GI
Terms to be familiar with:
Diarrhea; 3 or more
Gastritis
Peptic ulcer disease
Constipation;
Appendicitis
Peritonitis
Crohn’s disease
Ulcerative colitis
Bowel obstruction
Hernia
GI decompression; removing content from stomach
Diverticulitis;
Strangulated hernia;
Low residue diet
High fiber diet
Digestive System
GI tract - pathway in length that extends from the mouth to esophagus, stomach, small and large intestine, and rectum to the anus.
Major functions: Breakdown of food particles into the molecular form for digestion.
Absorption into the bloodstream of small nutrient molecules produced by digestion.
Elimination of undigested unabsorbed food and other waste products.
Discussion
The nurse is obtaining a health history of a client admitted for dysfunction of the GI system. Using assessment parameters appropriate for determining the status of GI function, what key parameters should the nurse focus on in collecting the client’s GI health history and physical assessment?
1. Health History
Symptoms: Chief complaint, onset, duration, and triggers of symptoms.
Appetite and Diet: Changes in appetite, dietary habits, and food intolerances.
Weight: Recent weight changes indicating potential GI issues.
Bowel Habits: Frequency, consistency, color of stools, and any changes.
Pain: Location, nature, and factors affecting pain or discomfort.
2. Physical Assessment
Inspection: Abdominal shape, distention (acistes, bowel obstruction), and skin changes
Auscultation: Bowel sounds in all quadrants.
Palpation: Tenderness, masses, or abnormal findings.
Percussion: Detection of fluid, air, or organ enlargement.
A client seeking care because of recurrent heartburn and regurgitation is subsequently diagnosed with a hiatal hernia. Which of the following should the nurse include in health education?
A. "Drinking beverages after your meal, rather than with your meal, may bring some relief."
B. "It's best to avoid dry foods, such as rice and chicken, because they're harder to swallow."
C. "Many clients obtain relief by taking over-the-counter antacids 30 minutes before eating."
D. "Instead of eating three meals a day, try eating smaller amounts more often."
Assessment
Health history:
Information about abdominal pain, dyspepsia, gas, nausea and vomiting, diarrhea, constipation, fecal incontinence, jaundice, and previous GI disease is obtained
Dyspepsia
Most common symptom of patients with GI dysfunction
Intestinal gas
Bloating, distention, or feeling “full of gas” with excessive flatulence as a symptom of food intolerance or gallbladder disease
Nausea and vomiting
Nausea is a vague, uncomfortable sensation of sickness or “queasiness” that may or may not be followed by vomiting
Change in bowel habits and stool characteristics
May signal colonic dysfunction or disease
Constipation, diarrhea
Stool characteristics - can vary greatly, normal is light to dark brown
Abnormal
Tarry/black - upper GI bleed
bright/dark red - lower GI bleed
Bulky, greasy, foamy that are foul in odor may or may not float
Light gray or clay colored- decreased or absence of conjugated bilirubin
Stool with mucus thread or pus may be visible on gross inspection of the stool
Small, dry rock hard masses occasional streaked with blood
Loose, watery stool that may or may not be streaked with blood - indicate constipation
Past health, family and social history
Oral care and dental visits
Lesions in mouth
Discomfort with certain foods
Use of alcohol and tobacco
Dentures
Cancers
Pain:
Pain scale, character, duration, pattern, frequency, location, distribution of referred abdominal pain, and time of the pain vary greatly depending on the underlying cause
Physical Assessment
Oral cavity
Lips
Gums; inspect bleeding, breath, etc
Tongue; texture, color, lesion
Pharynx
Abdominal assessment; four quadrant method
draw invisible line to divide quads - Sounds?
Inspection;
Auscultation;
Percussion;
Palpation;
Palpate - determines tenderness, not so much for rebound tenderness because of pain
Rectal inspection
Rectal - inspection of hemorrhoids
Percussion - size, density of abdominal organs, air filled, fluid filled, solid masses, assess tympany, dullness
Quadrants in the abdomen
Epigastric - above the belly button
Umbilical - belly button area
Suprapubic - have you seen a suprapubic catheter? #3
under the belly button; surgically implanted.
Diagnostic Tests
Serum laboratory studies
CBC (WBC,RBC), CMP (ELECTROLYTE AND KIDNEY FUNCTION, PT/PTT, triglycerides, LFT’s, amylase, lipase, CEA, CA 19-9
Stool tests
FOBT
Bacteria, pathogens, parasites
Breath tests; H Pylori (bacteria in the stomach)
Abdominal ultrasonography - appy, gallbladder
Imaging studies: CT (localized inflammation; contrast, kidney function), MRI (abscesses)
Upper GI tract study
drink contrast, stomach motility, detect ulcers,
Lower GI tract study
Endoscopic procedures - EGD, colonoscopy
Diagnostics- r/o, stage, and diagnose various disease states including cancer
Preparation is important. Nursing interventions pg 1217
Inform the primary provider of known medical conditions or abnormal laboratory values that may affect the procedure
Assess for adequate hydration before, during, and immediately after the procedure, and provide education about the maintenance of hydration
Provide health information and procedural education to patients and significant others
Provide instructions about post procedure care and activity restrictions
Help the patient cope with discomfort and alleviate anxiety
Patients undergoing Gastroscopy
Colonoscopy and Flexible Fiber Optic Sigmoidoscopy
Oral Disorders
Lips
Actinic Cheilitis
Herpes Simplex 1
Mouth
Leukoplakia
Candidiasis
Karposi’s sarcoma
Gums
Gingivitis
Periodontitis
Herpes Simplex 1
Leukoplakia
Candidiasis
Karposi’s sarcoma
Gingivitis
Periodontitis
May see these disorders in hospitalized patients. Not necessarily why they are admitted.
Esophageal Disorders
Hiatal hernias
Gastroesophageal reflux disease (GERD)
Barrett esophagus
Esophageal Disorders
Hiatal Hernia- Define
Hernia- opening in the diaphragm through which the esophagus passes becomes enlarged and part of the upper stomach moves up into the lower portion of the thorax also referred to as a sliding hernia
Occurs more often in women than men
Sliding hiatal hernia is more common
Clinical Manifestations - pyrosis, regurgitation, dysphagia.
