Care of the adult with Cardiovascular Disorder: Heart Failure (HF) lecture notes (completed)
Overview and Epidemiology of Heart Failure (HF)
Definition: Heart Failure is a complex clinical syndrome resulting in an insufficient blood supply or oxygen delivery to tissues and organs. It involves structural or functional impairments that lead to systolic dysfunction (inadequate pumping) or diastolic dysfunction (inadequate filling).
Epidemiology Statistics:
Nearly people currently experience HF.
It is the most common reason for hospitalization in adults over the age of .
Projections suggest that by the year , over Americans will have HF.
Contributing Trends:
The aging population contributes significantly to prevalence.
Improved survival rates post-Myocardial Infarction (MI) mean more patients live with damaged heart muscle.
Persistent risk factors in the general population maintain high incidence rates.
Cardiac Circulation and Congestion Mechanisms
The Right Heart: Receives deoxygenated blood from the body and pumps it through the pulmonary artery to the lungs for oxygenation.
Path: Superior and inferior vena cava right atrium (tricuspid valve) right ventricle (pulmonic valve) pulmonary artery Lungs.
The Left Heart: Receives oxygenated blood from the lungs and pumps it through the aorta to the rest of the body.
Path: Lungs left atrium (mitral valve) left ventricle (aortic valve) aorta rest of the body.
Hemodynamic Flow and Congestion Pathways:
Systemic/Right Heart focus: Capillaries Veins Vena Cava RIGHT heart LUNGS.
Left Heart/Systemic focus: LEFT heart Arteries Capillaries.
Congestion results in fluid buildup and low output ( deprivation).
Risk Factors for Heart Failure
Primary Risk Factors:
Coronary Artery Disease (CAD), including history of Myocardial Infarction (MI).
Hypertension (HTN).
Contributing Risk Factors:
Diabetes Mellitus.
Metabolic syndrome.
Advancing age.
Tobacco use.
Valvular disease.
Pathophysiology and Compensatory Mechanisms
Initial Development: HF usually begins with left ventricular systolic dysfunction, characterized by diminished pumping ability. Remaining blood increases pressure in pulmonary capillaries, and the left ventricle becomes stiff. Right ventricle dysfunction often follows due to high pulmonary pressure transferring back to the right atrium and systemic circulation.
Sympathetic Nervous System (SNS) Activation:
Triggers the release of catecholamines (epinephrine and norepinephrine).
Leads to increased Heart Rate (HR) and increased myocardial contractility.
This is a temporary compensatory mechanism; eventually, the heart "wears out."
Renin-Angiotensin-Aldosterone System (RAAS):
Causes vasoconstriction and the retention of fluid and sodium.
Leads to increased blood volume and blood pressure (BP).
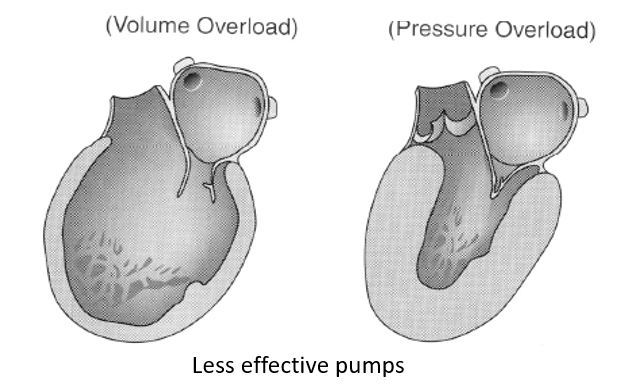
Ventricular Modeling Changes:
Ventricular Dilation: Increase in the size of the heart chambers to accommodate increased blood volume. Myocardial fibers stretch for greater force (Frank-Starling law).
Loss of Elasticity: The heart becomes stiff due to extra volume and pressure.
Myocardial Hypertrophy: Thickening of the heart wall due to increased pressure.
Long-term Effects: While beneficial at first, these mechanisms eventually increase demand and work against the heart, leading to "Ventricular Remodeling" where the heart becomes a less effective pump due to volume and pressure overload.
Classification and Types of Heart Failure
Core Categories:
Left-sided (Think of congested lungs) vs. Right-sided.
Acute vs. Chronic.
