Clinical Psychology
Definitions of Mental Health
Specification
Definitions of mental health: deviation from ideal mental health, deviation from social norms, failure to function adequately & statistical infrequency
Deviation from Ideal Mental Health
Based on the idea that there are distinct markers that signal ideal mental health.
The DIMH measure assumes that if a person is mentally well, they will possess all the markers of IMH. To diagnose a mental health disorder, it is necessary to look for a lack of IMH behaviours in someone.
The 6 criteria - Marie Jahoda
Peter Is Really Struggling At Everything
Positive self-attitudes
High self-esteem, strong sense of identity, knowing where u fit in the world
Independence
Self-regulation, being able to work on your own
Resistance to stress
Resisting stress and being able to cope in stressful situations
Self actualisation
Developing yourself and achieving the goals you set for yourself in life
Accurate perception of reality
Having a realistic view of the world and your place in it
Environmental mastery
Being able to adapt and meet the demands of the environment and the situation you are in
strengths
Holistic measure
A person is not viewed simply in terms of their innate, biological traits. The person’s place in the world, their lifestyle and their individuality are all components
IRL application
This measure can be used as the basis for therapy treatments as a checklist
Limitations
Unrealistic
It is almost impossible to maintain all of the criteria.
Culture bias
It’s not aligned with the attitudes and beliefs of collectivist cultures
Deviation from Social Norms
Social norms = unwritten rules of how members in a society are expected to behave, think and act
When a behaviour goes against social norms, it may be labelled as ‘abnormal’ and therefore a deviation from social norms.
Strengths
Easily applicable
Socially deviant behaviour can indicate if a person has a mental illness
Protects society
Social norms ensure that societies are harmonious, and identifying socially deviant behaviour can protect members from distressing or harmful acts
Limitations
Dispositional variables
Some behaviours could be examples of eccentricity, and therefore not abnormal
Not generalisable
Cannot apply to other cultures as they have different social and cultural norms. In China, it is considered polite and a compliment to the food to burp while eating, whereas in the Western world, burping is seen as rude.
Cannot apply over time, things that were considered abormal 50years ago, are no longer considered abnormal. Homosexuality was once considered a disorder; in modern society, it has been recognised as a normal thing.
Failure to function adequately
When a person is unable to cope with the demands of everyday life. Those being:
good personal hygiene
Regular eating habits
Attending work or school
Socialising with others
People who experience FFA struggle with all of these aspects, and as a result, they often have to deal with a reduction in income, job loss and a lack of contact with colleagues. Including that, FFA can lead to damaging effects within interpersonal relationships.
Identifying factors
Severe distress - personal or to others around them
Behaviour that goes against social norms
Behaving irrationally
Harm - self-inflicted or at others
Strengths
Easily observable
Behaviours are easily recognisable, and the definition provides a clear classification and diagnosis for them.
Checklists provided by Rosenham & Seligman
used to assess the degree of FFA, which increases the reliability of the measure
Limitations
Overly subjective measure
Someone’s version of hygiene may be different from another’s
Some behaviours are expressions of personal choice, e.g. swimming with sharks
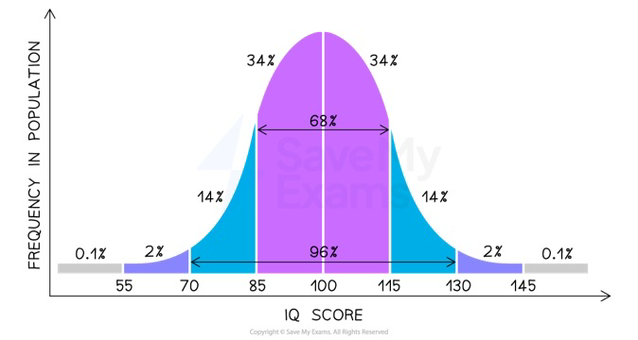
Statistical Infrequency
Defining mental health using statistical measures.
A behaviour is abnormal if it is statistically infrequent: 2 standard deviations from the average, top/bottom 2.5% of the population.
Measured using normal distribution (when the graph is symmetrical)
Strengths
Clear Measure
provides clear points of comparison between people, making it easy to test and use as an analytical tool
Reliable
Measures are replicable, meaning large data sets can also be included in the calculation, as it is less likely that they will be affected by outliers or anomalous results.