Vague symptoms - intermittent epigastric pain or fullness after eating
Assessment/ Diagnostics - xray, barium swallow, EGD
Pts may have pyrosis, regurgitation, and dysphagia- many are asymptomatic
Vagus sx are intermittent epigastric pain or fullness after they eat
Large hiatal leads to intolerance to food, n/v, sliding hernias commonly assoc with GERD
Assessment/ Diagnostics - xray, barium swallow, EGD
Management - frequent small feedings
don’t recline for 1 hour after eating to prevent reflux or movement of the hernia and elevate HOB
surgical intervention for those that are symptomatic, done to relieve the reflux versus the repair of the hernia
Gastroesophageal Reflux Disease (GERD)
Common disorder marked by backflow of gastric or duodenal contents into the esophagus that causes troublesome symptoms and/or mucosal injury to the esophagus
Excessive reflux may occur because of an incompetent lower esophageal sphincter, pyloric stenosis, hiatal hernia, or a motility disorder
Incidence: increases with age; irritable bowel syndrome and obstructive airway disorders (asthma, COPD, cystic fibrosis); Barrett esophagus, peptic ulcer disease, and angina
Other risk factors: tobacco use, coffee drinking, alcohol consumption, gastric infection with Helicobacter pylori
GERD- incompetent lower esophageal sphincter, pyloric stenosis, hiatal hernia, or motility disorder
Incidence increases with age also seen in pts with IBS and airway obstructive disorders, BE, peptic ulcer disease, and angina
Association with tobacco use, ETOH, and H. pylori
Medications
Sucralfate given in clinical
Nissan Fundoplication - more severe cases use this surgical procedure
Management of GERD
Low-fat diet
Avoid caffeine, tobacco, beer, milk, foods containing peppermint or spearmint, and carbonated beverages
Avoid eating or drinking 2 hours before bedtime
Elevate the head of the bed by at least 30 degrees
Barret’s Esophagus
Lining of esophageal mucosa becomes damaged by stomach acid
Typically seen in conjunction with GERD, can be precursor to esophageal cancer
Gastric and Duodenal Disorders
Disruption of the mucosal barrier that normally protects the stomach tissue from digestive juices
Acute: rapid onset of symptoms usually caused by dietary indiscretion; self-limiting. Other causes include medications, alcohol, bile reflux, and radiation therapy. Ingestion of strong acid or alkali may cause serious complications
Chronic: prolonged inflammation, atrophy of gastric tissue, due to benign or malignant ulcers of the stomach or by Helicobacter pylori. May also be associated with some autoimmune diseases, dietary factors, medications, alcohol, smoking, or chronic reflux of pancreatic secretions or bile
Erosive- damage stomach lining, frequent use of ASA, NSAIDS, corticosteroids, ETOH, and gastric radiation therapy
Nonreosive- H. Pylori
Erosive Gastritis
Mucosa protects the stomach if no protection eating away in which this may cause ulcerations that may bleed and leak into the abd cavity
Gastritis Manifestations
Acute: epigastric pain, dyspepsia, anorexia, hiccups, nausea, vomiting. Erosive gastritis can lead to melena, hematemesis or hematochezia
Chronic: fatigue, pyrosis, belching, sour taste in the mouth, halitosis, early satiety, anorexia, nausea and vomiting. May have pernicious anemia due to malabsorption of B12. Some are asymptomatic
Definitive diagnosis by endoscopy and biopsy specimen
Medical Management of Gastritis
Acute
Refrain from alcohol and food until symptoms subside
Supportive therapy: IV fluids, nasogastric intubation, antacids, histamine-2 receptor antagonists, proton pump inhibitors
Chronic
Modify diet, promote rest, reduce stress, avoid alcohol and NSAIDs
Pharmacologic therapy including a variety of medications (Table 40-2)
Appetite my be diminished for an additional 2-3 days
Nursing Management
Reduce anxiety; use calm approach and explain all procedures and treatments
Promote optimal nutrition; for acute gastritis, the patient should take no food or fluids by mouth. Introduce clear liquids and solid foods as prescribed. Evaluate and report symptoms. Discourage caffeinated beverages, alcohol, cigarette smoking. Refer for alcohol counseling and smoking cessation
• Promote fluid balance; monitor I&O, for signs of dehydration, electrolyte imbalance, and hemorrhage
Measures to relieve pain: diet and medications
Test Your Knowledge #2
A client who experienced a large upper gastrointestinal (GI) bleed due to gastritis has had the bleeding controlled and is now stable. For the next several hours, the nurse caring for this client should assess for what signs and symptoms of recurrence?
A. Tachycardia, hypotension, and tachypnea
B. Tarry, foul-smelling stools
C. Diaphoresis and sudden onset of abdominal pain
D. Sudden thirst, unrelieved by oral fluid administration
A client was treated in the emergency department and critical care unit after ingesting bleach. What possible complication of the resulting gastritis should the nurse recognize?
A. Esophageal or pyloric obstruction related to scarring
B. Uncontrolled proliferation of H. pylori
C. Gastric hyperacidity related to excessive gastrin secretion
D. Chronic referred pain in the lower abdomen
Peptic Ulcer Disease
Erosion of a mucous membrane forms an excavation in the stomach, pylorus, duodenum, or esophagus
Associated with infection of H. pylori, not stress, stress can aggravate
Risk factors include excessive secretion of stomach acid, dietary factors, chronic use of NSAIDs, alcohol, smoking, and familial tendency
Manifestations include a dull gnawing pain or burning in the midepigastrium; heartburn and vomiting may occur
Treatment includes medications (Table 40-3), lifestyle changes, and occasionally surgery (Table 40-4)
Gastric Ulcer- pain is after eating versus Duodenal Ulcer 2-3 hours later
History including presenting signs and symptoms
Dietary history and dietary associations with symptoms such as predictable time for pain
72-hour diet; a diary may be helpful
Abdominal assessment, vital signs
Medications; include use of NSAIDs
Sign and symptoms of anemia or bleeding
Nursing Interventions for the Patient with Gastritis or Peptic Ulcer Disease
Relieving pain
Reducing anxiety
Maintaining optimal nutritional status
Monitoring and managing potential complications
Hemorrhage
Perforation and penetration
Gastric outlet obstruction
Patient education
Management of Patients with Intestinal and Rectal Disorders
Elimination Abnormalities
Constipation
Defined as fewer than three bowel movements weekly or bowel movements that are hard, dry, small, or difficult to pass
Causes include medications, chronic laxative use, weakness, immobility, fatigue, inability to increase intra-abdominal pressure, diet, ignoring urge to defecate, and lack of regular exercise
Perceived constipation: a subjective problem in which the person’s elimination pattern is not consistent with what he or she believes is normal
Manifestations of Constipation
Fewer than three bowel movements per week
Abdominal distention, pain, and bloating
A sensation of incomplete evacuation
Straining at stool
Elimination of small-volume, hard, dry stools
Assessment and Diagnostic Findings of Constipation
Chronic constipation is usually idiopathic
Further testing for severe, intractable constipation
Thorough history and physical examination
Barium enema, sigmoidoscopy, and stool testing
Defecography and colonic transit studies
MRI
Complications of Constipation
Decreased cardiac output (Valsalva manuever)
Fecal impaction
Hemorrhoids
Fissures
Rectal prolapse
Megacolon
Fecal impaction- digital removal/ enema
Megacolon- fecal mass that can obstruct the colon may lead to perforation of the colon and contents leak into the sterile peritoneal cavity (peritonitis)
Management
Medical Management
Identify underlying cause and aim to prevent recurrence
Medication
Laxatives
Medications that enhance colonic transit
Nursing Management
Health hx interview focusing on symptoms of constipation
Teaching/Education Chart 41-2 pg 1289
Pt needs to include education, exercise, bowel habit training, increased fiber and fluid intake and judicious use of laxatives
Increase fiber slowly in the diet to avoid cramping/ bloating
Enemas and rectal supp are generally not recommended for treating constipation unless other meds have failed
Diarrhea
Increased frequency of bowel movements (more than three per day) with altered consistency (i.e., increased liquidity) of stool
Usually associated with urgency, perianal discomfort, incontinence, or a combination of these factors
May be acute, persistent, or chronic
Causes include infections, medications, tube feeding formulas, metabolic and endocrine disorders, and various disease processes
Manifestations of Diarrhea
Increased frequency and fluid content of stools
Abdominal cramps
Distention
Borborygmus
Anorexia and thirst
Painful spasmodic contractions of the anus
Tenesmus
Assessment and Diagnostic Findings of Diarrhea
CBC
Serum chemistries
Urinalysis
Stool examination
Endoscopy or barium enema
Ask patient about recent travel
if cause is not obvious may do CBC, metabolic profile, stool sample for infectious or parasitic organisms, bacterial toxins, blood, fat, electrolytes, and WBCs
Clostridium Difficile most commonly identified agent in antibiotic associated diarrhea
Endoscopy and Barium Enema may be used.
