ADH and the Control of Osmolality in the Kidney
Body Water and Physiological Control
Total Body Water: In an adult human, approximately of the body is composed of water.
Physiological Control Factors: Two primary properties of body water are under strict physiological control:
Volume: Regulated via mechanisms such as blood pressure control, baroreceptors, and the renin-angiotensin-aldosterone system (RAAS).
Osmolality: This must be maintained at a constant level to ensure optimal physiological function, including muscle contraction and the generation of action potentials.
Osmolality and Osmolarity: Definitions and Usage
Osmolality: Defined as the number of osmoles per kilogram () of water.
Osmolarity: Defined as the number of osmoles per litre () of water.
Core Concept: Both terms describe the ability of solutes to lower the concentration of water in a solution.
Clinical and Practical Usage:
In clinical settings, the term "osmolality" is usually preferred.
In practice, there is no consistent usage, and the two terms are often used interchangeably.
Plasma Standard: Normal plasma osmolality is often cited as approximately .
Relative Osmolality and Cellular Impact
Isoosmotic (or Isotonic) Solution: A solution having the same osmolality as another. For example, a solution of approximately is isoosmotic to human plasma.
Hypoosmotic (or Hypotonic) Solution: A solution with a lower osmolality than another. For example, a solution of is hyposmotic relative to plasma.
Hyperosmotic (or Hypertonic) Solution: A solution with a higher osmolality than another. For example, a solution of is hyperosmotic relative to plasma.
Effects of Extracellular Osmolality on Cells:
Isoosmotic Environment: No net movement of water; the cell remains unchanged. spherical membrane surrounding a solution, water can cross membrane solute cant
Hypoosmotic Environment: Water moves into the cell along its concentration gradient, causing the cell to expand/swell.
Hyperosmotic Environment: Water moves out of the cell into the extracellular space, causing the cell to shrink.
Assumption: These effects assume a spherical membrane where water can cross but solutes cannot.
Functional Anatomy of the Kidney and Nephron
Structures of the Nephron:
Glomerulus and Bowman’s Capsule: Site of initial filtration.
Proximal Convoluted Tubule (PCT): Specialised for bulk reabsorption; possesses microvilli to increase surface area. It absorbs salt and water in equal proportions.
Loop of Henle: Divided into the descending limb and the ascending limb.
Distal Convoluted Tubule (DCT): The site for fine-tuning and regulation of reabsorption.
Collecting Duct: Divided into cortical and medullary sections.
Vasa Recta: The capillary system associated with the loop of Henle.
Zonal Organization: The kidney is divided into the Cortex (outer layer) and the Medulla (inner layer).
Evolutionary Perspective on Water Conservation
Loop of henle → essential to the ability to conserve water and control extracellular osmolarity
Vertebrate Groups with Loop of Henle: Mammalia and Aves (Birds). These groups possess a loop of Henle and a kidney subdivided into cortex and medulla. This allows them to inhabit environments where the water supply is variable.
Vertebrate Groups without Loop of Henle: Reptilia, Amphibia, Agnatha, Chondrichthyes, and Osteichthyes. These lack a loop of Henle and/or a subdivided kidney. They typically require a plentiful supply of water
Requirements for Osmotic Homeostasis
Obligatory Water Loss: The body produces waste that must be excreted in urine. The minimum daily urine production required to remove this waste is approximately . Water cannot be saved by simply avoiding urine production.
Urine Concentration Range: To regulate extracellular fluid osmolality, the kidneys must produce a range of concentrations, from hypoosmotic to hyperosmotic urine.
Passive Reabsorption: The kidney cannot actively reabsorb water because the energy demand would be too great. Instead, water is reabsorbed passively by osmosis to produce hyperosmotic urine.
Hyperosmotic Interstitium: To reabsorb water in excess of solute (to concentrate urine), there must be a region in the kidney medulla that is hyperosmotic.