Limitations
Prevalent disorders
Disorders like depression wouldn’t be recognised, as it is a disorder that has a high prevalence rate, and therefore is not statistically infrequent.
Desirable characteristic - measuring utility
characteristic such as a high IQ is considered statistically infrequent, it is a desirable characteristic.
Phobias
Specification
Behavioural, emotional and cognitive characteristics of phobias
The behavioural approach to explaining phobias: the two-process model, classical and operant conditioning
Treatment for phobias (behavioural): systematic desensitisation & flooding
Characteristics
Phobias are an anxiety disorder
To be diagnosed, all of these symptoms must be present when confronted by the phobic stimulus:
Persistant fear and anxiety due to the phobic stimulus
Emotional
Irrational beliefs about the phobic stimulus
Cognitive
Avoidance or endurance of the phobic stimulus
Behavioural
Types of Phobias
Specific phobia - fear of objects or situations
Social phobia - fear of social situations or interactions
Agoraphobia - fear of not being able to escape public places or the outsides
Explanation
The Two-Process Model
Behaviour is learned through classical conditioning
Behaviour is maintained through operant conditioning
Classical Conditioning
When a neutral stimulus becomes associated with an unconditioned stimulus, which provokes a response. e.g. Little Albert:
NS (white rat) = no response
UCS (loud noise) = UCR (fear & anxiety)
NS (white rat) + UCS (loud noise) = UCR (fear & anxiety) x3
CS (white rate) = CR (fear & anxiety)
Supporting Study - Little Albert by Watson & Rayner (1920)
Little Albert was introduced to various animals, and it was established that they caused no emotional response, he took a particular liking to the white rat
Whenever Little Albert tried to touch the white rat, researchers made a loud noise. This loud noise would scare Little Albert and make him cry. They repeated this process 3 times.
Little Albert would no longer attempt to play with the rat, and instead began to cry and experience fear whenever he saw it.
Including that, whenever Little Albert saw any animal with fur, a fur coat, and a Santa Claus beard, he began to cry. This shows that his phobia generalised to all objects that resembled the white rat.
Operant Conditioning
Takes place when our behaviour is either reinforced or punished, positive & negative reinforcement.
Negative reinforcement = avoidance of unpleasant situations
Positive reinforcement = behaviour will be repeated
Phobias are reinforced via positive reinforcement, for example:
Phobic stimulus = anxiety and fear
Avoidance of phobic stimulus = relief
Because they always experience relief in the absence of the phobic stimulus, they are inclined to repeat the behaviour of avoiding the phobic stimulus.
Evaluation
Phobias and trauma
The LA study illustrates how a traumatic experience can lead to a phobia. A study was done for people with driving phobias, 50% of people said that they had a traumatic experience with a car.
Alternative explanation
Not all phobias are caused by a traumatic experience. In the driving phobias study, 50% could not recall a traumatic event. This means there could also be a genetic component which causes phobias.
IRL application
The idea of the two-process model is present in exposure therapies, and it is crucial in explaining why people benefit from exposure therapy.
Cognitive aspects of phobias are ignored
The two-process model explains behaviour, but cannot explain the cognitive aspects of a phobia (irrational beliefs, etc.). Overall, this means that the two-process model cannot explain all of the symptoms of phobias.
Treatments
Systematic Desensitisation
Behavioural therapy, reducing anxiety of the phobic stimulus via counterconditioning.
If a person can learn to relax around a phobic stimulus = cured.
It requires multiple sessions, over a period of time.
The 3 Processes:
The anxiety hierarchy
The client with a phobia and a therapist create a list of situations related to the phobic stimulus. Arranged from least to most frightening.
For example:
picture of a small spider
video of a spider
same room as a spider
holding a tarantula
Relaxation techniques
The therapist teaches the client breathing exercises (controlling breath) and visualisation (imagined environment).
To ensure that when facing the phobic stimulus, they remain as calm as possible.
Exposure
While in a relaxed state, the client is exposed to the phobic stimulus, gradually going up on the fear hierarchy.
The aim is for the patient to move up to the top of the hierarchy whilst remaining relaxed and in control
Evaluation
Case Study - Ost et al (1989)
20 patients with a phobia of blood or injury went through systematic desensitisation. After 4 years, patients were interviewed - 90% had completely recovered from their phobia.