Systolic vs. Diastolic.
Acute Heart Failure: An emergency situation where a patient was asymptomatic prior to onset; often seen in acute heart injury like MI.
Chronic Heart Failure: A long-term syndrome where symptoms manifest over a long period, usually resulting from pre-existing cardiac conditions.
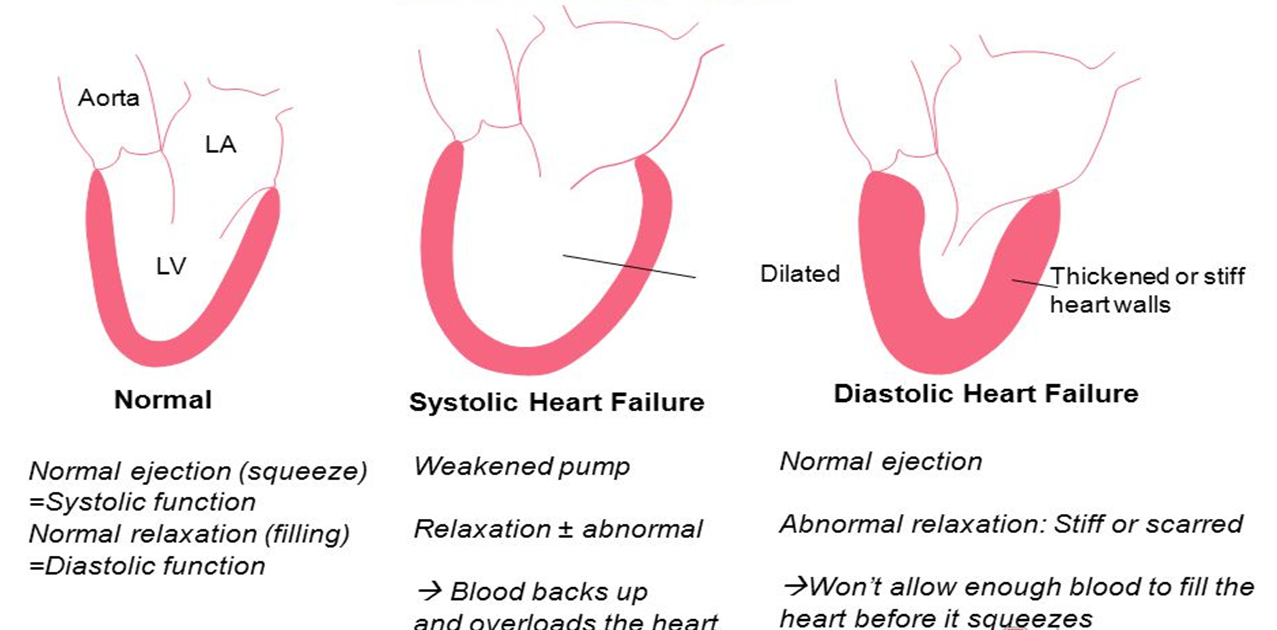
Systolic Dysfunction (Weakened Pump):
Inability to squeeze effectively.
Ejection Fraction (EF) is typically less than .
Results in blood backing up and overloading the heart.
Diastolic Dysfunction (Filling Problem):
The heart walls are thickened or stiff (scarred).
The heart cannot relax/fill enough before it squeezes.
EF may be normal (typically greater than ) but output is low because total volume is low.