The Loop of Henle: Countercurrent Multiplier Mechanism
Separation of Salt and Water Reabsorption:
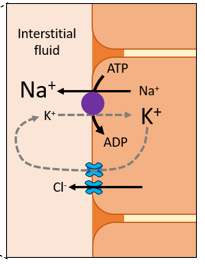
Ascending Limb: This limb is impermeable to water. It actively reabsorbs solutes ( and ) from the tubule lumen into the medullary interstitium.
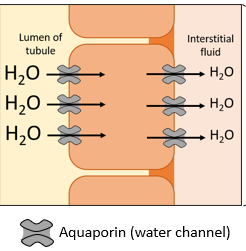
Descending Limb: This limb is freely permeable to water (due to the expression of aquaporins) but is not permeable to solutes. Water is passively reabsorbed into the medullary interstitium.
Osmolality Changes in the Filtrate: reabsorption of salt is separated form the reabsorption of water
Entering the Loop: Filtrate is isoosmotic to plasma ().
At the Bend of the Loop: Filtrate becomes highly concentrated/hyperosmotic ().
Exiting the Loop: Filtrate becomes hypoosmotic to plasma () and the volume is significantly reduced.
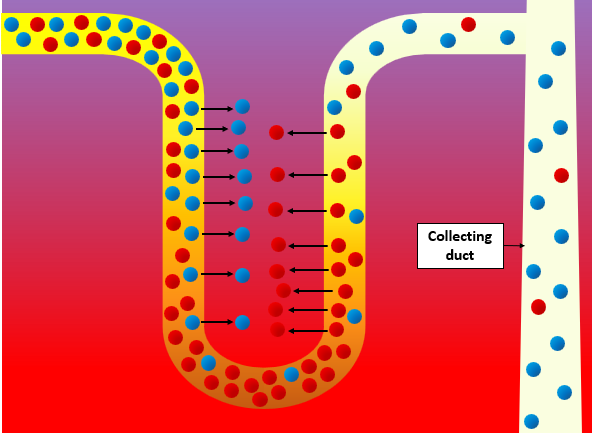
The Medullary Interstitium: At each level of the descending limb, water is reabsorbed until equilibrium is reached between the osmolarity of the filtrate and the osmolarity of the medullary interstitium (becomes progressively hyperosmotic, reaching a maximum of approximately at the deepest part of the medulla.
This gradient is created by the "countercurrent multiplier" mechanism (named for the counter-permeability of the limbs).
Urea Handling and Urea Trapping
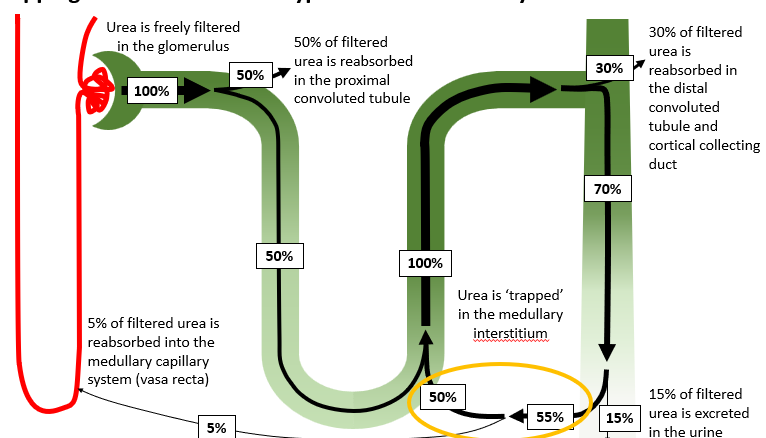
Urea Filtration: Urea is freely filtered in the glomerulus ( filtered load).
Proximal Reabsorption: Approximately of filtered urea is reabsorbed in the Proximal Convoluted Tubule.
Medullary Secretion: Approximately of filtered urea is secreted back into the Loop of Henle by passive diffusion.
Distal Reabsorption: Approximately of filtered urea is reabsorbed in the Distal Convoluted Tubule and cortical collecting duct.