Complications of Diarrhea
Fluid and electrolyte imbalances
Dehydration
Cardiac dysrhythmias
Chronic diarrhea can result in skin care issues related to irritant dermatitis
Management
Medical
Directed at controlling symptoms, preventing complications, and eliminating or treating underlying disease
Medications used: antibiotics, anti-inflammatory agents, anti-diarrheals
Nursing
Health Hx- including any exposure to acute illness or travel outside of country
Assess and monitor characteristics and pattern of diarrhea
Abdominal Examination
During acute phase encourage bedrest and intake of liquids and low bulk foods, then advance to bland diet of semisolids and solid foods.
Anti-diarrheals (not long term)
Rectal tubes- bowel management system Figure 41-1
Use to eliminate fecal skin contact and are especially used when there is extensive excoriation or skin breakdown
Tube is placed in the rectum to drain stool short term use no more than 4 weeks
Patient Learning Needs for Diarrhea
Recognition of need for medical treatment
Rest
Diet and fluid intake
Avoid irritating foods, including caffeine, carbonated beverages, very hot and cold foods
Perianal skin care
Medications
May need to avoid milk, fat, whole grains, fresh fruit, and vegetables
Lactose intolerance
Irritable Bowel Syndrome
Chronic functional disorder characterized by recurrent abdominal pain associated with disordered bowel movements, which may include diarrhea, constipation, or both (IBS-D, IBS-C, IBS-M)
Triggers: chronic stress, sleep deprivation, surgery, infections, diverticulitis, and some foods
Manifestations: Wide variability in symptom presentation, range in intensity and duration from mild and infrequent to severe and continuous
Pain, bloating, and abdominal distention may be present
More common in women than men before age of mid 40’s,
Assessment/Diagnostics: ROME IV, stool diary using the Bristol Stool Form, CBC, C-reactive protein, stool studies, and colonoscopy
Patient Learning Needs for Irritable Bowel Syndrome
Medication management
Aimed at relieving abdominal pain, controlling the diarrhea or constipation, and reducing stress
Try to identify foods that are irritants (food diary)
High Fiber Diet
Exercise and Stress Reduction
Complimentary medicine (peppermint oil)
Dietary changes
Food diary
Adequate fluid intake
Avoid alcohol and smoking
Relaxation techniques
Medications Medical
IBS-D- antidiarrheal agents
All pts- antispasmodic agents, antidepressants these both improve abd comfort
probiotics- decrease and bloating/gas
Nursing Management
Provide patient and family education
Good dietary habits, avoidance of triggers
Eat at regular times, chew food slowly and thoroughly
Acute Abdomen
-
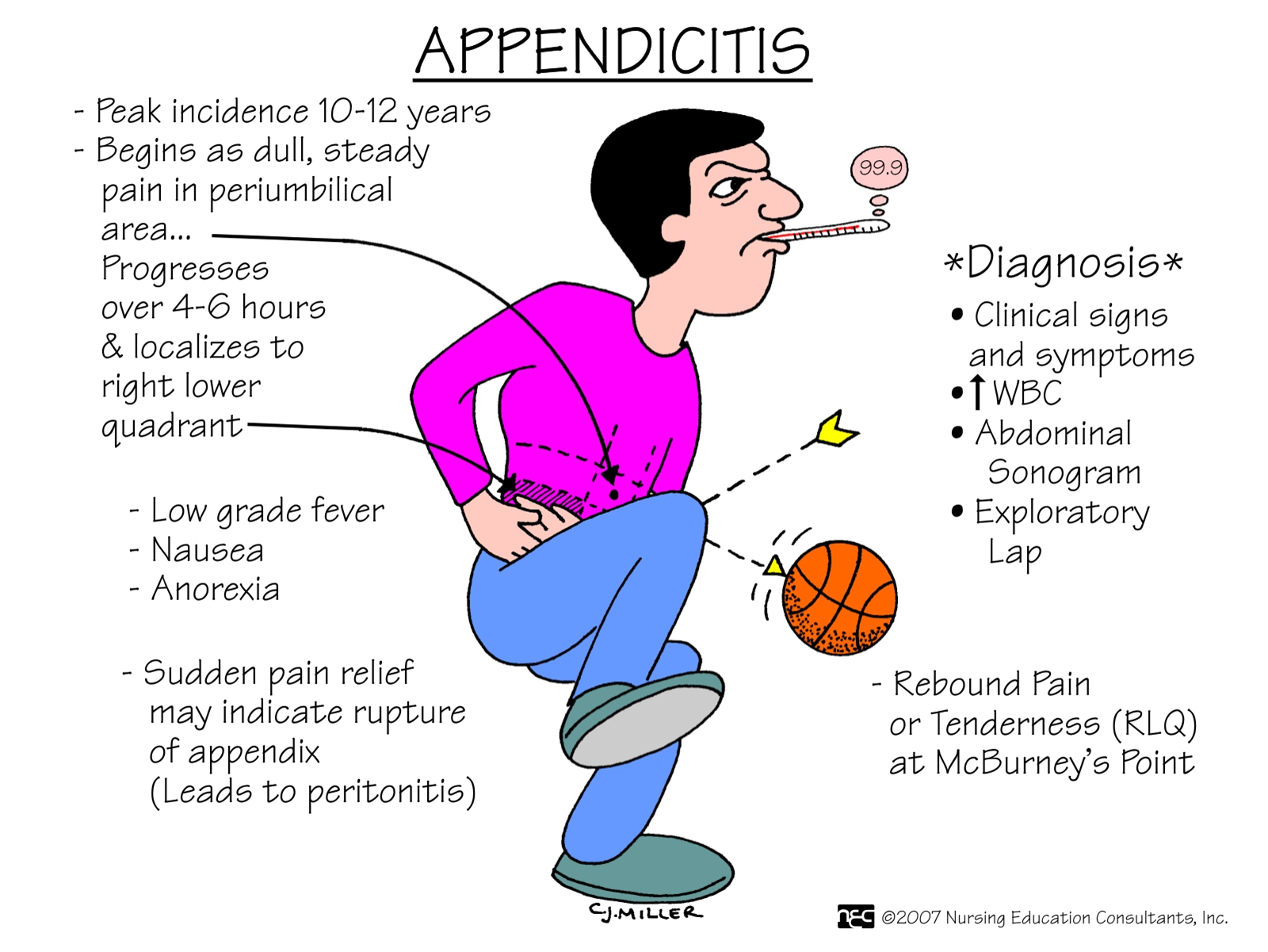
Appendicitis
Appendicitis is the most frequent cause of acute abdomen in the United States, most common reason for emergency abdominal surgery
Appendix becomes inflamed and edematous as a result of becoming kinked or occluded by a fecalith or lymphoid hyperplasia
The inflammatory process increases intraluminal pressure, causing edema and obstruction of the orifice
Once obstructed, the appendix becomes ischemic, bacterial overgrowth occurs, and eventually gangrene or perforation occurs
Clinical Manifestations
Epigastric or peri-umbilical pain that progresses to RLQ pain, N/V, low grade fever, loss of appetite, tenderness at
McBurney’s point, rebound tenderness, possible constipation
Diagnosis
