L4: Cognitive perspectives
Learning objectives
1) The significance of cognition in the development of psychological problems.
Cognition is considered a central factor in the development of psychological problems. We do not simply just respond to events; instead, our response is a result of our own cognitive interpretation of those events.
It is the ‘unhelpful interpretations of events’ that are believed to produce emotional and behavioural disturbances.
2)The role of irrational beliefs and cognitive distortions in producing psychological problems.
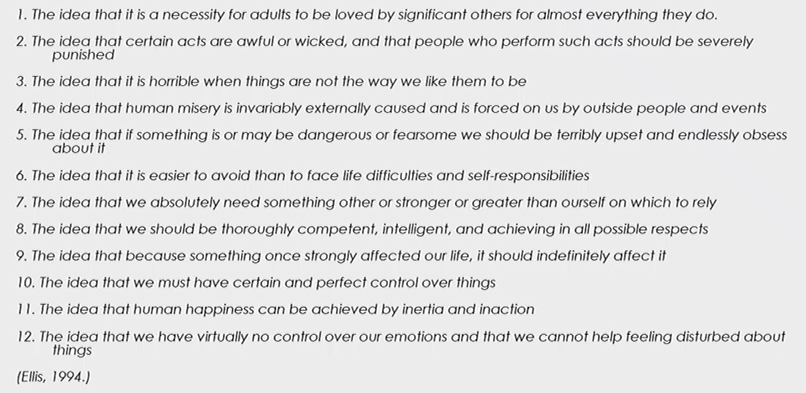
Irrational beliefs (Ellis) and cognitive distortions (Beck) describe systematic errors in thinking.
Albert Ellis and the ABC Model: Ellis proposed the ABC model, which states that an Activating event combined with our Beliefs leads to emotional and behavioural Consequences.
The model suggests that irrational beliefs are the root of psychological distress. Such as the idea that ‘we absolutely need something Smart, stronger or greater than ourselves’.
These are often rigid, exaggerated, and dysfunctional thought patterns that fuel emotional suffering (e.g., ‘I must be perfect or I’m worthless’).
3) Techniques to challenge irrational thoughts/create more helpful thoughts.
Techniques to challenge irrational thoughts and create more helpful ones
CBT equips clients with skills to examine evidence, test beliefs, and generate more adaptive ways of thinking.
e.g., cognitive restructuring, where clients learn to identify and reframe negative thoughts, and the use of thought records to track and analyse their thinking patterns over time.
Further: Socratic questioning, thought diaries, and behavioural experiments.
__________________________________________________________________
Key Features of Cognitive Theory (and CBT Practice)
It’s not enough to merely focus on observable behaviour- too reductionist.
Cognitive theory argues that thoughts mediate between events and emotions
We respond not to the actual event itself, but our cognitive interpretations of the event.
e.g., 2 students fail an exam; One thinks ‘I’m hopeless, I’ll never succeed’ and feels depressed. The other thinks ‘that was tough, but I’ll do better next time’ and feels motivated to try harder.
Dysfunctional interpretations create emotional and behavioural disturbances.
misinterpretations of events → emotional suffering → maladaptive behaviour
__________________________________________________________________
Albert Ellis: The ABC model
Pioneered Rational Emotive Behaviour Therapy: REBT
ABC model breakdowns/explains the relationship between events, beliefs, and consequences.
A= Activating Event
B= Beliefs
C= Consequences
ABC model demonstrates that it isn’t the actual activating event (A) that directly causes the consequence (C), but rather our Beliefs (B) about the event (cognitive interpretations).
This means that two individuals may experience the same activating event but react differently based on their beliefs.
Clinical significance: By targeting B, therapy can change C. This is the logic of CBT.
__________________________________________________________________
Irrational beliefs:
core irrational ideas that underpin psychological distress.
rigid, absolutist beliefs, often characterised by words like ‘must,’ ‘should,’ or ‘have to.’
e.g.,‘we should be thoroughly competent... in all possible respects’ = an irrational standard that can lead to significant anxiety and feelings of failure.
These beliefs contrast with rational ones, which are flexible and based in reality.
_________________________________________________________________
Aaron Beck:
sought an egalitarian perspective/experience of the world between the Client and the therapist.