Ethical
Less distressing for a patient
Phobia types
Less effective at treating social phobias & agoraphobias, as cognitive factors play a key role in them.
Flooding
Sudden, extreme exposure to the phobic stimulus without any prior build-up or gradual approach. For example, putting someone with arachnophobia in a room full of spiders.
To extinguish the association between the CS and the UCS, so that the person is forced to deal with the phobic stimulus and realise that it is, ‘just a spider…’
One session only.
Evaluation
Case Study - Kaplan & Tolin (2011)
Patients went through 1 flooding session. After 4 years, patients were interviewed - 65% of patients showed no symptoms of specific phobias.
Cheap
One session, and it has a high chance of working.
Unethical & risky
Patients will become extremely distressed. This can lead to the risk of an accident, meaning a new UCS will become associated with the CS, overall worsening the phobia.
Phobia types
Less effective at treating social phobias & agoraphobias, as cognitive factors play a key role in them.
Depression
Specification
Behavioural, emotional and cognitive characteristics of depression
The cognitive approach to explaining depression: Beck’s negative triad & Ellis’s ABC model
Treatment for depression (cognitive): CBT & SSRIs
Characteristics
Depression is a mood disorder
To be diagnosed, 5 symptoms must be present, at least 1 emotional symptom and must last over 2 weeks.
Low mood
Emotional
Loss of pleasure
Emotional
Irrational negative beliefs
Cognitive
Difficulty concentrating
Cognitive
Change in appetite (more/less)
Behavioural
Change in sleeping patterns (more/less)
Behavioural
Social Withdrawal
Behavioural
Explanations
Beck’s Negative Triad
Irrational thoughts, faulty information processing and distorted perceptions are what cause depression.
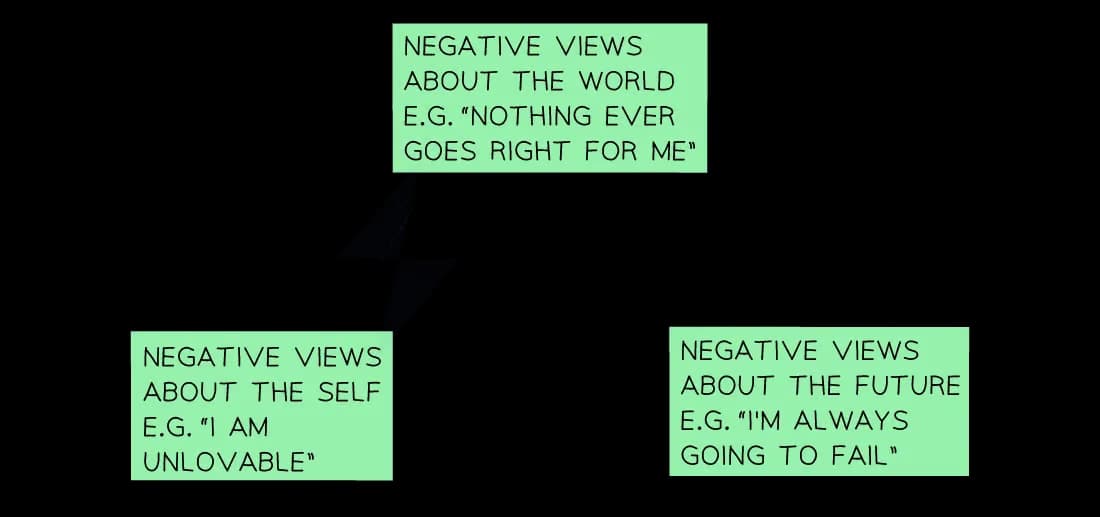
Negative Self Schema
A negative self-schema is when a person solely focuses on the negative, undesirable aspects of themselves. This creates a constant cycle of feeling worthless and self-evaluation.
Schema = a mental framework people use to organise their ideas based on their real-life experiences.
Self-schema = the framework a person has about themselves, e.g. ‘I am worthy of love’
Negative Cognitive Bias
Pay attention only to the negative aspects in a conversation. This contributes to a persons irratonal negative beliefs, which assimilate and strengthen their negative self-schema.