Based on physical exam, labs, and imaging studies
Management
Emergent Appendectomy unless perforation has occurred
Labs WBC increased, Plt increased, CT scan or US go to definitive
Preg test, trans vaginal US may ne used to confirm diagnosis
NPO
Urinalysis- r/o UTI, kidney stones
Goals include:
Relieving pain
Preventing fluid volume deficit
Reducing anxiety
Preventing or treating surgical site infection
Preventing atelectasis
Maintaining skin integrit
Attaining optimal nutrition
Diverticular Disease
Diverticulum: sac-like herniation of the lining of the bowel that extends through a defect in the muscle layer
May occur anywhere in the intestine but most common in the sigmoid colon
Diverticulosis: multiple diverticula without inflammation
Diverticulitis: infection and inflammation of diverticula
Diverticular disease increases with age and is associated with a low-fiber diet
Diagnosis is usually by colonoscopy
Nursing Management of Diverticulitis
Encourage fluid intake of at least 2 L/day
Soft foods with increased fiber, such as cooked vegetables
Avoid foods such as nuts and popcorn
Individualized exercise program
Bulk laxatives (psyllium) and stool softeners
Medical Management
Inpatient treatment
In acute cases hospitalization can be necessary for older and immunocompromised, taking steroids, and unable to tolerate oral fluids. Treatments would include:
NPO until symptoms subside, IV fluids, NGT if vomiting or distention, antibiotics for 7-10 days, opioid analgesics, antispasmodics, low fiber diet once infection signs decrease
Surgery is an option
Outpatient treatment
Rest, analgesics, and anti-spasmodics
Clear liquid diet until inflammation subsides, then high-fiber, low fat diet
Antibiotics for 7-10 days
Bulk-forming laxatives
Complications
Peritonitis, abscess, fistulas, and bleeding
Manifestations
Diffuse pain becomes constant, localized and more intense. Movement aggravates the pain, affected areas tender and distended, and the muscle becomes rigid
Rebound tenderness, anorexia, n/v, peristalsis is dimished followed by paralytic ileus
Increased temp, hr progresses with hypotension oliguric and anuric will mirror those with sepsis and septic shock
Medical Management
Fluids, electrolyte replacement, analgesics, antiemetics, oxygen, abx, nutritional support
Nursing
Assessment, fluids, food intake
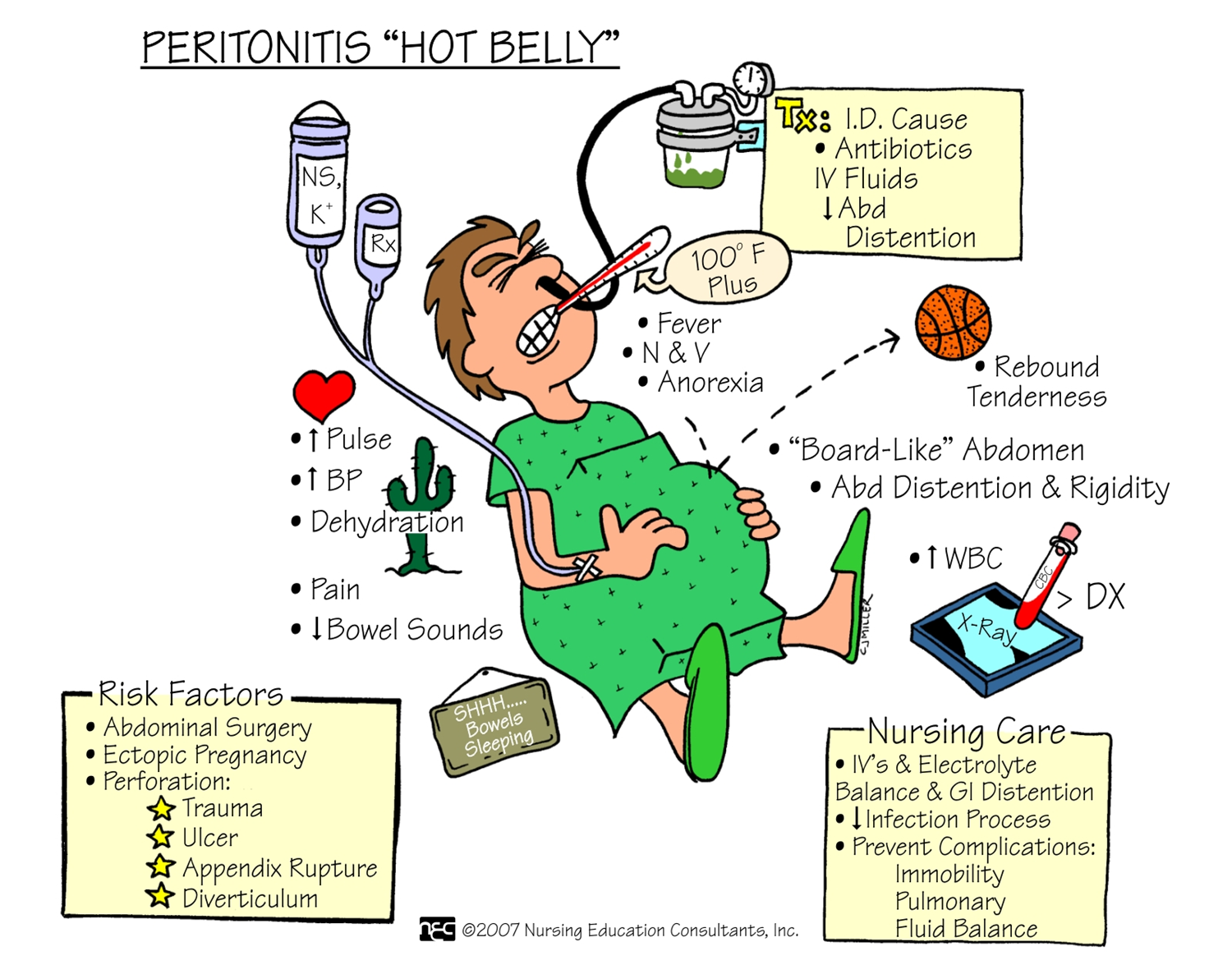
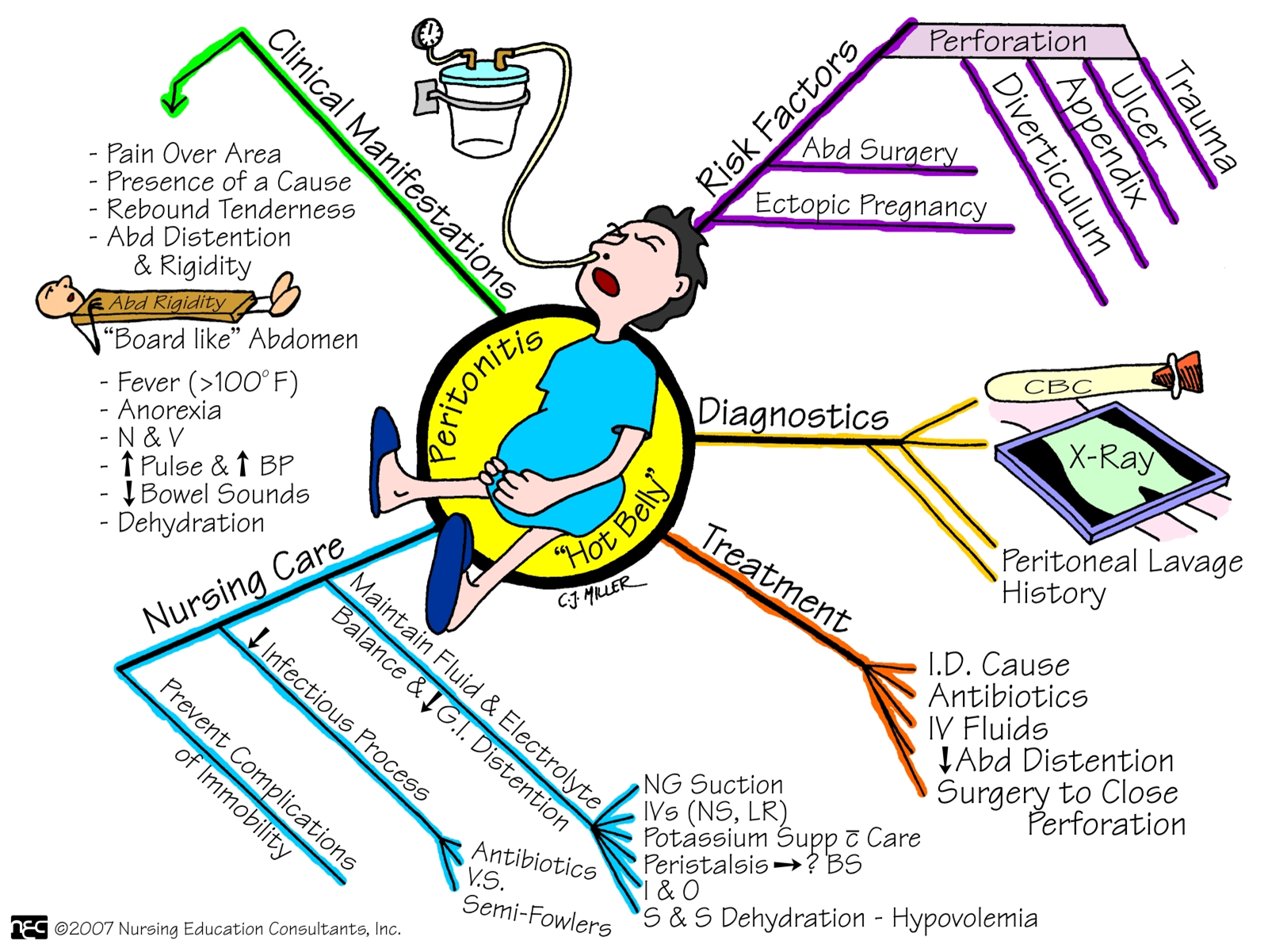
Peritonitis
Inflammation of the peritoneum
Can result from external or internal source
Leakage of contents from abdominal organs into abdominal cavity, bacterial proliferation occurs, leads to tissue edema and exudation of fluid.
Manifestations
Based on location and extent of inflammation
Diagnostics
X-ray, abdominal U/S, CT scan
Management
Supportive tx of symptoms, antibiotics &fluids, surgical interventions
Manifestations
Diffuse pain becomes constant, localized and more intense.
Movement aggravates the pain, affected areas tender and distended, and the muscle becomes rigid
Rebound tenderness, anorexia, n/v, peristalsis is dimished followed by paralytic ileus
Increased temp, hr progresses with hypotension oliguric and anuric will mirror those with sepsis and septic shock
Medical management
Fluids, electrolyte replacement, analgesics, antiemetics, oxygen, abx, nutritional support
Nursing
Assessment, fluids, food intake
Inflammatory Bowel Disease Chronic
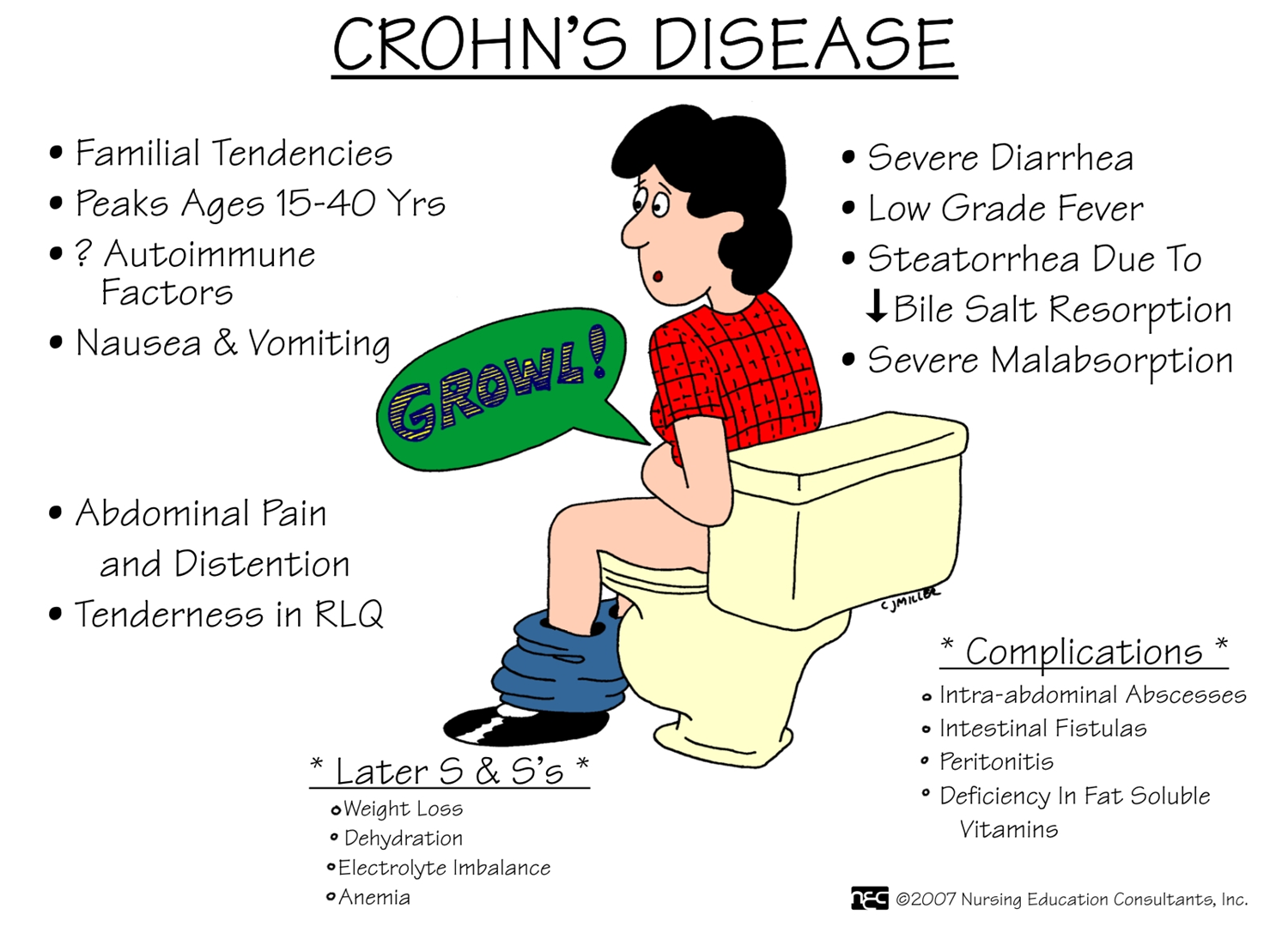
Chron’s Disease