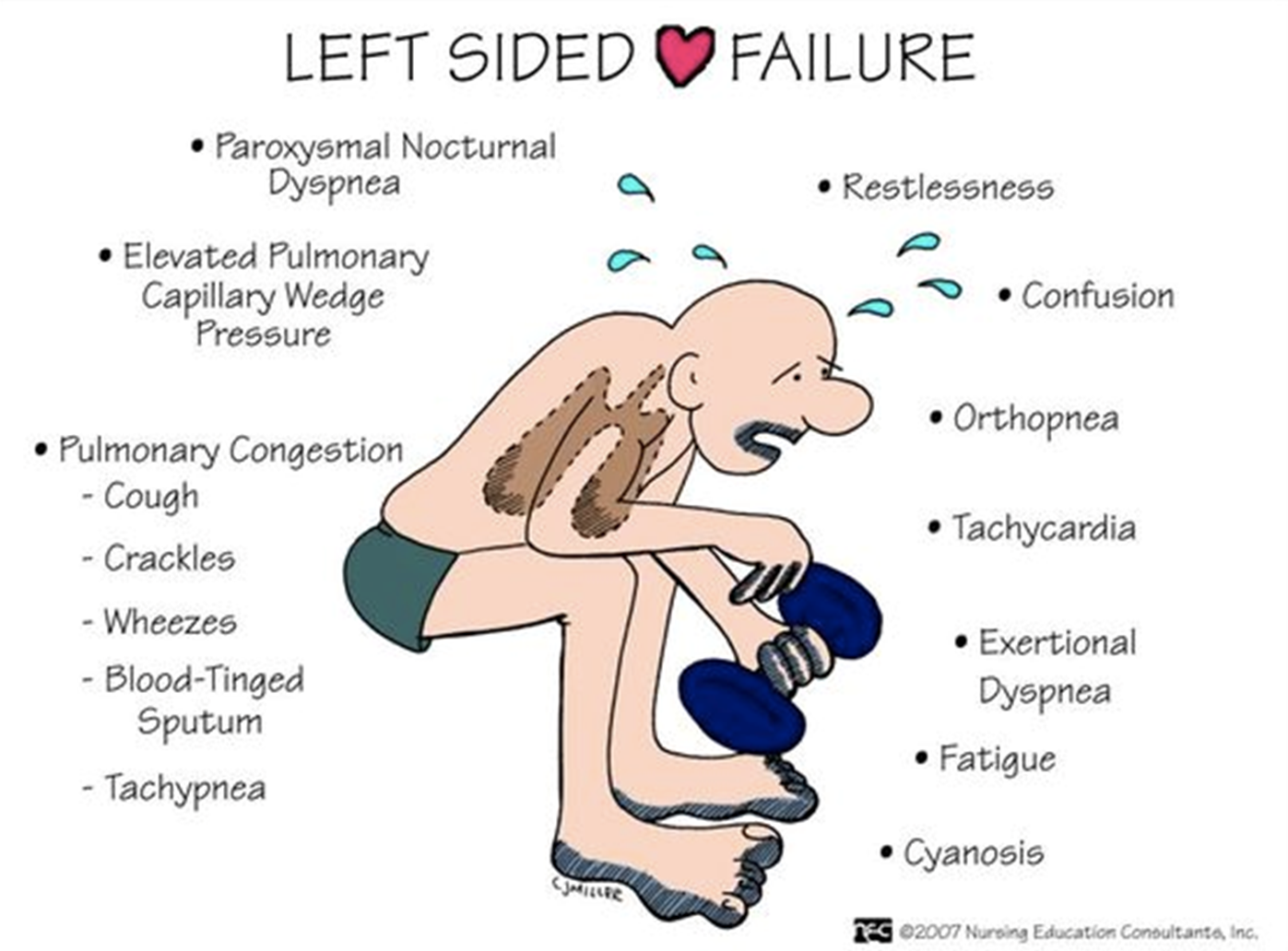
Left-Sided Heart Failure (LHF)
Etiology/Nature: The most common form of HF, often caused by MI or untreated hypertension. It results from the left ventricle's inability to pump adequately during systole or fill adequately during diastole.
Pathophysiology: Blood backs up into the lungs, increasing pulmonary pressure and causing pulmonary edema. This leads to impaired gas exchange.
Classic Symptoms:
Orthopnea (shortness of breath when lying flat).
Exertional dyspnea.
Paroxysmal Nocturnal Dyspnea (PND).
Dry, hacking cough.
Unexplained fatigue.
Physical Assessment Findings:
Tachypnea and use of respiratory accessory muscles.
Wheezing or rales (bubbling crackles).
Tachycardia and S3 gallop.
Elevated Pulmonary Capillary Wedge Pressure.
Restlessness, confusion, and cyanosis (late signs).
Complications: Acute pulmonary edema.
Right-Sided Heart Failure (RHF)
Etiology/Nature: The right ventricle is unable to maintain adequate output. The most common cause is Left-Sided HF (as the failed LV causes pulmonary pressure to rise, the RV must work harder and eventually weakens). Other factors include chronic pulmonary disease (Cor Pulmonale).
