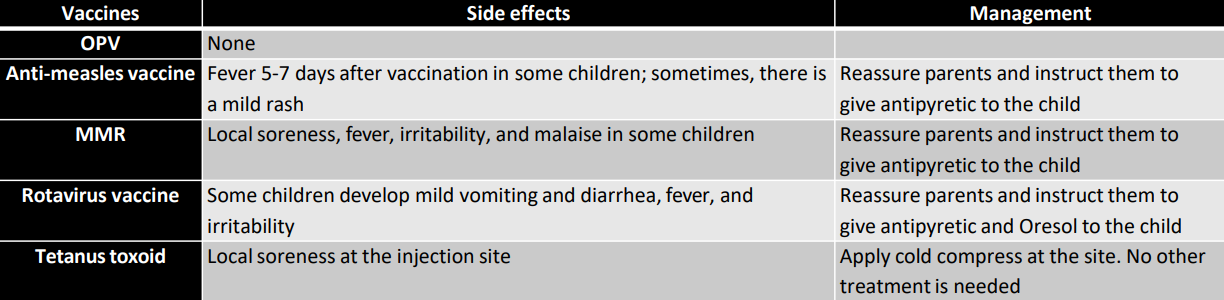
Side Effects of Vaccination

Contraindications to Immunization
In general, there are no contraindications to immunization of a sick child if the child is well enough to go home.
Do not give:
Ꭓ Pentavalent vaccine/DPT to children over 5 years of age.
Pentavalent vaccine/DPT to a child with recurrent convulsions or another active neurological disease of the central nervous system.
Pentavalent vaccine 2 or 3/DPT 2 or 3 to a child who has had convulsions or shock within 3 days of the most recent dose.
BCG to a child who has signs and symptoms of AIDS or other immune deficiency conditions or who are immunosuppressed
Moderate fever, malnutrition, a mild respiratory infection, a cough, diarrhea, and vomiting is not absolute contraindication and must give the scheduled vaccines
Procedures in Giving Vaccines
BCG
Reconstitution of Freeze Dried (Powder Form)
Keep the diluent cold by sustaining with BCG vaccine ampule in refrigerator or vaccine carrier.
Using 5ml syringe fitted with a long needle, aspirate 2ml. Of saline solution from the open ampule of diluent
Inject the 2ml. Saline into the ampule of freeze dried BCG .
Thoroughly mix the diluent and vaccine by drawing the mixture back into the syringe and expel it slowly into the ampule several times.
Return the reconstituted vaccine on the slit of the foam provided in the vaccine carrier.
Giving BCG Vaccine (Intradermal)
Clean the skin with a cotton ball moistened with water and let the skin dry.
Hold the child’s arm with your left hand so that your hand is under the arm, and your thumb and fingers come around the arm and stretch the skin.
Hold the syringe in your right hand with bevel and the scale pointing up towards you.
Let the syringe and needle almost flat alone the child’s arm.
Insert the tip of the needle into the skin-just the bevel and a little bit more. Keep the needle flat along the skin and the bevel facing upwards, so that the vaccine only goes into the upper layer of the skin.
Put your left thumb over the needle end of the syringe to hold it in position. Hold the plunger end of the syringe between the index and middle fingers of your right hand and press the plunger in with right thumb.
If the vaccine is injected correctly into the skin, a flat wheal with the surface pitted like an orange peel will appear into the injection site.
Withdraw the needle gently
Oral Polio Vaccine
Giving Oral Polio Vaccine (Oral)
Read the manufacture’s instructions to determine number of drops to be given. Use the dropper provided for.
Let the mother hold the child lying firmly on his back.
If necessary open the child’s moth by squeezing the cheeks gently between your fingers to make his lips point upwards.
Put drops of vaccine straight from the dropper onto the child’s tongue but do not let the dropper touch the child’s tongue.
Make sure that the child swallow the vaccine. If he spits it out, give another dose.
Penta Hib Vaccine
Giving Penta Hib Vaccine (Intramuscular)
Ask the mother to hold the child across her knees so that his thigh is facing upwards. Ask her to hold child’s legs.