Regional Enteritis
Subacute and chronic inflammation that extends through all layers of GI tract wall
Most commonly occurs in distal ileum and ascending colon
Course is prolonged and variable, are some periods of remissions and exacerbations
Fistulas, Fissures, and Abscesses common
Ulcerative Colitis
Ulcerative and inflammatory disease of mucosal and submucosal layer
Most commonly occurs in rectum and colon
Periods of remissions and exacerbations
Fistulas and Fissures are uncommon
Chron’s- inflammatory process that begins with crypt inflammation & abscesses which turn into small, focal ulcers
Bowel wall thickens and becomes fibrotic and the intestinal wall narrows, diseased bowel loops can adhere to other loops surrounding them
Sx- insidious with diarrhea and prominent RLQ pain unrelieved by defecation
Eating can cause intestinal peristalsis, crampy pain pt tend not to eat leads to weigh loss and malnutrition and secondary anemia
Ulcers can leak a discharge in the colon
Disrupted absorption can cause chronic diarrhea and nutritional deficits---- weight loss and dehydration
Inflammed intestine perforates- lead to intrabdominal abscess----- fever, leukocytosis, chronnc symptoms- diarrhea, abd pain, steatorrhea, anorexia, weight loss, and nutritional deficiencies
CT scan, MRI, CBC, albumin and protein levels
Complications-intestinal obstruction or structure formation, perianal disease, fluid and electrolyte imbalances, malnutrition, fistula and abscess formation
Ulcerative Colitis
Bouts of abd cramps and bloody or purulent diarrhea, typically begin in rectum and progress through the colon
Bleeding occurs because of the ulcerations, the mucosa becomes edematous and inflamed , lesions occur one after the other, bowel eventually shortens, narrows, and thickens because of the muscular hypertrophy and fate deposits
The inflammatory is not transmural (only the inner lining) that is why abscesses, fistulas, obstruction, and fissures
Sx- diarrhea, with passage of mucus, pus, blood. LLQ, pain, tenesmus
Bleeding can be mild or severe. May see pallor, anemia, and fatigue. Anorexia, weight loss, fever, vomiting, dehydration. Cramping and the passage of at least 6 stools per day
Classified as mild, severe, fulminant depending on how severe the symptoms are
Hypoalbuminemia, electrolyte imbalance, and anemia
Extraintestinal manifestaions such as skin lesions, eye lesions, and joint abnormalities, and liver disease
Assessment/Diagnostics
Abd xray, Colonoscopy. Biopsies may be taken
CT scan, MRI, and US- indicate abscess
CBC- WBC, Hgb, HCT, electrolytes, stool for occult and parasites, C-reactive proteins
Complications
Toxic megacolon, perforation, bleeding- ulceration. Surgical intervention may be needed
Steroid use can lead to diminshed bone density
Colon cancer may develop
Management of Chron’s and UC
Nutritional Therapy
Oral Fluids
Low Residue High Protein High Calorie Diet
Vitamin Replacement
Pharmacologic Therapy
Corticosteroids, Immunomodulators, Aminosalicylates
Surgical Management
Stricturplasty
Intestinal transplant
Colectomy
See pg 1306 Table 41-5 and Nursing process pg 1310-1312
Bowel Obstruction
Can be mechanical or functional obstruction
Obstruction can be partial or complete and located in small or large bowel.
Most obstructions occur in the small intestine and are caused by adhesions
Manifestations
In SBO initial symptom is usually crampy pain that is wave-like and colicky. Other symptoms can include vomiting, dehydration, abdominal distention.