Pathophysiology: Blood backs up into the systemic venous system, causing fluid movement into tissues and organs.
Symptoms and Signs:
Peripheral edema (dependent edema is an early manifestation).
Abdominal ascites.
Hepatomegaly (enlarged liver) and Splenomegaly (enlarged spleen).
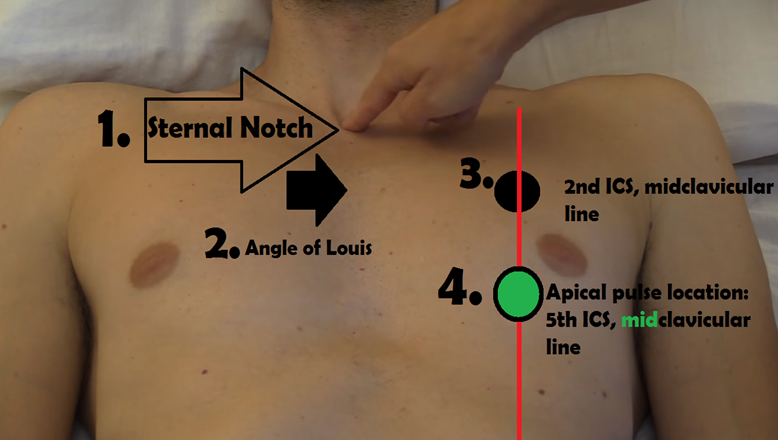
Jugular Venous Distention (JVD) — distended neck veins observed with the patient sitting at a - degree angle.
Unexplained weight gain.
Anorexia, nausea, bloating, and GI distress.
S3 or S4 heart sounds.
Complications: Venous congestion of organs and anasarca (late-stage generalized edema).


Clinical Severity and Classification Systems
FACES Acronym (Symptoms of Worsening HF):
F: Fatigue (one of the earliest chronic symptoms).
A: Limitation of Activities.
C: Chest congestion/cough.
E: Edema (pitting edema).
S: Shortness of breath.
New York Heart Association (NYHA) Functional Class (Dont memorize):
Class 1: No limitation of physical activity. Ordinary activity does not cause fatigue, palpitations, or dyspnea.
Class 2: Slight limitation. Comfortable at rest, but ordinary activity causes fatigue/palpitations/dyspnea.
Class 3-A: Significant limitation. Comfortable at rest, but minimal activity causes symptoms.
Class 3-B: Marked limitation. Comfortable at rest, but ordinary activity results in severe symptoms.
Class 4: Unable to carry on any physical activity without discomfort. Symptoms of HF are present at rest.
ACCF/AHA Staging (Dont memorize):
Stage A: At high risk for HF but without structural heart disease or symptoms.
Stage B: Structural heart disease but without signs or symptoms of HF.
Stage C: Structural heart disease with prior or current symptoms of HF.
Stage D: Refractory HF requiring specialized interventions.
Diagnostic Studies for Heart Failure
Echocardiogram: Provides critical information on Ejection Fraction (EF), heart valves, and chamber size.
Chest X-Ray (CXR): May show cardiac enlargement (cardiomegaly), pulmonary congestion, or edema.
Electrocardiogram (ECG/EKG): May be normal or show indicators of atrial/ventricular enlargement.
Cardiac Catheterization & Nuclear Stress Test: Used primarily for patients with CAD to determine EF and underlying blockages.
Ejection Fraction (EF) Ranges:
Normal: to .
Below Normal: to (may indicate previous MI/damage).
Heart Failure Indicator: Less than .
Hypertrophic Cardiomyopathy Indicator: Higher than .
B-type Natriuretic Peptide (BNP) Labs:
BNP or NT-proBNP (precursor) are released when the heart is stressed or overworked.
Helps differentiate between acute HF and other causes of dyspnea.
Values:
Unlikely HF: < 100\,pg/mL.
Suggests HF present: -.
Mild HF: > 300\,pg/mL.
Moderate HF: > 600\,pg/mL.
Severe HF: > 900\,pg/mL.
Pharmacotherapeutic Management
HF management:
Goals
Improve cardiac performance without increasing cardiac workload.