Clean the skin with a cotton ball, moistened with water and let skin dry.
Place your thumb and index finger on each side of the injection site and grasp the muscles slightly. The best injection is the outer part of the child's mid-thigh.
Quickly push the needle into the space between your fingers, going deep in the muscle.
Slightly pull the plunger back before injecting to be sure that vaccine is not injected into a vein
Inject the vaccine. Withdraw the needle and press the injection spot quickly with a piece of cotton.
Measles Vaccine
Reconstituting Freeze Dried (Powder Form)
Using a 10 ml. Syringe fitted with a long needle, aspirate 5ml. Of special diluent, from the ampule.
Empty the diluent from the syringe into the vial with the vaccine.
Thoroughly mix the diluent by drawing the mixture back into the syringe and expelling it slowly into the vial several. Do not shake the vial
Protect reconstituted measles vaccine from sunlight. Wrap vial in foil.
Place the reconstituted vaccine in the slit of the foam provided in the vaccine carrier.
Giving Measles Vaccine (Intramuscular)
Ask the mother to hold the child firmly.
Clean the skin with a cotton ball, moistened with water and let the skin dry.
With the fingers of one hand, pinch up the skin on the outer side of the upper arm.
Without touching the needle, push the needle into the pinched-up skin so that it is not pointing.
Slightly pull the plunger back to make sure that the vaccine in not injected into a vein
Press the plunger gently and inject.
Tetanus Toxoid/ Diptheria Tetanus
Giving Tetanus Toxoid (To Pregnant Mother: Prevents Neonatal Tetanus) (Intramuscular)
Shake the vial
Clean the skin with a cotton ball, moistened with water and let skin dry.
Place your thumb and index finger on each side of the injection and grasp the muscles, slightly. The best injection site for a women is outer side of the left upper arm.
Slightly pull the plunger back before injecting to be sure that vaccine is not injected into a vein.
Quickly push the needle into the space between your finger, going deep in the muscle. 6. Inject the vaccine. Withdraw the needle and press the injection spot quickly with a piece of cotton
Documentation and Reporting
EPI recording and reporting are accomplished using the FHSIS.
Fully Immunized Children (FIC) are those who were given BCG , three doses of OPV, three doses of DPT and hepatitis B vaccine or three doses of Pentavalent vaccine, and one dose of anti-measles vaccine before reaching one year of age.
Completely immunized child refer to children who completed their immunization schedule at the age of 12-23 months.
A child protected at birth (CPAB) is a term used to describe a child whose mother has received:
two doses of TT during this pregnancy, provided that the second dose was given at least a month prior to delivery;
At least three doses of TT anytime prior to pregnancy with this child.
Role of Nurse in Improving Immunization Delivery
Actively master the list of infant eligible for vaccination in the community.
Immunize infants following the recommended immunization schedule, route of administration, correct dosage and following the proper cold chain storage of vaccines.
Disposed used syringes and needles properly by using collector box and disposing in the septic vault to prevent hazard.
Actively master the list of infant eligible for vaccination in the community.
Immunize infants following the recommended immunization schedule, route of administration, correct dosage and following the proper cold chain storage of vaccines.
Disposed used syringes and needles properly by using collector box and disposing in the septic vault to prevent hazard.
Inform, educate and communicate with the parents
To create awareness/motivate to submit their children for vaccination.
To provide health teaching on the importance and benefits of immunization, importance of follow-up dose to avoid defaulters and normal course of vaccine
Conduct health visit in the community to assess other health needs of the community and be able to provide package of health services to targets.
Identify cases of EPI target diseases per standard case definition.
Manage vaccine properly by following the recommended storage of vaccine
Record the children given with vaccination in the Target Client list and GECD/GMC card or any standard recording form utilized
Submit report and record of children vaccinated, cases and deaths on EPI diseases, vaccine received and utilized and any other EPI related reports.
Identify and actively search cases and deaths of EPI target diseases following standard case definition