Medullary Reabsorption (Trapping): Approximately of filtered urea is reabsorbed in the Medullary Collecting Duct into the medullary interstitium.
Secreted: about 50
5 of filtered urea is secreted by passive diffusion into the loop of henle
Vasa Recta Removal: About of filtered urea is reabsorbed into the vasa recta capillary system.
Excretion: Only about of filtered urea is ultimately excreted in the urine.
Function: This "trapping" of urea in the medullary interstitium is a critical contributor to the hyperosmotic environment required for water reabsorption.
The Vasa Recta capillary system
Structure: The vasa recta consists of "straight loops" of capillaries.
Function: blood flow passing directly through the interstitium would wash away the osmotic gradient
plasma osmolarity in the vasa recta equilibrates with the interstitium
Maintenance of Gradient: Solute and water reabsorbed by the Loop of Henle are removed by the vasa recta in equal proportions, thus preserving the hyperosmotic medullary interstitium.
Regulation of Urine Concentration by ADH
Antidiuretic Hormone (ADH): Also known as vasopressin or arginine vasopressin. It is a peptide hormone.
Production of Hypoosmotic (Dilute) Urine:
Occurs when the medullary collecting duct is not very permeable to water.
The hypoosmotic filtrate exiting the Loop of Henle flows down the collecting duct and is released as hypoosmotic urine.
Production of Hyperosmotic (Concentrated) Urine:
ADH causes the insertion of aquaporins into the membranes of the medullary collecting duct cells.
This significantly increases the permeability of the collecting duct to water.
Water is reabsorbed via osmosis into the hyperosmotic interstitium.
The filtrate becomes progressively hyperosmotic as it descends, resulting in concentrated urine.
Cellular Mechanism and Secretion of ADH
ADH is a peptide, also known as vasopressin or arginine vasopressin
Mechanism of Action:
ADH binds to V2 receptors on the medullary collecting duct cell membranes.
The V2 receptor is a G protein-coupled receptor.
Activation triggers a signalling cascade that leads to the insertion of water channels (aquaporins) into the cell membrane, allowing water absorption into the hyperosmotic interstitium.
Synthesis and Release:
ADH is synthesized by neurons located in the supraoptic and paraventricular nuclei of the hypothalamus.
It is transported down these neurons and released into the capillaries of the posterior pituitary, entering the general circulation.
Control of Secretion (Osmoreceptors):
The ADH neurons in the supraoptic and paraventricular nuclei receive input from central osmoreceptors
these osmoreceptors detect changes in plasma osmolarity
Increased plasma osmolality: Increases the rate of ADH secretion.
Decreased plasma osmolality: Decreases the rate of ADH secretion.
Secondary Control (Baroreceptors): In cases of severe fluid loss, such as a haemorrhage, baroreceptors can stimulate ADH secretion to promote water conservation even if osmolality isn't the primary trigger.
Summary of Systemic Response to Increased Plasma Osmolality
Increase in Plasma Osmolality leads to:
Osmoreceptor Activation, which triggers:
Thirst, leading to the ingestion of water.
ADH Secretion from the hypothalamus/posterior pituitary.
Increased Plasma ADH leads to:
Increased permeability of kidney collecting ducts.
Increased Water Reabsorption results in:
Decreased water excretion.
A negative feedback loop that brings plasma osmolality back toward normal.
Questions & Discussion
Question: Diabetes insipidus is caused by an inability to produce or respond to ADH (e.g., a mutation in the V2 receptor). Which of the following would be a symptom of diabetes insipidus? A) ‘Overproduction’ of urine. B) Limited production of urine.
Answer: A) ‘Overproduction’ of urine.
Explanation: If there is no response to ADH, the permeability of the collecting duct is not increased. Water cannot be reabsorbed into the hyperosmotic medullary interstitium, leading to the production of a large volume of very dilute urine. This is distinct from Diabetes mellitus, which involves blood sugar regulation.