Improve ability to perform ADLs and reduce symptoms.
Medications are critical part of the care of patients with HF.
Current HF treatments- objectives:
Reduce preload
High Fowler’s position (decrease venous return & enhance lung expansion)
Controlling sodium and water retention (restrict sodium intake, avoid NSAIDs)
Diuretics (decrease blood volume)
Vasodilators
Reduce afterload
ACE Inhibitors/ARBs
Vasodilators
Increase ventricular contractility
Inotropes (digoxin)
ACE Inhibitors (e.g., benazepril, enalapril, lisinopril):
Action: Prevents conversion of Angiotensin I to Angiotensin II; leads to vasodilation, BP reduction, and afterload reduction.
Benefits: Slows ventricular remodeling; excrete sodium and retain potassium.
Side Effects: Dry cough, hyperkalemia, hypotension, dizziness, angioedema.
Angiotensin II Receptor Blockers (ARBs) (e.g., irbesartan, olmesartan, losartan):
Action: Used if ACEIs are not tolerated (e.g., due to cough). Prevents vasoconstriction and aldosterone effects.
Leads to vasodilation.
Also causes decrease in blood pressure and reduction of afterload, allowing heart to not work as hard.
Decrease fluid volume, excrete sodium, retain potassiym.
ARBs slow heart remodeling, preventing the heart from getting weaker over time.
Side Effects: Hyperkalemia, hypotension, dizziness.
Diuretics:
Loop Diuretics (e.g., furosemide/Lasix, bumetanide/Bumex): Potent, rapid onset ( via IV). Reduces preload. Administer in the morning.
Thiazide Diuretics (e.g., HCTZ): Routine management.
Nursing: Monitor output, BP, and lung sounds. Risk of hypokalemia implies a need for potassium-rich foods (bananas, citrus, leafy greens).
Aldosterone Antagonists (e.g., spironolactone/Aldactone, eplerenone/Inspra):
Action: Blocks aldosterone effects; retains potassium (risk of hyperkalemia).
Monitor potassium level, avoid foods high in potassium (bananas, oranges, dried apricots, citrus fruit, green leafy vegetables).
Beta Blockers (e.g., bisoprolol, carvedilol, metoprolol Toprol XL):
Action: Slows HR to allow for complete LV filling; reduces SNS effects.
Nursing: Hold if HR < 50-. Side effects include bradycardia, fatigue, and hypotension.
Teach family to check heart rate for one minute, hold if HR <50-60 bpm.
Positive Inotropes (Digoxin):
Action: Increases contractility force () while slowing HR ().
Sodium forced out of cell in exchange for calcium which increases force of cardiac contraction, increases CO (+ inotropic), improves LV function
Decrease heart rate, slows conduction through AV nodes, ( – chronotropic), more complete emptying from ventricles
Teach patient/family to check heart rate for one minute, Hold digoxin if HR <50-60, report symptoms of toxicity
Toxicity Warning: Symptoms include anorexia, nausea, vomiting, lethargy, halos (yellow-green), and blurred vision. Hypokalemia (often from diuretics) increases toxicity risk.
Vasodilators (Hydralazine & Isosorbide Dinitrate): Add-on therapy for symptomatic patients, particularly African Americans.
Nursing Management and Patient Education
Fluid and Weight Monitoring:
Daily Weights: Same time, same scale, same clothes, after urination, before breakfast.
Reporting Thresholds: Weight gain of over OR - over must be reported to the HCP.
Nutritional Therapy:
Sodium restriction: limit to () per day.
Avoid MSG, baking soda, and baking powder. Try lemon juice or spices.
Avoid canned, pickled, or processed foods (> 400\,mg/serving is too high).
Warning: Do not use salt substitutes (NuSalt) without approval as they contain potassium salts.
HF management:
Activity – acute HF pts on bedrest to minimize O2 demands but increase ASAP after BP, HR, O2 sat stabilize
Referrals – work with many providers to improve quality of life in HF pts including nutritionists, exercise physiologists, RNs, stress management professionals, chaplains, resp therapists, social workers, MDs/NPs
Surgical management – may reverse course of some HF depending on etiology
Medication Safety:
Avoid NSAIDs (causes fluid retention).