In LBO symptoms develop and progress relatively slowly. May experience constipation that can last for months, weakness, weight loss, anorexia. Eventually ABD will become distended and pt will have crampy lower abdominal pain.
Diagnosis
Typically diagnosed by abdominal Xray or CT
Management
Decompression of bowel through NG tube, if unsuccessful or if obstruction is complete surgical intervention is necessary
Diagnosis based on symptoms, physical findings, results of imaging
Bowel sounds are high-pitched and hyperactive in an attempt to pass obstruction
Later hypoactive, may indicate strangulation when there is a change in pattern
Lab studies CBC, electrolytes reveal dehydration, loss of plasma volume, and possible infection
Gastric Tubes
NGT (for suction or feeds)
Large-bore (larger than 12 Fr)
Small-bore (Dobhoff)
Gastric
Stomach
Duodenum
Proximal jejunum
Nasoduodenal and nasojejunal feedings are indicated when the esophagus and stomach needs to be bypassed or when the patient at risk for aspiration
Tube feedings longer than 4 weeks, gastrostomy or jejunostomy tubes are preferred admin of meds or nutrition
Nursing assessment Chart 39-5 pg 1246
Complications- dumping syndrome, aspiration, residual checks, and patency
Xrays should be performed before using an NGT pg. 1249-1252
G-tube and J-tube
Peds- may have a PEG “button” than a tube
Nutrition
Parenteral Nutrition
Provides nutrients to the body by IV route
Given through Peripheral or Central Line, depends on pt condition
Inability to ingest at least 50% of daily required calories
Timeframe when to start depend on pt
Length of therapy is usually 5-7 days
Enteral Nutrition
Given to meet nutritional requirements when oral intake is inadequate or not possible and the middle and lower portions of the GI tract are functionally normal.
Can be given through NG, ND, G-tube, J-tube
Parental Nutrition- mixture of providing nutrients proteins, carbs, fats, electrolytes, vit, trace minerals, sterile water
Table 41-6 pg 1313 Indications for Parental Nutrition
Start therapy slow then increase to goal
Give peripheral route because solution is less hypertonic, not nutritionally complete because of the low dextrose content
Give central route because it is very high in solute concentration of blood
Diets
High Fiber Diet
Increases bulk in stool and reduces pressure within the colon
Low Residue Diet
Residue includes any food, including fiber that remains in your intestinal tract and contributes to stool.
Low Residue Diet is like low-fiber
May be used following abdominal surgery or during a flare-up of a digestive disorder such as diverticulitis or IBD.
Should only be used for a short time because it cannot provide al the nutrients necessary for staying healthy.
Foods that can be consumed include refined breads, cereals, crackers, chips, and pasta with less than 1 gram of fiber/serving, white rice, fruit juice with no pulp, strained broth-based soups
Foods to avoid whole grain breads, cereals, and pastas, peanut butter, seeds and nuts, tough or coarse meats
Surgeries
Avoided until complications such as bowel obstruction, perforation abscess and perianal occur.
Bowel resection-end to end anastomosis remove diseased portion and retaining as much bowel as possible
Ostomy-surgical creation of an opening into the bowel, allows for drainage of fecal matter to the outside of the body.