Cognitive disorders are associated with certain specific & habitualised thinking patterns;
These result in persistent errors with how individuals interpret events (A→ B→C)
These errors arise from faulty thinking of ‘cognitive distortions’
Cognitive Distortions: habitual errors in thinking that sustain depression and anxiety.
Examples of cognitive distortions:
Black and white thinking: All-or-nothing thought processes, ‘If I’m not perfect, I’m a failure’.
Selective thinking: paying attention only to negative details, over critical and ‘rational’ (pessimism).
Over-generalising: Drawing sweeping conclusions from one event; ‘I failed this test, so I’ll fail everything’.
Catastrophising: expecting the worst outcome (‘If my hands shake, everyone will mock me’
Personalisation: Blaming oneself for external events/ Attributing personal responsibility to events over which the person has no control; 'If my team doesn't win, it's my fault.'
__________________________________________________________________
How does CBT work?
Cognitive Behavioural Therapy (CBT) works by helping individuals identify and challenge their negative thought patterns, replacing them with more positive and realistic thoughts.
Present-focused: targets current thoughts, rather than digging endlessly into past
collaborative relationship: therapist and client work together as equals, ‘guided discovery’.
clients as scientists: clients are encouraged to analyse their own thoughts & beliefs, and actually examine what the ‘evidence’ is for them?
NATs (Negative Automatic Thoughts): quick, unexamined thoughts that reflect deeper core-beliefs (CB)
e.g., NAT= ‘I’ll fail this test, CB= I am a failure
Five-part model (linking thoughts, mood, body, behaviour, situation).
Thought records to evaluate evidence.
Socratic questioning (gentle but logical challenge).
Behavioural experiments to test reality (e.g., see if anyone notices shaky hands).
__________________________________________________________________
Five-Part Model:(Christine Padesky)
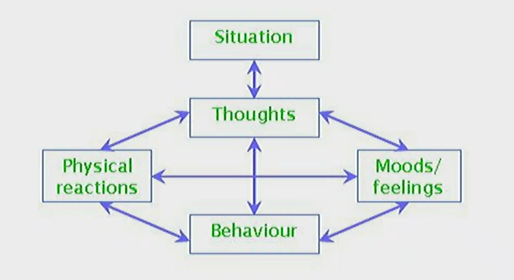
Situation → Thoughts → Emotions → Physiology → Behaviour.
Changing one part (e.g., thoughts) has cascading effects on the whole system; interactive across levels.
e.g.,
Situation = giving a speech <> Thought = ‘Everyone will laugh’ <> Emotion = anxiety <> Physiology = sweating <> Behaviour = avoidance
__________________________________________________________________
Thought Records [Mood Diary] (Greenberger & Padesky, 1995)

Identify the situation. (who, what, when, where?)
» ’Wednesday night, I am struggling to complete my assignment- particularly after receiving criticism from my professor earlier in the week.’
Record mood & intensity [What do you feel %?]
‘very intense, feels like I am drowning- 90%’
Capture the automatic thought
What was going through your mind before you felt this way?
» ‘My assignment is not anywhere near completed & the work I have done is not good enough’
Circle the ‘hot thought’ - what jumps out as the strongest/most distressing [NATs]
‘not good enough’
What is the evidence for this thought?
‘ I didn’t understand the last assignment brief well and did badly- I feel myself repeating the same mistake'
What is the evidence against this thought?
‘I did well enough to get into my degree with a higher rank score; I have successfully completed many other assignments in the past; I have received positive feedback on my work, telling me I am capable of understanding and executing tasks effectively’
Develop your Balanced thought.
'I might be struggling with this particular assignment, but it does not define my overall abilities. Though I’m stressed out right now, I can use this experience to improve my understanding. I have proven my skills in the past, and I can approach future assignments with more resilience & strategy.’
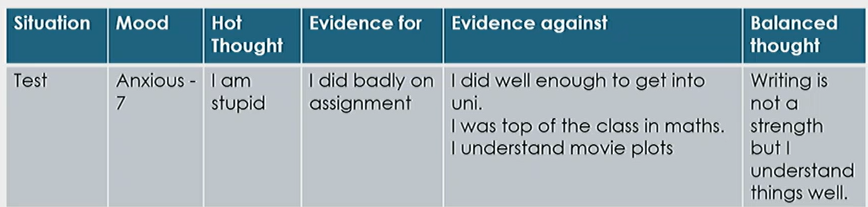
→ promotes metacognition; thinking about thinking. Helps clients to replace distorted interpretations with balanced ones.