Only use Tylenol (acetaminophen) for pain, max daily.
Do not take any herbal medications without the approval of doctor.
Do not take any aspirin in addition to what is prescribed by the health care provider.
Activity and Health Promotion:
Acute HF: Bedrest initially.
Chronic: Walk on flat surfaces; space activities; get - hours of sleep; avoid straining/Valsalva maneuver (lifting, grunting).
Vaccinations: Annual influenza and Pneumococcal (Pneumovax) at diagnosis and regular intervals.
Acute Pulmonary Edema Management
Nature: A life-threatening medical emergency involving fluid accumulation in the alveoli.
Clinical Presentation: Severe dyspnea, orthopnea, and a cough producing frothy, pink (blood-tinged) sputum.
Immediate Care Interventions:
High Fowler’s position or elevating the head of the bed.
Oxygen therapy, BiPAP (to open alveoli and reduce work of breathing), or intubation.
IV access and cardiac monitoring.
Medications: Nitrates (preload/afterload reduction), IV Diuretics, IV Morphine (vasodilation), and ACE inhibitors.
HF: Nursing Assessment
Subjective Data:
Past health history
Hypertension, CAD (including recent MI)
Drugs
Any cardiac drugs, NSAIDs, OTC drugs
Usual sodium intake
Dyspnea, orthopnea, cough
Number of pillows used for sleeping
Paroxysmal nocturnal dyspnea
Objective Data:
Skin color and temperature
Edema
Respiratory rate and sounds
Frothy, blood-tinged sputum
Heart rate and sounds
Abdominal distention
BNP
Serum electrolytes
BUN, creatinine
Liver function tests
Echocardiogram
O2 saturation
HF: Nursing diagnosis
Impaired gas exchange
Decreased cardiac output
Excess fluid volume
Activity intolerance
HF: Nursing management
Impaired gas exchange (or risk for) RT alveolar-capillary membrane changes (e.g., fluid collection, shifts into interstitial space/alveoli)
Desired outcomes
Demonstrate adequate ventilation & oxygenation of tissues by ABGs/pulse oximetry; free of S/S of respiratory distress
Decreased cardiac output RT altered myocardial contractility; alterations in rate, rhythm, electrical conduction.
AEB:
Tachycardia, dysrhythmias Check rhythm of apical pulse
Extra heart sounds (S3, S4)
Decreased urine output
Desired outcomes – cardiac pump effectiveness
Vital signs within acceptable range
No dysrhythmias or controlled
Urinary output adequate
Fluid volume excess RT reduced glomerular filtration rate (decreased cardiac output) & sodium/water retention
AEB:
Orthopnea
Edema, JVD, positive hepatojugular reflux
Weight gain
Desired outcomes
Stabilized fluid volume with balanced I & O
Stable weight
Absence of edema
Activity intolerance RT imbalance between oxygen supply/demand
AEB:
Weakness, fatigue
Dyspnea
Desired outcomes
Participate in desired activities; meet own self-care needs; achieve measurable increase in activity tolerance, evidenced by reduced fatigue & weakness & VS stable for patient
HF: Planning
Overall Goals
Decrease in symptoms
Decrease in peripheral edema
Increase in exercise tolerance
Compliance with the treatment regimen
No complications related to HF
HF: Nursing interventions
Monitor vital signs especially BP, heart rate, pulse oximetry
Auscultate breath sounds and heart sounds
Check apical pulse, heart rate & rhythm
Inspect skin for pallor, cyanosis
Monitor I & O for decreased urine output &/or concentrated urine
Encourage rest, avoid activities that elicit a vasovagal response
Increase activity &/or ambulation as tolerated
If on digoxin, assess for toxicity
Administer medications as ordered
Monitor/replace electrolytes; monitor labs (creatinine, BUN, LFT)
Monitor urine output, noting amount & color
Monitor/calculate 24 hour I & O; look at trends
Maintain chair or bedrest in high Fowler’s position during acute phase
Establish fluid intake schedule if fluids are medically restricted
Provide frequent mouth care
Daily weights – same time, same scale, same clothes, emptied bladder
Assess for distended neck & peripheral vessels. Inspect dependent body areas for edema
Fluid:
Auscultate breath sounds and observe for change in breathing pattern; ROS – dyspnea, tachypnea, orthopnea, paroxysmal nocturnal dyspnea, persistent cough