Name of ostomy is based on its location
Colostomy is opening into large colon (formed)
Ileostomy is opening into the ileum or small intestine (liquid)
Nursing Care for Ostomy
Abd surgery post op
Ambulation
Pain meds
Monitor for fecal drainage 24-48 hours after ileostomy, 3-6 after colostomy
Monitor labs esp electrolytes, fluid replacement
NGT to suction may be indicated
Emotional support
Managing skin and stoma care, change appliance
Managing dietary and fluid needs
Preventing complications
Chart 41-9 pg 1325
Management of Patients with Intestinal and Rectal Disorders
Elimination Abnormalities
Constipation
Defined as fewer than three bowel movements weekly or bowel movements that are hard, dry, small, or difficult to pass
Causes include medications, chronic laxative use, weakness, immobility, fatigue, inability to increase intra-abdominal pressure, diet, ignoring urge to defecate, and lack of regular exercise
Perceived constipation: a subjective problem in which the person’s elimination pattern is not consistent with what he or she believes is normal
Manifestations of Constipation
Fewer than three bowel movements per week
Abdominal distention, pain, and bloating
A sensation of incomplete evacuation
Straining at stool
Elimination of small-volume, hard, dry stools
Assessment and Diagnostic Findings of Constipation
Chronic constipation is usually idiopathic
Further testing for severe, intractable constipation
Thorough history and physical examination
Barium enema, sigmoidoscopy, and stool testing
Defecography and colonic transit studies
X-ray, colonoscopy, lower GI endoscopy
Complications of Constipation
Decreased cardiac output (Valsalva manuever)
Fecal impaction - digital removal/ enema
Hemorrhoids
Fissures
Rectal prolapse
Megacolon - fecal mass that can obstruct the colon may lead to perforation of the colon and contents leak into the sterile peritoneal cavity (peritonitis)
Management
Medical Management
Identify underlying cause and aim to prevent recurrence
Medication
Laxatives
Medications that enhance colonic transit
Nursing Management
Health hx interview focusing on symptoms of constipation
Teaching/Education Chart 41-2 pg 1289
Pt needs to include education, exercise, bowel habit training, increased fiber and fluid intake and judicious use of laxatives
Increase fiber slowly in the diet to avoid cramping/ bloating
Enemas and rectal supp are generally not recommended for treating constipation unless other meds have failed
Diarrhea
Increased frequency of bowel movements (more than three per day) with altered consistency (i.e., increased liquidity) of stool
Usually associated with urgency, perianal discomfort, incontinence, or a combination of these factors
May be acute, persistent, or chronic
Causes include infections, medications, tube feeding formulas, metabolic and endocrine disorders, and various disease processes
Manifestations of Diarrhea
Increased frequency and fluid content of stools
Abdominal cramps
Distention
Borborygmus
Anorexia and thirst
Painful spasmodic contractions of the anus\
Tenesmus
Assessment and Diagnostic Findings of Diarrhea
CBC
Serum chemistries
Urinalysis
Stool examination
Endoscopy or barium enema
Ask patient about recent travel if cause is not obvious may do CBC, metabolic profile, stool sample for infectious or parasitic organisms, bacterial toxins, blood, fat, electrolytes, and WBCs
Clostridium Difficile most commonly identified agent in antibiotic associated diarrhea
Endoscopy and Barium Enema may be used.
Complications of Diarrhea
Fluid and electrolyte imbalances
Dehydration
Cardiac dysrhythmias
Chronic diarrhea can result in skin care issues related to irritant dermatitis
Management
Medical
Directed at controlling symptoms, preventing complications, and eliminating or treating underlying disease
Medications used: antibiotics, anti-inflammatory agents, anti-diarrheals
Nursing
Health Hx- including any exposure to acute illness or travel outside of country
Assess and monitor characteristics and pattern of diarrhea
Abdominal Examination
During acute phase encourage bedrest and intake of liquids and low bulk foods, then advance to bland diet of semisolids and solid foods.
Anti-diarrheals (not long term)
Rectal tubes- bowel management system Figure 41-1
Use to eliminate fecal skin contact and are especially used when there is extensive excoriation or skin breakdown
Tube is placed in the rectum to drain stool short term use no more than 4 weeks
Patient Learning Needs for Diarrhea
Recognition of need for medical treatment
Rest
Diet and fluid intake
Avoid irritating foods, including caffeine, carbonated beverages, very hot and cold foods
Perianal skin care
Medications
May need to avoid milk, fat, whole grains, fresh fruit, and vegetables
Manage lactose intolerance
Irritable Bowel Syndrome
Chronic functional disorder characterized by recurrent abdominal pain associated with disordered bowel movements, which may include diarrhea, constipation, or both (IBS-D, IBS-C, IBS-M)
Triggers: chronic stress, sleep deprivation, surgery, infections, diverticulitis, and some foods
Manifestations: Wide variability in symptom presentation, range in intensity and duration from mild and infrequent to severe and continuous
Pain, bloating, and abdominal distention may be present
More common in women than men before age of mid 40’s,
Assessment/Diagnostics: ROME IV, stool diary using the Bristol Stool Form, CBC, C-reactive protein, stool studies, and colonoscopy
Patient Learning Needs for Irritable Bowel Syndrome
Medication management
Aimed at relieving abdominal pain, controlling the diarrhea or constipation, and reducing stress
Try to identify foods that are irritants (food diary)
High Fiber Diet
Exercise and Stress Reduction
Complimentary medicine (peppermint oil)
Dietary changes
Food diary
Adequate fluid intake
Avoid alcohol and smoking
Relaxation techniques
Medications Medical
IBS-D- antidiarrheal agents
All pts- antispasmodic agents, antidepressants these both improve abd comfort
Probiotics- decrease abd bloating/gas
Nursing Management
Provide patient and family education
Good dietary habits, avoidance of triggers
Eat at regular times, chew food slowly and thoroughly
Acute Abdomen
Appendicitis
Appendicitis is the most frequent cause of acute abdomen in the United States, most common reason for emergency abdominal surgery
Appendix becomes inflamed and edematous as a result of becoming kinked or occluded by a fecalith or lymphoid hyperplasia
The inflammatory process increases intraluminal pressure, causing edema and obstruction of the orifice
Once obstructed, the appendix becomes ischemic, bacterial overgrowth occurs, and eventually gangrene or perforation occurs
Clinical Manifestations
Epigastric or peri-umbilical pain that progresses to RLQ pain, N/V, low grade fever, loss of appetite, tenderness at McBurney’s point, rebound tenderness, possible constipation
Diagnosis
Based on physical exam, labs, and imaging studies
Management
Emergent Appendectomy unless perforation has occurred
Labs WBC increased, CRP, CT scan or US go to definitive
Preg test, trans vaginal US may ne used to confirm diagnosis
NPO
Urinalysis- r/o UTI, kidney stones
Goals include:
Relieving pain
Preventing fluid volume deficit
Reducing anxiety
Preventing or treating surgical site infection
Preventing atelectasis
Maintaining skin integrity
Attaining optimal nutrition
Peritonitis
Inflammation of the peritoneum
Can result from external or internal source
Leakage of contents from abdominal organs into abdominal cavity, bacterial proliferation occurs, leads to tissue edema and exudation of fluid.
Manifestations
Based on location and extent of inflammation
Diffuse pain becomes constant, localized and more intense.