__________________________________________________________________
Behavioural Experiments
Behavioural experiments are action-based techniques designed to directly test the validity of a client’s beliefs.
e.g., a client with social anxiety who believes ‘everyone will notice my hands shaking’ might conduct a planned experiment to see if their fear is realised.
It can be a powerful, experiential way to gather evidence and disconfirm dysfunctional beliefs, often more effective than simply talking about the belief.
» Taking someone’s idea/belief or perception of the world, and testing it out in the real world.
» e.g., the client could engage in a social setting where they intentionally allow their hands to shake while speaking, observing whether others actually react in the way they fear.
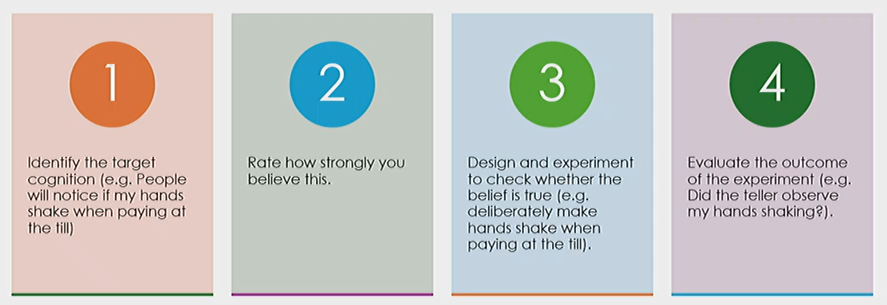
» Behavioural experiments help with providing concrete evidence against irrational beliefs, but also empower clients to challenge their self-imposed limitations.
» germ behaviours, social anxiety » exposure etc.
__________________________________________________________________
Strengths of CBT
Has become the leading/dominant psychological model for several reasons:
→ Strong Empirical Support: Extensive research and meta-analyses have demonstrated its effectiveness in treating a variety of mental health disorders, including depression, anxiety, and PTSD (Butler et al., 2007). [good to always remain cautious, though)
→ Consistency with the Scientist-Practitioner Model: Its structured, evidence-based approach aligns well with the scientific underpinnings of modern psychology.
→ Has revolutionised therapies by making them universal, widely accessible, and disestablished hierarchical therapy relationships.
→ Timely & Cost-effective: CBT is typically a short-term therapy, making it pragmatic, affordable and a more flexible therapeutic option that can be adapted to fit the needs and schedules of patients.
→ [Democratic] Empowering the Client: by teaching clients to become their own therapists, analyse their own thoughts, beliefs, situations, and behaviours, CBT fosters self-efficacy and encourages clients to take an active role in their therapy, thereby promoting long-term psychological resilience.
Weaknesses of CBT
Not without its limitations.
→ Limited focus on the Therapeutic Relationship: the emphasis on cognitive processes and skills may overlook the significance of the emotional bond between therapist and client, which can be crucial for effective therapy.
→ Not Enough Focus on Emotion: the cognitive approach (where cognition drives emotion) may fail to properly address the emotional aspects of a client's issues, potentially leading to a lack of true understanding of various underlying psychological struggles, contributing towards distress.
→ Limits the Outcome of Studies: Are the techniques really what make the therapy successful? Short-term motivation or long-term success?. Raises questions about whether the observed improvements are actually from CBT interventions or if they result from factors like client expectation and therapist influence.
→ Symptom vs Cause: A key criticism of CBT is that it is symptomatic, oriented towards treating symptoms without adequately addressing the underlying historical issues that continue to cause them.
→ Overestimation of Research Evidence: The Cognitive approach places heavier emphasis on empirical data/research/one-size-fits-all interventions; thus, it often overlooks the qualitative/patient-specific experience of clients and the complexities of human behaviour that are not easily quantified.
→ Social critique: CBT’s dominance reflects neoliberal priorities (efficiency, quick fixes), rather than clinical superiority, treatment efficacy, and client-therapist journey (Pilgrim, 2011; Rowland, 2024). CBT interventions/therapy emphasise individual responsibility/fault, ‘in and out’ therapy, and expectations of ongoing self-management over systemic/structural drivers of potential client issues: a lack of attention to social and economic factors that contribute to mental health conditions.
__________________________________________________________________