Investigate reports of sudden extreme dyspnea/ air hunger, sense of suffocation
Monitor vital signs – BP, heart rate; if tachycardic, check rhythm of apical pulse
Assess bowel sounds; ROS anorexia, nausea, abdominal distention, constipation
Provide small, frequent, easily digestible meals; maintain fluid/sodium restriction as indicated
Change position frequently; inspect skin keeping it dry
Palpate the abdomen. Note reports of upper quadrant pain/tenderness
Encourage verbalization of feelings toward limitations
Check vital signs before & immediately after activity
Document cardiopulmonary response to activity
Assess for other precipitators/causes of fatigue
Provide assistance with self-care activities (bedside commode to reduce cardiac workload); intersperse activity periods with rest periods
Cardiac rehabilitation
HF: Evaluation
Monitoring to assess outcomes
Vital Signs – blood pressure, heart rate (check apical pulse if tachycardic)
Pulse oximetry – oxygen saturation
Dyspnea – assessment of lung sounds and breathing pattern, respiratory rate
Weight – assessment of peripheral edema, daily weights, intake and output
Prevent/limit future hospitalizations
Verbalizes understanding of teaching
Achieve a realistic program of activity that balances physical activity with energy-conserving activities
Patient with HF will:
Maintain adequate O2/CO2 exchange to meet O2 needs of the body
Maintain adequate blood pumped by the heart to meet metabolic demands of the body
Experience reduction or absence of edema and stable baseline weight
Achieve a realistic program of activity that balances physical activity with energy-conserving activities.
HF: Patient education
About HF
Expected symptoms, when to call the doctor and report s/s
Self-monitoring, daily weights
Checking heart rate
Reading food labels
Substitutes for sodium
Role of family/caregivers in treatment plan
Take prescribed meds
Patient’s prognosis
Prevent infection
Health promotion: Vaccinations
Annual influenza immunization.
Pneumococcal (Pneumovax) at diagnosis and at regular intervals.
Case Study: M.W. Synthesis
Patient Profile: -year-old woman, history of HTN, CAD, and three previous MIs (last one ago).
Admitting Symptoms: Shortness of breath; ran out of medications ago.
Diagnostics: CXR shows HF; BNP level is ; EF is .
Relevant Questions & Discussion:
Risk Factors: Age, HTN, CAD, repeated MIs, and medication non-compliance.
Follow-up Questions: Check for dietary habits, history of smoking, other contributing factors like diabetes.
Diagnosis Suspected: Based on BNP and EF, Left-sided heart failure (potentially leadings to Right-sided involvement if edema/JVD were present).
Questions & Discussion
Question: The nurse notes JVD, weight gain, peripheral edema, and a HR of . What is suspected?
Answer: Right-sided HF.
Question: The nurse notes exertional dyspnea, orthopnea, crackles, and a HR of . What is suspected?
Answer: Left-sided HF.
Question: Which diagnostic test is most useful for determining if acute dyspnea is heart failure?
Answer: B-type natriuretic peptide (BNP).
Question: An older female patient is effectively taught about HF when she states what?
Answer: She will call the clinic for a weight gain of - in .
Complications, Prognosis, and Palliative Care
Major Complications:
Dysrhythmias: Atrial fibrillation (A-fib) is the most common and increases stroke risk due to blood stasis in atria.
Multisystem failure: Renal failure, hepatomegaly, and pleural effusion.
Call provider if:
Weight gain of 3-5 pounds over a week or 3 pounds over two days
Increase in dyspnea or angina, especially with decreased activity or at rest
Cough or respiratory congestion that lasts longer than 3-4 days
Presence or increase in peripheral edema
Survival Rates Based on NYHA Class (dont memorize):
Class I/II: Survival of from diagnosis.
Class III: Survival of from diagnosis.
Class IV: Survival of from diagnosis.
EndOfLife Care:
Palliative Care: Appropriate at any stage of HF to manage symptoms and improve quality of life.
Hospice Care: Appropriate for Stage D or Class IV patients with a life expectancy of less than .