Movement aggravates the pain, affected areas tender and distended, and the muscle becomes rigid
Rebound tenderness, anorexia, n/v, peristalsis is diminished followed by paralytic ileus
Increased temp, hr progresses with hypotension oliguric and anuric will mirror those with sepsis and septic shock
Diagnostics
X-ray, abdominal U/S, CT scan
Management
Supportive tx of symptoms, antibiotics &fluids, surgical interventions
Fluids, electrolyte replacement, analgesics, antiemetics, oxygen, abx, nutritional support
Nursing Assessment, fluids, food intake
Diverticular Disease
Diverticulum: sac-like herniation of the lining of the bowel that extends through a defect in the muscle layer
May occur anywhere in the intestine but most common in the sigmoid colon
Diverticulosis: multiple diverticula without inflammation
Diverticulitis: infection and inflammation of diverticula
Diverticular disease increases with age and is associated with a low-fiber diet
Diagnosis is usually by colonoscopy
Nursing Management of Diverticulitis
Medical Management
Inpatient treatment
In acute cases hospitalization can be necessary for older and immunocompromised, taking steroids, and unable to tolerate oral fluids. Treatments would include:
NPO until symptoms subside, IV fluids, NGT if vomiting or distention, antibiotics for 7-10 days, opioid analgesics, low fiber diet once infection signs decrease
Surgery is an option
Outpatient treatment
Rest, analgesics, and selective antibiotics
Clear liquid diet until inflammation subsides, then high-fiber, low fat diet
Antibiotics for 7-10 days
Bulk-forming laxatives
Complications
Peritonitis, abscess, fistulas, and bleeding
Inflammatory Bowel Disease Chronic
Chron’s Disease
Regional Enteritis
Subacute and chronic inflammation that extends through all layers of GI tract wall
Most commonly occurs in distal ileum and ascending colon
Course is prolonged and variable, are some periods of remissions and exacerbations
Fistulas, Fissures, and Abscesses common
Chron’s- inflammatory process that begins with crypt inflammation & abscesses which turn into small, focal ulcers
Bowel wall thickens and becomes fibrotic and the intestinal wall narrows, diseased bowel loops can adhere to other loops surrounding them
Sx- insidious with diarrhea and prominent RLQ pain unrelieved by defecation
Eating can cause intestinal peristalsis, crampy pain pt tend not to eat leads to weigh loss and malnutrition and secondary anemia
Ulcers can leak a discharge in the colon
Disrupted absorption can cause chronic diarrhea and nutritional deficits---- weight loss and dehydration
Inflammed intestine perforates- lead to intrabdominal abscess----- fever, leukocytosis, chronnc symptoms- diarrhea, abd pain, steatorrhea, anorexia, weight loss, and nutritional deficiencies
CT scan, MRI, CBC, albumin and protein levels
Complications-intestinal obstruction or structure formation, perianal disease, fluid and electrolyte imbalances, malnutrition, fistula and abscess formation
Ulcerative Colitis
Ulcerative and inflammatory disease of mucuosal and submucosal layer
Most commonly occurs in rectum and colon
Periods of remissions and exacerbations
Fistulas and Fissures are uncommon
Bouts of abd cramps and bloody or purulent diarrhea, typically begin in rectum and progress through the colon
Bleeding occurs because of the ulcerations, the mucosa becomes edematous and inflamed , lesions occur one after the other, bowel eventually shortens, narrows, and thickens because of the muscular hypertrophy and fate deposits
The inflammatory is not transmural (only the inner lining) that is why abscesses, fistulas, obstruction, and fissures
Sx- diarrhea, with passage of mucus, pus, blood. LLQ, pain, tenesmus
Bleeding can be mild or severe. May see pallor, anemia, and fatigue. Anorexia, weight loss, fever, vomiting, dehydration.
Cramping and the passage of at least 6 stools per day
Classified as mild, severe, fulminant depending on how severe the symptoms are
Hypoalbuminemia, electrolyte imbalance, and anemia
Extraintestinal manifestaions such as skin lesions, eye lesions, and joint abnormalities, and liver disease
Assessment/Diagnostics
Abd xray, Colonoscopy. Biopsies may be taken
CT scan, MRI, and US- indicate abscess
CBC- WBC, Hgb, HCT, electrolytes, stool for occult and parasites,
C-reactive proteins
Complications
Toxic megacolon, perforation, bleeding- ulceration. Surgical intervention may be needed
Steroid use can lead to diminished bone density
Colon cancer may develop
Nutritional Therapy
Oral Fluids
Low Residue High Protein High Calorie Diet
Vitamin Replacement
Pharmacologic Therapy
Corticosteroids, Immunomodulators, Aminosalicylates
Surgical Management
Stricturplasty
Intestinal transplant
Colectomy
Bowel Obstruction
Can be mechanical or functional obstruction
Obstruction can be partial or complete and located in small or large bowel.
Most obstructions occur in the small intestine and are caused by adhesions
Manifestations
In SBO initial symptom is usually crampy pain that is wave-like and colicky. Other symptoms can include vomiting, dehydration, abdominal distention.
In LBO symptoms develop and progress relatively slowly. May experience constipation that can last for months, weakness, weight loss, anorexia. Eventually ABD will become distended and pt will have crampy lower abdominal pain.
Diagnosis
Typically diagnosed by abdominal Xray or CT
Diagnosis based on symptoms, physical findings, results of imaging
Bowel sounds are high-pitched and hyperactive in an attempt to pass obstruction
Later hypoactive, may indicate strangulation when there is a change in pattern
Lab studies CBC, electrolytes reveal dehydration, loss of plasma volume, and possible infection
Management
Decompression of bowel through NG tube, if unsuccessful or if obstruction is complete surgical intervention is necessary.
Gastric Tubes
NGT (for suction or feeds)
Large-bore (larger than 12 Fr)
Small-bore (Dobhoff)
Gastric
Stomach
Duodenum
Proximal jejunum
Nasoduodenal and nasojejunal feedings are indicated when the esophagus and stomach needs to be bypassed or when the patient at risk for aspiration
Tube feedings longer than 4 weeks, gastrostomy or jejunostomy tubes are preferred admin of meds or nutrition
Complications- dumping syndrome, aspiration, residual checks, and patency
Xrays should be performed before using an NGT
G-tube and J-tube
Peds- may have a PEG “button” than a tube
Nutrition
Parenteral Nutrition
Provides nutrients to the body by IV route
Given through Peripheral or Central Line, depends on pt condition
Inability to ingest at least 50% of daily required calories
Timeframe when to start depend on pt
Length of therapy is usually 5-7 days
Parental Nutrition- mixture of providing nutrients proteins, carbs, fats, electrolytes, vit, trace minerals, sterile water
Enteral Nutrition
Given to meet nutritional requirements when oral intake is inadequate or not possible and the middle and lower portions of the GI tract are functionally normal.
Can be given through NG, ND, G-tube, J-tube
Start therapy slow then increase to goal
Give peripheral route because solution is less hypertonic, not nutritionally complete because of the low dextrose content
Give central route because it is very high in solute concentration of blood
Diets
High Fiber Diet
Increases bulk in stool and reduces pressure within the colon
Low Residue Diet
Residue includes any food, including fiber that remains in your intestinal tract and contributes to stool.
Low Residue Diet is like low-fiber
May be used following abdominal surgery or during a flare-up of a digestive disorder such as diverticulitis or IBD.
Should only be used for a short time because it cannot provide al the nutrients necessary for staying healthy.
Foods that can be consumed include refined breads, cereals, crackers, chips, and pasta with less than 1 gram of fiber/serving, white rice, fruit juice with no pulp, strained broth-based soups
Foods to avoid whole grain breads, cereals, and pastas, peanut butter, seeds and nuts, tough or coarse meats
Surgeries
Avoided until complications such as bowel obstruction, perforation abscess and perianal occur.
Bowel resection-end to end anastomosis remove diseased portion and retaining as much bowel as possible
Ostomy-surgical creation of an opening into the bowel, allows for drainage of fecal matter to the outside of the body.
Name of ostomy is based on its location
Colostomy is opening into large colon (formed) effluent
Ileostomy is opening into the ileum or small intestine (liquid) effluent
Abd surgery post op
Ambulation
Pain meds
Monitor for fecal drainage 24-48 hours after ileostomy, 3-6 days after colostomy
Monitor labs esp electrolytes, fluid replacement
NGT to suction may be indicated
Emotional support
Managing skin and stoma care, change appliance
Managing dietary and fluid needs
Preventing complications