Cognitive Bias = The tendency to pay attention to only some info.
Positive, negative and none.
Ellis’s ABC Model
Irrational thoughts interfere with happiness.
A = Activating event
Losing your job
B = Beliefs about activating event
‘I lost my job because I’m useless and talentless’
Musturbation - ‘I must never fail’
I-can’t-stand-it-itis - ‘I can’t stand this jerk being my boss’
C = Consequences of beliefs
‘I will never find another job, so my whole life will fall apart’
Evaluation
Case Study - Koster et al (2005)
Two groups were tested: the non-depression group (control group) and the depression group (experimental group).
Participants were seated in front of a computer that flashed a word (positive, negative, neutral) before showing a square on the left or right side of a screen, and asking the person to click a button for the corresponding side (left or right).
Findings: (The experimental group)
Negative word = longer reaction time
Positive word = same reaction time as control
Neutral word = same reaction time as control
Conclusion
People with major depression have a negative cognitive bias, which causes their delayed reaction times.
Case Study - McGuffin et al
Investigated the concordance rate for depression in monozygotic and dyzygotic twins
Findings:
Monozygotic twins = 46%
Dyzygotic twins = 20%
Conclusion:
Depression is likely to be partially inherited, as the concordance rate of monozygotic twins was higher than dyzygotic twins.
Irrational negative beliefs are not the only cause of depression
Case Study - Alloy & Abramson (1979)
Two groups were tested: the non-depression group (control group) and the depression group (experimental group).
Participants were asked to press a button, and could see a light that turned on/off (the button was not connected to the light).
Participants were asked how much control they had over the light bulb.
Findings:
The control group massively overestimated their control
The experimental group was more accurate than the control group
Conclusion:
People with major depression don’t always have irrational beliefs.
Treatments
Cognitive Behavioural Therapy (CBT)
The most common psychological treatment for depression.
Client learns how to be independent and to use strategies to help regulate themselves. It lasts around 5-20 sessions.
Focused on the here-and-now.
Cognitive Therapy
The application of Beck’s theory of depression within a CBT framework
Identifying negative beliefs
Challenging negative beliefs
Testing their hypothesis
Evaluating the evidence
The therapist uses this to confront the client directly and to highlight their irrational thoughts, or at least to look for other reasons why people may have acted the way they did.
Ellis’ Rational Emotive Behaviour (REBT)
Extends the ABC model to ABCDE.
D = Dispute
The therapist gives robust arguments to dispute the irrational thought
Empirical arguments - disputing whether there is real evidence to support the irrational belief
Logical arguments - disputing whether negative thoughts follow logically from the facts
E = Effect
Breaking the link between negative life effects and depression by changing the client’s irrational beliefs.
Evaluation of CBT
Review - Cujipers et al (2013)
Reviewed the effectiveness of CBT as a treatment in studies with a control and an experimental group.
Findings:
The experimental group improved while the control group did not
Conclusion:
CBT is more effective than no treatment
Effectiveness
CBT may not be effective for everyone, and it may not be as effective as other treatments.
Studies have shown that some people with depression have naturally lower levels of serotonin - this is something that CBT cannot resolve.
SSRIs
Selective Serotonin Reuptake Inhibitors
Drug therapy
The most effective antidepressant.

Some people with depression have less naturally occurring serotonin. SSRIs combat this:
Serotonin is a neurotransmitter that circulates throughout the body via synapses.
Serotonin that is left in the synapse is taken back into the presynaptic nerve - this reduces the amount of serotonin in the body
SSRIs inhibit the reuptake of serotonin, meaning more serotonin is left in the synapse
Therefore, more serotonin is sent throughout the body.
Evaluation
Most effective treatment for depression
Works for people with clinical depression - there is no cure; however, it can be treated effectively
Relatively easy to use
Side effects
Nausea, sleep problems, etc.
Relapse risk
After stopping medication, depression could return
Not ideal for people without clinical depression
OCD
Obsessive Compulsive Disorder
Specification
Behavioural, emotional and cognitive characteristics of OCD
The biological approach to explaining OCD: genetic & neural
Treatments for OCD (biological): drug therapy
Characteristics
To be diagnosed, a person must display all 3 of these symptoms:
Obsessions - recurring disturbing thoughts about certain topics
Cognitive
Guilty & Anxiety - caused by obsessions, feel ashamed → guilt and panic → Anxiety
Emotional
Compulsions - a strong urge to perform specific actions to try reduce feelings of anxiety, can be repetitive
Behavioural
Explanations
Neural Explanation
Normal brain:
Worrying stimuli → OFC → Motor Cortex → BG → (inhibiting neurotransmitters) → OFC
OCD:
Worrying stimuli → OFC → Motor Cortex → BG → (impaired communications) → OFC → obsessions/compulsions
Orbital Frontal Cortex (OFC)
Detects worrying stimuli in the surroundings and makes decisions in order to deal with the stimuli.
Motor Cortex
Part of the brain that controls movement.
Basal Ganglia (BG)
Monitors the outcome of our actions, and determines if the worrying stimuli has been dealt with.
IF it has been dealt with, the BG sends neurotransmitters to inhibit the OFC
Impaired Communications (between BG and OFC)
This is when the BG sends less inhibiting neurotransmitters, and therefore the OFC is left hyperactive. This means that the brain is constantly being signalled for worrying stimuli, even though they are unnecessary.
Evaluation
OCD after car accident - Max et al (1995)
Patient had an MRI, to evaluate her brain structure
Findings: Brain damage to the BG
Conclusion: The BG has a crucial part in OCD
Brain-imaging studies in adults - Saxena & Rauch (2000)
Two groups were tested, control & experimental
Findings: OCD group had more activity in the OFC
Conclusion: The OFC has a crucial part in OCD
Brain-imaging studies have been inconsistent - Aylward et al (1996)
Two groups were tested, control & experimental
Findings: No significant difference of the BG between both groups
Conclusion: Damage to the BG is not the only cause of OCD
Genetic Explanation
OCD is heritable
Can be passed on generationally as a recessive or dominant trait
Polygenic
Several genetic variations (candidate genes) that contribute to an individuals vulnerability to OCD.
Candidate Genes
SERT
Controls the levels of serotonin available at the synapse by producing reuptake proteins. More reuptake proteins = less serotonin.
A lack of serotonin is associated with OCD
Variation in SERT gene can contribute to the vulnerability to OCD
COMT gene
Controls the levels of dopamine by de-activating it
Irregular dopamine levels is associated with OCD
Variation in COMT gene can contribute to the vulnerability to OCD
Can be ‘awakened’ by environmental factors
Evaluation
Review of twin studies - Billet et al
Concordance rate between monozygotic and dizygotic twins was compared
Findings: MZ = 68%, DZ = 31%
Conclusion: Percentage difference indicates that OCD is partially inherited
Family Studies - Nestadt et al
Two groups were tested, control & experimental
Parents & siblings were interviewed
Findings:
12% of participants with OCD had a relative with OCD
3% of participants without OCD had a relative with OCD
Conclusion:
It is likely that a person with OCD has a relative who also has OCD - OCD is partially inherited
DNA analysis - Hu et al
Two groups were tested, control & experimental
Findings:
OCD were more likely to carry the long allele of the SERT gene (more serotonin reuptake)
Conclusion:
Genetic variation in the SERT gene contributes to the likelihood to develop OCD
Twin Studies
They are based on the assumption that both pairs are the same, and have grown up in the same encironment
Treatments
SSRIs
Commonly used to treat depression, but it is also highly effective for OCD as it also has low serotonin levels.
Serotonin is a neurotransmitter that circulates throughout the body via synapses.
Serotonin that is left in the synapse is taken back into the presynaptic nerve - this reduces the amount of serotonin in the body
SSRIs inhibit the reuptake of serotonin, meaning more serotonin is left in the synapse
Therefore, more serotonin is sent throughout the body.
Anti-anxiety drugs
Benzodiazepines (BZs)
Anti-anxiety drugs designed to induce a feeling of calm. They control neuron hyperactivity, which is associated with fear, anxiety and stress.
They help ‘quieten’ the brain.
Evaluation
Cost-effective and widely-available
cheaper and more readily available
Impact on the economy is lessened
Side effects
SSRIs cause blurred vision, loss of libido, irritability, indigestion and sleep problems
BZs cause drowsiness, light-headedness, confusion, dizziness and slurred speech
Limiting usefulness of these drugs in the treatment of OCD